


An Interplay between Oxidative Stress (Lactate Dehydrogenase) and Inflammation (Anisocytosis) Mediates COVID-19 Severity Defined by Routine Clinical Markers
 ,
,  , , , , ,
, , , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Subjects
2.3. Data Collection
2.4. Statistical Analyses
3. Results
3.1. Clinical and Phenotypical Characterization of the Cohort
3.2. Exploration of the Role of Anisocytosis and LDH in COVID-19 Severity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An Interactive Web-Based Dashboard to Track COVID-19 in Real Time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Biancolella, M.; Colona, V.L.; Mehrian-Shai, R.; Watt, J.L.; Luzzatto, L.; Novelli, G.; Reichardt, J.K.V. COVID-19 2022 Update: Transition of the Pandemic to the Endemic Phase. Hum. Genom. 2022, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Galanopoulos, M.; Gkeros, F.; Doukatas, A.; Karianakis, G.; Pontas, C.; Tsoukalas, N.; Viazis, N.; Liatsos, C.; Mantzaris, G.J. COVID-19 Pandemic: Pathophysiology and Manifestations from the Gastrointestinal Tract. World J. Gastroenterol. 2020, 26, 4579–4588. [Google Scholar] [CrossRef]
- Loo, W.K.; Hasikin, K.; Suhaimi, A.; Yee, P.L.; Teo, K.; Xia, K.; Qian, P.; Jiang, Y.; Zhang, Y.; Dhanalakshmi, S.; et al. Systematic Review on COVID-19 Readmission and Risk Factors: Future of Machine Learning in COVID-19 Readmission Studies. Front. Public Health 2022, 10, 1311. [Google Scholar] [CrossRef] [PubMed]
- Daniels, N.F.; Burrin, C.; Chan, T.; Fusco, F. A Systematic Review of the Impact of the First Year of COVID-19 on Obesity Risk Factors: A Pandemic Fueling a Pandemic? Curr. Dev. Nutr. 2022, 6, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, M.; Kedarisetty, C.K. Cytokine Storm of COVID-19 and Its Impact on Patients with and without Chronic Liver Disease. J. Clin. Transl. Hepatol. 2021, 9, 256–264. [Google Scholar] [CrossRef]
- Hayden, M.R. An Immediate and Long-Term Complication of COVID-19 May Be Type 2 Diabetes Mellitus: The Central Role of β-Cell Dysfunction, Apoptosis and Exploration of Possible Mechanisms. Cells 2020, 9, 2475. [Google Scholar] [CrossRef]
- Martinez-Urbistondo, M.; Mora-Vargas, A.; Expósito-Palomo, E.; Castejón, R.; Citores, M.J.; Rosado, S.; De Mendoza, C.; Baños, I.; Fernández-Cruz, A.; Daimiel, L.; et al. Inflammatory-Related Clinical and Metabolic Outcomes in COVID-19 Patients. Mediat. Inflamm. 2020, 2020, 2914275. [Google Scholar] [CrossRef]
- Aalinezhad, M.; Alikhani, F.; Akbari, P.; Rezaei, M.H.; Soleimani, S.; Hakamifard, A. The Relationship between CT Severity Score and Capillary Blood Oxygen Saturation in Patients with COVID-19 Infection. Indian J. Crit. Care Med. 2021, 25, 279–283. [Google Scholar] [CrossRef]
- Choi, K.J.; Hong, H.L.; Kim, E.J. The Association between Mortality and the Oxygen Saturation and Fraction of Inhaled Oxygen in Patients Requiring Oxygen Therapy Due to COVID-19–Associated Pneumonia. Tuberc. Respir. Dis. 2021, 84, 125–133. [Google Scholar] [CrossRef]
- Laforge, M.; Elbim, C.; Frère, C.; Hémadi, M.; Massaad, C.; Nuss, P.; Benoliel, J.J.; Becker, C. Tissue Damage from Neutrophil-Induced Oxidative Stress in COVID-19. Nat. Rev. Immunol. 2020, 20, 515–516. [Google Scholar] [CrossRef]
- Beltrán-García, J.; Osca-Verdegal, R.; Pallardó, F.V.; Ferreres, J.; Rodríguez, M.; Mulet, S.; Sanchis-Gomar, F.; Carbonell, N.; García-Giménez, J.L. Oxidative Stress and Inflammation in COVID-19-Associated Sepsis: The Potential Role of Anti-Oxidant Therapy in Avoiding Disease Progression. Antioxidants 2020, 9, 936. [Google Scholar] [CrossRef]
- Jensen, I.J.; McGonagill, P.W.; Berton, R.R.; Wagner, B.A.; Silva, E.E.; Buettner, G.R.; Griffith, T.S.; Badovinac, V.P. Prolonged Reactive Oxygen Species Production Following Septic Insult. ImmunoHorizons 2021, 5, 477–488. [Google Scholar] [CrossRef]
- Hirano, T. IL-6 in Inflammation, Autoimmunity and Cancer. Int. Immunol. 2021, 33, 127–148. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 Infection: An Overview on Cytokine Storm and Related Interventions. Virol. J. 2022, 19, 1–15. [Google Scholar] [CrossRef]
- Melo, A.K.G.; Milby, K.M.; Caparroz, A.L.M.A.; Pinto, A.C.P.N.; Santos, R.R.P.; Rocha, A.P.; Ferreira, G.A.; Souza, V.A.; Valadares, L.D.A.; Vieira, R.M.R.A.; et al. Biomarkers of Cytokine Storm as Red Flags for Severe and Fatal COVID-19 Cases: A Living Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, 1–21. [Google Scholar] [CrossRef]
- Al-Jassas, H.K.; Al-Hakeim, H.K.; Maes, M. Intersections between Pneumonia, Lowered Oxygen Saturation Percentage and Immune Activation Mediate Depression, Anxiety, and Chronic Fatigue Syndrome-like Symptoms Due to COVID-19: A Nomothetic Network Approach. J. Affect. Disord. 2020, 297, 233–245. [Google Scholar] [CrossRef]
- Karu, N.; Kindt, A.; Van Gammeren, A.J.; Ermens, A.A.M.; Harms, A.C.; Portengen, L.; Vermeulen, R.C.H.; Dik, W.A.; Langerak, A.W.; Van der Velden, V.H.J.; et al. Severe COVID-19 Is Characterised by Perturbations in Plasma Amines Correlated with Immune Response Markers, and Linked to Inflammation and Oxidative Stress. Metabolites 2022, 12, 618. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Al-Rubaye, H.T.; Al-Hadrawi, D.S.; Almulla, A.F.; Maes, M. Long-COVID Post-Viral Chronic Fatigue Syndrome and Affective Symptoms Are Associated with Oxidative Damage, Lowered Antioxidant Defenses and Inflammation: A Proof of Concept and Mechanism Study. Mol. Psychiatry 2022, 28, 1–15. [Google Scholar] [CrossRef]
- Singh, B.; Singh, S.; Bhatia, J.K.; Kapoor, R.; Bhatia, K. Role of Matrix Degradation, Oxidative Stress, Inflammation & Trace Elements in COVID-19 Patients: A Multivariate Study from India. Indian J. Clin. Biochem. 2022, 1–11. [Google Scholar] [CrossRef]
- Moro-García, M.A.; Mayo, J.C.; Sainz, R.M.; Alonso-Arias, R. Influence of Inflammation in the Process of T Lymphocyte Differentiation: Proliferative, Metabolic, and Oxidative Changes. Front. Immunol. 2018, 9, 339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Tsermpini, E.E.; Glamočlija, U.; Ulucan-Karnak, F.; Redenšek Trampuž, S.; Dolžan, V. Molecular Mechanisms Related to Responses to Oxidative Stress and Antioxidative Therapies in COVID-19: A Systematic Review. Antioxidants 2022, 11, 1609. [Google Scholar] [CrossRef] [PubMed]
- Bondia-Pons, I.; Ryan, L.; Martinez, J.A. Oxidative Stress and Inflammation Interactions in Human Obesity. J. Physiol. Biochem. 2012, 68, 701–711. [Google Scholar] [CrossRef]
- Keykavousi, K.; Nourbakhsh, F.; Abdollahpour, N.; Fazeli, F.; Sedaghat, A.; Soheili, V.; Sahebkar, A. A Review of Routine Laboratory Biomarkers for the Detection of Severe COVID-19 Disease. Int. J. Anal. Chem. 2022, 2022, 1–14. [Google Scholar] [CrossRef]
- Moreno-Torres, V.; Sánchez-Chica, E.; Castejón, R.; Caballero Bermejo, A.F.; Mills, P.; Diago-Sempere, E.; Rosado, S.; Sancho-López, A.; Vargas-Núñez, J.A.; Ruiz-Antorán, B.; et al. Red Blood Cell Distribution Width as a Marker of Hyperinflammation and Mortality in COVID-19. Ann. Palliat. Med. 2022, 11, 2609–2621. [Google Scholar] [CrossRef]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and High-Resolution CT Features of the COVID-19 Infection: Comparison of the Initial and Follow-up Changes. Investig. Radiol. 2020, 55, 332–339. [Google Scholar] [CrossRef]
- Mokwatsi, G.G.; Schutte, A.E.; Kruger, R.; Mokwatsi, G.G.; Schutte, A.E.; Kruger, R. A Biomarker of Tissue Damage, Lactate Dehydrogenase, Is Associated with Fibulin-1 and Oxidative Stress in Blacks: The SAfrEIC Study. Biomarkers 2016, 21, 48–55. [Google Scholar] [CrossRef]
- Hornick, A.; Tashtish, N.; Osnard, M.; Shah, B.; Bradigan, A.; Albar, Z.; Tomalka, J.; Dalton, J.; Sharma, A.; Sekaly, R.P.; et al. Anisocytosis Is Associated with Short-Term Mortality in COVID-19 and May Reflect Proinflammatory Signature in Uninfected Ambulatory Adults. Pathog. Immun. 2020, 5, 312–326. [Google Scholar] [CrossRef]
- Battaglini, D.; Lopes-Pacheco, M.; Castro-Faria-Neto, H.C.; Pelosi, P.; Rocco, P.R.M. Laboratory Biomarkers for Diagnosis and Prognosis in COVID-19. Front. Immunol. 2022, 13, 1–11. [Google Scholar] [CrossRef]
- Gibbs, D.V.; Shreenivas, S.S.; Hudock, K.M. Role of Acute Thrombosis in Coronavirus Disease 2019. Crit. Care Clin. 2022, 38, 491–504. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Anemia. Available online: https://www.who.int/es/health-topics/anaemia#tab=tab_1 (accessed on 1 November 2022).
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S.F. A Simple Noninvasive Index Can Predict Both Significant Fibrosis and Cirrhosis in Patients with Chronic Hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An Inexpensive and Accurate Marker of Fibrosis in HCV Infection. Comparison with Liver Biopsy and FibroTest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- San-Cristobal, R.; Martín-Hernández, R.; Ramos-Lopez, O.; Martinez-Urbistondo, D.; Micó, V.; Colmenarejo, G.; Fernandez, P.V.; Daimiel, L.; Martínez, J.A. Longwise Cluster Analysis for the Prediction of COVID-19 Severity within 72 h of Admission: COVID-DATA-SAVE-LIFES Cohort. J. Clin. Med. 2022, 11, 3327. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Del-Villar-Carrero, R.; Martinez-Urbistondo, D.; Cuevas-Sierra, A.; Ibañez-Sustacha, I.; Candela-Fernandez, A.; Dominguez-Calvo, A.; Ramos-Lopez, O.; Vargas, J.A.; Reglero, G.; Villares-Fernandez, P.; et al. Hematological-and Immunological-Related Biomarkers to Characterize Patients with COVID-19 from Other Viral Respiratory Diseases. J. Clin. Med. 2022, 11, 3578. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; San-Cristobal, R.; Martinez-Urbistondo, D.; Micó, V.; Colmenarejo, G.; Villares-Fernandez, P.; Daimiel, L.; Alfredo Martinez, J. Proinflammatory and Hepatic Features Related to Morbidity and Fatal Outcomes in COVID-19 Patients. J. Clin. Med. 2021, 10, 3112. [Google Scholar] [CrossRef]
- Arévalo-Lorido, J.C.; Carretero-Gómez, J.; Casas-Rojo, J.M.; Antón-Santos, J.M.; Melero-Bermejo, J.A.; López-Carmona, M.D.; Palacios, L.C.; Sanz-Cánovas, J.; Pesqueira-Fontán, P.M.; De La Peña-Fernández, A.A.; et al. The Importance of Association of Comorbidities on COVID-19 Outcomes: A Machine Learning Approach. Curr. Med. Res. Opin. 2022, 38, 501–510. [Google Scholar] [CrossRef]
- Sarkar, S.; Kannan, S.; Khanna, P.; Singh, A.K. Role of Red Blood Cell Distribution Width, as a Prognostic Indicator in COVID-19: A Systematic Review and Meta-Analysis. Rev. Med. Virol. 2022, 32, 1–10. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Sanchis-Gomar, F.; Picanza, A.; Lippi, G. Red Blood Cell Distribution Width: A Simple Parameter with Multiple Clinical Applications. Crit. Rev. Clin. Lab. Sci. 2015, 52, 86–105. [Google Scholar] [CrossRef]
- Tauffenberger, A.; Fiumelli, H.; Almustafa, S.; Magistretti, P.J. Lactate and Pyruvate Promote Oxidative Stress Resistance through Hormetic ROS Signaling. Cell Death Dis. 2019, 10, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Urbistondo, M.; Moreno-Torres, V.; Mora-Vargas, A.; Expósito-Palomo, E.; Castejón-Díaz, R.; Daimiel, L.; Ramos-Lopez, O.; San-Cristóbal, R.; Vargas, J.A.; Martínez, J.A. Interaction of ACEI Antihypertensive Agent’s Administration with the Inflammatory Status at Admission Concerning COVID-19 Clinical Stay Outcomes. Vascul. Pharmacol. 2022, 143, 106955. [Google Scholar] [CrossRef]
- Zendelovska, D.; Atanasovska, E.; Petrushevska, M.; Spasovska, K.; Stevanovikj, M.; Demiri, I.; Labachevski, N. Evaluation of Oxidative Stress Markers in Hospitalized Patients with Moderate and Severe COVID-19. Rom. J. Intern. Med. 2021, 59, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-N.; Gao, Y.; Wang, X.-T.; Li, N.-N.; Du, X.; Tang, Y.-J.; Lai, Q.-Q.; Chen, P.-F.; Yue, C.-S.; Wu, J.-H.; et al. Lymphocyte–C-Reactive Protein Ratio Can Differentiate Disease Severity of COVID-19 Patients and Serve as an Assistant Screening Tool for Hospital and ICU Admission. Front. Immunol. 2022, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.J.; Acosta, D.; Vassell, R.; Tang, J.; Khurana, S.; Weiss, C.D.; Golding, H.; Zaitseva, M. D-Dimer and CoV-2 Spike-Immune Complexes Contribute to the Production of PGE2 and Proinflammatory Cytokines in Monocytes. PLoS Pathog. 2022, 18, 1–20. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic Inflammation in the Etiology of Disease across the Life Span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Tiotiu, A.; Chong Neto, H.; Bikov, A.; Kowal, K.; Steiropoulos, P.; Labor, M.; Cherrez-Ojeda, I.; Badellino, H.; Emelyanov, A.; Garcia, R.; et al. Impact of the COVID-19 Pandemic on the Management of Chronic Noninfectious Respiratory Diseases. Expert Rev. Respir. Med. 2021, 15, 1035–1048. [Google Scholar] [CrossRef]
- Pérusse, L.; Jacob, R.; Drapeau, V.; Llewellyn, C.; Arsenault, B.J.; Bureau, A.; Labonté, M.È.; Tremblay, A.; Vohl, M.C. Understanding Gene-Lifestyle Interaction in Obesity: The Role of Mediation versus Moderation. Lifestyle Genom. 2022, 15, 67–76. [Google Scholar] [CrossRef]
- Monserrat-Mesquida, M.; Quetglas-Llabr, M.; Bouzas, C.; Mascar, C.M.; Casares, M.; Llompart, I.; Ugarriza, L.; Martínez, J.A.; Tur, J.A.; Sureda, A. Increased Adherence to the Mediterranean Diet after Lifestyle Intervention Improves Oxidative and Inflammatory Status in Patients with Non-Alcoholic Fatty Liver Disease. Antioxidants 2022, 11, 1440. [Google Scholar] [CrossRef]
- Subudhi, S.; Verma, A.; Patel, A.B.; Hardin, C.C.; Khandekar, M.J.; Lee, H.; McEvoy, D.; Stylianopoulos, T.; Munn, L.L.; Dutta, S.; et al. Comparing Machine Learning Algorithms for Predicting ICU Admission and Mortality in COVID-19. NPJ Digit. Med. 2021, 4, 1–7. [Google Scholar] [CrossRef]
- Fan, X.; Zhu, B.; Nouri-Vaskeh, M.; Jiang, C.; Feng, X.; Poulsen, K.; Baradaran, B.; Fang, J.; Ade, E.A.; Sharifi, A.; et al. Scores Based on Neutrophil Percentage and Lactate Dehydrogenase with or without Oxygen Saturation Predict Hospital Mortality Risk in Severe COVID-19 Patients. Virol. J. 2021, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, A.; Garg, A.; Vinod, P.K.; Priyakumar, U.D. Machine Learning Based Clinical Decision Support System for Early COVID-19 Mortality Prediction. Front. Public Health 2021, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Daimiel, L.; De Molina, A.R.; Martínez-Urbistondo, D.; Vargas, J.A.; Alfredo Martínez, J. Exploring Host Genetic Polymorphisms Involved in SARS-CoV Infection Outcomes: Implications for Personalized Medicine in COVID-19. Int. J. Genom. 2020, 2020, 6901217. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, A.R.; Ezzeldin, T.; Siddiqui, I.A.; Alzahrani, M.S.; Alghamdi, M.A.; Alotaibi, W.H.; Almutairi, M.Z.; Alqannas, N.K. Correlation of Racial Effect with Severity of Disease and In-Hospital Outcome in Individuals Diagnosed with COVID-19. Int. J. Clin. Pract. 2021, 75, 1–6. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variables | O2 Sat ≤ 94 (n = 958) | O2 Sat > 94 (n = 850) | p Value |
|---|---|---|---|
| Phenotypical Variables | |||
| Age (y) | 70 ± 0.5 | 66 ± 0.6 | <0.001 |
| Sex (n, %) | |||
| Male | 605 (63.2) | 479 (56.4) | 0.003 |
| Female | 353 (36.8) | 371 (43.6) | 0.17 |
| Days of hospitalization (d) | 9 ± 0.2 | 7 ± 0.2 | <0.001 |
| Biochemical Variables | |||
| Oxygen saturation (%) | 88 ± 0.2 | 96 ± 0.04 | <0.001 |
| Glucose (mg/dL) | 134 ± 2 | 120 ± 2 | <0.001 |
| Anisocytosis coefficient (%) | 13.1 ± 0.1 | 12.7 ± 0.1 | 0.001 |
| Prothrombin activity (s) | 72.4 ± 0.7 | 74.3 ± 0.8 | 0.06 |
| LDH (U/L) | 682.6 ± 12.1 | 529.6 ± 11.2 | <0.001 |
| D dimer (µg/mL) | 2576.7 ± 273.1 | 2095.5 ± 337.6 | <0.001 |
| AST (U/L) | 42.6 ± 1.9 | 36.9 ± 4.1 | <0.001 |
| ALT (U/L) | 51.5 ± 2.5 | 42.8 ± 5.6 | <0.001 |
| AST/ALT ratio | 1.5 ± 0.02 | 1.4 ± 0.03 | 0.04 |
| FIB—4 index | 3.1 ± 0.1 | 2.5 ± 0.1 | 0.001 |
| APRI index | 0.7 ± 0.02 | 0.6 ± 0.06 | 0.17 |
| C reactive protein (mg/L) | 129.8 ± 3.5 | 67.5 ± 2.9 | <0.001 |
| Platelets (×103/µL) | 226.7 ± 3.3 | 217.8 ± 3.4 | 0.09 |
| Creatinine (mg/dL) | 1.05 ± 0.02 | 1.00 ± 0.02 | 0.12 |
| Hemoglobin (g/dL) | 14.0 ±0.06 | 13.7 ± 0.07 | 0.02 |
| Eosinophils (×103/µL) | 0.03 ± 0.002 | 0.05 ± 0.01 | 0.03 |
| Leukocytes (×103/µL) | 8.3 ± 0.2 | 6.9 ± 0.1 | <0.001 |
| Lymphocytes (×103/µL) | 1.1 ± 0.03 | 1.3 ± 0.07 | 0.002 |
| Monocytes (×103/µL) | 0.62 ± 0.08 | 0.56 ± 0.01 | 0.52 |
| Neutrophils (×103/µL) | 6.5 ± 0.1 | 4.9 ± 0.1 | <0.001 |
| NLR | 8.6 ± 0.4 | 5.1 ± 0.2 | <0.001 |
| Variables of Comorbidities | |||
| Diabetes mellitus (%) | 142 (14.8) | 81 (9.5) | 0.001 |
| Cardiovascular disease (%) | 188 (19.6) | 131 (15.4) | 0.02 |
| Overweight and obesity (%) | 63 (6.5) | 35 (4.1) | 0.02 |
| Anemia (%) | 44 (4.6) | 40 (4.7) | 0.89 |
| Liver diseases (%) | 28 (2.9) | 24 (2.8) | 0.91 |
| Gastrointestinal diseases (%) | 121 (12.6) | 127 (14.9) | 0.14 |
| Dementia (%) | 106 (11.0) | 92 (10.8) | 0.89 |
| Endocrine diseases (%) | 344 (35.9) | 237 (27.8) | <0.001 |
| Other respiratory diseases (%) | 698 (72.8) | 451 (53.0) | <0.001 |
| Kidney diseases (%) | 121 (12.6) | 85 (10.0) | 0.08 |
| Hypertension (%) | 348 (36.2) | 226 (26.6) | <0.001 |
| Variables | Lymphocytes ≤ 1.05 (n = 982) | Lymphocytes >1.05 (n = 826) | p Value |
|---|---|---|---|
| Phenotypical Variables | |||
| Age (y) | 70 ± 0.5 | 65 ± 0.5 | <0.001 |
| Sex (n, %) | |||
| Male | 548 (55.8) | 592 (71.7) | 0.001 |
| Female | 434 (44.2) | 234 (28.3) | 0.002 |
| Days of hospitalization (d) | 8.9 ± 0.2 | 7.4 ± 0.1 | <0.001 |
| Oxygen saturation (%) | 91 ± 0.2 | 93 ± 0.2 | <0.001 |
| Biochemical Variables | |||
| Glucose (mg/dL) | 133 ± 1.6 | 123± 1.3 | <0.001 |
| Anisocytosis coefficient (%) | 13.1 ± 0.1 | 12.7 ± 0.1 | <0.001 |
| Prothrombin activity (s) | 72.0 ± 0.6 | 75.4 ± 0.6 | 0.002 |
| LDH (U/L) | 657.1 ± 11.2 | 578.9 ± 12.5 | <0.001 |
| D dimer (µg/mL) | 2504.6 ± 315.4 | 2311.5 ± 258.8 | 0.63 |
| AST (U/L) | 47.7 ± 1.3 | 47.2 ± 4.7 | 0.91 |
| ALT (U/L) | 39.9 ± 1.4 | 41.2 ± 3.4 | 0.72 |
| AST/ALT ratio | 1.5 ± 0.04 | 1.3 ± 0.02 | 0.002 |
| FIB—4 index | 3.2 ± 0.09 | 2.4 ± 0.1 | <0.001 |
| APRI index | 0.7 ± 0.02 | 0.6 ± 0.05 | 0.04 |
| C reactive protein (mg/L) | 128.1 ± 3.4 | 76.7 ± 2.8 | <0.001 |
| Platelets (×103/µL) | 207.7 ± 2.6 | 241.9 ± 3.4 | <0.001 |
| Creatinine (mg/dL) | 1.04 ± 0.02 | 0.99 ± 0.02 | 0.12 |
| Hemoglobin (g/dL) | 13.6 ± 0.06 | 14.0 ± 0.06 | <0.001 |
| Eosinophils (×103/µL) | 0.02 ± 0.001 | 0.06 ± 0.009 | <0.001 |
| Leukocytes (×103/µL) | 7.3 ± 0.1 | 7.9 ± 0.1 | 0.005 |
| Lymphocytes (×103/µL) | 0.7 ± 0.006 | 1.6 ± 0.05 | <0.001 |
| Monocytes (×103/µL) | 0.4 ± 0.008 | 0.7 ± 0.07 | <0.001 |
| Neutrophils (×103/µL) | 6.2 ± 0.1 | 5.4 ± 0.1 | <0.001 |
| NLR | 10.4 ± 0.4 | 3.7 ± 0.08 | <0.001 |
| Variables of Comorbidities | |||
| Diabetes mellitus (%) | 124 (12.6) | 156 (18.9) | 0.64 |
| Cardiovascular disease (%) | 191 (19.4) | 210 (25.4) | 0.03 |
| Overweight and obesity (%) | 56 (5.7) | 69 (8.3) | 0.67 |
| Anemia (%) | 56 (5.7) | 47 (5.7) | 0.01 |
| Liver diseases (%) | 32 (3.2) | 43 (5.2) | 0.95 |
| Gastrointestinal diseases (%) | 153 (15.6) | 153 (18.5) | 0.87 |
| Dementia (%) | 112 (11.4) | 130 (15.7) | 0.27 |
| Endocrine diseases (%) | 333 (33.9) | 379 (45.9) | 0.01 |
| Other respiratory diseases (%) | 646 (65.8) | 739 (89.4) | <0.001 |
| Kidney diseases (%) | 126 (12.8) | 132 (15.9) | 0.04 |
| Hypertension (%) | 341 (34.7) | 381 (46.1) | 0.04 |
| Variables | D-Dimer ≤ 743 | D-Dimer > 743 | p Value |
|---|---|---|---|
| (n = 723) | (n = 1085) | ||
| Phenotypical Variables | |||
| Age (y) | 64 ± 0.5 | 72 ± 0.5 | <0.001 |
| Sex (n, %) | |||
| Male | 456 (63.1) | 417 (38.4) | 0.23 |
| Female | 267 (36.9) | 668 (61.6) | 0.001 |
| Days of hospitalization (d) | 7.7 ± 0.2 | 8.3 ± 0.2 | 0.03 |
| Oxygen saturation (%) | 93 ± 0.2 | 90 ± 0.3 | <0.001 |
| Biochemical Variables | |||
| Glucose (mg/dL) | 123.7 ± 1.7 | 133± 1.9 | <0.001 |
| Anisocytosis coefficient (%) | 12.4 ± 0.1 | 13.1 ± 0.1 | <0.001 |
| Prothrombin activity (s) | 73.2 ± 0.8 | 73.8 | 0.62 |
| LDH (U/L) | 550.2 ± 7.6 | 712.5 | <0.001 |
| D dimer (µg/mL) | 460 ± 6.1 | 4362.9 ± 395.4 | <0.001 |
| AST (U/L) | 41.7 ± 1.2 | 54.9 ± 5.8 | 0.02 |
| ALT (U/L) | 39.5 ± 1.7 | 43.7 ± 4.1 | 0.34 |
| AST/ALT ratio | 1.3 ± 0.02 | 1.6 ± 0.05 | <0.001 |
| FIB—4 index | 2.4 ± 0.1 | 3.1 ± 0.1 | <0.001 |
| APRI index | 0.5 ± 0.02 | 0.7 ± 0.06 | 0.07 |
| C reactive protein (mg/L) | 85.6 ± 3.1 | 132.2± 4.3 | <0.001 |
| Platelets (×103/µL) | 218.2 ± 3.1 | 245.5 ± 4.1 | <0.001 |
| Creatinine (mg/dL) | 0.9 ± 0.01 | 1.1 ± 0.03 | <0.001 |
| Hemoglobin (g/dL) | 14.1 ± 0.06 | 13.5 ± 0.1 | <0.001 |
| Eosinophils (×103/µL) | 0.03 ± 0.002 | 0.05 ± 0.01 | 0.17 |
| Leukocytes (×103/µL) | 7.0 ± 0.1 | 8.5 ± 0.2 | <0.001 |
| Lymphocytes (×103/µL) | 1.2 ± 0.03 | 1.2 ± 0.06 | 0.66 |
| Monocytes (×103/µL) | 0.5 ± 0.01 | 0.6 ± 0.1 | 0.18 |
| Neutrophils (×103/µL) | 5.2 ± 0.1 | 6.6 ±0.1 | <0.001 |
| NLR | 5.9 ± 0.2 | 8.7 ± 0.6 | <0.001 |
| Variables of Comorbidities | |||
| Diabetes mellitus (%) | 210 (29.0) | 281 (25.9) | <0.001 |
| Cardiovascular disease (%) | 103 (14.2) | 158 (14.5) | 0.04 |
| Overweight and obesity (%) | 45 (6.2) | 34 (3.1) | 0.23 |
| Anemia (%) | 16 (2.2) | 40 (3.7) | 0.001 |
| Liver diseases (%) | 13 (1.8) | 26 (2.4) | 0.03 |
| Gastrointestinal diseases (%) | 114 (15.7) | 72 (6.6) | 0.002 |
| Dementia (%) | 49 (6.7) | 103 (9.5) | <0.001 |
| Endocrine diseases (%) | 224 (30.9) | 241 (22.2) | 0.22 |
| Other respiratory diseases (%) | 447 (61.8) | 480 (44.2) | 0.02 |
| Kidney diseases (%) | 48 (6.6) | 98 (9.0) | <0.001 |
| Hypertension (%) | 200 (27.7) | 263 (24.2) | <0.001 |
| Variables | NLR Ratio ≤ 4.5 (n = 973) | NLR Ratio > 4.5 (n = 835) | p Value a | LDH ≤ 544 (n = 869) | LDH > 544 (n = 939) | p Value b | Anisocytosis ≤ 12.8 (n = 936) | Anisocytosis > 12.8 (n = 872) | p Value c |
|---|---|---|---|---|---|---|---|---|---|
| Phenotypical Variables | |||||||||
| Age (y) | 64 ± 0.5 | 70 ± 0.4 | <0.001 | 66 ± 0.6 | 68 ± 0.4 | 0.002 | 65 ± 0.5 | 70 ± 0.4 | <0.001 |
| Sex (n, %) | |||||||||
| Male | 469 (48.2) | 671 (80.4) | <0.001 | 594 (68.4) | 549 (58.5) | 0.21 | 575 (61.5) | 597 (68.5) | 0.26 |
| Female | 504 (51.8) | 164 (19.6) | <0.001 | 275 (31.6) | 390 (41.5) | 0.02 | 361 (38.5) | 275 (31.5) | |
| Days of hospitalization (d) | 7.7 ± 0.2 | 8.3 ± 0.1 | 0.04 | 7.6 ± 0.2 | 8.3 ± 0.2 | 0.009 | 7.8 ± 0.2 | 8.6 ± 0.2 | 0.005 |
| Biochemical Variables | |||||||||
| Oxygen saturation (%) | 93 ± 0.1 | 90 ± 0.3 | <0.001 | 94 ± 0.1 | 89 ± 0.3 | <0.001 | 93 ± 0.2 | 91 ± 0.2 | <0.001 |
| Glucose (mg/dL) | 116 ± 1.0 | 139 ± 1.8 | <0.001 | 125 ± 1.5 | 130 ± 1.5 | 0.02 | 127 ± 2 | 128 ± 2 | 0.55 |
| Anisocytosis coefficient (%) | 12.6 ± 0.06 | 13.1 ± 0.07 | <0.001 | 12.6 ± 0.06 | 13.1 ± 0.06 | <0.001 | 11.3 ± 0.03 | 14.3 ± 0.05 | <0.001 |
| Prothrombin activity (s) | 77.5 ± 0.6 | 70.2 ± 0.6 | <0.001 | 76.4 ± 0.6 | 71.4 ± 0.6 | <0.001 | 75.0 ± 0.6 | 72.5 ± 0.7 | 0.006 |
| LDH (U/L) | 540.8± 10.3 | 694.2 ± 12.8 | <0.001 | 418.5 ± 2.6 | 817.7 ± 13.7 | <0.001 | 573.8 ± 8.2 | 656.0 ± 13.3 | <0.001 |
| D dimer (µg/mL) | 1301 ± 89 | 3447 ± 382 | <0.001 | 1406 ± 143 | 3209 ± 346 | <0.001 | 2039.4 ± 260.7 | 2651.5 ± 303.4 | 0.12 |
| AST (U/L) | 39.8 ± 1.3 | 54.7 ± 4.6 | 0.002 | 34.8 ± 4.3 | 58.5 ± 2.3 | <0.001 | 43.2 ± 1.1 | 51.5 ± 4.6 | 0.09 |
| ALT (U/L) | 35.5 ± 1.2 | 45.2 ± 3.6 | 0.008 | 32.3 ± 3.3 | 47.6 ± 1.9 | <0.001 | 38.5 ± 1.3 | 42.7 ± 3.4 | 0.25 |
| AST/ALT ratio | 1.4 ± 0.02 | 1.5 ± 0.04 | 0.01 | 1.3 ± 0.04 | 1.5 ± 0.02 | 0.001 | 1.4 ± 0.04 | 1.4 ± 0.02 | 0.39 |
| FIB—4 index | 2.6 ± 0.08 | 3.1 ± 0.1 | 0.001 | 2.3 ± 0.1 | 3.3 ± 0.09 | <0.001 | 2.4 ± 0.06 | 3.2 ± 0.1 | <0.001 |
| APRI index | 0.5 ± 0.02 | 0.7 ± 0.05 | 0.04 | 0.5 ± 0.05 | 0.7 ± 0.02 | <0.001 | 0.5 ± 0.02 | 0.7 ± 0.05 | 0.01 |
| C reactive protein (mg/L) | 56.5 ± 1.8 | 147.3 ± 3.6 | <0.001 | 65.7 ± 2.5 | 133.5 ± 3.4 | <0.001 | 95.7 ± 3.1 | 108.8 ± 3.4 | 0.005 |
| Platelets (×103/µL) | 214.0 ± 2.9 | 235.3 ± 3.2 | <0.001 | 222.8 ± 3.3 | 226.3 ± 2.9 | 0.43 | 234.4 ± 3.2 | 216.4 ± 3.0 | <0.001 |
| Creatinine (mg/dL) | 0.9 ± 0.01 | 1.1 ± 0.02 | <0.001 | 0.9 ± 0.02 | 1.1 ± 0.02 | 0.01 | 0.9 ± 0.01 | 1.1 ± 0.02 | <0.001 |
| Hemoglobin (g/dL) | 13.9 ± 0.05 | 13.6 ± 0.06 | <0.001 | 13.7 ± 0.06 | 13.9 ± 0.05 | 0.09 | 14.0 ± 0.05 | 13.6 ± 0.06 | <0.001 |
| Eosinophils (×103/µL) | 0.05 ± 0.009 | 0.02 ± 0.001 | <0.001 | 0.05 ± 0.009 | 0.02 ± 0.001 | <0.001 | 0.05 ± 0.009 | 0.04 ± 0.002 | 0.31 |
| Leukocytes (×103/µL) | 6.0 ± 0.1 | 9.2 ± 0.1 | <0.001 | 7.1 ± 0.1 | 8.1 ± 0.1 | <0.001 | 7.2 ± 0.1 | 8.1 ± 0.2 | <0.001 |
| Lymphocytes (×103/µL) | 1.5 ± 0.05 | 0.8 ± 0.01 | <0.001 | 1.3 ± 0.05 | 1.1 ± 0.02 | <0.001 | 1.2 ± 0.02 | 1.2 ± 0.05 | 0.72 |
| Monocytes (×103/µL) | 0.6 ± 0.07 | 0.5 ± 0.01 | 0.51 | 0.6 ± 0.01 | 0.6 ± 0.06 | 0.95 | 0.54 ± 0.01 | 0.62 ± 0.07 | 0.27 |
| Neutrophils (×103/µL) | 3.8 ± 0.05 | 7.8 ± 0.1 | <0.001 | 5.1 ± 0.1 | 6.3 ± 0.1 | <0.001 | 5.3 ± 0.1 | 6.2 ± 0.1 | <0.001 |
| NLR | 2.8 ± 0.03 | 11.3 ± 0.4 | <0.001 | 5.3 ± 0.2 | 8.4 ± 0.4 | <0.001 | 6.0 ± 0.2 | 8.0 ± 0.4 | <0.001 |
| Variables of Comorbidities | |||||||||
| Diabetes mellitus (%) | 116 (11.9) | 164 (19.6) | 0.51 | 117 (13.4) | 163 (17.3) | 0.22 | 97 (10.3) | 149 (17.1) | 0.004 |
| Cardiovascular disease (%) | 135 (13.8) | 266 (31.8) | 0.01 | 145 (16.7) | 256 (27.2) | 0.28 | 139 (14.8) | 218 (25.0) | <0.001 |
| Overweight and obesity (%) | 50 (5.1) | 75 (8.9) | 0.44 | 47 (5.4) | 78 (8.3) | 0.82 | 51 (5.4) | 58 (6.6) | 0.79 |
| Anemia (%) | 33 (3.4) | 70 (8.4) | 0.01 | 38 (4.3) | 65 (6.9) | 0.73 | 17 (1.8) | 69 (7.9) | <0.001 |
| Liver diseases (%) | 29 (2.9) | 46 (5.5) | 0.41 | 29 (3.3) | 46 (4.9) | 0.97 | 15 (1.6) | 45 (5.1) | <0.001 |
| Gastrointestinal diseases (%) | 138 (14.2) | 168 (20.1) | 0.49 | 134 (15.4) | 172 (18.3) | 0.04 | 128 (13.6) | 154 (17.6) | 0.34 |
| Dementia (%) | 97 (9.9) | 145 (17.3) | 0.28 | 85 (9.8) | 157 (16.7) | 0.25 | 96 (10.2) | 115 (13.2) | 0.44 |
| Endocrine diseases (%) | 297 (30.5) | 415 (49.7) | 0.31 | 278 (31.9) | 434 (46.2) | 0.72 | 275 (29.4) | 358 (41.0) | 0.005 |
| Other respiratory diseases (%) | 570 (58.6) | 815 (97.6) | 0.009 | 517 (59.5) | 868 (92.4) | 0.14 | 547 (58.4) | 682 (78.2) | <0.001 |
| Kidney diseases (%) | 87 (8.9) | 171 (20.5) | 0.001 | 100 (11.5) | 158 (16.8) | 0.93 | 77 (8.2) | 148 (16.9) | <0.001 |
| Hypertension (%) | 304 (31.2) | 418 (50.0) | 0.43 | 276 (31.7) | 446 (47.5) | 0.84 | 286 (30.5) | 364 (41.7) | 0.01 |
| Model (Oxygen Saturation as Dependent Variable) | ß Coefficient ± Standard Error | p Value | R Squared Adj. |
|---|---|---|---|
| 0.26 | |||
| Age (years) | −0.06 ± 0.01 | <0.001 | |
| Sex | 0.52 ± 0.34 | 0.13 | |
| Anisocytosis coefficient | −0.05 ± 0.11 | 0.63 | |
| NLR | −0.05 ± 0.01 | <0.001 | |
| CRP (mg/L) | −0.01 ± 0.001 | <0.001 | |
| LDH (U/L) | 2.81 ± 2.0 | 0.19 | |
| Other respiratory diseases | −1.5 ± 0.34 | <0.001 | |
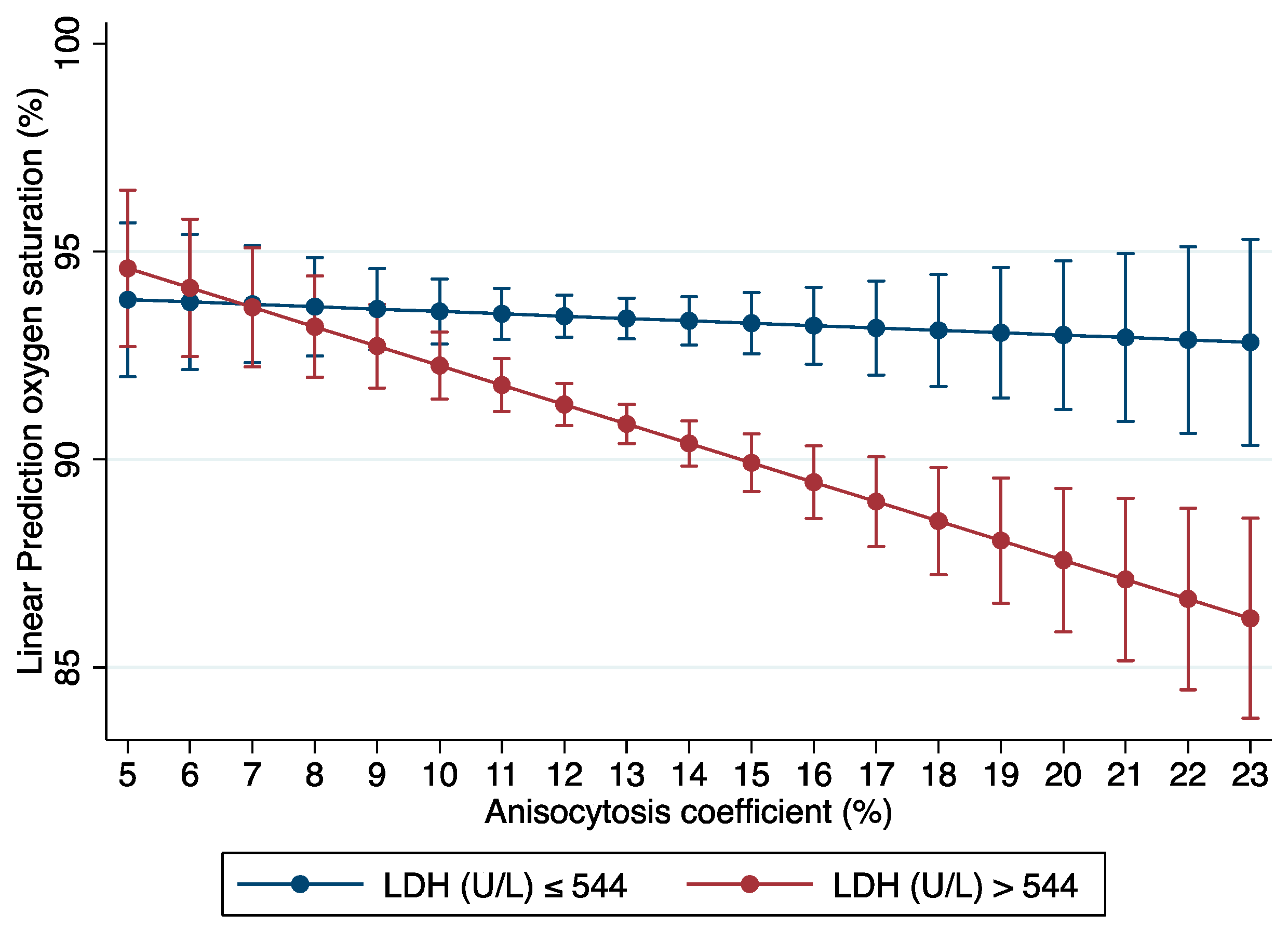
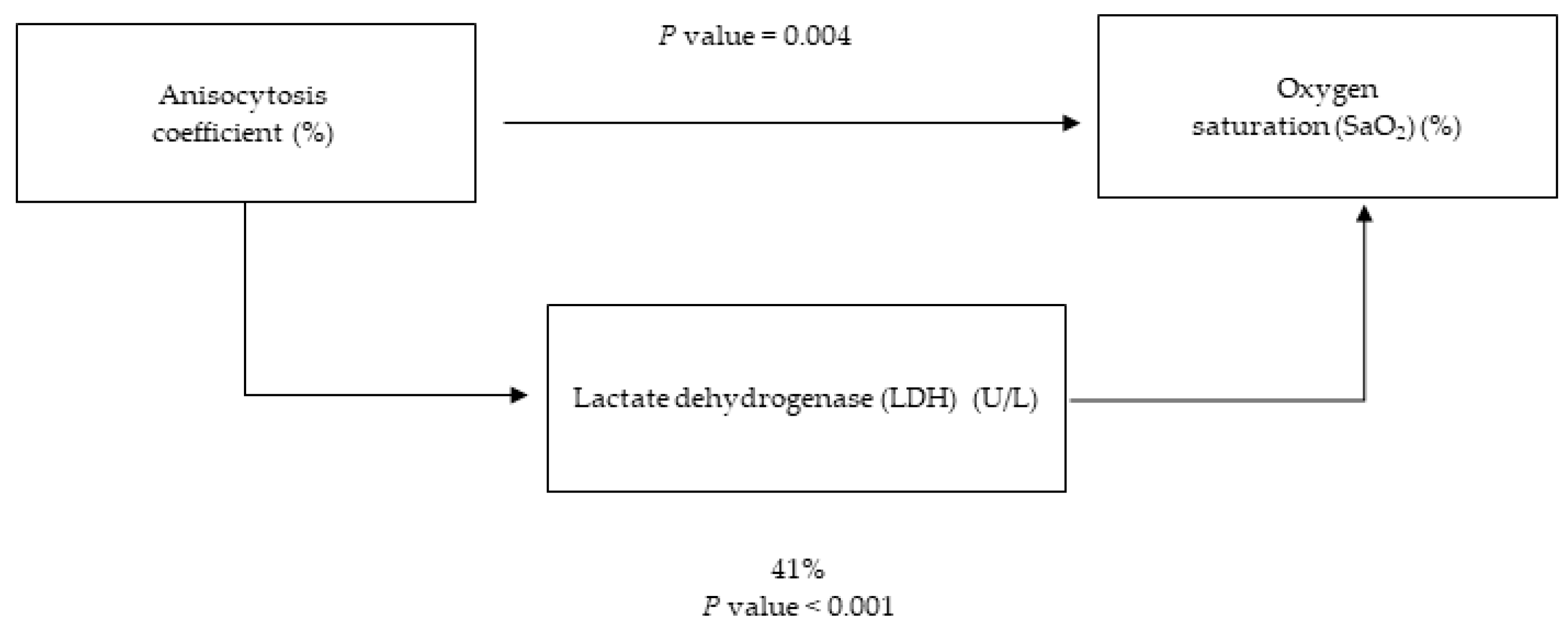
| Anisocytosis#LDH | 0.41± 0.16 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Bernáldez, M.; Cuevas-Sierra, A.; Micó, V.; Higuera-Gómez, A.; Ramos-Lopez, O.; Daimiel, L.; Dávalos, A.; Martínez-Urbistondo, M.; Moreno-Torres, V.; Ramirez de Molina, A.; et al. An Interplay between Oxidative Stress (Lactate Dehydrogenase) and Inflammation (Anisocytosis) Mediates COVID-19 Severity Defined by Routine Clinical Markers. Antioxidants 2023, 12, 234. https://doi.org/10.3390/antiox12020234
Alonso-Bernáldez M, Cuevas-Sierra A, Micó V, Higuera-Gómez A, Ramos-Lopez O, Daimiel L, Dávalos A, Martínez-Urbistondo M, Moreno-Torres V, Ramirez de Molina A, et al. An Interplay between Oxidative Stress (Lactate Dehydrogenase) and Inflammation (Anisocytosis) Mediates COVID-19 Severity Defined by Routine Clinical Markers. Antioxidants. 2023; 12(2):234. https://doi.org/10.3390/antiox12020234
Chicago/Turabian StyleAlonso-Bernáldez, Marta, Amanda Cuevas-Sierra, Víctor Micó, Andrea Higuera-Gómez, Omar Ramos-Lopez, Lidia Daimiel, Alberto Dávalos, María Martínez-Urbistondo, Víctor Moreno-Torres, Ana Ramirez de Molina, and et al. 2023. "An Interplay between Oxidative Stress (Lactate Dehydrogenase) and Inflammation (Anisocytosis) Mediates COVID-19 Severity Defined by Routine Clinical Markers" Antioxidants 12, no. 2: 234. https://doi.org/10.3390/antiox12020234