Vitamin C and Cardiovascular Disease: An Update
by
 ,
,
Marco B. Morelli
1,2,†, 
Jessica Gambardella
1,2,3,4,†,
Vanessa Castellanos
1 ,
,
Valentina Trimarco
5,* and
Gaetano Santulli
1,2,3,4,*
1
Division of Cardiology, Department of Medicine, Institute of Aging Research, Wilf Family Cardiovascular Research Institute, Albert Einstein College of Medicine, Montefiore University Hospital, New York, NY 10461, USA
2
Department of Molecular Pharmacology, Fleischer Institute for Diabetes and Metabolism (FIDAM), Einstein-Sinai Diabetes Research Center (ES-DRC), Albert Einstein College of Medicine, New York, NY 10461, USA
3
Department of Advanced Biomedical Sciences, “Federico II” University, 80131 Naples, Italy
4
International Translational Research and Medical Education (ITME), 80100 Naples, Italy
5
Department of Neuroscience, “Federico II” University, 80131 Naples, Italy
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally.
Antioxidants 2020, 9(12), 1227; https://doi.org/10.3390/antiox9121227
Submission received: 5 October 2020
/
Revised: 24 November 2020
/
Accepted: 27 November 2020
/
Published: 3 December 2020
(This article belongs to the Special Issue Free Radicals and Cardiovascular Diseases)
Abstract
:The potential beneficial effects of the antioxidant properties of vitamin C have been investigated in a number of pathological conditions. In this review, we assess both clinical and preclinical studies evaluating the role of vitamin C in cardiac and vascular disorders, including coronary heart disease, heart failure, hypertension, and cerebrovascular diseases. Pitfalls and controversies in investigations on vitamin C and cardiovascular disorders are also discussed.
1. Physiology of Vitamin C
Vitamin C is a carbohydrate-like substance first isolated in 1928 by Albert Szent-Györgyi from cabbage, paprika, and the adrenal glands of some animals [1,2]; it was later found to be identical with the antiscorbutic factor that had been isolated from lemon juice by Sylvester Solomon Zilva in 1924 [3]. Originally called ‘hexuronic acid’ by Györgyi, the current denomination as vitamin C was proposed in 1933 by Walter Norman Haworth [4,5].
Among the vastly biological functions in which vitamin C is involved, as a potent antioxidant and radical scavenger, it protects cell constituents against oxidative stress, mediated by reactive oxygen species (ROS) and free radicals [6,7,8]. Moreover, vitamin C redox potential allows the maintenance of reduced and regeneration of other antioxidants, including glutathione and α–tocopherol (vitamin E) [9,10,11]. It is also required for the synthesis of several crucial biomolecules since it acts as a cofactor of the monooxygenase and dioxygenase enzymes [12]. Vitamin C-dependent enzymatic reactions are involved in the biosynthesis of collagen and cellular procollagen secretion, L-carnitine, norepinephrine, epinephrine, and for the regulation of the biosynthesis of other molecules [13,14]. Furthermore, vitamin C intake from food or supplements can increase the bioavailability of iron by improving the absorption of the non-heme iron [15,16,17,18].
2. Genetics and Diet
The crucial biological functions of vitamin C and the severity of the pathological consequences of its deficiency somehow explain the evolutive conservation of its biosynthesis within the great part of the mammalian class, as well as in many vertebrate animals [19]. However, this ancestral function has been lost during the evolution in humans, anthropoid primates, guinea pigs, and some species of monkeys and bats [20,21]. Albert Lehninger between the 1950s and 1960s was the first scientist to indicate that human cells are not able to perform the last reaction of vitamin C biosynthesis, i.e., the conversion of L-gulono-γ-lactone into ascorbic acid, which is catalyzed by the enzyme L-gulono-γ-lactone (GULO) oxidase [21,22,23]. It was only in 1991 that Nishikimi and colleagues demonstrated that the gene encoding for GULO is still present in humans but is not active due to the accumulation of a number of mutations that eventually turned it into a non-functional pseudogene [24,25]. Biochemists are continuing to investigate the exact reasons that led to the propagation of this inborn genetic flaw, namely the loss of a gene coding for an essential compound, during the evolution from a primate ancestor to humans. Although several mechanisms were proposed, the primary argument supporting the paradox that mammalian species with the loss-of-function mutations of the GULO gene were not under selective pressure is that all these species have diets that provide a high amount of vitamin C; therefore, the loss of their GULO gene did not cause any evolutive disadvantage [20,26,27,28]. This explanation is in agreement with the fact that wild anthropoid primates consume a considerably larger quantity of vitamin C per body weight compared to the human recommended daily amount for vitamin C (65 to 90 mg/day) [29]: dietary intake of vitamin C reported for gorillas (Gorilla gorilla) is 20–30 mg/kg/day, for spider monkeys (Ateles geoffroyi) is 106 mg/kg/day, and for howler monkeys (Alouatta palliata) is 88 mg/kg/day; similar considerations are valid for bats, with Artibeus jamaicensis consuming 258 mg/kg/day [20,28].
Based on the Third National Health and Nutrition Examination Survey (NHANES III, 1988–1994), the percentage of US males with vitamin C deficiency (less than 11.4 µmol/L in serum) was found to be greater compared to females, reaching a peak of 17% among 25- to 64-year-old subjects [30]. The more recent 2003–2004 NHANES revealed the one vitamin C status improved in the US population, and vitamin C deficiency was significantly lower than that observed during NHANES III; indeed, the overall prevalence of age-adjusted vitamin C deficiency was 7.1 ± 0.9% [31]. Yet, various studies have evidenced low vitamin C levels in both adults and children living in low-income countries [32,33,34,35]. In India, vitamin C deficiency has been relatively well characterized by large population-based studies of >5600 adults aged over 60, in which a marked deficiency was observed in 74% of adults living in north India and 46% of adults living in south India [32,36].
3. Pharmacokinetics and Bioavailability of Vitamin C
Vitamin C is a lactone (C6H8O6) and can exist both in a reduced and in an oxidized form: L-ascorbic acid (reduced form) and dehydro-L-ascorbic acid (oxidized form), as shown in Figure 1. Its hydroxyl groups are located at positions 2 and 3 ionize with pK values of 4.17 and 11.57. Although both forms are biologically active [37,38], in most body fluids, reduced vitamin C is mainly present as an ascorbate anion [39,40,41]. Due to its size and charge, ascorbate does not readily permeate the lipid bilayer [42,43,44]. The majority of intestinal uptake, tissue distribution, and renal reuptake is mediated by the Na+-dependent vitamin C transporters (SVCT1 and SCVT2), which co-transports Na+ and ascorbate across membranes: SVCT1 is widely distributed, while SVCT2 is the main isoform in the adrenal gland and in the eye [45,46,47,48,49,50,51,52,53,54,55].
Ingested vitamin C is mostly absorbed across the intestinal epithelium by membrane transporters in the apical brush border membrane, either as ascorbate via the SVCT transporters or as dehydroascorbic acid through facilitated diffusion via GLUT1 or GLUT3 transporters [56,57,58]; once inside the cell, dehydroascorbic acid is then converted to ascorbate or transported to the bloodstream by GLUT1 and GLUT2 in the basolateral membrane. Specifically, SVCT1 is mainly located on the apical membrane of enterocytes whereas SVCT2 is expressed at the basolateral surface [59,60,61,62,63,64]. SVCT1 is also present in the epithelium of the proximal renal tubuli [50], where it orchestrates the active reabsorption of ascorbate in the kidneys. A murine model lacking SVCT1 exhibited a significantly increased (18-fold) renal fractional excretion, though intestinal absorption was not reduced [65], indicating that the renal SVCT1-mediated reabsorption of vitamin C is crucial in determining its systemic homeostasis.
The non-linear pharmacokinetics and the unique compartmentalization of vitamin C at physiological levels [50,66,67,68,69] can be mostly attributed to the differences between organs in expression, concentration dependency, and substrate affinity of the SVCT and GLUT transporters [49,57,60,61,62,70,71,72]. In contrast to oral administration, parenteral administration of vitamin C bypasses the saturable transport mechanism that governs its intestinal absorption [73,74]. However, intravenous administration of vitamin C is an impractical mode of administration and carries risks of discomfort, infection, and phlebitis. Hence, alternative modes of effective vitamin C delivery have been proposed, with the ultimate goal of improving its bioavailability. In this regard, oral consumption of vitamin C encapsulated in liposomes may hold promise. Liposomes consist of single or multiple concentric membrane-like phospholipid bilayers encapsulating an aqueous compartment [75,76,77,78]. The size of these lipid vesicles can range from a few nanometers to several micrometers; liposomes specifically applied to medical use range between 50 and 450 nm [78,79,80,81]. Liposomes seem to be an ideal drug-carrier system, since their morphology is similar to that of cellular membranes and because of their ability to incorporate various substances, including hydrophilic molecules [82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100]. Accordingly, several studies have indicated that liposomes are very useful for delivering vitamin C [99,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115]. For instance, Davis and coworkers evaluated plasma levels of oral, intravenous, and liposomal vitamin C, demonstrating that liposomal vitamin C has an enhanced bioavailability compared to non-liposomal vitamin C, while avoiding the risks associated with intravenous administration [116]. Another recent study has demonstrated that liposomal vitamin C increases the concentration of vitamin C in the blood by almost doubling the concentration obtainable via the non-liposomal form [117]. These results imply that liposomes might be an excellent carrier for vitamin C to achieve high blood levels.
4. Cardiovascular Effects of Vitamin C: Pre-Clinical Evidence
Severe vitamin C deficiency leads to a well-established disease, known as scurvy, a pathological condition characterized by bleeding, poor wound healing, hair and tooth loss, joint pain, and bone fragility [4]. Albeit scurvy is a fatal disease if not promptly treated, in several clinical studies, low levels of vitamin C (assessed by dietary intake or plasma analysis) have been associated with a number of conditions, including high blood pressure (BP), endothelial dysfunction, heart disease, atherosclerosis, and stroke [118,119,120,121]. Several pre-clinical studies investigated the role of vitamin C in cardiac and vascular protection and in the amelioration of pathological conditions. In 1999, Heller and collaborators demonstrated that ascorbic acid potentiates nitric oxide (NO) synthesis in cultured human endothelial cells, a mechanism that can preserve vessels from altered myogenic tone (vasoconstriction), atherosclerosis, and coagulation abnormalities [122]. Huang et al., in 2000, reported similar effects on the endothelium-derived NO synthase (eNOS) bioactivity, through the increase of the intracellular tetrahydrobiopterin content in porcine aortic endothelial cells [123]. These results were then confirmed by Baker et al., who reported a significant enhancement of eNOS enzymatic activity in human umbilical vein endothelial cells (HUVECs) treated with vitamin C, following the increase of the eNOS cofactor tetrahydrobiopterin [124].
Similar protective effects of vitamin C on vascular endothelial functions were reported in 2002 by d’Uscio et al., who observed that supplementation with ascorbate increases tetrahydrobiopterin and eNOS activity in the aortas of apoE-deficient and control mice [125]. Further evidence of the endothelial protection derived by vitamin C and tetrahydrobiopterin was provided later by Yan et al., who reported in a rat model that oral co-supplementation of vitamin C with tetrahydrobiopterin and L-arginine significantly increases vascular perfusion after hindlimb ischemia by augmenting eNOS activity and reducing oxidative stress and tissue necrosis [126].
In 2003, Ülker and collaborators reported that incubation of aortas from spontaneously hypertensive rats with different concentrations of vitamin C (10 to 100 μmol/L) improved endothelial function, reduced NAD(P)H oxidase activity, as well as superoxide production, and increased eNOS activity and NO generation to the levels observed in control rat aortas [127].
These observations were corroborated by Ladurner et al., who discovered that ascorbate rapidly activates eNOS in HUVEC and immortalized human endothelial cells, through a dose-dependent increased phosphorylation of eNOS-Ser1177 and concomitant decreased phosphorylation at eNOS-Thr495 [128], a phosphorylation pattern highly indicative of increased eNOS activity [129]. Glutathione in its reduced form (GSH) plays crucial roles in protecting cells from oxidative damage, as well as in maintaining cellular redox homeostasis [130,131]. GSH is essential for the physiological function of vitamin C because it is required in vivo for the reduction of dehydroascorbate in guinea pigs, unable to synthesize ascorbate [132]; moreover, GSH deficiency in adult mice stimulates ascorbate synthesis in the liver [132]. These findings strongly suggest the presence of a metabolic redundancy and overlap in the functions of these two important antioxidants [133].
While optimal levels of plasma vitamin C may be critical for maintaining glutathione in its reduced form, sparing it from depletion [134,135], the increment of the oxidized glutathione (GSSG) in the heart, with the consequent reduction of the GSH/GSSG ratio, could lead to ventricular arrhythmias via mechanisms that include mitochondrial depolarization in cardiomyocytes [136].
Overall, these observations indicate that vitamin C does not exert its antioxidative function only by direct interaction with ROS but also via maintenance of the redox regulation by increasing levels of other cellular radical scavengers.
5. Vitamin C and Cardiac Disease
Various clinical studies have investigated the association between supplementation of vitamin C and the risk of cardiovascular disease (CVD), heart failure (HF), coronary heart disease (CHD), and other major adverse cardiac events (Table 1 and Table 2), often yielding opposite results.
In 1993, Rimm et al. published a cohort study conducted on 39,910 US health professionals free of diagnosed CHD or other metabolic conditions at enrollment, and assessed by dietary questionnaires the intake of vitamin C, vitamin E, and carotene, showing that vitamin C (1162 mg/day) was not associated with a lower risk of CHD during a 4–year follow-up [137]. However, in 2003, a study conducted on 85,118 female nurses, based on a food-frequency questionnaire and using multivariate models to adjust for age, smoking, and other cardiovascular risk factors, indicated that the intake of vitamin C supplements was associated with a significantly lower risk of CHD during 16 years of follow-up [138].
These findings were confirmed in 2004 in a pooled analysis of nine prospective cohort studies, showing that supplementation of vitamin C (≥700 mg/day) was inversely associated with CHD risk during a mean 10–year follow-up [152].
Conversely, in the same year, a prospective (15–year follow-up) cohort study (the Iowa Women’s Health Study Cohort) found a positive association between mortality for CHD and vitamin C supplementation (≥300 mg/day), assessed via food-frequency questionnaires in diabetic postmenopausal women [153].
In 2008, a meta-analysis based on 14 studies, for a total of 374,488 individuals with a median follow-up of ~10 years, concluded that dietary vitamin C has an inverse association with CHD risk, whereas supplement intake of vitamin C has no significant association with CHD risk [154]. Another large prospective cohort study conducted for a median follow-up of 16.5 years found an inverse association between dietary vitamin C intake determined by a food frequency questionnaire and CHD mortality in Japanese women without a history of CVD or cancer [155]. In 2013, a meta-analysis evaluating 15 trials for a total of 188,209 subjects found that vitamin C (in a range from 120 to 1000 mg) in association with vitamin E and beta-carotene had no significant effect on CHD and major cardiovascular events [156].
Taken together, these analyses indicate that the association between vitamin C intake and CHD risk remains controversial, with variable association depending on the source of vitamin C. It is important to emphasize at this point that the relationship between vitamin C intake and the actual vitamin C levels in the blood is not linear, hence it is not appropriate to extrapolate vitamin C levels from food intake questionnaires, and values ascertained via blood analyses are necessary [32,72].
The better accuracy of the quantification of vitamin C levels from blood samples compared to food frequency questionnaires is further confirmed when analyzing the outcomes of the European Investigation into Cancer and Nutrition (EPIC)–Norfolk study, a prospective study investigating the relationship between vitamin C and incident HF in 20,299 healthy adults. After a median follow-up of ~12.8 years, ascorbate was inversely associated with incident cases of HF; specifically, every 20 μmol/L increase in plasma vitamin C concentration was associated with a 9% reduced risk of HF [121,139]. Interestingly, in this study, dietary intake was the primary source of vitamin C as assessed by the food frequency questionnaire; however, the investigators did not find a significant association between the reported consumption of fruit and vegetables and lower risk of HF. Therefore, food questionnaires are inadequate to establish the exact vitamin C levels of an individual, hence it is reasonable to consider blood samples as a more reliable source [32,72].
In 2007, the clinical trial Women Antioxidant Cardiovascular Study tested the effects of vitamin C, alongside beta carotene and vitamin E, on the combined outcome of myocardial infarction, coronary revascularization, or cardiovascular death among 8171 female health professionals aged 40 years or older, with a history of CVD or at least three CVD risk factors, followed up for ~9.4 years; the study found no significant effects of ascorbic acid (500 mg/day) on cardiovascular events [143]. Similarly, the Physicians Health Study II (PHS II), a large trial conducted on 14,641 male subjects, including 754 men (5.1%) with prevalent CVD at randomization, revealed that vitamin C (500 mg/day) for ~8 years of follow-up had no significant effect on cardiovascular mortality [147]. In 2017, a meta-analysis of eight randomized controlled trials with a total of 15,445 participants, found inconsistent or low-quality (downgraded) evidence for a correlation between vitamin C supplementation and major cardiovascular events or cardiovascular mortality [157].
In light of the contradictory outcomes herein discussed, it appears that better quality studies are necessary to examine the effects of vitamin C on cardiovascular endpoints, particularly in participants with different risks of CVD. Furthermore, study participants should be tested to exclude the contribution from singular or multiple micronutrient deficiencies, since vitamin C deficiency is commonly accompanied by other micronutrient deficiencies and associated with other confounding aspects, including poor-quality diet [32,158].
6. Vitamin C and Vascular Disease
We and others have shown that the endothelium plays a crucial role in the pathophysiology of vascular disorders [165,166,167,168,169,170,171,172,173,174,175,176,177]. Over the years, a significant number of clinical studies have investigated the effect of vitamin C on vascular disease, evidencing a promising association linking vitamin C intake, circulating levels of ascorbic acid, and lower risk of hypertension. Forman and coworkers reported data from three large prospective cohorts, namely the Nurses Health Study 1 (n = 88,540 women, median age 49 years), the Nurses Health Study 2 (n = 97,315 women, median age 36 years), and the Health Professionals Follow-up Study (n = 37,375 men, median age 52 years).
The risk of developing hypertension did not substantially change for individuals who had reported an intake upper or equal to 1500 mg/day of vitamin C compared to those with an intake lower than 250 mg/day [178].
However, when the vitamin C plasma concentration was directly measured, three independent cross-sectional studies indicated a significant inverse correlation between the concentrations of ascorbic acid and BP values [119,120,179]. Moran et al. reported that vitamin C plasma concentrations in a group of 168 healthy US citizen were inversely related to systolic BP (SBP) [119]. Myint et al. published their observations based on the EPIC-Norfolk cross-sectional study, showing a strong relationship between plasma vitamin C concentrations and lower clinic BP; after adjusting for confounders, the likelihood of having high BP was 22% lower for subjects in the top quartiles of plasma vitamin C levels compared to the bottom quartiles [120].
Block et al. examined in a cross-sectional analysis the association of plasma ascorbic acid with BP in a group of 242 women (aged 18–21 years), finding that plasma vitamin C was inversely associated with both SBP and diastolic BP (DBP), highlighting how persons in the highest quartile of the plasma ascorbic acid distribution had 4.66 mmHg lower systolic BP than those in the lowest quartile of the distribution [179].
These results are consistent with a meta-analysis of 29 trials for a total of 1407 participants including normotensive and hypertensive subjects, showing that daily supplementation with a range from 60 to 4000 mg of vitamin C (median dose: 500 mg) in hypertensive participants reduced systolic BP by 3.84 mm Hg and DBP by 1.48 mm Hg [159].
In 2015, the Coronary Artery Risk Development in Young Adults (CARDIA), a prospective cohort study collecting data from 2884 young adults initially hypertension free, revealed that higher plasma ascorbic acid can favorably influence BP [149]. A very recent meta-analysis, published in 2020 by Ran et al., selected 11 cross-sectional studies and 7 case-control studies conducted from 1990 to 2017; the authors reported that serum vitamin C levels in the study participants were significantly lower in hypertensive subjects than in normotensive ones; moreover, the authors found a significant reverse relationship between serum vitamin C concentration and both SBP and DBP [162].
In the same year, an independent meta-analysis published by Guan et al. supported the results of Ran’s study: The authors selected 8 randomized controlled trials in which vitamin C, varying from 300 to 1000 mg/day, was supplemented for 4–24 weeks to 614 hypertensive patients; the authors observed a marked reduction in DBP in the subgroup of patients with an age ≥35 years having a vitamin C supplementation ≥500 mg/day for 6 weeks, while a significant reduction of both SBP and DBP was observed in the subgroup of age ≥60 years [163].
Overall, these findings highlight how vitamin C is inversely associated with both SBP and DBP, indicating that people with hypertension could exhibit low serum vitamin C compared to normotensive subjects.
Bruno and colleagues demonstrated that acute vitamin C infusion (3 g i.v. in 5 min) significantly lowers BP in hypertensive patients but not in normotensive subjects; additionally, muscle sympathetic nerve activity was significantly reduced after vitamin C infusion in hypertensive patients but not in healthy subjects [180]. Corroborating these results, Heitzer et al. demonstrated that intra-arterial infusion of vitamin C (18 mg/min) had no significant effect on the forearm blood flow in response to acetylcholine (endothelium-dependent vasodilator) and sodium nitroprusside (endothelium-independent vasodilator) in 10 control subjects; however, in 10 chronic smokers, acetylcholine with the concomitant infusion of vitamin C markedly improved the impaired forearm blood flow responses [181]. Similarly, vitamin C supplementation (1000 mg for 4 weeks) significantly reduced LDL oxidative susceptibility in a group of smokers [182].
However, a subsequent clinical trial conducted on 34 male smokers did not support these observations; in fact, compared to placebo, supplementation of vitamin C (250 mg twice daily for 4 weeks) significantly increased plasma ascorbate concentrations but did not significantly change the levels of circulating oxidized LDL, nor of markers of endothelial activation like sICAM–1, sVCAM–1, and vWF-antigen [183].
In 2003, Salonen et al. published the results of the 6–year ASAP trial, in which slow-release vitamin C (250 mg) in addition to vitamin E (136 IU) were supplemented twice daily in hypercholesterolemic subjects [142]. Ultrasound assays proved that the vitamin C supplementation reduced the slope of the mean carotid artery intima-media thickness progression by 26%, with a significance that was reached in men (33% of reduction) but not in women (14% of reduction) [142]. These findings confirmed the observations previously obtained in the same ASAP trial at a shorter 3–year follow-up [184].
In 2014, two meta-analyses authored by Ashor and collaborators provided interesting findings concerning the link between vitamin C plasma levels and endothelial function, supporting the above-mentioned observations previously made by Heitzer [181] and Salonen [142]. The first meta-analysis, examining 44 randomized clinical trials comprising 1324 participants (964 males and 360 females) with a median age of ~51 years, revealed a significant positive effect of vitamin C supplementation (>500 mg/day) on endothelial function measured by flow-mediated dilation (19 studies) [161]. The action of vitamin C on endothelial function appeared to be dependent on health status, with stronger effects in atherosclerotic and diabetic patients. The second meta-analysis, performed on 22 randomized controlled trials, which included 1909 subjects (1088 males and 821 females) with an age that ranged from 22 to 63.5 (median of 29) years, reported that supplementation of vitamins C (120 to 4000 mg/day), E, A, and β–carotene improved arterial stiffness irrespective of the age group and duration of intervention [161]; notably, antioxidant vitamins were more effective in participants with low baseline plasma concentrations of vitamin C [161].
Recent trials have shown that Vitamin C ameliorates the oxidative imbalance and vascular remodeling induced by different stressors, including reperfusion injury following myocardial infarction [185], hyperoxya [186,187], shear stress [188], prolonged immobilization [189], glucose load [190], and mental stress [191,192]. Vitamin C also increases skeletal muscle blood flow and oxygen consumption via local vasodilation during exercise [193]. Vitamin C has also been shown to significantly attenuate endothelial barrier permeability [194,195,196], an aspect that has major implications in infectious disorders [197,198,199,200], which are also known to cause a systemic surge in oxidative stress [201,202,203].
Therefore, the antioxidant roles of Vitamin C and its protective effects on endothelial permeability could come into effect especially during infective processes [204,205,206,207]. Vitamin C has also been shown to improve the effects of other agents in a synergistic manner: for instance, when added to metformin, Vitamin C reduces cardiovascular diabetic complications [208], when added to glucagon-like peptide 1 (GLP–1), it further ameliorates endothelial function and reduces oxidative stress in Type 1 diabetic patients [209].
Thus, it is possible that the association of Vitamin C with other nutrients and micronutrients playing akin beneficial actions could be harnessed [210]. For instance, the supplementation of L-Arginine has been shown to play a favorable role in the regulation of immune responses [211,212]. Similarly, both Vitamin C and L-Arginine are known to improve endothelial function and reduce vascular permeability during infectious disorders [213,214,215,216]. Consequently, it is possible to speculate that their association could be synergistic in tackling infectious diseases; for instance, as COVID–19 is causing endotheliopathy [169], the association of oral L-arginine and liposomal vitamin C (e.g., Bioarginina® C, 2 vials/day) could be efficacious for COVID–19 and other infectious disorders.
Several studies have assessed the association between Vitamin C and the potential protection from cerebrovascular disease, and the results have been subject of much controversy, similarly to what observed in the investigations assessing CHD. A prospective cohort study that followed for 20 years the residents of a rural Japanese community, having an age of 40 years or older and initially free of stroke diagnosis, has shown that higher serum Vitamin C concentration was associated with a reduced risk of incidence of both hemorrhagic and ischemic stroke [217]. Only a small part of these associations could be explained by lowering BP and adjusting for the physical activity level [217]. Similarly, in 20,649 adults followed for 10 years in the prospective cohort study EPIC-Norfolk, plasma ascorbate concentrations in the top quartile were linked to a 42% lower risk of stroke compared to the values in the lowest quartile [140].
Of note, in both the EPIC-Norfolk [140] and Japanese [217] populations, blood Vitamin C concentrations were positively correlated with vegetable and fruit intake. In 2011 Del Rio and colleagues investigated the relationship between dietary total antioxidant capacity and the risk of hemorrhagic and ischemic stroke in 41,620 subjects not previously diagnosed with myocardial infarction or stroke, recruited from the Italian segment of the European Prospective Investigation into Cancer and Nutrition (EPIC) study; the results from specific sub-analyses on the different stroke types indicate that Vitamin C is associated with a decreased risk of ischemic stroke [151]. These studies were consistent with a meta-analysis published in 2013, in which 16 prospective studies reported a 19% lower risk of stroke (pooled analysis of 2 studies) when comparing the highest vs. the lowest dietary Vitamin C intake, and a 38% lower risk of stroke (pooled analysis of 6 studies) when comparing the highest vs. the lowest circulating Vitamin C concentration [160].
On the other hand, Sesso and collaborators reported the results of a randomized double-blind placebo-controlled trial conducted in 14,641 healthy US male physicians, enrolled in the PHS II study at ≥50 years of age, showing that Vitamin C supplementation (500 mg/day) had no significant effect on the mortality from, or the incidence of, any type of stroke after a mean follow-up of ~8 years [156]. In agreement with these observations, Ye and collaborators published a meta-analysis study of 15 trials for a total of 188,209 participants, reporting that the supplementation of Vitamin C (in a range from 120 to 1000 mg) in association with Vitamin E and beta-carotene, had no significant effects on the risk of stroke compared to placebo [156].
7. Conclusions
Both preclinical and clinical data available in the literature show that Vitamin C plays a pivotal role in a number of processes involved in the pathogenesis of CVD. Nevertheless, major limitations have to be taken in consideration when interpreting the results of the studies investigating the effects of Vitamin C on human health; for instance, dietary assessment methods such as questionnaires or food diaries lack precision and accuracy and do not embrace other conditions that can affect Vitamin C levels and homeostasis [35,218,219,220,221,222]; therefore, these approaches are inadequate to ascertain the accurate Vitamin C status of an individual. Henceforth, it is reasonable to consider blood samples as more reliable indicators. Equally important, plasma Vitamin C level may considerably fluctuate following food or supplement ingestion. Consequently, the most reliable and practically available information on Vitamin C status can only be obtained from blood samples withdrawn in fasted conditions [32,72]. Ascorbate is rapidly oxidized ex vivo and the resulting oxidation products are quickly metabolized or degraded [38], hence, in order to obtain valid and consistent Vitamin C concentrations, a scrupulous sample handling is essential. Furthermore, the use of liposomal Vitamin C should be preferred to other forms since liposomes might be an excellent carrier for Vitamin C to achieve high blood levels.
Therefore, further studies are needed to clarify whether Vitamin C supplementation is actually effective in the prevention or cure of CVD. Specifically, prospective randomized clinical trials in large populations are needed to better define the best dose, the ideal administration route, the optimal targets, as well as the contribution of dietary supplementation of other antioxidant elements; in order to have standardized and reproducible data, it will be important to evaluate the Vitamin C status using blood samples obtained from fasted individuals.
Author Contributions
Data curation, writing—original draft preparation, M.B.M., J.G., V.C., and G.S.; writing—review and editing, M.B.M., J.G., V.T., and G.S.; supervision, G.S.; funding acquisition, G.S. and J.G. All authors have read and agreed to the published version of the manuscript.
Funding
The Santulli’s lab is supported in part by the NIH (R01–DK123259, R01–HL146691, R01–DK033823, R00–DK107895, R56–AG066431 to G.S.) and by the American Heart Association (AHA–20POST35211151 to J.G.).
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the paper.
References
- Kyle:, R.A.; Shampo, M.A. Albert Szent-Gyorgy—Nobel laureate. Mayo Clin. Proc. 2000, 75, 722. [Google Scholar] [CrossRef]
- Szent-Gyorgyi, A. The Identification of Vitamin C. Science 1938, 87, 214–215. [Google Scholar] [CrossRef] [PubMed]
- Zilva, S.S. The Antiscorbutic Fraction of Lemon Juice. I. Biochem. J. 1924, 18, 182–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, K.J. The discovery of vitamin C. Ann. Nutr. Metab. 2012, 61, 259–264. [Google Scholar] [CrossRef]
- De Tullio, M.C. Beyond the antioxidant: The double life of vitamin C. Subcell. Biochem. 2012, 56, 49–65. [Google Scholar]
- Frei, B.; England, L.; Ames, B.N. Ascorbate is an outstanding antioxidant in human blood plasma. Proc. Natl. Acad. Sci. USA 1989, 86, 6377–6381. [Google Scholar] [CrossRef] [Green Version]
- Frei, B.; Stocker, R.; England, L.; Ames, B.N. Ascorbate: The most effective antioxidant in human blood plasma. Adv. Exp. Med. Biol. 1990, 264, 155–163. [Google Scholar]
- Wyckelsma, V.L.; Venckunas, T.; Brazaitis, M.; Gastaldello, S.; Snieckus, A.; Eimantas, N.; Baranauskiene, N.; Subocius, A.; Skurvydas, A.; Paasuke, M.; et al. Vitamin C and E Treatment Blunts Sprint Interval Training-Induced Changes in Inflammatory Mediator-, Calcium-, and Mitochondria-Related Signaling in Recreationally Active Elderly Humans. Antioxidants 2020, 9, 879. [Google Scholar] [CrossRef]
- Jacob, R.A.; Sotoudeh, G. Vitamin C function and status in chronic disease. Nutr. Clin. Care 2002, 5, 66–74. [Google Scholar] [CrossRef]
- Van den Berg, J.J.; Kuypers, F.A.; Roelofsen, B.; den Kamp, J.A.O. The cooperative action of vitamins E and C in the protection against peroxidation of parinaric acid in human erythrocyte membranes. Chem. Phys. Lipids 1990, 53, 309–320. [Google Scholar] [CrossRef]
- Johnston, C.S.; Meyer, C.G.; Srilakshmi, J.C. Vitamin C elevates red blood cell glutathione in healthy adults. Am. J. Clin. Nutr. 1993, 58, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Englard, S.; Seifter, S. The biochemical functions of ascorbic acid. Annu. Rev. Nutr. 1986, 6, 365–406. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Schellhorn, H.E. New developments and novel therapeutic perspectives for vitamin C. J. Nutr. 2007, 137, 2171–2184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, A.C.; Frei, B. Toward a new recommended dietary allowance for vitamin C based on antioxidant and health effects in humans. Am. J. Clin. Nutr. 1999, 69, 1086–1107. [Google Scholar] [CrossRef] [Green Version]
- Warner, M.J.; Kamran, M.T. Anemia, Iron Deficiency; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Sourabh, S.; Bhatia, P.; Jain, R. Favourable improvement in haematological parameters in response to oral iron and vitamin C combination in children with Iron Refractory Iron Deficiency Anemia (IRIDA) phenotype. Blood Cells Mol. Dis. 2019, 75, 26–29. [Google Scholar] [CrossRef]
- Hunt, J.R.; Gallagher, S.K.; Johnson, L.K. Effect of ascorbic acid on apparent iron absorption by women with low iron stores. Am. J. Clin. Nutr. 1994, 59, 1381–1385. [Google Scholar] [CrossRef]
- Davidsson, L.; Galan, P.; Kastenmayer, P.; Cherouvrier, F.; Juillerat, M.A.; Hercberg, S.; Hurrell, R.F. Iron bioavailability studied in infants: The influence of phytic acid and ascorbic acid in infant formulas based on soy isolate. Pediatr. Res. 1994, 36, 816–822. [Google Scholar] [CrossRef] [Green Version]
- Linster, C.L.; Van Schaftingen, E. Vitamin C. Biosynthesis, recycling and degradation in mammals. FEBS J. 2007, 274, 1–22. [Google Scholar] [CrossRef]
- Drouin, G.; Godin, J.R.; Page, B. The genetics of vitamin C loss in vertebrates. Curr. Genom. 2011, 12, 371–378. [Google Scholar] [CrossRef]
- Grollman, A.P.; Lehninger, A.L. Enzymic synthesis of L-ascorbic acid in different animal species. Arch. Biochem. Biophys. 1957, 69, 458–467. [Google Scholar] [CrossRef]
- Bublitz, C.; Lehninger, A.L. The enzymic conversion of L-gulonate to L-as-corbate by rat-liver enzymes. Biochim. Biophys. Acta 1959, 32, 290–291. [Google Scholar] [CrossRef]
- Chatterjee, I.B.; Chatterjee, G.C.; Ghosh, N.C.; Ghosh, J.J.; Guha, B.C. Biological synthesis of L-ascorbic acid in animal tissues: Conversion of L-gulonolactone into L-ascorbic acid. Biochem. J. 1960, 74, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikimi, M.; Yagi, K. Molecular basis for the deficiency in humans of gulonolactone oxidase, a key enzyme for ascorbic acid biosynthesis. Am. J. Clin. Nutr. 1991, 54, 1203S–1208S. [Google Scholar] [CrossRef] [PubMed]
- Nishikimi, M.; Kawai, T.; Yagi, K. Guinea pigs possess a highly mutated gene for L-gulono-gamma-lactone oxidase, the key enzyme for L-ascorbic acid biosynthesis missing in this species. J. Biol. Chem. 1992, 267, 21967–21972. [Google Scholar]
- Pollock, J.I.; Mullin, R.J. Vitamin C biosynthesis in prosimians: Evidence for the anthropoid affinity of Tarsius. Am. J. Phys. Anthropol. 1987, 73, 65–70. [Google Scholar] [CrossRef]
- Birney, E.C.; Jenness, R.; Ayaz, K.M. Inability of bats to synthesise L-ascorbic acid. Nature 1976, 260, 626–628. [Google Scholar] [CrossRef]
- Milton, K.; Jenness, R. Ascorbic acid content of neotropical plant parts available to wild monkeys and bats. Experientia 1987, 43, 339–342. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Hampl, J.S.; Taylor, C.A.; Johnston, C.S. Vitamin C deficiency and depletion in the United States: The Third National Health and Nutrition Examination Survey, 1988 to 1994. Am. J. Public Health 2004, 94, 870–875. [Google Scholar] [CrossRef]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003–2004 National Health and Nutrition Examination Survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef]
- Rowe, S.; Carr, A.C. Global Vitamin C Status and Prevalence of Deficiency: A Cause for Concern? Nutrients 2020, 12, 2008. [Google Scholar] [CrossRef]
- Villalpando, S.; Montalvo-Velarde, I.; Zambrano, N.; Garcia-Guerra, A.; Ramirez-Silva, C.I.; Shamah-Levy, T.; Rivera, J.A. Vitamins A, and C and folate status in Mexican children under 12 years and women 12–49 years: A probabilistic national survey. Salud Publica Mex 2003, 45, S508–S519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, O.P.; Ronquillo, D.; Mdel, C.C.; Camacho, M.; Long, K.Z.; Rosado, J.L. Zinc, vitamin A, and vitamin C status are associated with leptin concentrations and obesity in Mexican women: Results from a cross-sectional study. Nutr. Metab. 2012, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahill, L.; Corey, P.N.; El-Sohemy, A. Vitamin C deficiency in a population of young Canadian adults. Am. J. Epidemiol. 2009, 170, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, R.D.; Vashist, P.; Gupta, S.K.; Young, I.S.; Maraini, G.; Camparini, M.; Jayanthi, R.; John, N.; Fitzpatrick, K.E.; Chakravarthy, U.; et al. Inverse association of vitamin C with cataract in older people in India. Ophthalmology 2011, 118, 1958–1965.e2. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, Y.; Kurata, T. Interconversion between dehydro-L-ascorbic acid and L-ascorbic acid. Biosci. Biotechnol. Biochem. 2000, 64, 476–483. [Google Scholar] [CrossRef]
- Dewhirst, R.A.; Fry, S.C. The oxidation of dehydroascorbic acid and 2,3-diketogulonate by distinct reactive oxygen species. Biochem. J. 2018, 475, 3451–3470. [Google Scholar] [CrossRef] [Green Version]
- Sauberlich, H.E. Pharmacology of vitamin C. Annu. Rev. Nutr. 1994, 14, 371–391. [Google Scholar] [CrossRef]
- Arrigoni, O.; De Tullio, M.C. Ascorbic acid: Much more than just an antioxidant. Biochim. Biophys. Acta 2002, 1569, 1–9. [Google Scholar] [CrossRef]
- Pauling, L. Ascorbic acid. Lancet 1979, 1, 615. [Google Scholar] [CrossRef]
- Przybylo, M.; Langner, M. On the physiological and cellular homeostasis of ascorbate. Cell Mol. Biol. Lett. 2020, 25, 32. [Google Scholar] [CrossRef]
- Rose, R.C. Solubility properties of reduced and oxidized ascorbate as determinants of membrane permeation. Biochim. Biophys. Acta 1987, 924, 254–256. [Google Scholar] [CrossRef]
- Zhitkovich, A. Nuclear and Cytoplasmic Functions of Vitamin C. Chem. Res. Toxicol. 2020, 33, 2515–2526. [Google Scholar] [CrossRef] [PubMed]
- Tsukaguchi, H.; Tokui, T.; Mackenzie, B.; Berger, U.V.; Chen, X.Z.; Wang, Y.; Brubaker, R.F.; Hediger, M.A. A family of mammalian Na+-dependent L-ascorbic acid transporters. Nature 1999, 399, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Sotiriou, S.; Gispert, S.; Cheng, J.; Wang, Y.; Chen, A.; Hoogstraten-Miller, S.; Miller, G.F.; Kwon, O.; Levine, M.; Guttentag, S.H.; et al. Ascorbic-acid transporter Slc23a1 is essential for vitamin C transport into the brain and for perinatal survival. Nat. Med. 2002, 8, 514–517. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.S.; Srinivasan, P.; Wildman, A.J.; Marchant, J.S.; Said, H.M. Molecular mechanism(s) involved in differential expression of vitamin C transporters along the intestinal tract. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G340–G347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macias, R.I.; Hierro, C.; de Juan, S.C.; Jimenez, F.; Martin, F.G.-S.; Marin, J.J. Hepatic expression of sodium-dependent vitamin C transporters: Ontogeny, subtissular distribution and effect of chronic liver diseases. Br. J. Nutr. 2011, 106, 1814–1825. [Google Scholar] [CrossRef] [Green Version]
- Larsson, N.; Rankin, G.D.; Bicer, E.M.; Roos-Engstrand, E.; Pourazar, J.; Blomberg, A.; Mudway, I.S.; Behndig, A.F. Identification of vitamin C transporters in the human airways: A cross-sectional in vivo study. BMJ Open 2015, 5, e006979. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Mackenzie, B.; Tsukaguchi, H.; Weremowicz, S.; Morton, C.C.; Hediger, M.A. Human vitamin C (L-ascorbic acid) transporter SVCT1. Biochem. Biophys. Res. Commun. 2000, 267, 488–494. [Google Scholar] [CrossRef]
- Santulli, G. Adrenal Glands: From Pathophysiology to Clinical Evidence; Nova Science Publishers, Inc.: Hauppauge, NY, USA, 2015. [Google Scholar]
- Portugal, C.C.; Socodato, R.; Canedo, T.; Silva, C.M.; Martins, T.; Coreixas, V.S.; Loiola, E.C.; Gess, B.; Rohr, D.; Santiago, A.R.; et al. Caveolin-1-mediated internalization of the vitamin C transporter SVCT2 in microglia triggers an inflammatory phenotype. Sci. Signal. 2017, 10. [Google Scholar] [CrossRef] [Green Version]
- Ludke, A.R.; Sharma, A.K.; Akolkar, G.; Bajpai, G.; Singal, P.K. Downregulation of vitamin C transporter SVCT-2 in doxorubicin-induced cardiomyocyte injury. Am. J. Physiol. Cell Physiol. 2012, 303, C645–C653. [Google Scholar] [CrossRef] [Green Version]
- Portugal, C.C.; da Encarnacao, T.G.; Socodato, R.; Moreira, S.R.; Brudzewsky, D.; Ambrosio, A.F.; Paes-de-Carvalho, R. Nitric oxide modulates sodium vitamin C transporter 2 (SVCT-2) protein expression via protein kinase G (PKG) and nuclear factor-kappaB (NF-kappaB). J. Biol. Chem. 2012, 287, 3860–3872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.; Chae, J.S.; Shin, H.; Shin, Y.; Song, H.; Kim, Y.; Yoo, B.C.; Roh, K.; Cho, S.; Kil, E.J.; et al. Hormetic dose response to L-ascorbic acid as an anti-cancer drug in colorectal cancer cell lines according to SVCT-2 expression. Sci. Rep. 2018, 8, 11372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malo, C.; Wilson, J.X. Glucose modulates vitamin C transport in adult human small intestinal brush border membrane vesicles. J. Nutr. 2000, 130, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nualart, F.; Mack, L.; Garcia, A.; Cisternas, P.; Bongarzone, E.R.; Heitzer, M.; Jara, N.; Martinez, F.; Ferrada, L.; Espinoza, F.; et al. Vitamin C Transporters, Recycling and the Bystander Effect in the Nervous System: SVCT2 versus Gluts. J. Stem. Cell Res. Ther. 2014, 4, 209. [Google Scholar] [CrossRef] [Green Version]
- Vera, J.C.; Rivas, C.I.; Fischbarg, J.; Golde, D.W. Mammalian facilitative hexose transporters mediate the transport of dehydroascorbic acid. Nature 1993, 364, 79–82. [Google Scholar] [CrossRef]
- Corpe, C.P.; Eck, P.; Wang, J.; Al-Hasani, H.; Levine, M. Intestinal dehydroascorbic acid (DHA) transport mediated by the facilitative sugar transporters, GLUT2 and GLUT8. J. Biol. Chem. 2013, 288, 9092–9101. [Google Scholar] [CrossRef] [Green Version]
- Dong, W.; Tian, C.; Jiao, Y.; Blackwell, S.; Lou, G.; Postlethwaite, A.; Gu, W.; Sun, D. Multiple genome analyses reveal key genes in Vitamin C and Vitamin D synthesis and transport pathways are shared. Sci. Rep. 2019, 9, 16811. [Google Scholar] [CrossRef]
- Lukawski, M.; Dalek, P.; Witkiewicz, W.; Przybylo, M.; Langner, M. Experimental evidence and physiological significance of the ascorbate passive diffusion through the lipid bilayer. Chem. Phys. Lipids 2020, 232, 104950. [Google Scholar] [CrossRef]
- Pozzer, D.; Invernizzi, R.W.; Blaauw, B.; Cantoni, O.; Zito, E. Ascorbic Acid Route to the Endoplasmic Reticulum: Function and Role in Disease. Antioxid. Redox Signal. 2020. [Google Scholar] [CrossRef]
- Nygaard, G. On a Novel, Simplified Model Framework Describing Ascorbic Acid Concentration Dynamics. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2019, 2019, 2880–2886. [Google Scholar]
- Bozonet, S.M.; Carr, A.C. The Role of Physiological Vitamin C Concentrations on Key Functions of Neutrophils Isolated from Healthy Individuals. Nutrients 2019, 11, 1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corpe, C.P.; Tu, H.; Eck, P.; Wang, J.; Faulhaber-Walter, R.; Schnermann, J.; Margolis, S.; Padayatty, S.; Sun, H.; Wang, Y.; et al. Vitamin C transporter Slc23a1 links renal reabsorption, vitamin C tissue accumulation, and perinatal survival in mice. J. Clin. Investig. 2010, 120, 1069–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, M.; Padayatty, S.J.; Espey, M.G. Vitamin C: A concentration-function approach yields pharmacology and therapeutic discoveries. Adv. Nutr. 2011, 2, 78–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, M.; Conry-Cantilena, C.; Wang, Y.; Welch, R.W.; Washko, P.W.; Dhariwal, K.R.; Park, J.B.; Lazarev, A.; Graumlich, J.F.; King, J.; et al. Vitamin C pharmacokinetics in healthy volunteers: Evidence for a recommended dietary allowance. Proc. Natl. Acad. Sci. USA 1996, 93, 3704–3709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padayatty, S.J.; Sun, H.; Wang, Y.; Riordan, H.D.; Hewitt, S.M.; Katz, A.; Wesley, R.A.; Levine, M. Vitamin C pharmacokinetics: Implications for oral and intravenous use. Ann. Intern. Med. 2004, 140, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, B.; Illing, A.C.; Hediger, M.A. Transport model of the human Na+-coupled L-ascorbic acid (vitamin C) transporter SVCT1. Am. J. Physiol. Cell Physiol. 2008, 294, C451–C459. [Google Scholar] [CrossRef] [PubMed]
- Wohlrab, C.; Phillips, E.; Dachs, G.U. Vitamin C Transporters in Cancer: Current Understanding and Gaps in Knowledge. Front. Oncol. 2017, 7, 74. [Google Scholar] [CrossRef] [Green Version]
- Roa, F.J.; Pena, E.; Inostroza, E.; Sotomayor, K.; Gonzalez, M.; Gutierrez-Castro, F.A.; Maurin, M.; Sweet, K.; Labrousse, C.; Gatica, M.; et al. Data on SVCT2 transporter expression and localization in cancer cell lines and tissues. Data Br. 2019, 25, 103972. [Google Scholar] [CrossRef]
- Lykkesfeldt, J. On the effect of vitamin C intake on human health: How to (mis)interprete the clinical evidence. Redox Biol. 2020, 34, 101532. [Google Scholar] [CrossRef]
- Wilson, J.X. Regulation of vitamin C transport. Annu. Rev. Nutr. 2005, 25, 105–125. [Google Scholar] [CrossRef]
- Stephenson, C.M.; Levin, R.D.; Spector, T.; Lis, C.G. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemother. Pharmacol. 2013, 72, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangham, A.D.; Horne, R.W. Negative Staining of Phospholipids and Their Structural Modification by Surface-Active Agents as Observed in the Electron Microscope. J. Mol. Biol. 1964, 8, 660–668. [Google Scholar] [CrossRef]
- Yao, X.; Fan, X.; Yan, N. Cryo-EM analysis of a membrane protein embedded in the liposome. Proc. Natl. Acad. Sci. USA 2020, 117, 18497–18503. [Google Scholar] [CrossRef] [PubMed]
- Deamer, D.W. From “banghasomes“ to liposomes: A memoir of Alec Bangham, 1921–2010. FASEB J. 2010, 24, 1308–1310. [Google Scholar] [CrossRef] [PubMed]
- Mozafari, M.R. Liposomes: An overview of manufacturing techniques. Cell. Mol. Biol. Lett. 2005, 10, 711–719. [Google Scholar] [PubMed]
- Madni, A.; Sarfraz, M.; Rehman, M.; Ahmad, M.; Akhtar, N.; Ahmad, S.; Tahir, N.; Ijaz, S.; Al-Kassas, R.; Lobenberg, R. Liposomal drug delivery: A versatile platform for challenging clinical applications. J. Pharm. Pharm. Sci. 2014, 17, 401–426. [Google Scholar] [CrossRef] [Green Version]
- Karn, P.R.; Cho, W.; Hwang, S.J. Liposomal drug products and recent advances in the synthesis of supercritical fluid-mediated liposomes. Nanomedicine 2013, 8, 1529–1548. [Google Scholar] [CrossRef]
- Nayerhoda, R.; Hill, A.; Pfeifer, B.A. Liposomal Dual Delivery of Both Polysaccharide and Protein Antigens. Methods Mol. Biol. 2021, 2183, 477–487. [Google Scholar]
- Bozzuto, G.; Molinari, A. Liposomes as nanomedical devices. Int. J. Nanomed. 2015, 10, 975–999. [Google Scholar] [CrossRef] [Green Version]
- Kauffman, K.J.; Dorkin, J.R.; Yang, J.H.; Heartlein, M.W.; DeRosa, F.; Mir, F.F.; Fenton, O.S.; Anderson, D.G. Optimization of Lipid Nanoparticle Formulations for mRNA Delivery in Vivo with Fractional Factorial and Definitive Screening Designs. Nano Lett. 2015, 15, 7300–7306. [Google Scholar] [CrossRef]
- Kamaly, N.; Miller, A.D. Paramagnetic liposome nanoparticles for cellular and tumour imaging. Int. J. Mol. Sci. 2010, 11, 1759–1776. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Shin, Y.; Lee, W.; Whang, K.; Kim, D.; Lee, L.P.; Choi, J.W.; Kang, T. General and programmable synthesis of hybrid liposome/metal nanoparticles. Sci. Adv. 2016, 2, e1601838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.; Liu, C.; Liu, W.; Yu, H.; Zheng, H.; Zhou, W.; Hu, Y. Preparation and characterization of nanoliposomes entrapping medium-chain fatty acids and vitamin C by lyophilization. Int. J. Mol. Sci. 2013, 14, 19763–19773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moribe, K.; Limwikrant, W.; Higashi, K.; Yamamoto, K. Drug nanoparticle formulation using ascorbic Acid derivatives. J. Drug. Deliv. 2011, 2011, 138929. [Google Scholar] [CrossRef] [PubMed]
- Preiss, M.R.; Bothun, G.D. Stimuli-responsive liposome-nanoparticle assemblies. Expert Opin. Drug Deliv. 2011, 8, 1025–1040. [Google Scholar] [CrossRef]
- Ross, C.; Taylor, M.; Fullwood, N.; Allsop, D. Liposome delivery systems for the treatment of Alzheimer’s disease. Int. J. Nanomed. 2018, 13, 8507–8522. [Google Scholar] [CrossRef] [Green Version]
- Ickenstein, L.M.; Garidel, P. Lipid-based nanoparticle formulations for small molecules and RNA drugs. Expert Opin. Drug Deliv. 2019, 16, 1205–1226. [Google Scholar] [CrossRef]
- Seleci, M.; Seleci, D.A.; Scheper, T.; Stahl, F. Theranostic Liposome-Nanoparticle Hybrids for Drug Delivery and Bioimaging. Int. J. Mol. Sci. 2017, 18, 1415. [Google Scholar] [CrossRef] [Green Version]
- Zylberberg, C.; Gaskill, K.; Pasley, S.; Matosevic, S. Engineering liposomal nanoparticles for targeted gene therapy. Gene Ther. 2017, 24, 441–452. [Google Scholar] [CrossRef]
- Michel, R.; Gradzielski, M. Experimental aspects of colloidal interactions in mixed systems of liposome and inorganic nanoparticle and their applications. Int. J. Mol. Sci. 2012, 13, 11610–11642. [Google Scholar] [CrossRef] [Green Version]
- Zamani, P.; Momtazi-Borojeni, A.A.; Nik, M.E.; Oskuee, R.K.; Sahebkar, A. Nanoliposomes as the adjuvant delivery systems in cancer immunotherapy. J. Cell. Physiol. 2018, 233, 5189–5199. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.; Compton, R.G. Investigation of single-drug-encapsulating liposomes using the nano-impact method. Angew. Chem. Int. Ed. Engl. 2014, 53, 13928–13930. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Seike, Y.; Saeki, A.; Kozawa, T.; Takeuchi, F.; Tsubaki, M. A pulse radiolysis study of the dynamics of ascorbic acid free radicals within a liposomal environment. ChemPhysChem 2014, 15, 2994–2997. [Google Scholar] [CrossRef] [PubMed]
- Vanaja, K.; Wahl, M.A.; Bukarica, L.; Heinle, H. Liposomes as carriers of the lipid soluble antioxidant resveratrol: Evaluation of amelioration of oxidative stress by additional antioxidant vitamin. Life Sci. 2013, 93, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Song, W.; Shen, L.; Qiu, N.; Hu, M.; Liu, Y.; Liu, Q.; Huang, L. Vasodilator Hydralazine Promotes Nanoparticle Penetration in Advanced Desmoplastic Tumors. ACS Nano 2019, 13, 1751–1763. [Google Scholar] [CrossRef] [PubMed]
- Attia, M.; Essa, E.A.; Zaki, R.M.; Elkordy, A.A. An Overview of the Antioxidant Effects of Ascorbic Acid and Alpha Lipoic Acid (in Liposomal Forms) as Adjuvant in Cancer Treatment. Antioxidants 2020, 9, 359. [Google Scholar] [CrossRef] [PubMed]
- Felice, B.; Prabhakaran, M.P.; Rodriguez, A.P.; Ramakrishna, S. Drug delivery vehicles on a nano-engineering perspective. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 41, 178–195. [Google Scholar] [CrossRef]
- Tavano, L.; Muzzalupo, R.; Picci, N.; de Cindio, B. Co-encapsulation of antioxidants into niosomal carriers: Gastrointestinal release studies for nutraceutical applications. Colloids Surf. B Biointerfaces 2014, 114, 82–88. [Google Scholar] [CrossRef]
- Castro, R.A.; Silva-Barcellos, N.M.; Licio, C.S.; Souza, J.B.; Souza-Testasicca, M.C.; Ferreira, F.M.; Batista, M.A.; Silveira-Lemos, D.; Moura, S.L.; Frezard, F.; et al. Association of liposome-encapsulated trivalent antimonial with ascorbic acid: An effective and safe strategy in the treatment of experimental visceral leishmaniasis. PLoS ONE 2014, 9, e104055. [Google Scholar] [CrossRef]
- Prantl, L.; Eigenberger, A.; Gehmert, S.; Haerteis, S.; Aung, T.; Rachel, R.; Jung, E.M.; Felthaus, O. Enhanced Resorption of Liposomal Packed Vitamin C Monitored by Ultrasound. J. Clin. Med. 2020, 9, 1616. [Google Scholar] [CrossRef]
- Liu, N.; Park, H.J. Factors effect on the loading efficiency of Vitamin C loaded chitosan-coated nanoliposomes. Colloids Surf. B Biointerfaces 2010, 76, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, P.; Zou, Y.X.; Luo, Z.G.; Tamer, T.M. Co-encapsulation of Vitamin C and beta-Carotene in liposomes: Storage stability, antioxidant activity, and in vitro gastrointestinal digestion. Food Res. Int. 2020, 136, 109587. [Google Scholar] [CrossRef] [PubMed]
- Khalili, A.; Alipour, S.; Fathalipour, M.; Purkhosrow, A.; Mashghoolozekr, E.; Bayat, G.; Nekooeian, A.A. Liposomal and Non-Liposomal Formulations of Vitamin C: Comparison of the Antihypertensive and Vascular Modifying Activity in Renovascular Hypertensive Rats. Iran. J. Med. Sci. 2020, 45, 41–49. [Google Scholar]
- Carita, A.C.; Fonseca-Santos, B.; Shultz, J.D.; Michniak-Kohn, B.; Chorilli, M.; Leonardi, G.R. Vitamin C: One compound, several uses. Advances for delivery, efficiency and stability. Nanomedicine 2020, 24, 102117. [Google Scholar] [CrossRef] [PubMed]
- Lukawski, M.; Dalek, P.; Borowik, T.; Forys, A.; Langner, M.; Witkiewicz, W.; Przybylo, M. New oral liposomal vitamin C formulation: Properties and bioavailability. J. Liposome Res. 2020, 30, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Maione-Silva, L.; de Castro, E.G.; Nascimento, T.L.; Cintra, E.R.; Moreira, L.C.; Cintra, B.A.S.; Valadares, M.C.; Lima, E.M. Ascorbic acid encapsulated into negatively charged liposomes exhibits increased skin permeation, retention and enhances collagen synthesis by fibroblasts. Sci. Rep. 2019, 9, 522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, W.; Fu, Q.; Zhao, Y.; Zhang, L.; Yue, Q.; Hai, L.; Guo, L.; Wu, Y. Ascorbic acid-modified brain-specific liposomes drug delivery system with “lock-in” function. Chem. Phys. Lipids 2019, 224, 104727. [Google Scholar] [CrossRef] [PubMed]
- Parhizkar, E.; Rashedinia, M.; Karimi, M.; Alipour, S. Design and development of vitamin C-encapsulated proliposome with improved in-vitro and ex-vivo antioxidant efficacy. J. Microencapsul. 2018, 35, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Jiao, Z.; Wang, X.; Yin, Y.; Xia, J.; Mei, Y. Preparation and evaluation of a chitosan-coated antioxidant liposome containing vitamin C and folic acid. J. Microencapsul. 2018, 35, 272–280. [Google Scholar] [CrossRef]
- Miura, Y.; Fuchigami, Y.; Hagimori, M.; Sato, H.; Ogawa, K.; Munakata, C.; Wada, M.; Maruyama, K.; Kawakami, S. Evaluation of the targeted delivery of 5-fluorouracil and ascorbic acid into the brain with ultrasound-responsive nanobubbles. J. Drug Target 2018, 26, 684–691. [Google Scholar] [CrossRef]
- Tsai, W.C.; Rizvi, S.S.H. Simultaneous microencapsulation of hydrophilic and lipophilic bioactives in liposomes produced by an ecofriendly supercritical fluid process. Food Res. Int. 2017, 99, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Duconge, J.; Miranda-Massari, J.R.; Gonzalez, M.J.; Jackson, J.A.; Warnock, W.; Riordan, N.H. Pharmacokinetics of vitamin C: Insights into the oral and intravenous administration of ascorbate. P. R. Health Sci. J. 2008, 27, 7–19. [Google Scholar] [PubMed]
- Davis, J.L.; Paris, H.L.; Beals, J.W.; Binns, S.E.; Giordano, G.R.; Scalzo, R.L.; Schweder, M.M.; Blair, E.; Bell, C. Liposomal-encapsulated Ascorbic Acid: Influence on Vitamin C Bioavailability and Capacity to Protect Against Ischemia-Reperfusion Injury. Nutr. Metab. Insights 2016, 9, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopi, S.; Balakrishnan, P. Evaluation and Clinical Comparison Studies on Liposomal and Non-Liposomal Ascorbic Acid (Vitamin C) and their Enhanced Bioavailability. J. Liposome Res. 2020, 1–35. [Google Scholar] [CrossRef]
- Ashor, A.W.; Siervo, M.; Lara, J.; Oggioni, C.; Mathers, J.C. Antioxidant vitamin supplementation reduces arterial stiffness in adults: A systematic review and meta-analysis of randomized controlled trials. J. Nutr. 2014, 144, 1594–1602. [Google Scholar] [CrossRef] [Green Version]
- Moran, J.P.; Cohen, L.; Greene, J.M.; Xu, G.; Feldman, E.B.; Hames, C.G.; Feldman, D.S. Plasma ascorbic acid concentrations relate inversely to blood pressure in human subjects. Am. J. Clin. Nutr. 1993, 57, 213–217. [Google Scholar] [CrossRef]
- Myint, P.K.; Luben, R.N.; Wareham, N.J.; Khaw, K.T. Association between plasma vitamin C concentrations and blood pressure in the European prospective investigation into cancer-Norfolk population-based study. Hypertension 2011, 58, 372–379. [Google Scholar] [CrossRef] [Green Version]
- Pfister, R.; Sharp, S.J.; Luben, R.; Wareham, N.J.; Khaw, K.T. Plasma vitamin C predicts incident heart failure in men and women in European Prospective Investigation into Cancer and Nutrition-Norfolk prospective study. Am. Heart J. 2011, 162, 246–253. [Google Scholar] [CrossRef]
- Heller, R.; Munscher-Paulig, F.; Grabner, R.; Till, U. L-Ascorbic acid potentiates nitric oxide synthesis in endothelial cells. J. Biol. Chem. 1999, 274, 8254–8260. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.; Vita, J.A.; Venema, R.C.; Keaney, J.F., Jr. Ascorbic acid enhances endothelial nitric-oxide synthase activity by increasing intracellular tetrahydrobiopterin. J. Biol. Chem. 2000, 275, 17399–17406. [Google Scholar] [CrossRef] [Green Version]
- Baker, T.A.; Milstien, S.; Katusic, Z.S. Effect of vitamin C on the availability of tetrahydrobiopterin in human endothelial cells. J. Cardiovasc. Pharmacol. 2001, 37, 333–338. [Google Scholar] [CrossRef] [PubMed]
- D’Uscio, L.V.; Milstien, S.; Richardson, D.; Smith, L.; Katusic, Z.S. Long-term vitamin C treatment increases vascular tetrahydrobiopterin levels and nitric oxide synthase activity. Circ. Res. 2003, 92, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Tie, G.; Messina, L.M. Tetrahydrobiopterin, L-arginine and vitamin C actsynergistically to decrease oxidative stress, increase nitricoxide and improve blood flow after induction of hindlimb ischemia in the rat. Mol. Med. 2012, 18, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Ulker, S.; McKeown, P.P.; Bayraktutan, U. Vitamins reverse endothelial dysfunction through regulation of eNOS and NAD(P)H oxidase activities. Hypertension 2003, 41, 534–539. [Google Scholar] [CrossRef] [Green Version]
- Ladurner, A.; Schmitt, C.A.; Schachner, D.; Atanasov, A.G.; Werner, E.R.; Dirsch, V.M.; Heiss, E.H. Ascorbate stimulates endothelial nitric oxide synthase enzyme activity by rapid modulation of its phosphorylation status. Free Radic. Biol. Med. 2012, 52, 2082–2090. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Q.; Yang, J.; Santulli, G.; Reiken, S.R.; Wronska, A.; Kim, M.M.; Osborne, B.W.; Lacampagne, A.; Yin, Y.; Marks, A.R. Maintenance of normal blood pressure is dependent on IP3R1-mediated regulation of eNOS. Proc. Natl. Acad. Sci. USA 2016, 113, 8532–8537. [Google Scholar] [CrossRef] [Green Version]
- Forman, H.J.; Zhang, H.; Rinna, A. Glutathione: Overview of its protective roles, measurement, and biosynthesis. Mol. Aspect. Med. 2009, 30, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lushchak, V.I. Glutathione homeostasis and functions: Potential targets for medical interventions. J Amino Acids 2012, 2012, 736837. [Google Scholar] [CrossRef] [Green Version]
- Martensson, J.; Han, J.; Griffith, O.W.; Meister, A. Glutathione ester delays the onset of scurvy in ascorbate-deficient guinea pigs. Proc. Natl. Acad. Sci. USA 1993, 90, 317–321. [Google Scholar] [CrossRef] [Green Version]
- Guaiquil, V.H.; Vera, J.C.; Golde, D.W. Mechanism of vitamin C inhibition of cell death induced by oxidative stress in glutathione-depleted HL-60 cells. J. Biol. Chem. 2001, 276, 40955–40961. [Google Scholar] [CrossRef] [Green Version]
- Shang, F.; Lu, M.; Dudek, E.; Reddan, J.; Taylor, A. Vitamin C and vitamin E restore the resistance of GSH-depleted lens cells to H2O2. Free Radic. Biol. Med. 2003, 34, 521–530. [Google Scholar] [CrossRef]
- Waly, M.I.; Al-Attabi, Z.; Guizani, N. Low Nourishment of Vitamin C Induces Glutathione Depletion and Oxidative Stress in Healthy Young Adults. Prev. Nutr. Food Sci. 2015, 20, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.A.; Aon, M.A.; Frasier, C.R.; Sloan, R.C.; Maloney, A.H.; Anderson, E.J.; O’Rourke, B. Cardiac arrhythmias induced by glutathione oxidation can be inhibited by preventing mitochondrial depolarization. J. Mol. Cell. Cardiol. 2010, 48, 673–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Giovannucci, E.; Colditz, G.A.; Willett, W.C. Vitamin E consumption and the risk of coronary heart disease in men. N. Engl. J. Med. 1993, 328, 1450–1456. [Google Scholar] [CrossRef] [Green Version]
- Osganian, S.K.; Stampfer, M.J.; Rimm, E.; Spiegelman, D.; Hu, F.B.; Manson, J.E.; Willett, W.C. Vitamin C and risk of coronary heart disease in women. J. Am. Coll. Cardiol. 2003, 42, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Knekt, P.; Ritz, J.; Pereira, M.A.; O’Reilly, E.J.; Augustsson, K.; Fraser, G.E.; Goldbourt, U.; Heitmann, B.L.; Hallmans, G.; Liu, S.; et al. Antioxidant vitamins and coronary heart disease risk: A pooled analysis of 9 cohorts. Am. J. Clin. Nutr. 2004, 80, 1508–1520. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Folsom, A.R.; Harnack, L.; Halliwell, B.; Jacobs, D.R., Jr. Does supplemental vitamin C increase cardiovascular disease risk in women with diabetes? Am. J. Clin. Nutr. 2004, 80, 1194–1200. [Google Scholar] [CrossRef] [Green Version]
- Khaw, K.T.; Bingham, S.; Welch, A.; Luben, R.; Wareham, N.; Oakes, S.; Day, N. Relation between plasma ascorbic acid and mortality in men and women in EPIC-Norfolk prospective study: A prospective population study. European Prospective Investigation into Cancer and Nutrition. Lancet 2001, 357, 657–663. [Google Scholar] [CrossRef]
- Myint, P.K.; Luben, R.N.; Welch, A.A.; Bingham, S.A.; Wareham, N.J.; Khaw, K.T. Plasma vitamin C concentrations predict risk of incident stroke over 10 y in 20 649 participants of the European Prospective Investigation into Cancer Norfolk prospective population study. Am. J. Clin. Nutr. 2008, 87, 64–69. [Google Scholar] [CrossRef]
- Ascherio, A.; Rimm, E.B.; Hernan, M.A.; Giovannucci, E.; Kawachi, I.; Stampfer, M.J.; Willett, W.C. Relation of consumption of vitamin E, vitamin C, and carotenoids to risk for stroke among men in the United States. Ann. Intern. Med. 1999, 130, 963–970. [Google Scholar] [CrossRef]
- Salonen, R.M.; Nyyssonen, K.; Kaikkonen, J.; Porkkala-Sarataho, E.; Voutilainen, S.; Rissanen, T.H.; Tuomainen, T.P.; Valkonen, V.P.; Ristonmaa, U.; Lakka, H.M.; et al. Antioxidant Supplementation in Atherosclerosis Prevention, S., Six-year effect of combined vitamin C and E supplementation on atherosclerotic progression: The Antioxidant Supplementation in Atherosclerosis Prevention (ASAP) Study. Circulation 2003, 107, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Albert, C.M.; Gaziano, J.M.; Zaharris, E.; MacFadyen, J.; Danielson, E.; Buring, J.E.; Manson, J.E. A randomized factorial trial of vitamins C and E and beta carotene in the secondary prevention of cardiovascular events in women: Results from the Women’s Antioxidant Cardiovascular Study. Arch. Intern. Med. 2007, 167, 1610–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, J.A.; Hudes, E.S.; Tice, J.A. Relation of serum ascorbic acid to mortality among US adults. J. Am. Coll. Nutr. 2001, 20, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.A.; Hudes, E.S.; Browner, W.S. Serum ascorbic acid and cardiovascular disease prevalence in U.S. adults. Epidemiology 1998, 9, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Galan, P.; Preziosi, P.; Bertrais, S.; Mennen, L.; Malvy, D.; Roussel, A.M.; Favier, A.; Briancon, S. The SU.VI.MAX Study: A randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch. Intern. Med. 2004, 164, 2335–2342. [Google Scholar] [CrossRef] [Green Version]
- Sesso, H.D.; Buring, J.E.; Christen, W.G.; Kurth, T.; Belanger, C.; MacFadyen, J.; Bubes, V.; Manson, J.E.; Glynn, R.J.; Gaziano, J.M. Vitamins E and C in the prevention of cardiovascular disease in men: The Physicians’ Health Study II randomized controlled trial. JAMA 2008, 300, 2123–2133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heart Protection Study Collaborative, G. MRC/BHF Heart Protection Study of antioxidant vitamin supplementation in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 2002, 360, 23–33. [Google Scholar]
- Buijsse, B.; Jacobs, D.R., Jr.; Steffen, L.M.; Kromhout, D.; Gross, M.D. Plasma Ascorbic Acid, A Priori Diet Quality Score, and Incident Hypertension: A Prospective Cohort Study. PLoS ONE 2015, 10, e0144920. [Google Scholar] [CrossRef]
- Yochum, L.A.; Folsom, A.R.; Kushi, L.H. Intake of antioxidant vitamins and risk of death from stroke in postmenopausal women. Am. J. Clin. Nutr. 2000, 72, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Del Rio, D.; Agnoli, C.; Pellegrini, N.; Krogh, V.; Brighenti, F.; Mazzeo, T.; Masala, G.; Bendinelli, B.; Berrino, F.; Sieri, S.; et al. Total antioxidant capacity of the diet is associated with lower risk of ischemic stroke in a large Italian cohort. J. Nutr. 2011, 141, 118–123. [Google Scholar] [CrossRef] [Green Version]
- Ye, Z.; Song, H. Antioxidant vitamins intake and the risk of coronary heart disease: Meta-analysis of cohort studies. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Iso, H.; Date, C.; Kikuchi, S.; Watanabe, Y.; Wada, Y.; Inaba, Y.; Tamakoshi, A.; Group, J.S. Dietary intakes of antioxidant vitamins and mortality from cardiovascular disease: The Japan Collaborative Cohort Study (JACC) study. Stroke 2011, 42, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Li, J.; Yuan, Z. Effect of antioxidant vitamin supplementation on cardiovascular outcomes: A meta-analysis of randomized controlled trials. PLoS ONE 2013, 8, e56803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juraschek, S.P.; Guallar, E.; Appel, L.J.; Miller, E.R., 3rd. Effects of vitamin C supplementation on blood pressure: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 95, 1079–1088. [Google Scholar] [CrossRef]
- Chen, G.C.; Lu, D.B.; Pang, Z.; Liu, Q.F. Vitamin C intake, circulating vitamin C and risk of stroke: A meta-analysis of prospective studies. J. Am. Heart Assoc. 2013, 2, e000329. [Google Scholar] [CrossRef] [Green Version]
- Ashor, A.W.; Lara, J.; Mathers, J.C.; Siervo, M. Effect of vitamin C on endothelial function in health and disease: A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 2014, 235, 9–20. [Google Scholar] [CrossRef]
- Al-Khudairy, L.; Flowers, N.; Wheelhouse, R.; Ghannam, O.; Hartley, L.; Stranges, S.; Rees, K. Vitamin C supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 3, CD011114. [Google Scholar] [CrossRef] [Green Version]
- Ran, L.; Zhao, W.; Tan, X.; Wang, H.; Mizuno, K.; Takagi, K.; Zhao, Y.; Bu, H. Association between Serum Vitamin C and the Blood Pressure: A Systematic Review and Meta-Analysis of Observational Studies. Cardiovasc. Ther. 2020, 2020, 4940673. [Google Scholar] [CrossRef]
- Guan, Y.; Dai, P.; Wang, H. Effects of vitamin C supplementation on essential hypertension: A systematic review and meta-analysis. Medicine 2020, 99, e19274. [Google Scholar] [CrossRef]
- Jayedi, A.; Rashidy-Pour, A.; Parohan, M.; Zargar, M.S.; Shab-Bidar, S. Dietary and circulating vitamin C, vitamin E, beta-carotene and risk of total cardiovascular mortality: A systematic review and dose-response meta-analysis of prospective observational studies. Public Health Nutr. 2019, 22, 1872–1887. [Google Scholar] [CrossRef]
- Bird, J.K.; Murphy, R.A.; Ciappio, E.D.; McBurney, M.I. Risk of Deficiency in Multiple Concurrent Micronutrients in Children and Adults in the United States. Nutrients 2017, 9, 655. [Google Scholar] [CrossRef] [PubMed]
- Santulli, G.; Cipolletta, E.; Sorriento, D.; Del Giudice, C.; Anastasio, A.; Monaco, S.; Maione, A.S.; Condorelli, G.; Puca, A.; Trimarco, B.; et al. CaMK4 Gene Deletion Induces Hypertension. J. Am. Heart Assoc. 2012, 1, e001081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iaccarino, G.; Ciccarelli, M.; Sorriento, D.; Cipolletta, E.; Cerullo, V.; Iovino, G.L.; Paudice, A.; Elia, A.; Santulli, G.; Campanile, A.; et al. AKT participates in endothelial dysfunction in hypertension. Circulation 2004, 109, 2587–2593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R. The pathogenesis of atherosclerosis—An update. N. Engl. J. Med. 1986, 314, 488–500. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Hypertension, Thrombosis, Kidney Failure, and Diabetes: Is COVID-19 an Endothelial Disease? A Comprehensive Evaluation of Clinical and Basic Evidence. J. Clin. Med. 2020, 9, 1417. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Adams, M.R.; Clarkson, P.; Robinson, J.; McCredie, R.; Donald, A.; Deanfield, J.E. Passive smoking and impaired endothelium-dependent arterial dilatation in healthy young adults. N. Engl. J. Med. 1996, 334, 150–154. [Google Scholar] [CrossRef]
- Marti, C.N.; Gheorghiade, M.; Kalogeropoulos, A.P.; Georgiopoulou, V.V.; Quyyumi, A.A.; Butler, J. Endothelial dysfunction, arterial stiffness, and heart failure. J. Am. Coll. Cardiol. 2012, 60, 1455–1469. [Google Scholar] [CrossRef] [Green Version]
- Matarese, A.; Gambardella, J.; Sardu, C.; Santulli, G. miR-98 Regulates TMPRSS2 Expression in Human Endothelial Cells: Key Implications for COVID-19. Biomedicines 2020, 8, 462. [Google Scholar] [CrossRef]
- Aquila, G.; Morelli, M.B.; Vieceli Dalla Sega, F.; Fortini, F.; Nigro, P.; Caliceti, C.; Ferracin, M.; Negrini, M.; Pannuti, A.; Bonora, M.; et al. Heart rate reduction with ivabradine in the early phase of atherosclerosis is protective in the endothelium of ApoE-deficient mice. J. Physiol. Pharmacol. 2018, 69, 35–52. [Google Scholar]
- Gambardella, J.; Sorriento, D.; Bova, M.; Rusciano, M.; Loffredo, S.; Wang, X.; Petraroli, A.; Carucci, L.; Mormile, I.; Oliveti, M.; et al. Role of Endothelial G Protein-Coupled Receptor Kinase 2 in Angioedema. Hypertension 2020, 76, 1625–1636. [Google Scholar] [CrossRef] [PubMed]
- Sorriento, D.; Santulli, G.; Del Giudice, C.; Anastasio, A.; Trimarco, B.; Iaccarino, G. Endothelial cells are able to synthesize and release catecholamines both in vitro and in vivo. Hypertension 2012, 60, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambardella, J.; Morelli, M.B.; Wang, X.J.; Santulli, G. Pathophysiological mechanisms underlying the beneficial effects of physical activity in hypertension. J. Clin. Hypertens. 2020, 22, 291–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munro, J.M.; Cotran, R.S. The pathogenesis of atherosclerosis: Atherogenesis and inflammation. Lab. Investig. 1988, 58, 249–261. [Google Scholar] [PubMed]
- Forman, J.P.; Choi, H.; Curhan, G.C. Fructose and vitamin C intake do not influence risk for developing hypertension. J. Am. Soc. Nephrol. 2009, 20, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Jensen, C.D.; Norkus, E.P.; Hudes, M.; Crawford, P.B. Vitamin C in plasma is inversely related to blood pressure and change in blood pressure during the previous year in young Black and White women. Nutr. J. 2008, 7, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, R.M.; Daghini, E.; Ghiadoni, L.; Sudano, I.; Rugani, I.; Varanini, M.; Passino, C.; Emdin, M.; Taddei, S. Effect of acute administration of vitamin C on muscle sympathetic activity, cardiac sympathovagal balance, and baroreflex sensitivity in hypertensive patients. Am. J. Clin. Nutr. 2012, 96, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Heitzer, T.; Just, H.; Munzel, T. Antioxidant vitamin C improves endothelial dysfunction in chronic smokers. Circulation 1996, 94, 6–9. [Google Scholar] [CrossRef]
- Fuller, C.J.; Grundy, S.M.; Norkus, E.P.; Jialal, I. Effect of ascorbate supplementation on low density lipoprotein oxidation in smokers. Atherosclerosis 1996, 119, 139–150. [Google Scholar] [CrossRef]
- Van Hoydonck, P.G.; Schouten, E.G.; Manuel, Y.K.B.; van Campenhout, A.; Hoppenbrouwers, K.P.; Temme, E.H. Does vitamin C supplementation influence the levels of circulating oxidized LDL, sICAM-1, sVCAM-1 and vWF-antigen in healthy male smokers? Eur. J. Clin. Nutr. 2004, 58, 1587–1593. [Google Scholar] [CrossRef]
- Salonen, J.T.; Nyyssonen, K.; Salonen, R.; Lakka, H.M.; Kaikkonen, J.; Porkkala-Sarataho, E.; Voutilainen, S.; Lakka, T.A.; Rissanen, T.; Leskinen, L.; et al. Antioxidant Supplementation in Atherosclerosis Prevention (ASAP) study: A randomized trial of the effect of vitamins E and C on 3-year progression of carotid atherosclerosis. J. Intern. Med. 2000, 248, 377–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valls, N.; Gormaz, J.G.; Aguayo, R.; Gonzalez, J.; Brito, R.; Hasson, D.; Libuy, M.; Ramos, C.; Carrasco, R.; Prieto, J.C.; et al. Amelioration of persistent left ventricular function impairment through increased plasma ascorbate levels following myocardial infarction. Redox Rep. 2016, 21, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranadive, S.M.; Joyner, M.J.; Walker, B.G.; Taylor, J.L.; Casey, D.P. Effect of vitamin C on hyperoxia-induced vasoconstriction in exercising skeletal muscle. J. Appl. Physiol. 2014, 117, 1207–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barak, O.F.; Caljkusic, K.; Hoiland, R.L.; Ainslie, P.N.; Thom, S.R.; Yang, M.; Jovanov, P.; Dujic, Z. Differential influence of vitamin C on the peripheral and cerebral circulation after diving and exposure to hyperoxia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, R759–R767. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.D.; Mather, K.J.; Newcomer, S.C.; Mickleborough, T.D.; Wallace, J.P. Vitamin C prevents the acute decline of flow-mediated dilation after altered shear rate patterns. Appl. Physiol. Nutr. Metab. 2013, 38, 268–274. [Google Scholar] [CrossRef]
- Thosar, S.S.; Bielko, S.L.; Wiggins, C.C.; Klaunig, J.E.; Mather, K.J.; Wallace, J.P. Antioxidant vitamin C prevents decline in endothelial function during sitting. Med. Sci. Monit. 2015, 21, 1015–1021. [Google Scholar]
- De Marchi, S.; Prior, M.; Rigoni, A.; Zecchetto, S.; Rulfo, F.; Arosio, E. Ascorbic acid prevents vascular dysfunction induced by oral glucose load in healthy subjects. Eur. J. Intern. Med. 2012, 23, 54–57. [Google Scholar] [CrossRef]
- Batista, G.M.S.; Rocha, H.N.M.; Storch, A.S.; Garcia, V.P.; Teixeira, G.F.; Mentzinger, J.; Gomes, E.A.C.; Velasco, L.L.; Nobrega, A.C.L.; Rocha, N.G. Ascorbic acid inhibits vascular remodeling induced by mental stress in overweight/obese men. Life Sci. 2020, 250, 117554. [Google Scholar] [CrossRef]
- Plotnick, M.D.; D’Urzo, K.A.; Gurd, B.J.; Pyke, K.E. The influence of vitamin C on the interaction between acute mental stress and endothelial function. Eur. J. Appl. Physiol. 2017, 117, 1657–1668. [Google Scholar] [CrossRef]
- Richards, J.C.; Crecelius, A.R.; Larson, D.G.; Dinenno, F.A. Acute ascorbic acid ingestion increases skeletal muscle blood flow and oxygen consumption via local vasodilation during graded handgrip exercise in older adults. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H360–H368. [Google Scholar] [CrossRef] [Green Version]
- Meredith, M.E.; Qu, Z.C.; May, J.M. Ascorbate reverses high glucose- and RAGE-induced leak of the endothelial permeability barrier. Biochem. Biophys. Res. Commun. 2014, 445, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, W.H.; Rhea, E.M.; Qu, Z.C.; Hecker, M.R.; May, J.M. Intracellular ascorbate tightens the endothelial permeability barrier through Epac1 and the tubulin cytoskeleton. Am. J. Physiol. Cell Physiol. 2016, 311, C652–C662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulker, E.; Parker, W.H.; Raj, A.; Qu, Z.C.; May, J.M. Ascorbic acid prevents VEGF-induced increases in endothelial barrier permeability. Mol. Cell. Biochem. 2016, 412, 73–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chelazzi, C.; Villa, G.; Mancinelli, P.; De Gaudio, A.R.; Adembri, C. Glycocalyx and sepsis-induced alterations in vascular permeability. Crit. Care 2015, 19, 26. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Sarmiento, J.; Salazar-Pelaez, L.M.; Carcillo, J.A. The Endothelial Glycocalyx: A Fundamental Determinant of Vascular Permeability in Sepsis. Pediatr. Crit. Care Med. 2020, 21, e291–e300. [Google Scholar] [CrossRef]
- Kang, Q.; Chen, Y.; Zhang, X.; Yu, G.; Wan, X.; Wang, J.; Bo, L.; Zhu, K. Heat shock protein A12B protects against sepsis-induced impairment in vascular endothelial permeability. J. Surg. Res. 2016, 202, 87–94. [Google Scholar] [CrossRef]
- Li, Z.; Yin, M.; Zhang, H.; Ni, W.; Pierce, R.W.; Zhou, H.J.; Min, W. BMX Represses Thrombin-PAR1-Mediated Endothelial Permeability and Vascular Leakage During Early Sepsis. Circ. Res. 2020, 126, 471–485. [Google Scholar] [CrossRef]
- Mironova, G.D.; Belosludtseva, N.V.; Ananyan, M.A. Prospects for the use of regulators of oxidative stress in the comprehensive treatment of the novel Coronavirus Disease 2019 (COVID-19) and its complications. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8585–8591. [Google Scholar]
- Schonrich, G.; Raftery, M.J.; Samstag, Y. Devilishly radical NETwork in COVID-19: Oxidative stress, neutrophil extracellular traps (NETs), and T cell suppression. Adv. Biol. Regul. 2020, 77, 100741. [Google Scholar] [CrossRef]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J.; et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. Protein J. 2020, 1–13. [Google Scholar] [CrossRef]
- Montel-Hagen, A.; Kinet, S.; Manel, N.; Mongellaz, C.; Prohaska, R.; Battini, J.L.; Delaunay, J.; Sitbon, M.; Taylor, N. Erythrocyte Glut1 triggers dehydroascorbic acid uptake in mammals unable to synthesize vitamin C. Cell 2008, 132, 1039–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Russo, T.A.; Kwon, O.; Chanock, S.; Rumsey, S.C.; Levine, M. Ascorbate recycling in human neutrophils: Induction by bacteria. Proc. Natl. Acad. Sci. USA 1997, 94, 13816–13819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, S.R.; Kapoor, A.; Rath, M.; Thomas, S.A. What is the role of supplementation with ascorbic acid, zinc, vitamin D, or N-acetylcysteine for prevention or treatment of COVID-19? Clevel. Clin. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Rowe, S. The Emerging Role of Vitamin C in the Prevention and Treatment of COVID-19. Nutrients 2020, 12, 3286. [Google Scholar] [CrossRef]
- Gillani, S.W.; Sulaiman, S.A.S.; Abdul, M.I.M.; Baig, M.R. Combined effect of metformin with ascorbic acid versus acetyl salicylic acid on diabetes-related cardiovascular complication; a 12-month single blind multicenter randomized control trial. Cardiovasc. Diabetol. 2017, 16, 103. [Google Scholar] [CrossRef]
- Ceriello, A.; Novials, A.; Ortega, E.; Canivell, S.; La Sala, L.; Pujadas, G.; Bucciarelli, L.; Rondinelli, M.; Genovese, S. Vitamin C further improves the protective effect of glucagon-like peptide-1 on acute hypoglycemia-induced oxidative stress, inflammation, and endothelial dysfunction in type 1 diabetes. Diabetes Care 2013, 36, 4104–4108. [Google Scholar] [CrossRef] [Green Version]
- Bae, M.; Kim, H. Mini-Review on the Roles of Vitamin C, Vitamin D, and Selenium in the Immune System against COVID-19. Molecules 2020, 25, 5346. [Google Scholar] [CrossRef]
- Bronte, V.; Zanovello, P. Regulation of immune responses by L-arginine metabolism. Nat. Rev. Immunol. 2005, 5, 641–654. [Google Scholar] [CrossRef]
- Wijnands, K.A.; Castermans, T.M.; Hommen, M.P.; Meesters, D.M.; Poeze, M. Arginine and citrulline and the immune response in sepsis. Nutrients 2015, 7, 1426–1463. [Google Scholar] [CrossRef] [Green Version]
- Kuck, J.L.; Bastarache, J.A.; Shaver, C.M.; Fessel, J.P.; Dikalov, S.I.; May, J.M.; Ware, L.B. Ascorbic acid attenuates endothelial permeability triggered by cell-free hemoglobin. Biochem. Biophys. Res. Commun. 2018, 495, 433–437. [Google Scholar] [CrossRef]
- Lundblad, C.; Bentzer, P. Effects of L-arginine on cerebral blood flow, microvascular permeability, number of perfused capillaries, and brain water content in the traumatized mouse brain. Microvasc. Res. 2007, 74, 1–8. [Google Scholar] [CrossRef] [PubMed]
- May, J.M.; Qu, Z.C. Nitric oxide mediates tightening of the endothelial barrier by ascorbic acid. Biochem. Biophys. Res. Commun. 2011, 404, 701–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, A.C.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, T.; Date, C.; Kokubo, Y.; Yoshiike, N.; Matsumura, Y.; Tanaka, H. Serum vitamin C concentration was inversely associated with subsequent 20-year incidence of stroke in a Japanese rural community. The Shibata study. Stroke 2000, 31, 2287–2294. [Google Scholar] [CrossRef] [Green Version]
- Michels, A.J.; Frei, B. Myths, artifacts, and fatal flaws: Identifying limitations and opportunities in vitamin C research. Nutrients 2013, 5, 5161–5192. [Google Scholar] [CrossRef] [Green Version]
- Henriquez-Sanchez, P.; Sanchez-Villegas, A.; Doreste-Alonso, J.; Ortiz-Andrellucchi, A.; Pfrimer, K.; Serra-Majem, L. Dietary assessment methods for micronutrient intake: A systematic review on vitamins. Br. J. Nutr. 2009, 102, S10–S37. [Google Scholar] [CrossRef] [Green Version]
- Cahill, L.E.; El-Sohemy, A. Vitamin C transporter gene polymorphisms, dietary vitamin C and serum ascorbic acid. J. Nutrigenet. Nutrigenom. 2009, 2, 292–301. [Google Scholar] [CrossRef]
- Horska, A.; Mislanova, C.; Bonassi, S.; Ceppi, M.; Volkovova, K.; Dusinska, M. Vitamin C levels in blood are influenced by polymorphisms in glutathione S-transferases. Eur. J. Nutr. 2011, 50, 437–446. [Google Scholar] [CrossRef]
- Cahill, L.E.; El-Sohemy, A. Haptoglobin genotype modifies the association between dietary vitamin C and serum ascorbic acid deficiency. Am. J. Clin. Nutr. 2010, 92, 1494–1500. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Reduced (left) and oxidized (right) forms of vitamin C.


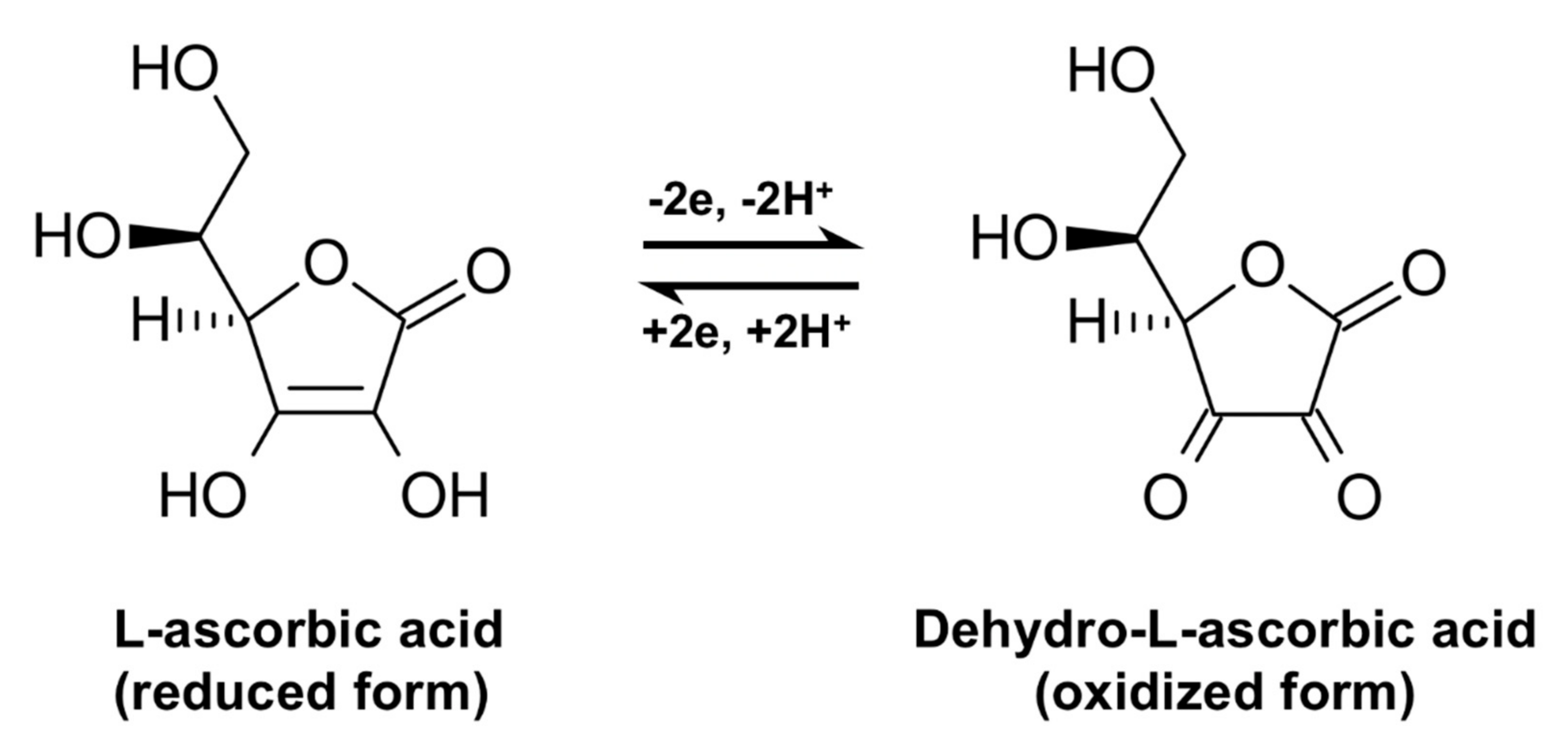{kind=link}
Table 1.
Major studies investigating the association between vitamin C and cardiovascular disease (CVD).
Table 1.
Major studies investigating the association between vitamin C and cardiovascular disease (CVD).
| Clinical Study | Study Population | Vitamin C Concentration Range | Fasting Blood Sample (Assay Used) | Adjustments | Outcome | Ref. |
|---|---|---|---|---|---|---|
| EPIC-Norfolk | 19,496 healthy men and women from Norfolk (US) | 25.9–79.2 μmol/L | Non-fasting venous blood (fluorometric assay) | Age, systolic BP, cholesterol, smoking, diabetes, and supplement use | A mean follow-up of 4 years showed that 20 μmol/L rising in plasma Vitamin C concentration was associated with ~20% reduced risk of all-cause mortality | [121,139] |
| EPIC-Norfolk | 20,299 healthy men and women from Norfolk (US) | 41–66 μmol/L | Non-fasting venous blood (fluorometric assay) | Age, sex, smoking, BMI, physical activity, systolic BP, diabetes, cholesterol, MI, social class, alcohol, and supplement used | A mean follow-up of 12.8 years showed that every 20 μmol/L increase in plasma Vitamin C was associated with a 9% relative reduction in the risk of HF. | [140] |
| HPFS—Health Professionals Follow-up Study | 39,910 healthy US male, health professionals | 95–116 mg/dL | Not reported | Age, season, smoking, energy intake, alcohol, hypertension, history of MI, profession, BMI, and physical activity | After a mean follow-up of 8 years, Vitamin C intake was not associated with a lower risk of CHD and stroke | [141] |
| NHS I—Nurses’ Health Study 1 | 85,118 healthy US female nurses | 70–704 mg/dL | Not reported | Age, energy intake, supplements use, alcohol, smoking status, and diabetes | Data from 16 years of follow-up indicate that Vitamin C supplement is associated with a significantly lower risk of CHD | [138] |
| ASAP—Antioxidant Supplementation in Atherosclerosis Prevention | 520 men and post-menopausal women, with hyper-cholesterolemia | Not specified | Not specified (HPLC assay) | Sex, baseline HDL cholesterol | A 6–year follow-up indicated that Vitamin C supplementation reduced the slope of the mean carotid artery intima-media thickness progression | [142] |
| Women’s Antioxidant Cardiovascular Study | 8171 female health professionals with CVD, or 3 or more CVD risk factors | Not specified | Not reported | Compliance-adjusted analyses | After a follow-up of 9.4 years, no overall effects of Vitamin C (500 mg/day) on all major cardiovascular events and stroke | [143] |
| NHANES II | 8417 US men and women | 17–79.5 μmol/L | Non-fasting venous blood (colorimetric assay) | Age, sex, race, education, physical activity, dietary energy and fat intake, cholesterol, BMI, alcohol, smoking, diabetes, hypertension, CHD, stroke, cancer, use of aspirin, Vitamin E intake | Decreased risk of all-cause mortality | [144] |
| NHANES III | 6624 US men and women | 17–85.2 μmol/L | Non-fasting venous blood (colorimetric assay) | Age, sex, race, education, physical activity, smoking, alcohol, cholesterol, BMI, diabetes, hypertension, use of aspirin, Vitamin E intake | Top Vitamin C group had a 27% lower CVD risk compared to bottom group | [145] |
| SU.VI.MAX study | 13,017 French adults | Not specified | Fasting venous blood (continuous flow segmented by air bubbles) | Bonferroni adjustment for multiple mean comparisons | After a follow-up of 7.5 years, no effect of Vitamin C supplementation (120 mg/d) on CVD; lower all-cause mortality in men | [146] |
| PHS II—Physicians Health Study II | 14,641 healthy US male physicians | Not specified | Not reported | Age, PHS cohort, randomized β–carotene, Vitamin E or Vitamin C, and multivitamin assignments | A mean follow-up of ~8 years showed that Vitamin C supplementation (500 mg/day) had no significant effect on the incidence of CVD, stroke, or mortality for cardiovascular events | [147] |
| Heart Protection Study | 20,536 British men and women with CHD, occlusive arterial disease, or diabetes | Not specified | Non-fasting venous blood | Not specified | After a follow-up of 5 years, Vitamin C supplementation (250 mg/d) had no significant effects on CVD | [148] |
| CARDIA | 2884 healthy US men and women | 24–70 μmol/L | Fasting venous blood (HPLC assay) | Age, sex, race, center, education, smoking, alcohol, physical activity, a priori diet quality score and food consumption, BMI, waist circumference, history of diabetes, systolic BP | Higher plasma Vitamin C, due to better diet quality, is inversely related to high BP. | [149] |
| Iowa Women’s Health Study | 1923 post-menopausal diabetic women from U.S. (55 to 69 years) | 82–≥679 mg/day | Not reported | Age, total energy intake, history of hypertension, BMI, waist-hip ratio, smoking status and amount smoked, alcohol consumption, physical activity score, hormone replacement therapy, main type and duration of diabetes, medications | After a follow-up of 11 years, an association between increased mortality for CVD or CHD and Vitamin C ≥ 300 mg/day was reported. Vitamin C intake was unrelated to CVD and stroke mortality in nondiabetic women. | [150] |
| Italian section of the EPIC Study | 41,620 Italians previously diagnosed with stroke or myocardial infarction (44 to 61 years) | 83–201 mg/day | Not reported | Age, sex, hypertension, smoking, alcohol, education, energy intake, waist circumference, obesity, and physical activity | After 7.9 years of follow-up, Vitamin C was associated with a lower risk of ischemic stroke | [151] |
Table 2.
Main meta-analyses investigating the correlation between vitamin C intake or its plasma levels and cardiovascular disease (CVD).
Table 2.
Main meta-analyses investigating the correlation between vitamin C intake or its plasma levels and cardiovascular disease (CVD).
| Meta-Analysis Topic | Number of Studies | Total Participants (n) | Trial Duration | Vitamin C Supplement Dosage | Outcome | Ref. |
|---|---|---|---|---|---|---|
| Coronary Heart Disease | 14 cohorts | 374,488 | mean duration: 10 y. | Not reported | Dietary Vitamin C had an inverse association with CHD risk, but supplement intake of Vitamin C had no significant association with CHD risk. | [154] |
| Hypertension | 29 trials | 1407 | mean duration: 8 wks. | 60 to 4000 mg/day (median 500 mg/day) | Daily supplementation of Vitamin C in hypertensive participants reduced systolic BP by 3.84 mm Hg and DBP by 1.48 mm Hg. | [159] |
| Coronary Heart Disease | 15 trials | 188,209 | from 1.4 y. to 12 y. | 120 to 1000 mg/day | Vitamin C in association with Vitamin E and beta-carotene had no effect on CHD or other major cardiovascular events. Vitamin C in association with Vitamin E and beta-carotene had no effect on stroke risk compared to placebo. | [156] |
| Stroke | 16 cohorts | 217,454 participants for studies on Vitamin C intake 29,648 participants for studies on circulating Vitamin C | from 6.1 y. to 30 y. | 45 to 1167 mg/day | 19% lower risk of stroke (pooled analysis of 2 studies) comparing the highest to the lowest dietary Vitamin C intakes. 38% lower risk of stroke (pooled analysis of 6 studies) with the highest versus lowest circulating Vitamin C concentrations. | [160] |
| Endothelial function | 44 trials | 1324 | from 1 d. to 8 wks. | 500 to 2000 mg/day | A significant positive effect of Vitamin C supplementation on endothelial function measured by flow-mediated dilation (19 trials), evaluating pulse-wave (5 trials) and forearm blood flow (20 trials). | [161] |
| Arterial stiffness | 22 trials | 1909 | from 1 d. to 7 y. (mean duration: 56 d.) | 120 to 4000 mg/day (mean 2000 mg/day) | Association of Vitamin C with Vitamin E and β–carotene improved arterial stiffness irrespective of the age group | [161] |
| Cardiovascular events | 8 trials | 15,445 | mean duration: 8 y. | – | Inconsistent or low-quality (downgraded) evidence for the correlation between Vitamin C supplementation and major cardiovascular events or cardiovascular mortality | [157] |
| Hypertension | 11 cross-sectional studies and 7 case-control studies | 22,200 | – | – | Serum Vitamin C level was significantly lower in hypertensive compared to normotensive subjects. Inverse correlation between serum Vitamin C concentration and SBP or DBP. | [162] |
| Hypertension | 8 trials | 614 | from 4 wks. to 24 wks. | 300 to 1000 mg/day | Significantly reduced SBP and DBP in the subgroups of age ≥35 and ≥60 years with Vitamin C supplementation ≥500 mg/day for 6 weeks or more. | [163] |
| Cardiovascular mortality | 15 trials | 320,548 | from 4 to 22y. | 50 to 450 mg/day | Higher Vitamin C intake is associated with a lower risk of cardiovascular mortality | [164] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Morelli, M.B.; Gambardella, J.; Castellanos, V.; Trimarco, V.; Santulli, G. Vitamin C and Cardiovascular Disease: An Update. Antioxidants 2020, 9, 1227. https://doi.org/10.3390/antiox9121227
AMA Style
Morelli MB, Gambardella J, Castellanos V, Trimarco V, Santulli G. Vitamin C and Cardiovascular Disease: An Update. Antioxidants. 2020; 9(12):1227. https://doi.org/10.3390/antiox9121227
Chicago/Turabian StyleMorelli, Marco B., Jessica Gambardella, Vanessa Castellanos, Valentina Trimarco, and Gaetano Santulli. 2020. "Vitamin C and Cardiovascular Disease: An Update" Antioxidants 9, no. 12: 1227. https://doi.org/10.3390/antiox9121227
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.