Towards an Ergonomic Assessment Framework for Industrial Assembly Workstations—A Case Study

 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
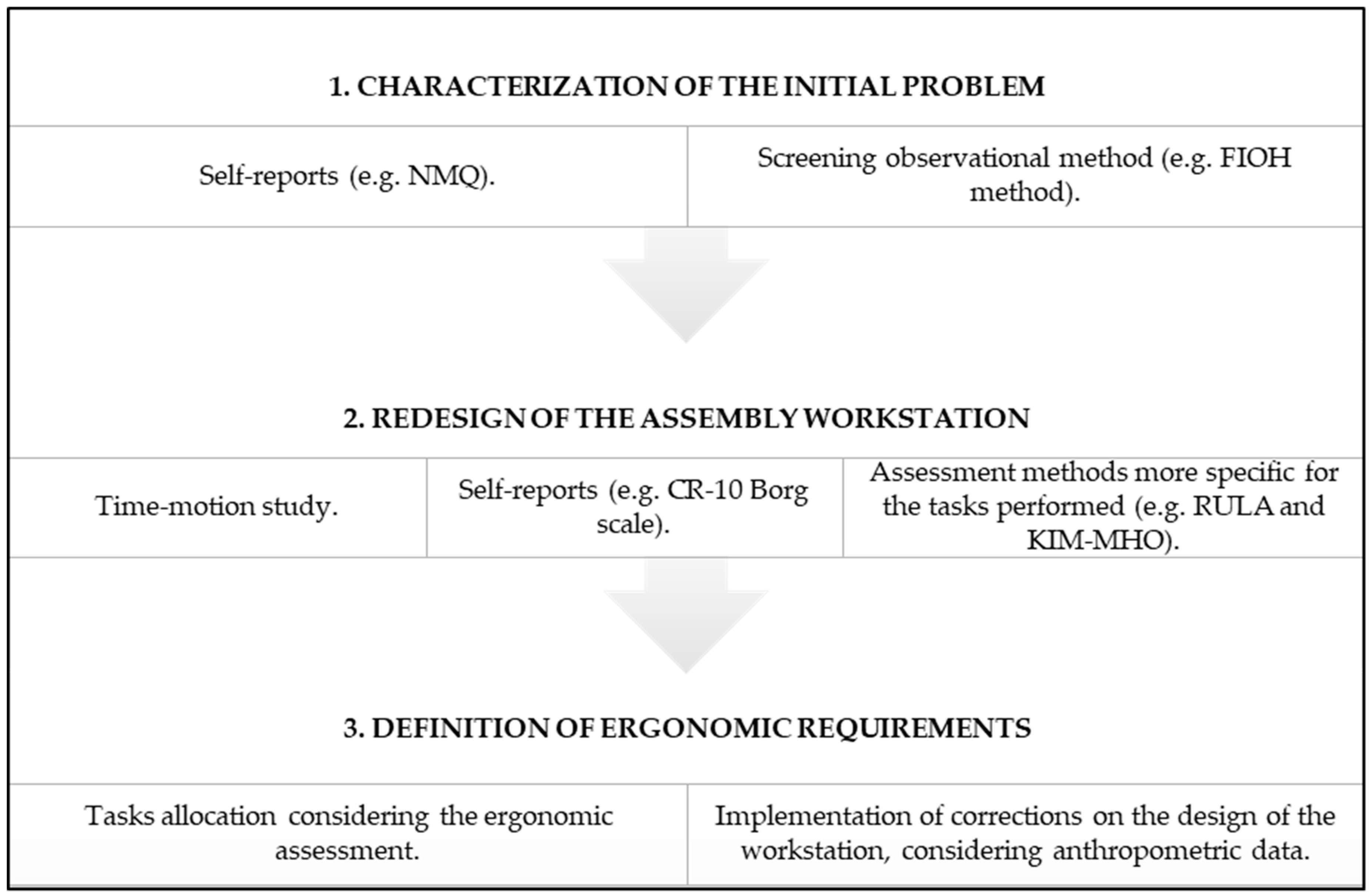
2. Materials and Methods
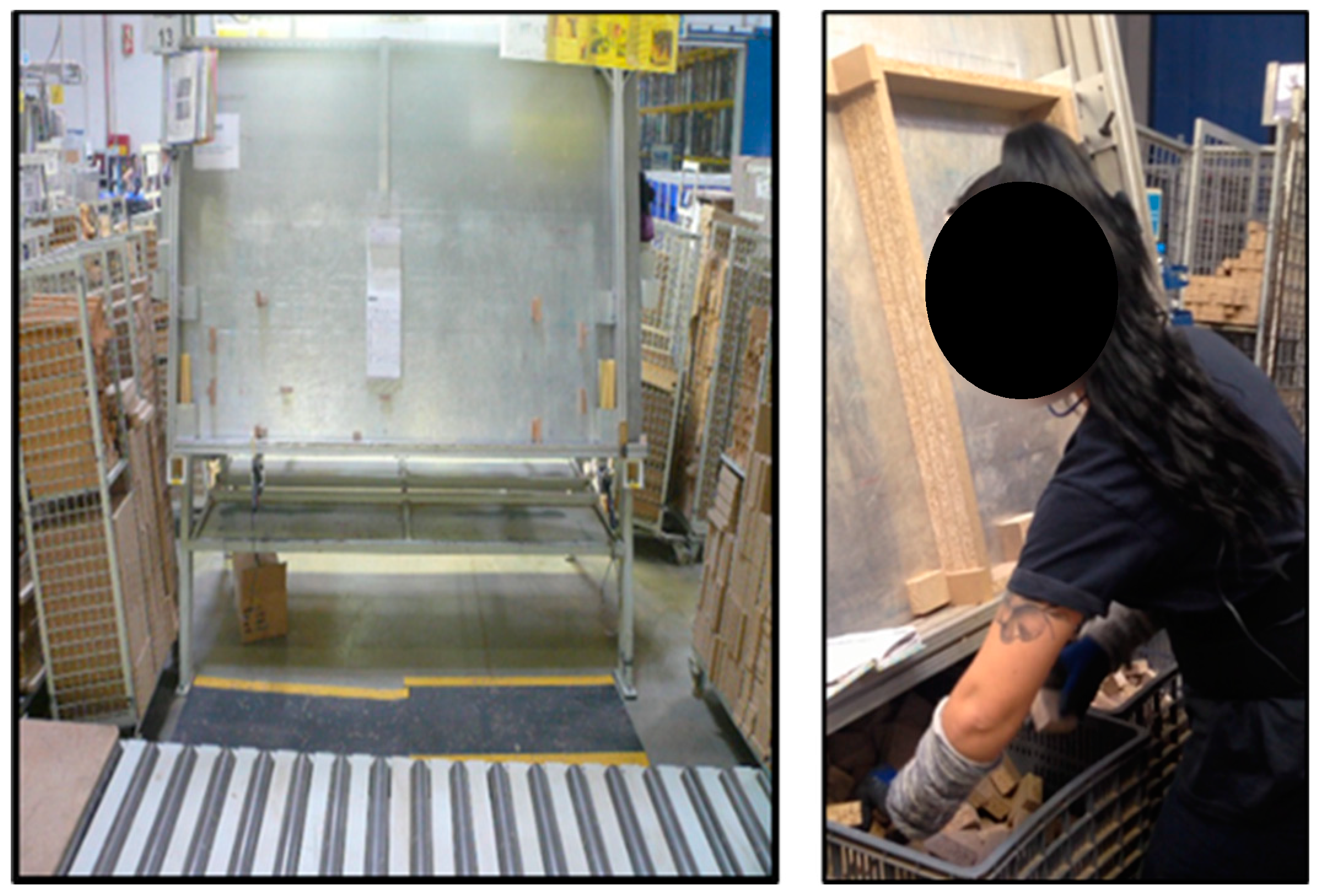
2.1. Description of the Initial Problem
2.2. Existing Assembly Workstations—Ergonomic Assessment
2.3. Preassembly Workstation—Ergonomic Assessment
2.4. Statistical Analysis
3. Results and Discussion
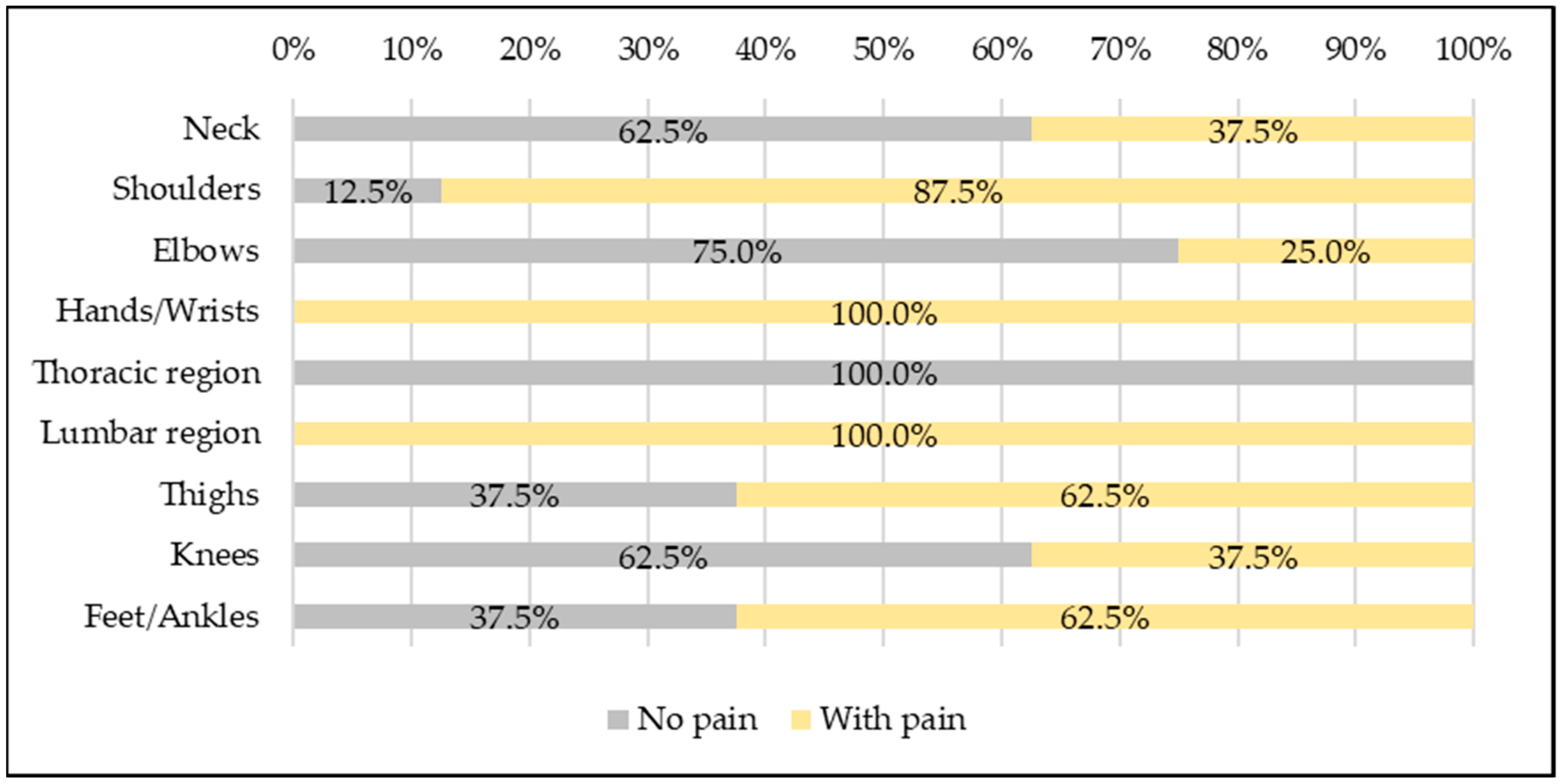
3.1. Characterization of the Initial Problem—Assembly Workers and Workstations
3.2. Redesign of the Assembly Process and Preassembly Workstation
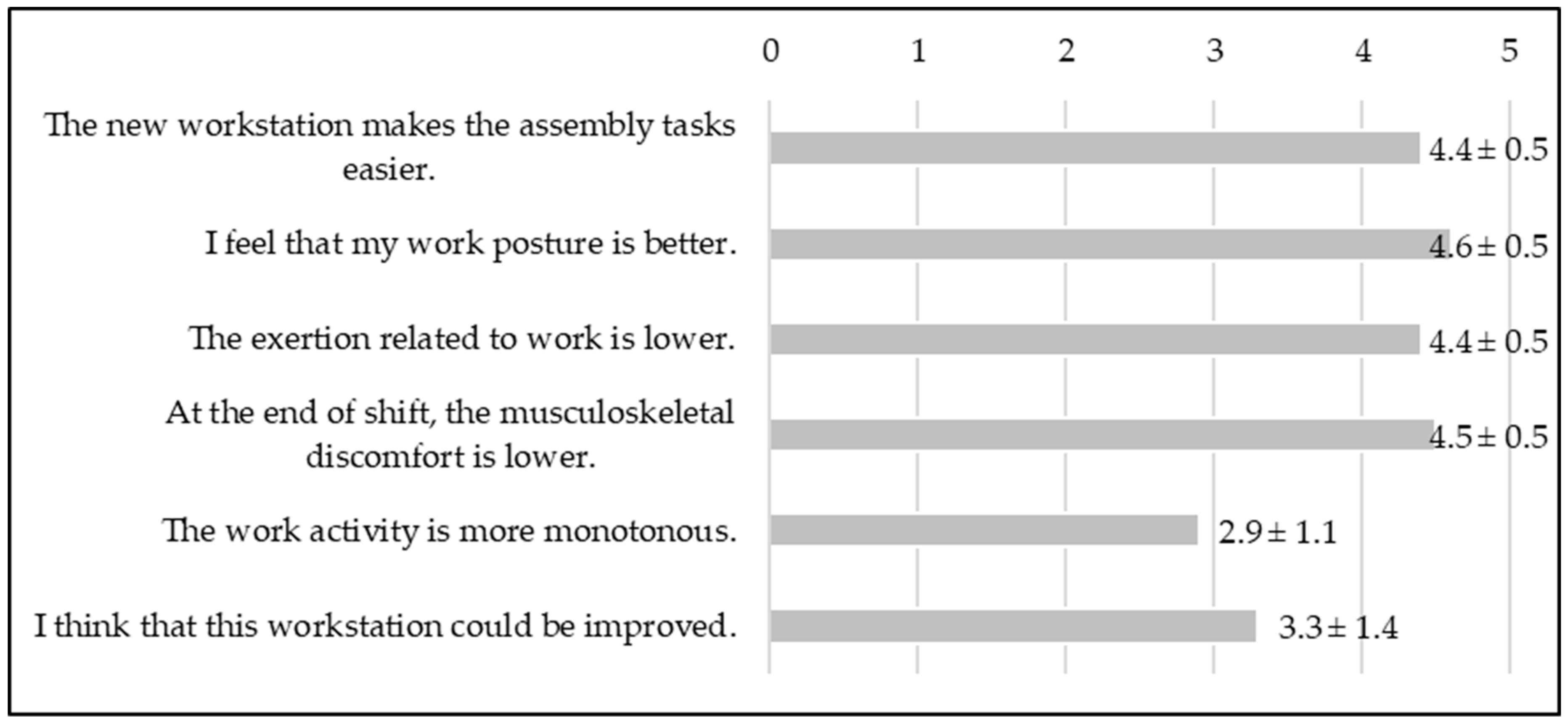
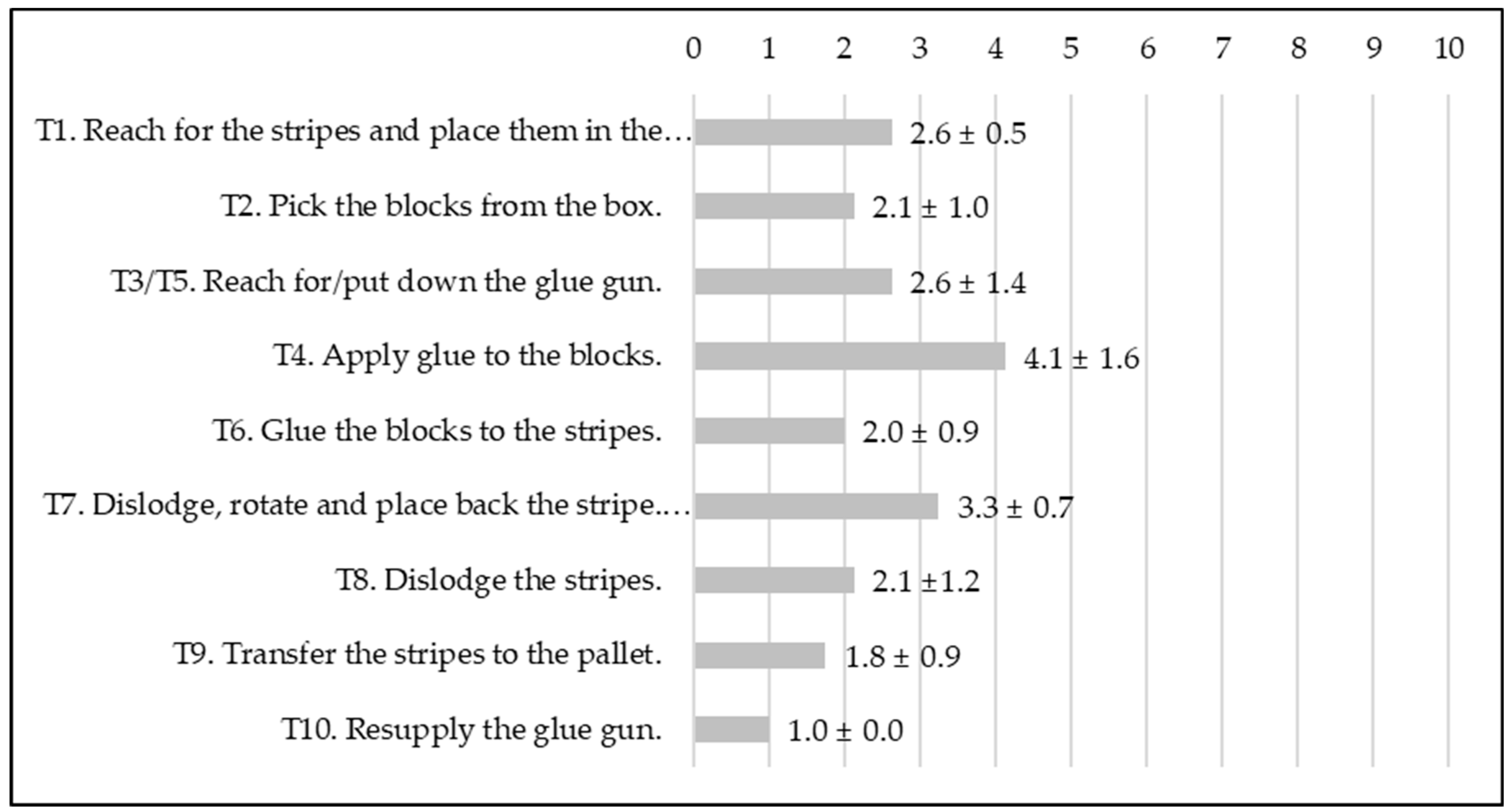
3.3. Preassembly Workers and Workstation
3.4. Definition of the Ergonomic Requirements and Future work
- (i)
- Replace/eliminate the task of apply glue, since it is a critical task according to ergonomics’ point of view and physically demanding due to the actions repeated. Moreover, the burns motivated by the hot glue constitute the accident more frequent in this section;
- (ii)
- Height-correction of the workbench to accommodate the workers’ variability in terms of anthropometric data [37], located between 1066 mm (95th percentile of shoulders height of the Portuguese adult women) and 914 mm (5th percentile of shoulders height of the Portuguese adult women);
- (iii)
- Diversification of the work content through the inclusion of different tasks/interactions between workers and/or COBOT (the preassembly workstation is monotonous and repetitive);
- (iv)
- Implementation of corrective measures to reduce noise exposure, which difficult communication and increases muscular tension;
- (v)
- Correct the baseboard location, eliminating the lateral conveyor or introducing a rotative table for the palletizing zone.
Author Contributions
Funding
Conflicts of Interest
References
- Schneider, E.; Irastorza, X.; Copsey, S. OSH in Figures: Work-Related Musculoskeletal Disorders in the EU; Publication: Luxembourg, Luxembourg, 2010. [Google Scholar]
- Bevan, S. Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Pract. Res. Clin. Rheumatol. 2015, 29, 356–373. [Google Scholar] [CrossRef]
- Chen, D.; Cai, Y.; Cui, J.; Chen, J.; Jiang, H.; Huang, M.C. Risk factors identification and visualization for work-related musculoskeletal disorders with wearable and connected gait analytics system and kinect skeleton models. Smart Heal. 2018, 7–8, 60–77. [Google Scholar] [CrossRef]
- Petreanu, V.; Seracin, A.M. Risk Factors for Musculoskeletal Disorders Development: Hand-Arm Tasks, Repetitive Work; National Research-Development for Health and Safety: Bucarest, Romania, 2017. [Google Scholar]
- Battini, D.; Faccio, M.; Persona, A.; Sgarbossa, F. New methodological framework to improve productivity and ergonomics in assembly system design. Int. J. Ind. Ergon. 2011, 41, 30–42. [Google Scholar] [CrossRef]
- Otto, A.; Scholl, A. Incorporating ergonomic risks into assembly line balancing. Eur. J. Oper. Res. 2011, 212, 277–286. [Google Scholar] [CrossRef]
- Burdorf, A. The role of assessment of biomechanical exposure at the workplace in the prevention of musculoskeletal disorders. Scand. J. Work. Environ. Heal. 2010, 36, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Takala, E.-P.; Pehkonen, I.; Forsman, M.; Hansson, G.-A.; Mathiassen, S.E.; Neumann, W.P.; Sjøgaard, G.; Veiersted, K.B.; Westgaard, R.H.; Winkel, J. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand. J. Work. Environ. Heal. 2010, 36, 3–24. [Google Scholar] [CrossRef] [Green Version]
- David, G. Ergonomic methods for assessing exposure to risk factors for work-related musculoskeletal disorders. Occup. Med. 2005, 55, 190–199. [Google Scholar] [CrossRef] [Green Version]
- Ellegast, R. Assessment of Physical Workloads to Prevent Work-Related MSDs; Institute for Occupational Safety and Health of the German Social Accident Insurance: Berlin, Germany, 2016. [Google Scholar]
- Kuorinka, I.; Jönsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sorensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Crawford, J. The Nordic Musculoskeletal Questionnaire. Occup. Med. 2007, 57, 300–301. [Google Scholar] [CrossRef] [Green Version]
- NIOSH. Ergonomic Hazard Identification Checklist; NIOSH: Washington, DC, USA.
- McAtamney, L.; Corlett, N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Baua–Federal Institute for Occupational Safety and Health. Key Indicator Method for Assessing and Designing Physical Workloads during Manual Handling Operations KIM-MHO; Baua–Federal Institute for Occupational Safety and Health: Dortmund, Germany, 2012. [Google Scholar]
- Schaub, K.; Caragnano, G.; Britzke, B.; Bruder, R. The European Assembly Worksheet. Theor. Issues Ergon. Sci. 2013, 14, 616–639. [Google Scholar] [CrossRef]
- Tan, J.T.C.; Duan, F.; Zhang, Y.; Watanabe, K.; Kato, R.; Arai, T. Human-robot collaboration in cellular manufacturing: Design and development. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2009), St. Louis, MO, USA, 10–15 October 2009; pp. 29–34. [Google Scholar]
- Cherubini, A.; Passama, R.; Crosnier, A.; Lasnier, A.; Fraisse, P. Collaborative manufacturing with physical human-robot interaction. Robot. Comput.-Integr. Manuf. 2016, 40, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Tsarouchi, P.; Makris, S.; Chryssolouris, G. Human–robot interaction review and challenges on task planning and programming. Int. J. Comput. Integr. Manuf. 2016, 29, 916–931. [Google Scholar] [CrossRef]
- Villani, V.; Sabattini, L.; Czerniak, J.; Mertens, A.; Vogel-Heuser, B.; Fantuzzi, C. Towards modern inclusive factories: A methodology for the development of smart adaptive human-machine interfaces. In Proceedings of the 22nd IEEE International Conference on Emerging Technologies and Factory Automation (ETFA), Limassol, Cyprus, 12–15 September 2017; pp. 1–7. [Google Scholar]
- El Zaatari, S.; Marei, M.; Li, W.; Usman, Z. Cobot programming for collaborative industrial tasks: An overview. Rob. Auton. Syst. 2019, 116, 162–180. [Google Scholar] [CrossRef]
- Bogataj, D.; Battini, D.; Calzavara, M.; Persona, A. The ageing workforce challenge: Investments in collaborative robots or contribution to pension schemes, from the multi-echelon perspective. Int. J. Prod. Econ. 2019, 210, 97–106. [Google Scholar] [CrossRef]
- Ahonen, M.; Launis, M.; Kuorinka, T. Ergonomic Workplace Analysis; Institute of Occupational Health: Logica, Finland, 1989. [Google Scholar]
- Kayis, B.; Kothiyal, K. A Multilevel Approach to Manual Lifting in Manufacturing Industries. Int. J. Occup. Saf. Ergon. 1996, 2, 251–261. [Google Scholar] [CrossRef]
- Petit, A.; Mairiaux, P.; Desarmenien, A.; Meyer, J.P.; Roquelaure, Y. French good practice guidelines for management of the risk of low back pain among workers exposed to manual material handling: Hierarchical strategy of risk assessment of work situations. Work 2016, 53, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Shariat, A.; Cleland, J.A.; Danaee, M.; Alizadeh, R.; Sangelaji, B.; Kargarfard, M.; Ansari, N.N.; Sepehr, F.H.; Tamrin, S.B.M. Borg CR-10 scale as a new approach to monitoring office exercise training. Work 2018, 60, 549–554. [Google Scholar] [CrossRef]
- Fischer, S.L.; Dickerson, C.R. Applying psychophysics to prevent overexposure: On the relationships between acceptable manual force, joint loading, and perception. Int. J. Ind. Ergon. 2014, 44, 266–274. [Google Scholar] [CrossRef]
- Mesquita, C.C.; Ribeiro, J.C.; Moreira, P. Portuguese version of the standardized Nordic musculoskeletal questionnaire: Cross cultural and reliability. J. Public Health 2010, 18, 461–466. [Google Scholar] [CrossRef]
- Kim, W.; Lorenzini, M.; Balatti, P.; Nguyen, P.D.; Pattacini, U.; Tikhanoff, V.; Peternel, L.; Fantacci, C.; Natale, L.; Metta, G.; et al. Adaptable Workstations for Human-Robot Collaboration: A Reconfigurable Framework for Improving Worker Ergonomics and Productivity. IEEE Robot. Autom. Mag. 2019, 26, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Chiasson, M.E.; Imbeau, D.; Major, J.; Aubry, K.; Delisle, A. Influence of musculoskeletal pain on workers’ ergonomic risk-factor assessments. Appl. Ergon. 2015, 49, 1–7. [Google Scholar] [CrossRef]
- Li, X.; Gül, M.; Al-Hussein, M. An improved physical demand analysis framework based on ergonomic risk assessment tools for the manufacturing industry. Int. J. Ind. Ergon. 2019, 70, 58–69. [Google Scholar] [CrossRef]
- Roman-Liu, D. Comparison of concepts in easy-to-use methods for MSD risk assessment. Appl. Ergon. 2014, 45, 420–427. [Google Scholar] [CrossRef]
- Klussmann, A.; Liebers, F.; Gebhardt, H.; Rieger, M.A.; Latza, U.; Steinberg, U. Risk assessment of manual handling operations at work with the key indicator method (KIM-MHO)—Determination of criterion validity regarding the prevalence of musculoskeletal symptoms and clinical conditions within a cross-sectional study. BMC Musculoskelet. Disord. 2017, 18, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Colim, A.; Sousa, N.; Carneiro, P.; Costa, N.; Arezes, P.; Cardoso, A. Ergonomic Intervention on a Packing Workstation with Robotic Aid—Case Study at a Furniture Manufacturing Industry. Work A J. Prev. Assess. Rehabil. 2020, 66. (in press). [Google Scholar]
- De Guimarães, L.B.M.; Anzanello, M.J.; Ribeiro, J.L.D.; Saurin, T.A. Participatory ergonomics intervention for improving human and production outcomes of a Brazilian furniture company. Int. J. Ind. Ergon. 2015, 49, 97–107. [Google Scholar] [CrossRef]
- Khan, M.; Pope-Ford, R. Improving and Modifying the Design of Workstations within a Manufacturing Environment. Procedia Manuf. 2015, 3, 4927–4934. [Google Scholar] [CrossRef]
- Barroso, M.P.; Arezes, P.M.; da Costa, L.G.; Miguel, A.S. Anthropometric study of Portuguese workers. Int. J. Ind. Ergon. 2005, 35, 401–410. [Google Scholar] [CrossRef]
- Fletcher, S.; Johnson, T.; Adlon, T.; Larreina, J.; Casla, P.; Parigot, L.; Alfaro, P.J.; Otero, M.D.M. Adaptive automation assembly: Identifying system requirements for technical efficiency and worker satisfaction. Comput. Ind. Eng. 2020, 139, 105772. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions’ Category | Parameters Assessed | Objectives | Tools Applied |
|---|---|---|---|
| Gender, age, work experience; preferred hand; WMSD. | To characterize the workers’ sample with demographic data. | Direct questions. |
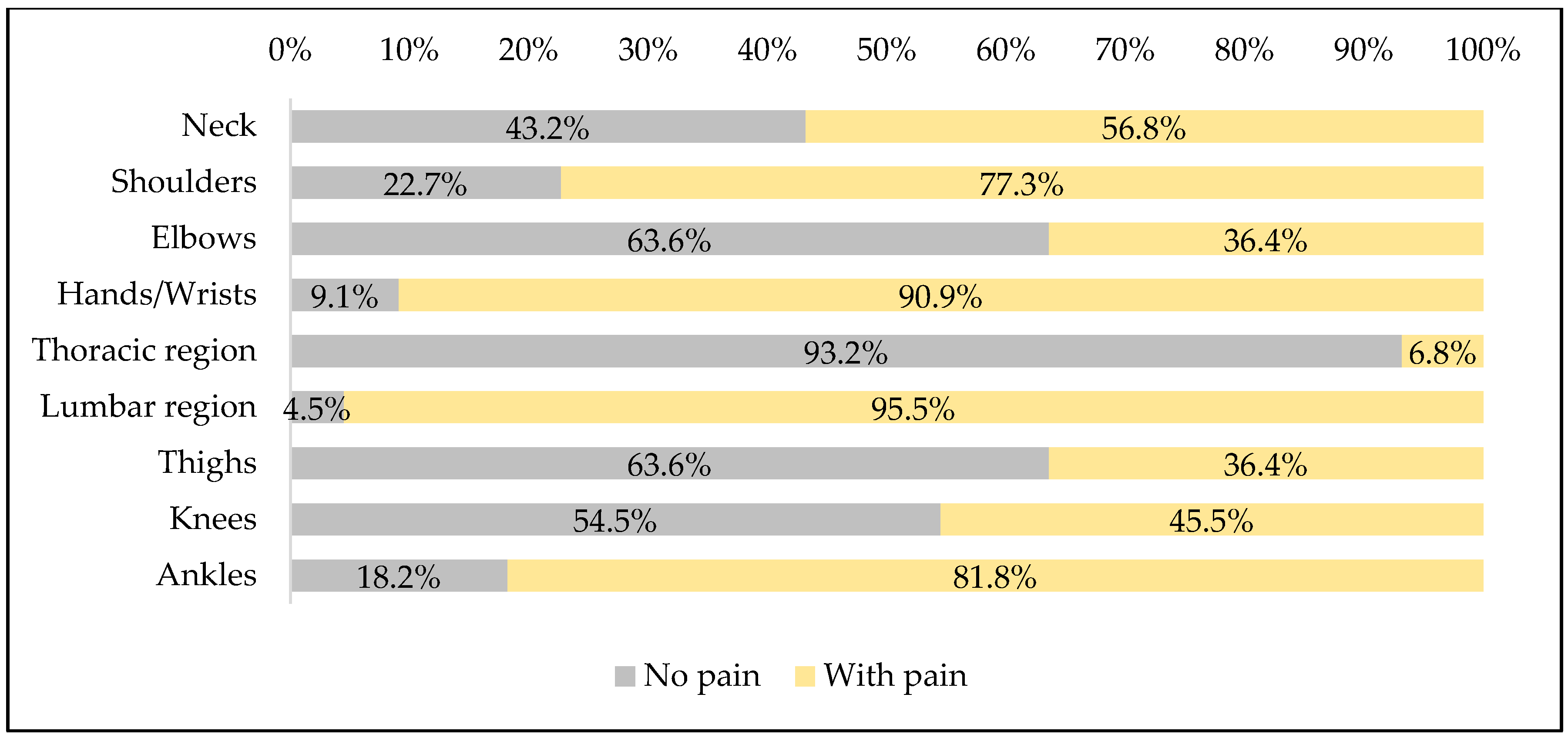
| Musculoskeletal symptomology self-reported for the entire body. | To characterize musculoskeletal symptomology of the preassembly workers. | NMQ with closed answers “yes/no” and VAS to assess pain intensity. |
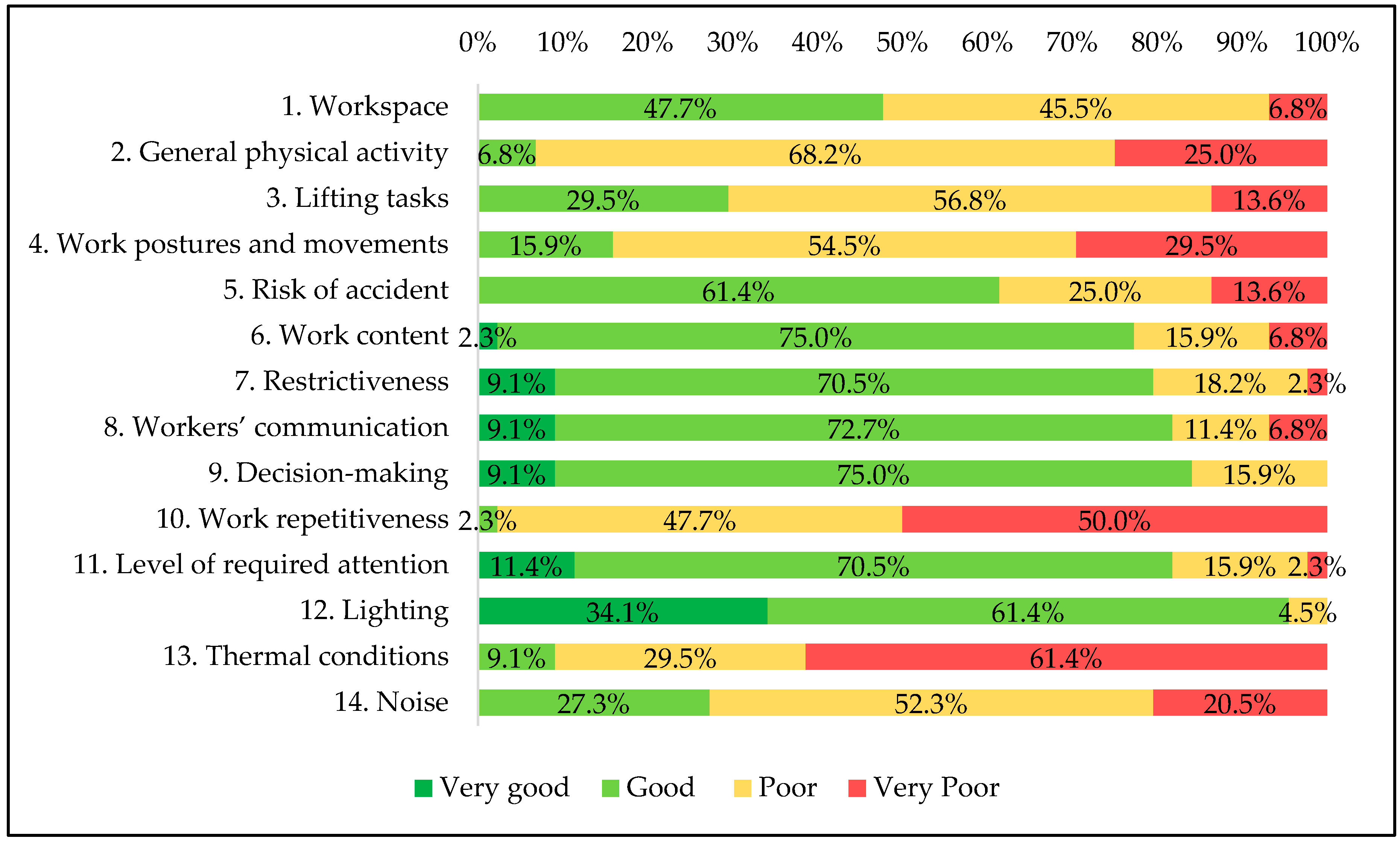
| 14 topics that influence the ergonomic conditions. | To assess globally the workstation by the workers’ perceptions. | Scale based on the FIOH method. |
| Questions’ Category | Parameters Assessed | Objectives | Tools Applied |
|---|---|---|---|
| Gender, age, work experience; preferred hand; WMSD. | To characterize the workers’ sample with demographic data. | Direct questions. |
| Musculoskeletal symptomology self-reported for the entire body. | To characterize musculoskeletal symptomology of the preassembly workers. | NMQ with closed answers “yes/no” and VAS to assess pain intensity. |
| Perceived exertion for each preassembly task. | To assess physical exertion perceived by the workers; To identify the most demanding tasks. | CR-10 Borg scale. |
| Global opinion about the preassembly workstation. | To compare the preassembly with the assembly workstation; To assess workers’ opinions about possible improvements to introduce in the preassembly workstation; | 5-Likert scale. |
| Method | Focus | Risk Factors Included | Output | Advantages | Limitations |
|---|---|---|---|---|---|
| RULA | Manufacturing and handling tasks in standing or seating posture, as well as work office, allowing the WMSD risk assessment for different body parts (upper limbs, shoulders, neck, and trunk). | Posture of arm, forearm, wrist, neck, and trunk; Repetition/frequency; Load/force. | RULA risk rating with four action levels, indicating the requirements for action on the workplace/task. | Detailed posture analysis considering different body parts; Relevant set of WMSD risk factors is considered. | Time-consuming; Difficulties to assess hand/wrist posture through observation; Repetition/frequency information is vague. |
| KIM-MHO | MHO with repetitive motion and predominantly lower force expenses of the upper extremities. | Duration of tasks; Type of force exertion in the finger-hand area; Repetition of movements/duration of holding; Force transfer/gripping conditions; Hand/arm position and movement; Work organization; Working conditions; Global body posture. | KIM final score with four risk ranges, indicating the possibility of physical overload occurrence and, consequently, the need for workplace redesign. | Complete analysis of the main risk factors for Work-related Upper Limb Disorders (WULD); Application facilitated by illustrations and descriptions for the rating points for the different risk factors. | Assessment of the level of force and posture is less accurate. |
| Global Risk Level | RULA | KIM-MHO | ||
|---|---|---|---|---|
| Final Score | Meaning | Final Score | Meaning | |
| I | 1 or 2 | It indicates that posture is acceptable if it is not maintained or repeated for long periods. | <10 | Low load situation, the health risk from physical overload is unlikely to appear. |
| II | 3 or 4 | It indicates that further investigation is needed and changes may be required. | 10 to <25 | Moderate load situation, physical overload is possible for less resilient persons. For this group redesign of the workplace is helpful. |
| III | 5 or 6 | It indicates that investigation and changes are required soon. | 25 to <50 | Increased load situation, physical overload also possible for normally resilient persons. The redesign of the workplace should be reviewed. |
| IV | 7 | It indicates that investigation and changes are required immediately. | ≥50 | High load situation, physical overload is likely to appear. Workplace redesign is necessary. |
| Topic Assessed | Expert Assessment | Comment |
|---|---|---|
| 4 | There are serious deviations from the recommendations. Workplace arrangement obliges workers to adopt difficult postures and movements (such as arms elevation above the shoulders). |
| 3 | The work activity depends on the production method and work organization. For some situations/references production, exist the risk of physical overload due to work peaks. |
| 4 | Heavier loads equal to 14 kg, frequently handling above the shoulders and below the knees. |
| 5 | Need for quick arm movements. |
| 3 | Burns for hot glue is very frequent, but the severity is low. |
| 3 | The workers perform only a part of the work entity. |
| 4 | Production management requirements restrict method and work pace. |
| 2 | The communication between workers is possible, but it is difficulted by the noise. |
| 2 | The work consists of simple tasks. |
| 4 | Cycle duration of less than 5 min. |
| 3 | Medium level of attention (assembly work) in more than half of the cycle. |
| 2 | Considering the workstation with a lower illuminance level (412 lux) and the recommended value (500 lux). |
| 4 | Air temperature is high for the metabolism associated with the tasks. |
| 5 | Noise level above 80 dB(A) and the workers need to communicate (teamwork). |
| Tasks | Description | Mean time per cycle (SD) (s) |
|---|---|---|
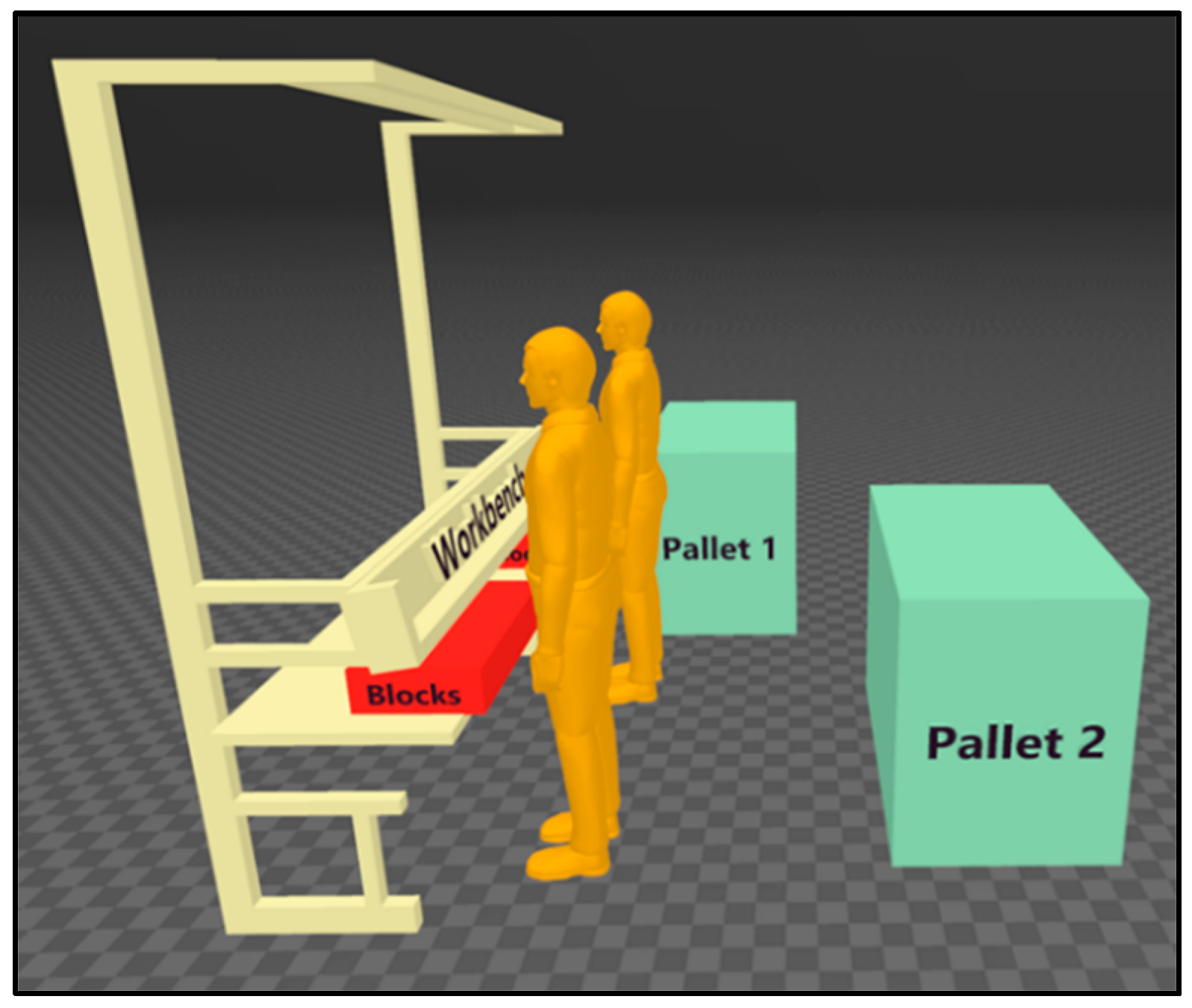
| T1 | Reach for the stripes from pallet 1 and place them in the assembly workbench (by one worker). | 2.5 ± 0.9 |
| T2 | Pick the blocks from the box. | 7.7 ± 1.2 |
| T3 | Reach for the glue gun. | 2.7 ± 0.3 |
| T4 | Apply glue to the blocks. | 4.1 ± 0.5 |
| T5 | Put down the glue gun. | 3.2 ± 0.6 |
| T6 | Glue the blocks to the stripes. | 9.4 ± 1.9 |
| T7 | Dislodge, rotate and place back the stripe. | 3.1 ± 0.9 |
| T8 | Dislodge the stripes. | 1.6 ± 1.0 |
| T9 | Transfer the stripes to the pallet 2. | 3.2 ± 2.0 |
| T10 | Resupply the glue gun. | 0.7 ± 0.0 |
| RULA | KIM-MHO | |||
|---|---|---|---|---|
| Task | Rating Mean (SD) | Risk Level | Risk Score | Risk Level |
| Task 1—Reach a stripe and align. | 3.2 (0.4) | II | 48 | III |
| Task 2—Reach blocks and stack. | 3.6 (0.9) | II | 48 | III |
| Task 3—Reach the glue pistol. | 3.0 (0.0) | II | 34 | III |
| Task 4—Apply glue to the blocks. | 3.0 (0.0) | II | 64 | IV |
| Task 5—Put the glue pistol on the support. | 3.0 (0.0) | II | 34 | III |
| Task 6—Fix blocks on the stripe. | 4.4 (0.5) | II | 48 | III |
| Task 7—Relocate or reverse the stripe. | 3.0 (0.0) | II | 30 | III |
| Task 8—Take off stripe. | 3.2 (0.4) | II | 40 | III |
| Task 9—Transfer stripe to the pallet. | 4.4 (1.3) | II | 46 | III |
| Task 10—Supply the glue pistol. | 3.0 (0.0) | II | 44 | III |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colim, A.; Faria, C.; Braga, A.C.; Sousa, N.; Rocha, L.; Carneiro, P.; Costa, N.; Arezes, P. Towards an Ergonomic Assessment Framework for Industrial Assembly Workstations—A Case Study. Appl. Sci. 2020, 10, 3048. https://doi.org/10.3390/app10093048
Colim A, Faria C, Braga AC, Sousa N, Rocha L, Carneiro P, Costa N, Arezes P. Towards an Ergonomic Assessment Framework for Industrial Assembly Workstations—A Case Study. Applied Sciences. 2020; 10(9):3048. https://doi.org/10.3390/app10093048
Chicago/Turabian StyleColim, Ana, Carlos Faria, Ana Cristina Braga, Nuno Sousa, Luís Rocha, Paula Carneiro, Nélson Costa, and Pedro Arezes. 2020. "Towards an Ergonomic Assessment Framework for Industrial Assembly Workstations—A Case Study" Applied Sciences 10, no. 9: 3048. https://doi.org/10.3390/app10093048