

Sepsis-Induced Coagulopathy Phenotype Induced by Oxidized High-Density Lipoprotein Associated with Increased Mortality in Septic-Shock Patients
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Volunteers
2.2. Plasma HDL and oxHDL Measurements, Extraction, and Determination of HDL Oxidation Kinetics Parameters
2.3. Plasma Measurements of Coagulation Parameters and Secreted Proteins Determination
2.4. Circulating Endothelial Cell (CECs) Separation and Protein Expression Determination Using Flow Cytometry
2.5. Endothelial Cell Culture, mRNA Isolation and RT-qPCR
2.6. Generation of Oxidization of HDL
2.7. Reagents and Inhibitors
2.8. Data Analyses
3. Results
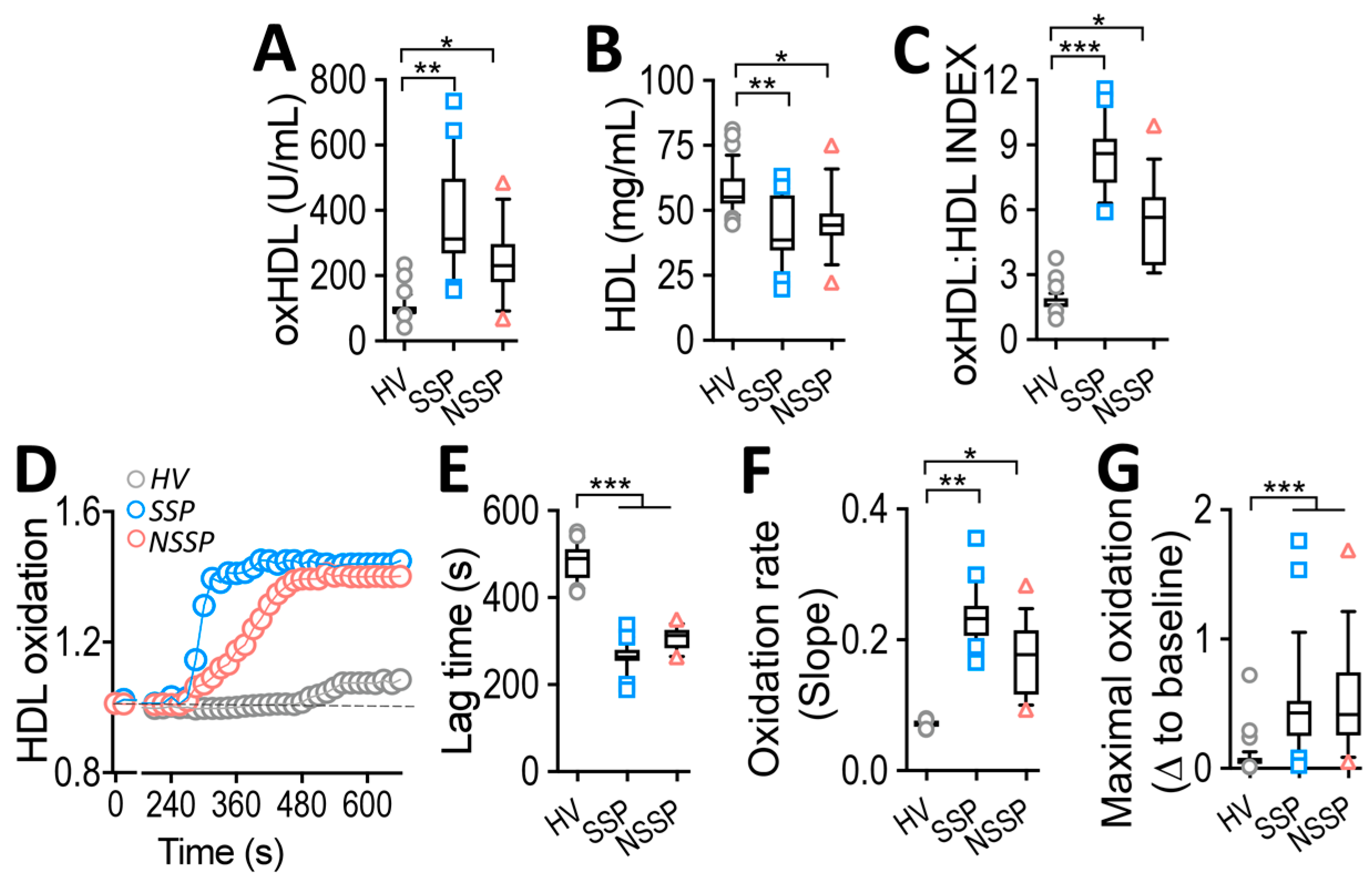
3.1. Increased oxHDL Plasma Level in SSP and NSSP
3.2. Susceptibility to Oxidation of HDL from SSP
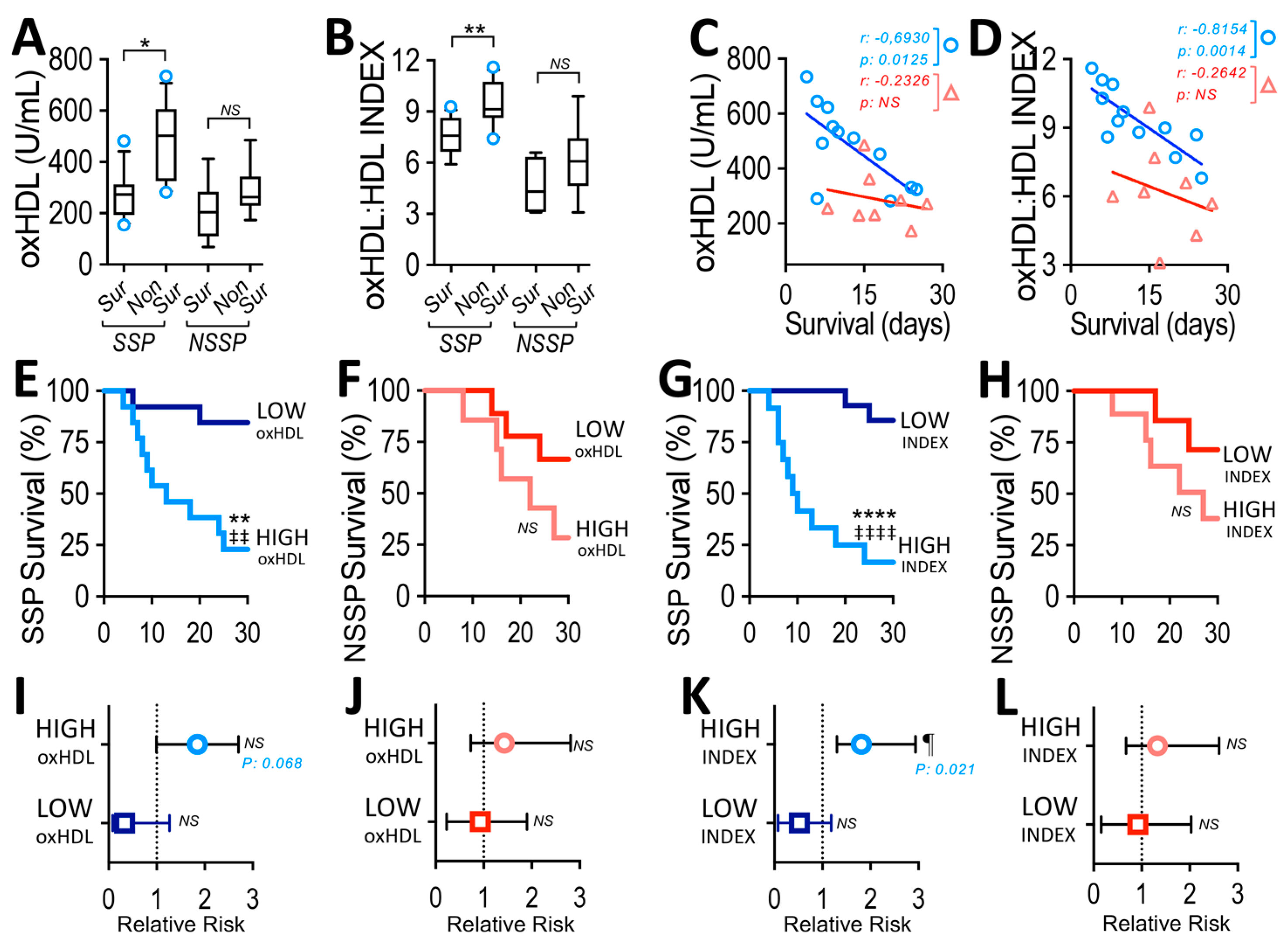
3.3. Plasma oxHDL Level and INDEX in Non-Survivor SSP
3.4. High-INDEX Increases Relative Risk of Death in SSP
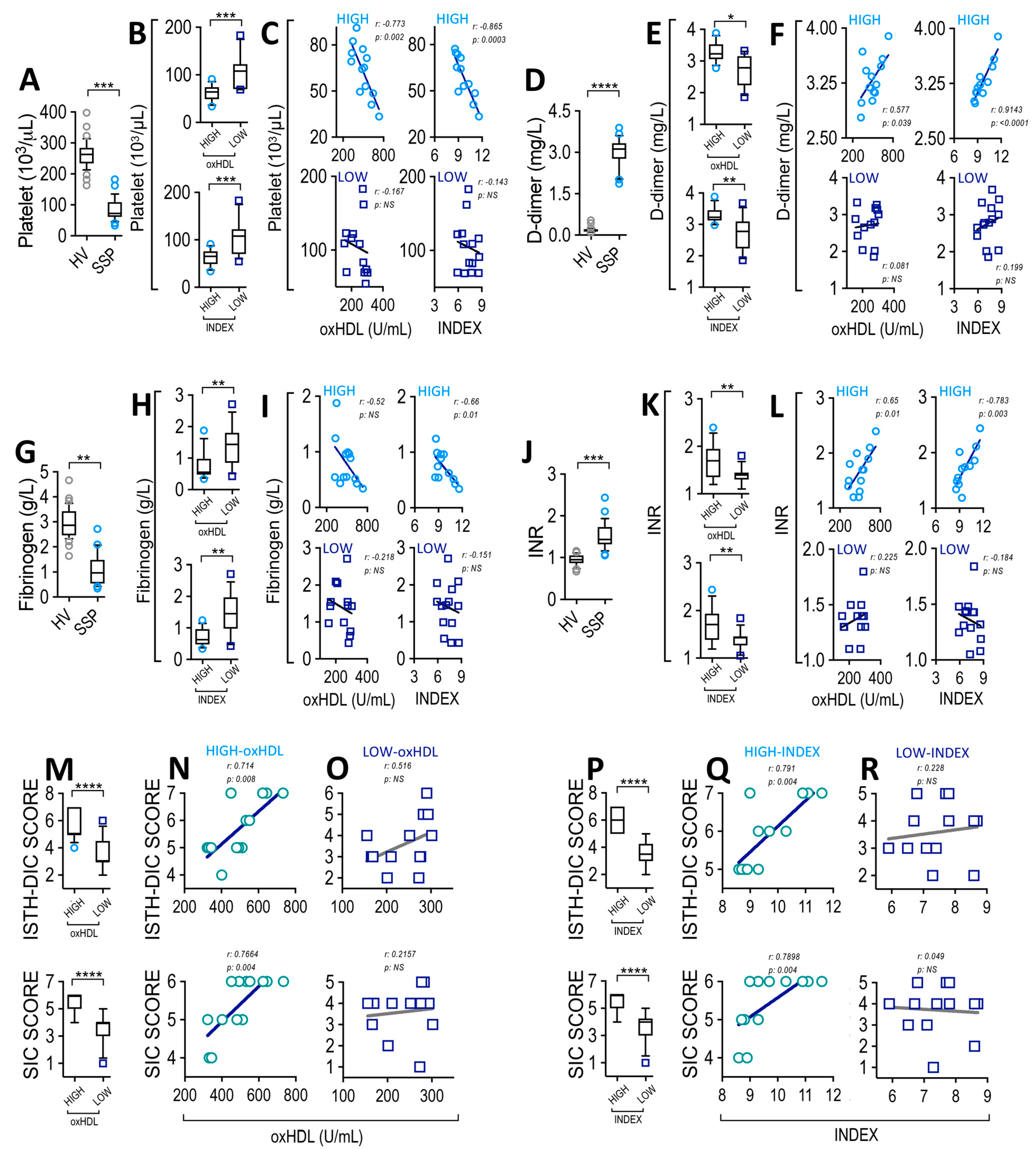
3.5. High-oxHDL Level and High-INDEX Correlates with SIC Score in SSP
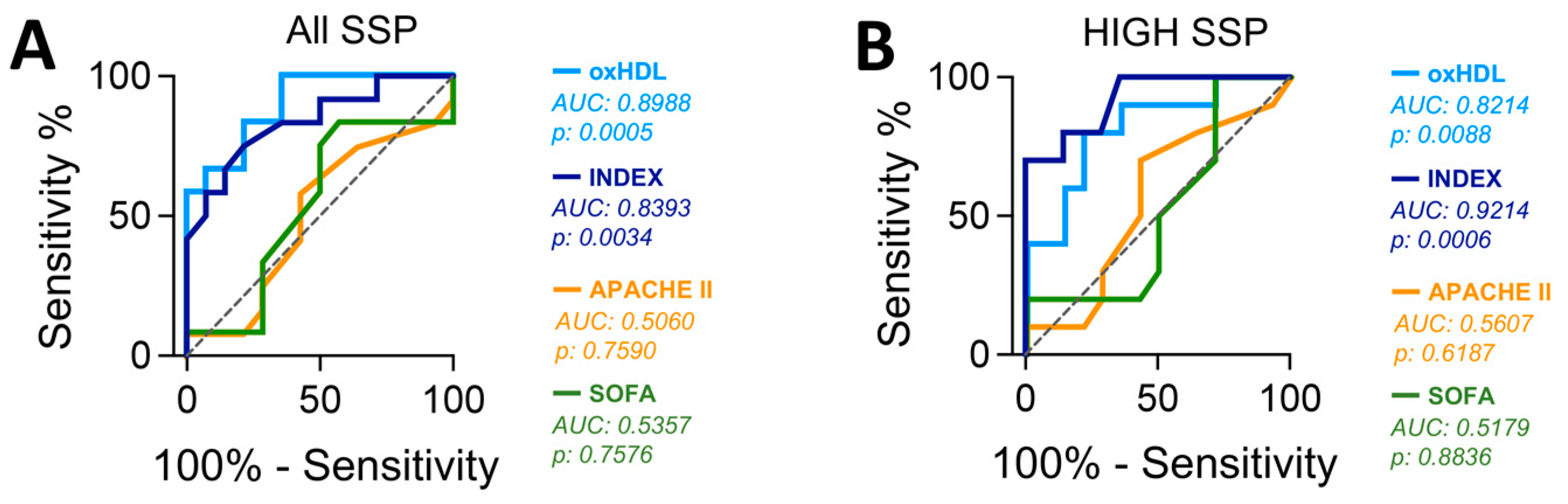
3.6. Plasma oxHDL Level and INDEX Are Associated with Increased Mortality in SSP
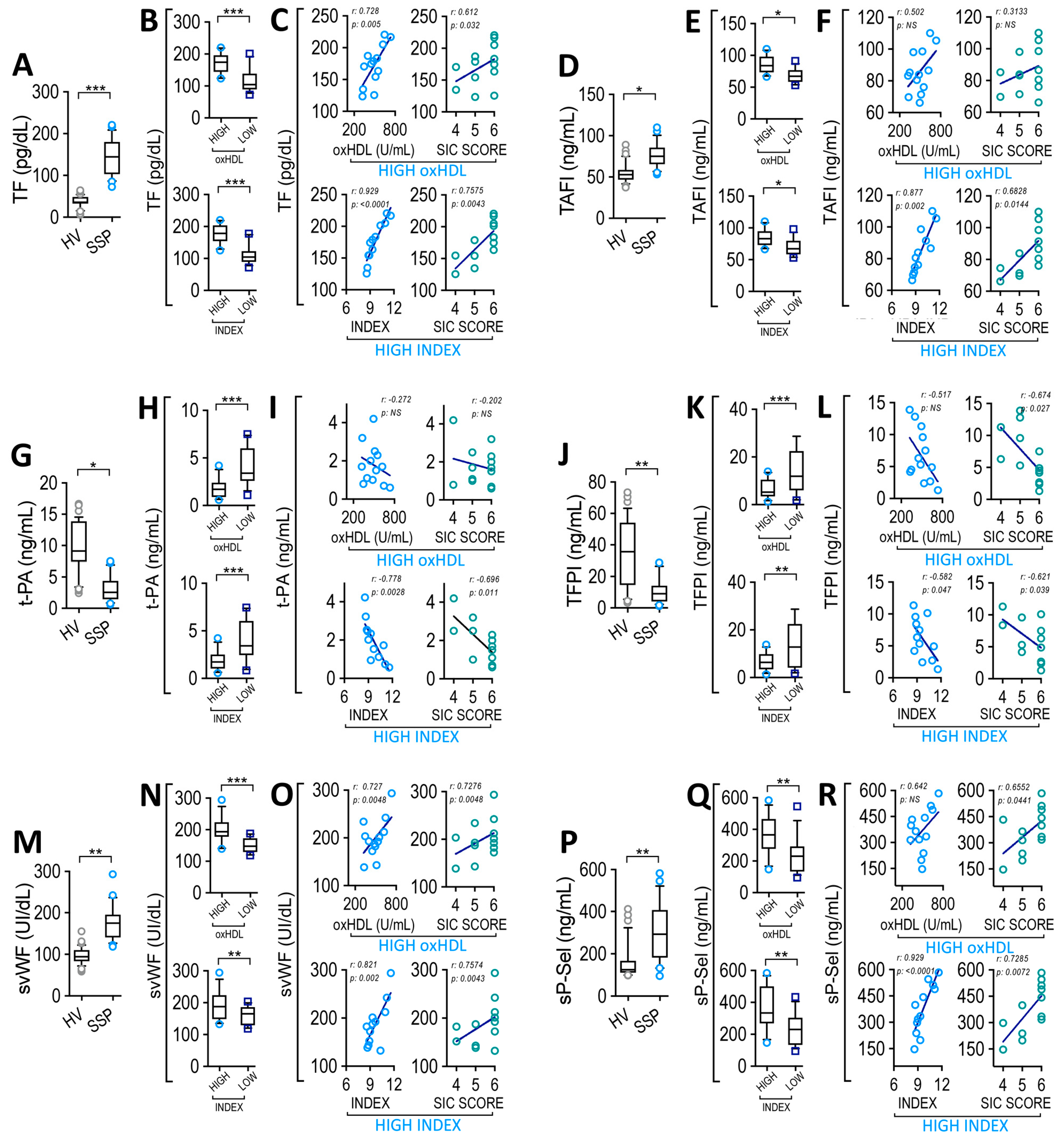
3.7. Plasma oxHDL Level and INDEX Correlate with Coagulation Factors and Platelet Adhesion Proteins Level in SSP
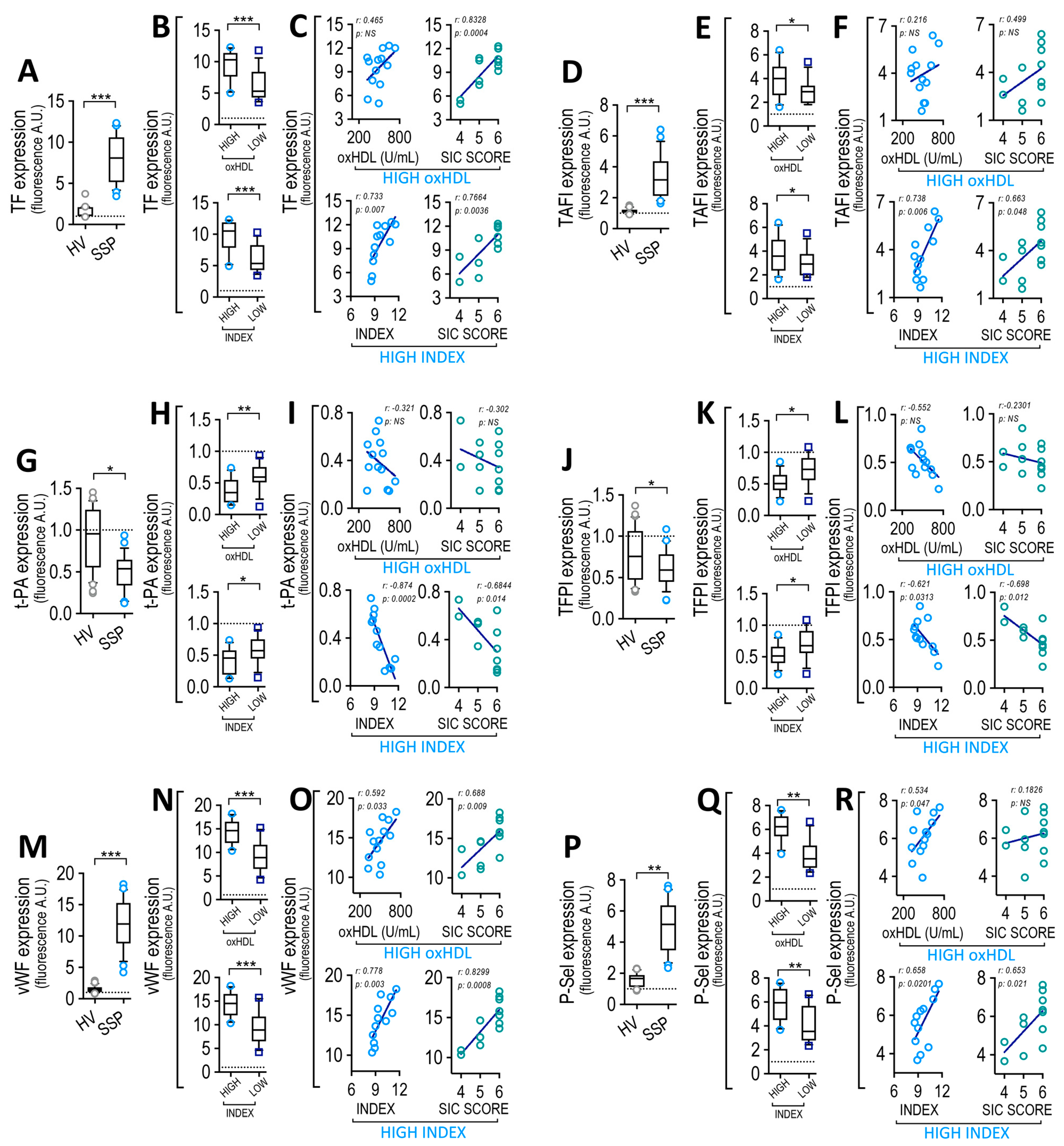
3.8. Circulating Endothelial Cells from SSP Exhibited Modified Coagulation Factors and Platelet Adhesion Protein Expression, which Correlate with Plasma oxHDL and INDEX
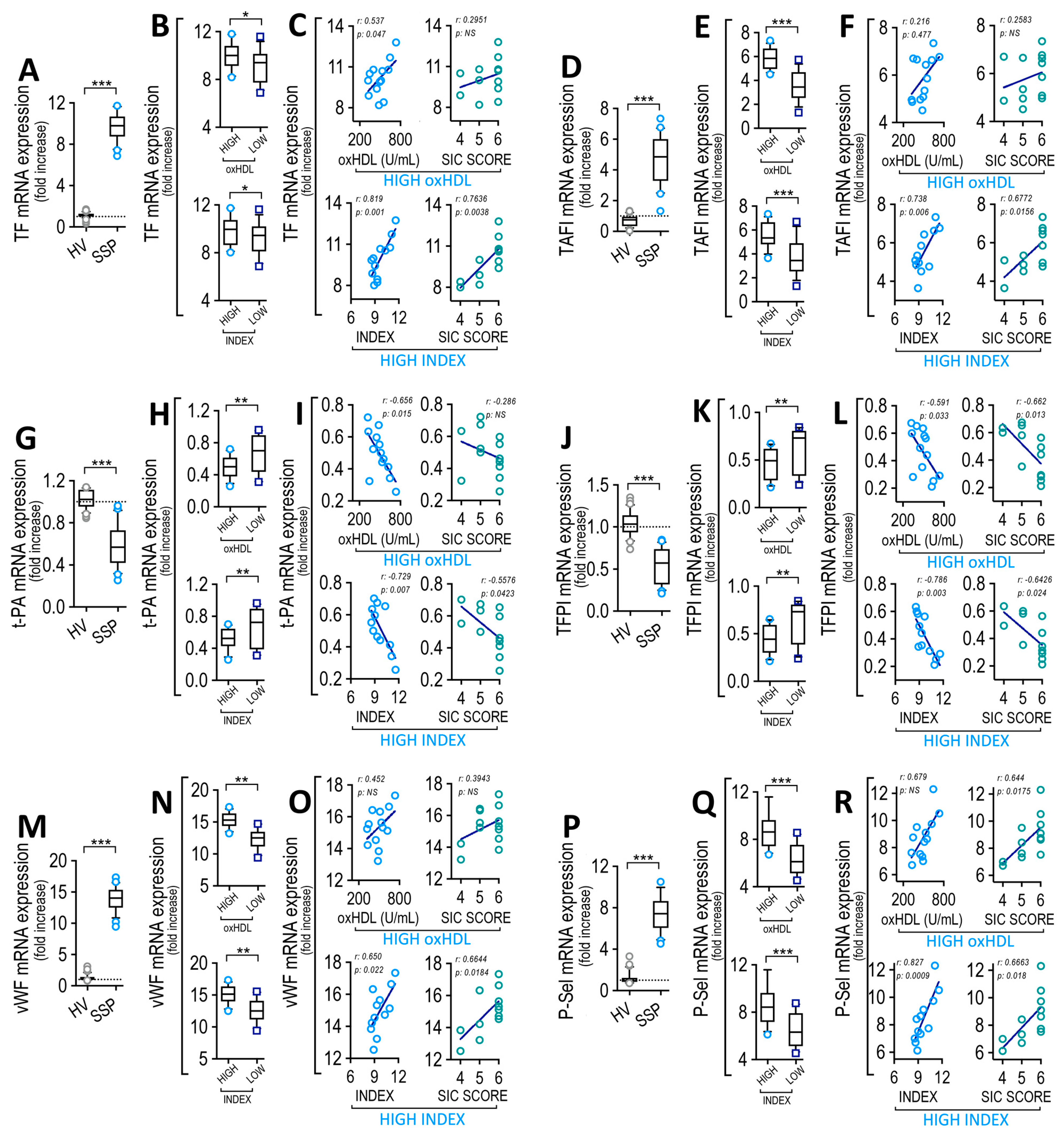
3.9. Endothelial Cells Exposed to Plasma from SSP Modified Coagulation Factors and Platelet Adhesion Protein Expression, Which Correlate with Plasma oxHDL and INDEX
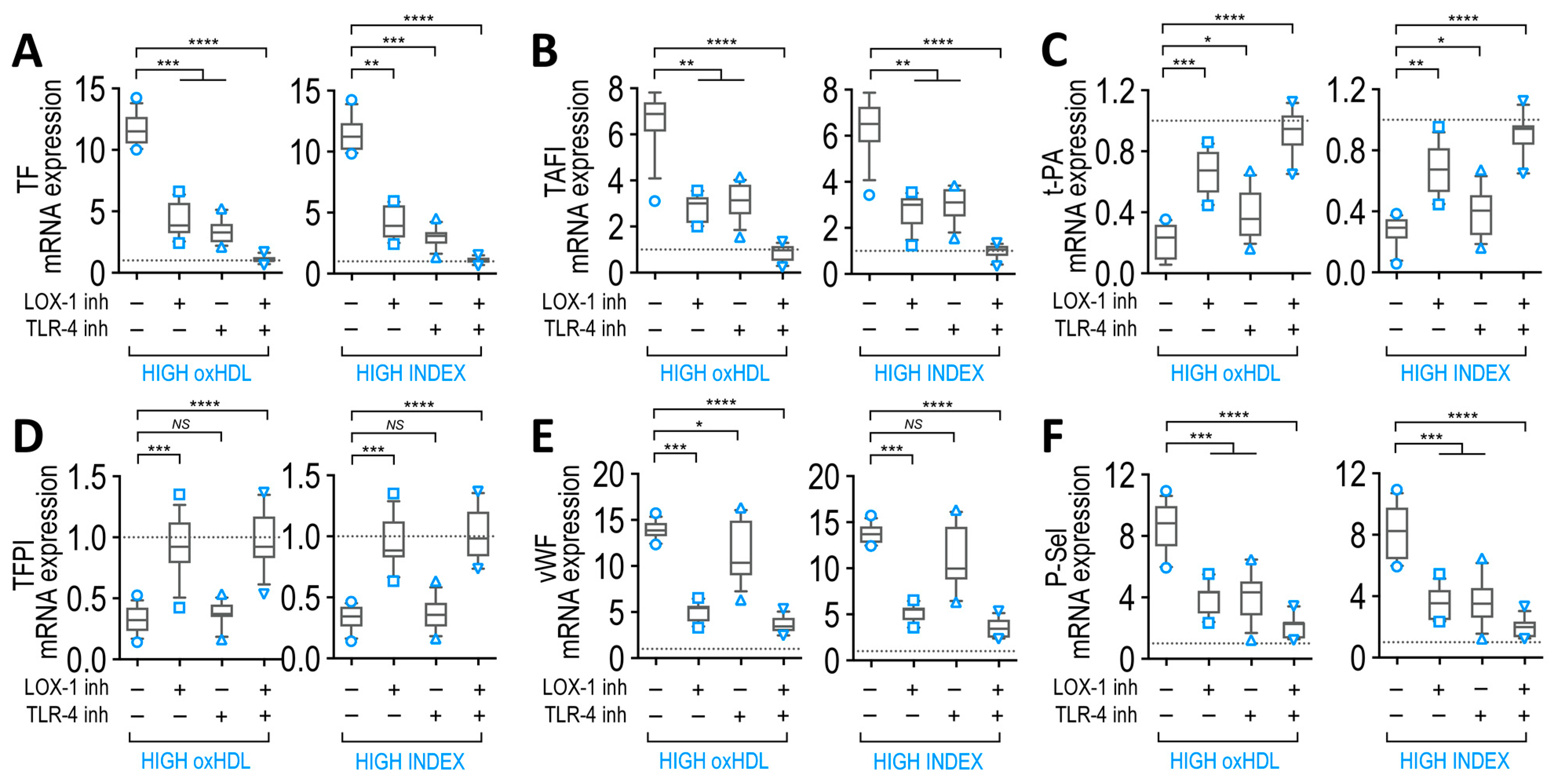
3.10. LOX-1 and TLR-4 Receptors Mediate Actions of SSP Plasma in Endothelial Cells
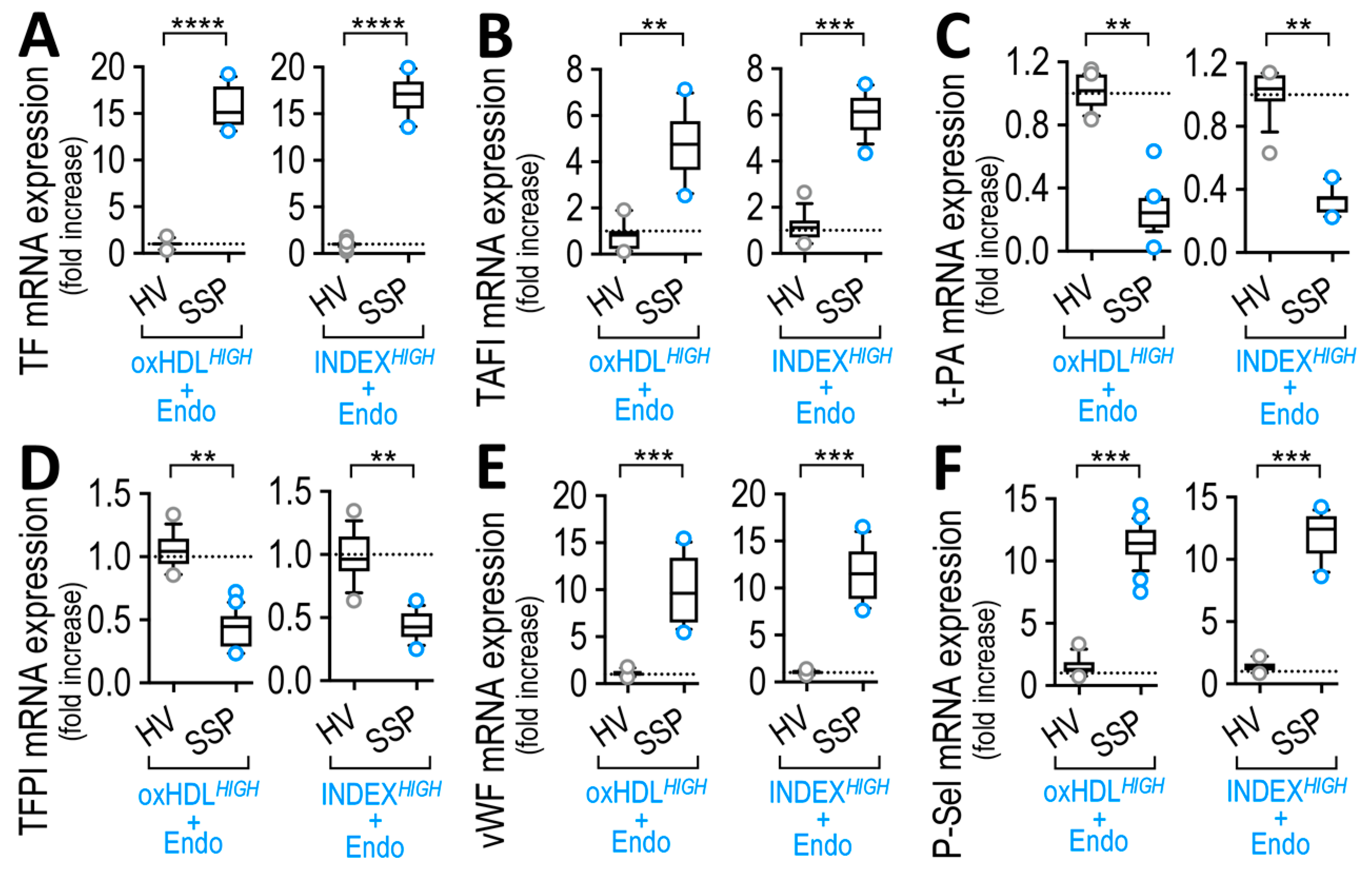
3.11. Endothelial Cells Exposed to Exogenous SSP Plasma Preparation Modified Coagulation Factors and Platelet Adhesion Protein Expression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Crit. Care Med. 2018, 46, 997–1000. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Shiraishi, A.; Yamakawa, K.; Ogura, H.; Saitoh, D.; Fujishima, S.; Mayumi, T.; Kushimoto, S.; Abe, T.; Shiino, Y.; et al. Role of Disseminated Intravascular Coagulation in Severe Sepsis. Thromb. Res. 2019, 178, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Tamura, T.; Sawatsubashi, Y. Sepsis and Disseminated Intravascular Coagulation. J. Intensive Care 2016, 4, 23. [Google Scholar] [CrossRef] [Green Version]
- Sakr, Y.; Dubois, M.-J.; Backer, D.D.; Creteur, J.; Vincent, J.-L. Persistent Microcirculatory Alterations Are Associated with Organ Failure and Death in Patients with Septic Shock. Crit. Care Med. 2004, 32, 1825–1831. [Google Scholar] [CrossRef]
- Backer, D.D.; Donadello, K.; Sakr, Y.; Ospina-Tascon, G.; Salgado, D.; Scolletta, S.; Vincent, J.-L. Microcirculatory Alterations in Patients with Severe Sepsis: Impact of Time of Assessment and Relationship with Outcome. Crit. Care Med. 2013, 41, 791–799. [Google Scholar] [CrossRef] [Green Version]
- Levi, M. Disseminated Intravascular Coagulation. Crit. Care Med. 2007, 35, 2191–2195. [Google Scholar] [CrossRef]
- Tanaka, T.; Tsujinaka, T.; Kambayashi, J.; Higashiyama, M.; Yokota, M.; Sakon, M.; Mori, T. The Effect of Heparin on Multiple Organ Failure and Disseminated Intravascular Coagulation in a Sepsis Model. Thromb. Res. 1990, 60, 321–330. [Google Scholar] [CrossRef]
- Suga, Y.; Tashiro, K.; Staub, Y.; Komura, S.; Yamada, S.; Morishita, E.; Asakura, H. Potential of Continuous TPA Infusion for Multiple-Organ Failure from Lipopolysaccharide-Induced Disseminated Intravascular Coagulation in Rats. Thromb. Res. 2021, 206, 84–87. [Google Scholar] [CrossRef]
- Taylor, F.; Toh, C.-H.; Hoots, K.; Wada, H.; Levi, M. Towards Definition, Clinical and Laboratory Criteria, and a Scoring System for Disseminated Intravascular Coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi, M.; Poll, T. van der. A Short Contemporary History of Disseminated Intravascular Coagulation. Semin. Thromb. Hemost. 2014, 40, 874–880. [Google Scholar] [PubMed]
- Gando, S.; Saitoh, D.; Ogura, H.; Mayumi, T.; Koseki, K.; Ikeda, T.; Ishikura, H.; Iba, T.; Ueyama, M.; Eguchi, Y.; et al. Disseminated Intravascular Coagulation (DIC) Diagnosed Based on the Japanese Association for Acute Medicine Criteria Is a Dependent Continuum to Overt DIC in Patients with Sepsis. Thromb. Res. 2009, 123, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Iba, T.; Eguchi, Y.; Ohtomo, Y.; Okamoto, K.; Koseki, K.; Mayumi, T.; Murata, A.; Ikeda, T.; Ishikura, H.; et al. A Multicenter, Prospective Validation of Disseminated Intravascular Coagulation Diagnostic Criteria for Critically Ill Patients: Comparing Current Criteria. Crit. Care Med. 2006, 34, 625–631. [Google Scholar] [CrossRef]
- Iba, T.; Nisio, M.D.; Levy, J.H.; Kitamura, N.; Thachil, J. New Criteria for Sepsis-Induced Coagulopathy (SIC) Following the Revised Sepsis Definition: A Retrospective Analysis of a Nationwide Survey. BMJ Open. 2017, 7, e017046. [Google Scholar] [CrossRef] [Green Version]
- Iba, T.; Umemura, Y.; Wada, H.; Levy, J.H. Roles of Coagulation Abnormalities and Microthrombosis in Sepsis: Pathophysiology, Diagnosis, and Treatment. Arch. Med. Res. 2021, 52, 788–797. [Google Scholar] [CrossRef]
- Tran-Dinh, A.; Diallo, D.; Delbosc, S.; Varela-Perez, L.M.; Dang, Q.B.; Lapergue, B.; Burillo, E.; Michel, J.B.; Levoye, A.; Martin-Ventura, J.L.; et al. HDL and Endothelial Protection. Br. J. Pharm. 2013, 169, 493–511. [Google Scholar] [CrossRef] [Green Version]
- Tall, A.R. Plasma High Density Lipoproteins: Therapeutic Targeting and Links to Atherogenic Inflammation. Atherosclerosis 2018, 276, 39–43. [Google Scholar] [CrossRef] [Green Version]
- Holy, E.W.; Besler, C.; Reiner, M.F.; Camici, G.G.; Manz, J.; Beer, J.H.; Luescher, T.F.; Landmesser, U.; Tanner, F.C. High-Density Lipoprotein from Patients with Coronary Heart Disease Loses Anti-Thrombotic Effects on Endothelial Cells: Impact on Arterial Thrombus Formation. Thromb. Haemost. 2014, 112, 1024–1035. [Google Scholar] [CrossRef]
- O’Connell, B.J.; Genest, J. High-Density Lipoproteins and Endothelial Function. Circulation 2001, 104, 1978–1983. [Google Scholar] [CrossRef] [Green Version]
- Pablo-Moreno, J.A.D.; Serrano, L.J.; Revuelta, L.; Sánchez, M.J.; Liras, A. The Vascular Endothelium and Coagulation: Homeostasis, Disease, and Treatment, with a Focus on the Von Willebrand Factor and Factors VIII and V. Int. J. Mol. Sci. 2022, 23, 8283. [Google Scholar] [CrossRef] [PubMed]
- Boos, C.J.; Goon, P.K.Y.; Lip, G.Y.H. The Endothelium, Inflammation, and Coagulation in Sepsis. Clin. Pharmacol. 2006, 79, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Pérez, L.; Muñoz-Durango, N.; Riedel, C.A.; Echeverría, C.; Kalergis, A.M.; Cabello-Verrugio, C.; Simon, F. Endothelial-to-Mesenchymal Transition: Cytokine-Mediated Pathways That Determine Endothelial Fibrosis under Inflammatory Conditions. Cytokine Growth Factor Rev. 2017, 33, 41–54. [Google Scholar] [CrossRef]
- Petäjä, J. Inflammation and Coagulation. An Overview. Thromb. Res. 2011, 127, S34–S37. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento, D.; Montorfano, I.; Cáceres, M.; Echeverría, C.; Fernández, R.; Cabello-Verrugio, C.; Cerda, O.; Tapia, P.; Simon, F. Endotoxin-Induced Vascular Endothelial Cell Migration Is Dependent on TLR4/NF-ΚB Pathway, NAD(P)H Oxidase Activation, and Transient Receptor Potential Melastatin 7 Calcium Channel Activity. Int. J. Biochem. Cell Biol. 2014, 55, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Simon, F.; Leiva-Salcedo, E.; Armisén, R.; Riveros, A.; Cerda, O.; Varela, D.; Eguiguren, A.L.; Olivero, P.; Stutzin, A. Hydrogen Peroxide Removes TRPM4 Current Desensitization Conferring Increased Vulnerability to Necrotic Cell Death. J. Biol. Chem. 2010, 285, 37150–37158. [Google Scholar] [CrossRef] [Green Version]
- Pérez, L.; Vallejos, A.; Echeverria, C.; Varela, D.; Cabello-Verrugio, C.; Simon, F. OxHDL Controls LOX-1 Expression and Plasma Membrane Localization through a Mechanism Dependent on NOX/ROS/NF-ΚB Pathway on Endothelial Cells. Lab. Investig. 2019, 99, 421–437. [Google Scholar] [CrossRef]
- Montorfano, I.; Becerra, A.; Cerro, R.; Echeverría, C.; Sáez, E.; Morales, M.G.; Fernández, R.; Cabello-Verrugio, C.; Simon, F. Oxidative Stress Mediates the Conversion of Endothelial Cells into Myofibroblasts via a TGF-Β1 and TGF-Β2-Dependent Pathway. Lab. Investig. 2014, 94, 1068–1082. [Google Scholar] [CrossRef] [Green Version]
- Tsimikas, S.; Miller, Y.I. Oxidative Modification of Lipoproteins: Mechanisms, Role in Inflammation and Potential Clinical Applications in Cardiovascular Disease. Curr. Pharm. Des. 2011, 17, 27–37. [Google Scholar] [CrossRef]
- Pirillo, A.; Norata, G.D.; Catapano, A.L. LOX-1, OxLDL, and Atherosclerosis. Mediat. Inflamm. 2013, 2013, 152786. [Google Scholar] [CrossRef] [Green Version]
- Nakano, T.; Nagata, A. Oxidative Susceptibility of Apolipoprotein AI in Serum. Clin. Chim. Acta. 2005, 362, 119–124. [Google Scholar] [CrossRef]
- Speer, T.; Rohrer, L.; Blyszczuk, P.; Shroff, R.; Kuschnerus, K.; Kränkel, N.; Kania, G.; Zewinger, S.; Akhmedov, A.; Shi, Y.; et al. Abnormal High-Density Lipoprotein Induces Endothelial Dysfunction via Activation of Toll-like Receptor-2. Immunity 2013, 38, 754–768. [Google Scholar] [CrossRef] [Green Version]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. Biological Consequences of Dysfunctional HDL. Curr. Med. Chem. 2018, 25, 1644–1664. [Google Scholar] [CrossRef] [PubMed]
- Norata, G.D.; Banfi, C.; Pirillo, A.; Tremoli, E.; Hamsten, A.; Catapano, A.L.; Eriksson, P. Oxidised-HDL3 Induces the Expression of PAI-1 in Human Endothelial Cells. Role of P38MAPK Activation and MRNA Stabilization. Br. J. Haematol. 2004, 127, 97–104. [Google Scholar] [CrossRef]
- Ebara, S.; Marumo, M.; Mukai, J.; Ohki, M.; Uchida, K.; Wakabayashi, I. Relationships of Oxidized HDL with Blood Coagulation and Fibrinolysis in Patients with Type 2 Diabetes Mellitus. J. Thromb. Thrombolysis. 2018, 45, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Ebara, S.; Marumo, M.; Yamabata, C.; Nishibe, I.; Soneda, J.-I.; Mukai, J.; Ohki, M.; Uchida, K.; Wakabayashi, I. Inverse Associations of HDL Cholesterol and Oxidized HDL with D-Dimer in Patients with Type 2 Diabetes Mellitus. Thromb. Res. 2017, 155, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.J.; Vanella, L.; Gotlinger, K.; Jiang, H.; Singh, S.P.; Sodhi, K.; Maher, E.; O’Hanlon, K.; Shapiro, J.I.; Abraham, N.G. Oxidized HDL Is a Potent Inducer of Adipogenesis and Causes Activation of the Ang-II and 20-HETE Systems in Human Obese Females. Prostaglandins Other Lipid Mediat. 2016, 123, 68–77. [Google Scholar] [CrossRef]
- Marin, M.T.; Dasari, P.S.; Tryggestad, J.B.; Aston, C.E.; Teague, A.M.; Short, K.R. Oxidized HDL and LDL in Adolescents with Type 2 Diabetes Compared to Normal Weight and Obese Peers. J. Diabetes Complicat. 2015, 29, 679–685. [Google Scholar] [CrossRef]
- Honda, H.; Ueda, M.; Kojima, S.; Mashiba, S.; Michihata, T.; Takahashi, K.; Shishido, K.; Akizawa, T. Oxidized High-Density Lipoprotein as a Risk Factor for Cardiovascular Events in Prevalent Hemodialysis Patients. Atherosclerosis 2012, 220, 493–501. [Google Scholar] [CrossRef]
- Tsumura, M.; Kinouchi, T.; Ono, S.; Nakajima, T.; Komoda, T. Serum Lipid Metabolism Abnormalities and Change in Lipoprotein Contents in Patients with Advanced-Stage Renal Disease. Clin. Chim. Acta. 2001, 314, 27–37. [Google Scholar] [CrossRef]
- Ungurianu, A.; Margină, D.; Grădinaru, D.; Băcanu, C.; Ilie, M.; Tsitsimpikou, C.; Tsarouhas, K.; Spandidos, D.A.; Tsatsakis, A.M. Lipoprotein Redox Status Evaluation as a Marker of Cardiovascular Disease Risk in Patients with Inflammatory Disease. Mol. Med. Rep. 2017, 15, 256–262. [Google Scholar] [CrossRef] [Green Version]
- Guirgis, F.W.; Dodani, S.; Leeuwenburgh, C.; Moldawer, L.; Bowman, J.; Kalynych, C.; Grijalva, V.; Reddy, S.T.; Jones, A.E.; Moore, F.A. HDL Inflammatory Index Correlates with and Predicts Severity of Organ Failure in Patients with Sepsis and Septic Shock. PLoS ONE 2018, 13, e0203813. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Wang, L.; Chen, B. Recombinant HDL (Milano) Protects Endotoxin-Challenged Rats from Multiple Organ Injury and Dysfunction. Biol. Chem. 2015, 396, 53–60. [Google Scholar] [CrossRef]
- Cirstea, M.; Walley, K.R.; Russell, J.A.; Brunham, L.R.; Genga, K.R.; Boyd, J.H. Decreased High-Density Lipoprotein Cholesterol Level Is an Early Prognostic Marker for Organ Dysfunction and Death in Patients with Suspected Sepsis. J. Crit. Care 2017, 38, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Inoue, I.; Noji, S.; Awata, T.; Takahashi, K.; Nakajima, T.; Sonoda, M.; Komoda, T.; Katayama, S. Bezafibrate Has an Antioxidant Effect: Peroxisome Proliferator-Activated Receptor Alpha Is Associated with Cu2+, Zn2+-Superoxide Dismutase in the Liver. Life Sci. 1998, 63, 135–144. [Google Scholar] [CrossRef]
- Esterbauer, H.; Striegl, G.; Puhl, H.; Rotheneder, M. Continuous Monitoring of in Vitro Oxidation of Human Low Density Lipoprotein. Free Radic. Res. Commun. 1989, 6, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Tapia, P.; Gatica, S.; Cortés-Rivera, C.; Otero, C.; Becerra, A.; Riedel, C.A.; Cabello-Verrugio, C.; Kalergis, A.M.; Simon, F. Circulating Endothelial Cells From Septic Shock Patients Convert to Fibroblasts Are Associated With the Resuscitation Fluid Dose and Are Biomarkers for Survival Prediction. Crit. Care Med. 2019, 47, 942–950. [Google Scholar] [CrossRef]
- Schlichting, D.E.; Waxman, A.B.; O’Brien, L.A.; Wang, T.; Naum, C.C.; Rubeiz, G.J.; Um, S.L.; Williams, M.; Yan, S.-C.B. Circulating Endothelial and Endothelial Progenitor Cells in Patients with Severe Sepsis. Microvasc. Res. 2011, 81, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Scoccia, A.E.; Molinuevo, M.S.; McCarthy, A.D.; Cortizo, A.M. A Simple Method to Assess the Oxidative Susceptibility of Low Density Lipoproteins. BMC Clin. Pathol. 2001, 1, 20963. [Google Scholar] [CrossRef] [Green Version]
- Lynch, S.M.; Frei, B. Reduction of Copper, but Not Iron, by Human Low Density Lipoprotein (LDL). Implications for Metal Ion-Dependent Oxidative Modification of LDL. J. Biol. Chem. 1995, 270, 5158–5163. [Google Scholar] [CrossRef] [Green Version]
- Soomro, A.Y.; Guerchicoff, A.; Nichols, D.J.; Suleman, J.; Dangas, G.D. The Current Role and Future Prospects of D-Dimer Biomarker. Eur. Heart J. Cardiovasc. Pharm. 2016, 2, 175–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, J.B.; Aggerbeck, M.A.; Granfeldt, A.; Schmidt, M.; Hvas, A.-M.; Adelborg, K. Disseminated Intravascular Coagulation Diagnosis: Positive Predictive Value of the ISTH Score in a Danish Population. Res. Pract. Thromb. Haemost. 2021, 5, e12636. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levi, M.; Levy, J.H. Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. Semin. Thromb. Hemost. 2020, 46, 89–95. [Google Scholar] [PubMed]
- Mutunga, M.; Fulton, B.; Bullock, R.; Batchelor, A.; Gascoigne, A.; Gillespie, J.I.; Baudouin, S.V. Circulating Endothelial Cells in Patients with Septic Shock. Am. J. Respir. Crit. Care Med. 2001, 163, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Echeverría, C.; Montorfano, I.; Sarmiento, D.; Becerra, A.; Nuñez-Villena, F.; Figueroa, X.F.; Cabello-Verrugio, C.; Elorza, A.A.; Riedel, C.; Simon, F. Lipopolysaccharide Induces a Fibrotic-like Phenotype in Endothelial Cells. J. Cell Mol. Med. 2013, 17, 800–814. [Google Scholar] [CrossRef]
- Echeverría, C.; Montorfano, I.; Tapia, P.; Riedel, C.; Cabello-Verrugio, C.; Simon, F. Endotoxin-Induced Endothelial Fibrosis Is Dependent on Expression of Transforming Growth Factors Β1 and Β2. Infect. Immun. 2014, 82, 3678–3686. [Google Scholar] [CrossRef] [Green Version]
- Vallejos, A.; Olivares, P.; Gatica, S.; Villegas, V.; Echeverria, C.; Cabello-Verrugio, C.; Simon, F. Endotoxemia-Induced Endothelial Fibrosis Inhibition Improves Hypotension, Tachycardia, Multiple Organ Dysfunction Syndrome, Cytokine Response, Oxidative Stress, and Survival. Lab. Investig. 2019, 99, 1173–1192. [Google Scholar] [CrossRef]
- Gatica, S.; Villegas, V.; Vallejos, A.; Olivares, P.; Aballai, V.; Lagos-Meza, F.; Echeverria, C.; Cabello-Verrugio, C.; Varela, D.; Simon, F. TRPM7 Mediates Kidney Injury, Endothelial Hyperpermeability and Mortality during Endotoxemia. Lab. Investig. 2019, 100, 234–249. [Google Scholar] [CrossRef]
- Chien, J.-Y.; Jerng, J.-S.; Yu, C.-J.; Yang, P.-C. Low Serum Level of High-Density Lipoprotein Cholesterol Is a Poor Prognostic Factor for Severe Sepsis. Crit. Care Med. 2005, 33, 1688–1693. [Google Scholar] [CrossRef]
- Rojas, M.; Prado, Y.; Tapia, P.; Carreño, L.J.; Cabello-Verrugio, C.; Simon, F. Oxidized High-Density Lipoprotein Induces Endothelial Fibrosis Promoting Hyperpermeability, Hypotension, and Increased Mortality. Antioxidants 2022, 11, 2469. [Google Scholar] [CrossRef]
- Takaeko, Y.; Matsui, S.; Kajikawa, M.; Maruhashi, T.; Kishimoto, S.; Hashimoto, H.; Kihara, Y.; Hida, E.; Chayama, K.; Goto, C.; et al. Association of Extremely High Levels of High-Density Lipoprotein Cholesterol with Endothelial Dysfunction in Men. J. Clin. Lipidol. 2019, 13, 664–672.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesa, S.T.; Charakida, M.; McLoughlin, E.; Nguyen, H.C.; Georgiopoulos, G.; Motran, L.; Elia, Y.; Marcovecchio, M.L.; Dunger, D.B.; Dalton, R.N.; et al. Elevated High-Density Lipoprotein in Adolescents with Type 1 Diabetes Is Associated with Endothelial Dysfunction in the Presence of Systemic Inflammation. Eur. Heart J. 2019, 40, 3559–3566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoep, M.; van der Korporaal, S.J.A.; Eck, M.V. High-Density Lipoprotein as a Modulator of Platelet and Coagulation Responses. Cardiovasc. Res. 2014, 103, 362–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memon, R.A.; Staprans, I.; Noor, M.; Holleran, W.M.; Uchida, Y.; Moser, A.H.; Feingold, K.R.; Grunfeld, C. Infection and Inflammation Induce LDL Oxidation in Vivo. Arter. Thromb. Vasc. Biol. 2000, 20, 1536–1542. [Google Scholar] [CrossRef] [Green Version]
- Dittrich, R.; Dragonas, C.; Mueller, A.; Maltaris, T.; Rupp, J.; Beckmann, M.W.; Maass, M. Endothelial Chlamydia Pneumoniae Infection Promotes Oxidation of LDL. Biochem. Biophys. Res. Commun. 2004, 319, 501–505. [Google Scholar] [CrossRef]
- Dirican, M.; Taş, S.; Sarandöl, E.; Tokullugil, H.A. Susceptibility of Non-HDL Fraction to Oxidation in Experimental Nephrotic Syndrome. Kobe. J. Med. Sci. 1998, 44, 235–245. [Google Scholar]
- Jurek, A.; Turyna, B.; Kubit, P.; Klein, A. LDL Susceptibility to Oxidation and HDL Antioxidant Capacity in Patients with Renal Failure. Clin. Biochem. 2006, 39, 19–27. [Google Scholar] [CrossRef]
- Chantepie, S.; Malle, E.; Sattler, W.; Chapman, M.J.; Kontush, A. Distinct HDL Subclasses Present Similar Intrinsic Susceptibility to Oxidation by HOCl. Arch. Biochem. Biophys. 2009, 487, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Khalil, A.; Jay-Gerin, J.P.; Fülöp, T. Age-Related Increased Susceptibility of High-Density Lipoproteins (HDL) to in Vitro Oxidation Induced by Gamma-Radiolysis of Water. FEBS Lett. 1998, 435, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Miura, K.; Arai, N.; Goka, R.; Morimoto, N.; Watanabe, S.; Isoda, N.; Yamamoto, H.; Kotani, K. Oxidized High-Density Lipoprotein Shows a Stepwise Increase as Fibrosis Progresses in Patients with Nonalcoholic Fatty Liver Disease. Antioxidants 2021, 10, 239. [Google Scholar] [CrossRef]
- Ichikawa, K.; Miyoshi, T.; Kotani, K.; Osawa, K.; Nakashima, M.; Nishihara, T.; Ito, H. Association between High Oxidized High-Density Lipoprotein Levels and Increased Pericoronary Inflammation Determined by Coronary Computed Tomography Angiography. J. Cardiol. 2022, 80, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.J.; Shapiro, J.I.; Thompson, E.; Singh, S.; Liu, L.; Weingarten, J.A.; O’Hanlon, K.; Bialczak, A.; Bhesania, S.R.; Abraham, N.G. Oxidized HDL, Adipokines, and Endothelial Dysfunction: A Potential Biomarker Profile for Cardiovascular Risk in Women with Obesity. Obesity 2019, 27, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.T.; Chen, Y.Y.; Mao, J.Y.; Wang, Y.P.; Chen, Y.F.; Hu, X.; Yang, K.; Liu, Y. Oxidized HDL, as a Novel Biomarker for Calcific Aortic Valve Disease, Promotes the Calcification of Aortic Valve Interstitial Cells. J. Cardiovasc. Transl. Res. 2019, 12, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Ansell, B.J.; Fonarow, G.C.; Fogelman, A.M. The Paradox of Dysfunctional High-Density Lipoprotein. Curr. Opin. Lipidol. 2007, 18, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Madoiwa, S. Recent Advances in Disseminated Intravascular Coagulation: Endothelial Cells and Fibrinolysis in Sepsis-Induced DIC. J. Intensive. Care 2015, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Prado, Y.; Pérez, L.; Eltit, F.; Echeverria, C.; Llancalahuen, F.M.; Tapia, P.; González, P.A.; Kalergis, A.M.; Cabello-Verrugio, C.; Simon, F. Procoagulant Phenotype Induced by Oxidized High-Density Lipoprotein Associates with Acute Kidney Injury and Death. Thromb. Res. 2023, 223, 7–23. [Google Scholar] [CrossRef]
- Walborn, A.; Rondina, M.; Mosier, M.; Fareed, J.; Hoppensteadt, D. Endothelial Dysfunction Is Associated with Mortality and Severity of Coagulopathy in Patients with Sepsis and Disseminated Intravascular Coagulation. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619852163. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.; Walborn, A.; Rondina, M.; Fareed, J.; Hoppensteadt, D. Markers of Inflammation and Infection in Sepsis and Disseminated Intravascular Coagulation. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619843338. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, I.; Mambo, N.; Ueda, T.; Nonaka, D.; Lee, L.-J.; Tanaka, K.; Kotani, J. New Biomarkers for Prediction of Disseminated Intravascular Coagulation in Patients With Sepsis. Clin. Appl. Thromb. Hemost. 2018, 24, 223S–229S. [Google Scholar] [CrossRef] [Green Version]
- Wada, H.; Thachil, J.; Nisio, M.D.; Mathew, P.; Kurosawa, S.; Gando, S.; Kim, H.K.; Nielsen, J.D.; Dempfle, C.-E.; Levi, M.; et al. Guidance for Diagnosis and Treatment of Disseminated Intravascular Coagulation from Harmonization of the Recommendations from Three Guidelines. J. Thromb. Haemost. 2013, 11, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Grafeneder, J.; Krychtiuk, K.A.; Buchtele, N.; Schoergenhofer, C.; Gelbenegger, G.; Lenz, M.; Wojta, J.; Heinz, G.; Huber, K.; Hengstenberg, C.; et al. The ISTH DIC Score Predicts Outcome in Non-Septic Patients Admitted to a Cardiovascular Intensive Care Unit. Eur. J. Intern. Med. 2020, 79, 37–42. [Google Scholar] [CrossRef]
- Mineo, C.; Shaul, P.W. Role of High-Density Lipoprotein and Scavenger Receptor B Type I in the Promotion of Endothelial Repair. Trends Cardiovasc. Med. 2007, 17, 156–161. [Google Scholar] [CrossRef]
- Valiyaveettil, M.; Kar, N.; Ashraf, M.Z.; Byzova, T.V.; Febbraio, M.; Podrez, E.A. Oxidized High-Density Lipoprotein Inhibits Platelet Activation and Aggregation via Scavenger Receptor BI. Blood 2008, 111, 1962–1971. [Google Scholar] [CrossRef]
- Barreto, J.; Karathanasis, S.K.; Remaley, A.; Sposito, A.C. Role of LOX-1 (Lectin-Like Oxidized Low-Density Lipoprotein Receptor 1) as a Cardiovascular Risk Predictor: Mechanistic Insight and Potential Clinical Use. Arter. Thromb. Vasc. Biol. 2021, 41, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, T.; Hokari, S.; Koyama, I.; Harada, T.; Komoda, T. NF-KB Activation in Endothelial Cells Treated with Oxidized High-Density Lipoprotein. Biochem. Biophys. Res. Commun. 2003, 303, 313–319. [Google Scholar] [CrossRef]
- Simon, F.; Fernández, R. Early Lipopolysaccharide-Induced Reactive Oxygen Species Production Evokes Necrotic Cell Death in Human Umbilical Vein Endothelial Cells. J. Hypertens. 2009, 27, 1202–1216. [Google Scholar] [CrossRef] [PubMed]
- Simon, F.; Stutzin, A. Protein Kinase C–Mediated Phosphorylation of P47phox Modulates Platelet-Derived Growth Factor–Induced H2O2 Generation and Cell Proliferation in Human Umbilical Vein Endothelial Cells. Endothelium 2009, 15, 175–188. [Google Scholar] [CrossRef]
- Ulevitch, R.J.; Johnston, A.R.; Weinstein, D.B. New Function for High Density Lipoproteins. Their Participation in Intravascular Reactions of Bacterial Lipopolysaccharides. J. Clin. Investig. 1979, 64, 1516–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prado, Y.; Tapia, P.; Eltit, F.; Reyes-Martínez, C.; Feijóo, C.G.; Llancalahuen, F.M.; Riedel, C.A.; Cabello-Verrugio, C.; Stehberg, J.; Simon, F. Sepsis-Induced Coagulopathy Phenotype Induced by Oxidized High-Density Lipoprotein Associated with Increased Mortality in Septic-Shock Patients. Antioxidants 2023, 12, 543. https://doi.org/10.3390/antiox12030543
Prado Y, Tapia P, Eltit F, Reyes-Martínez C, Feijóo CG, Llancalahuen FM, Riedel CA, Cabello-Verrugio C, Stehberg J, Simon F. Sepsis-Induced Coagulopathy Phenotype Induced by Oxidized High-Density Lipoprotein Associated with Increased Mortality in Septic-Shock Patients. Antioxidants. 2023; 12(3):543. https://doi.org/10.3390/antiox12030543
Chicago/Turabian StylePrado, Yolanda, Pablo Tapia, Felipe Eltit, Cristian Reyes-Martínez, Carmen G. Feijóo, Felipe M. Llancalahuen, Claudia A. Riedel, Claudio Cabello-Verrugio, Jimmy Stehberg, and Felipe Simon. 2023. "Sepsis-Induced Coagulopathy Phenotype Induced by Oxidized High-Density Lipoprotein Associated with Increased Mortality in Septic-Shock Patients" Antioxidants 12, no. 3: 543. https://doi.org/10.3390/antiox12030543