
Lipid Peroxidation Assessment in Preclinical Alzheimer Disease Diagnosis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sample Collection and Treatment
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
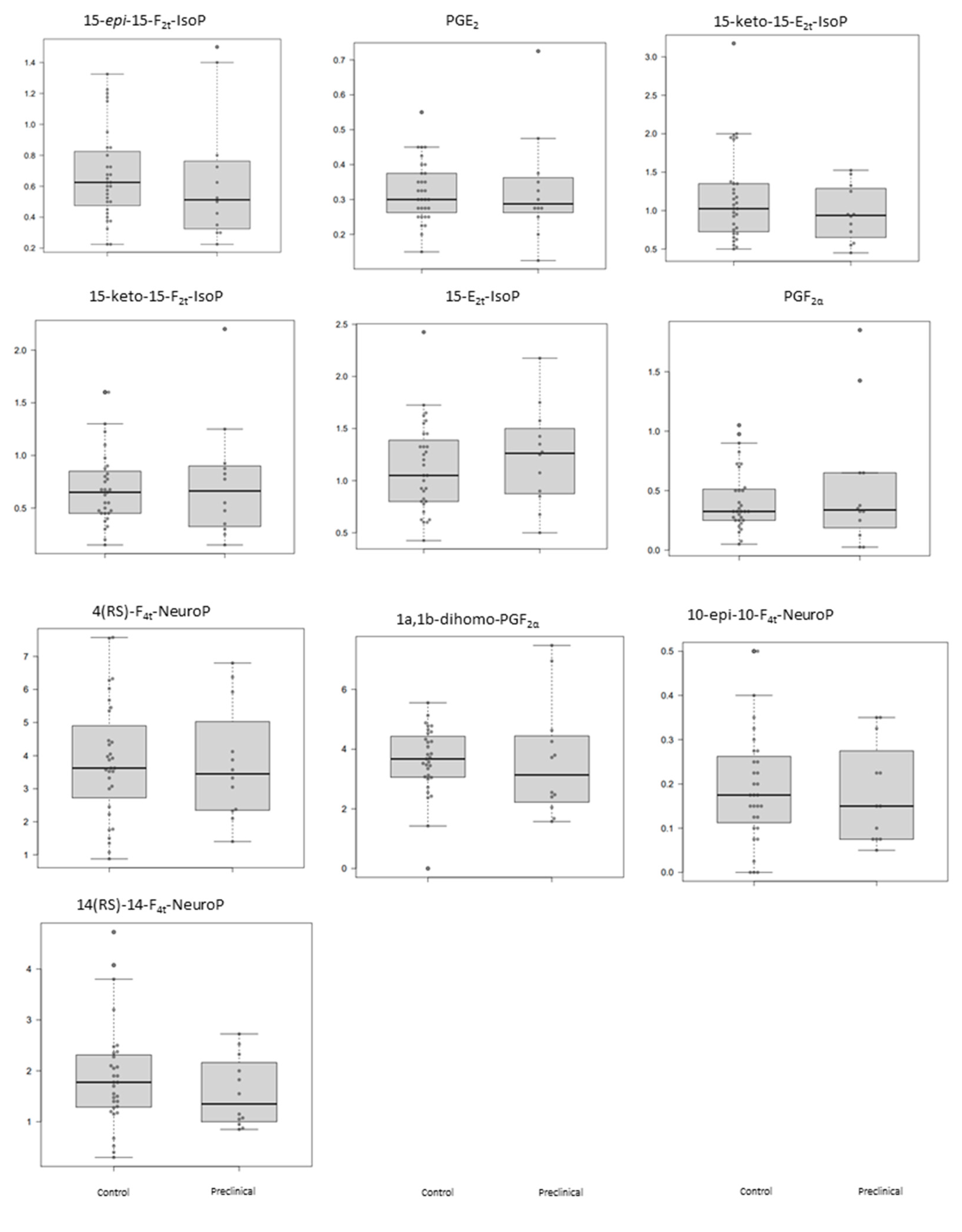
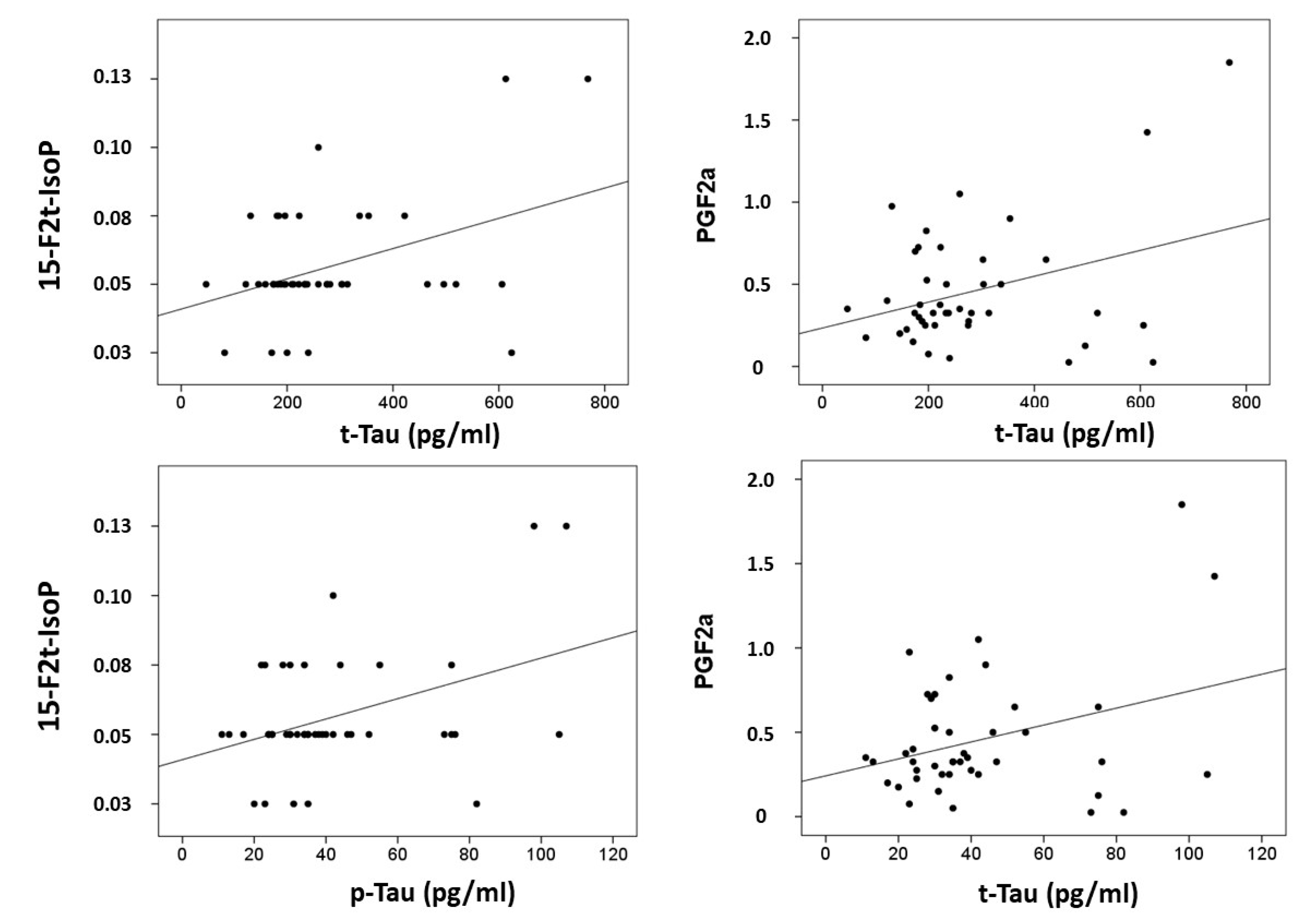
3.2. Plasma Levels of Lipid Peroxidation Lipid Compounds
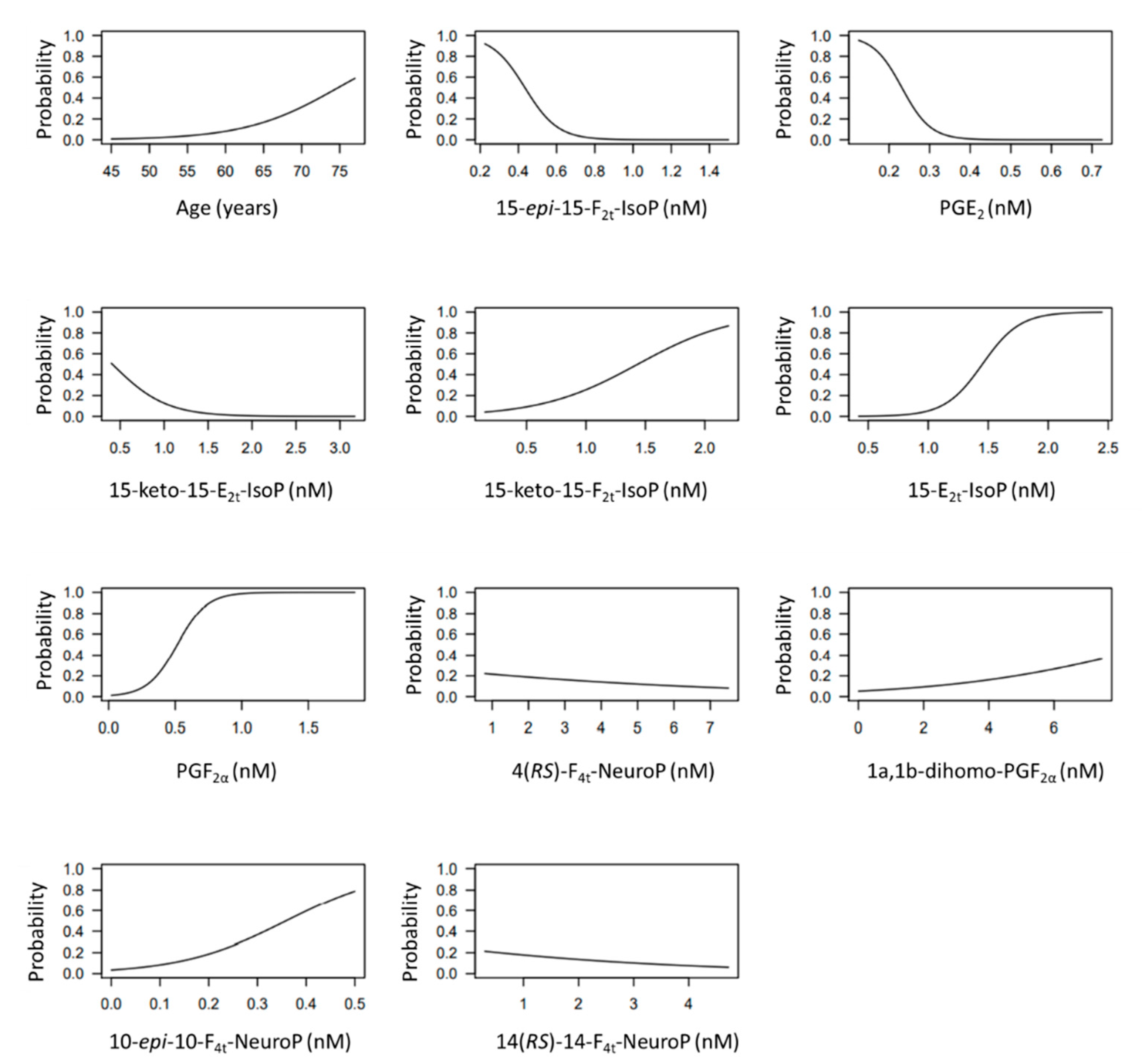
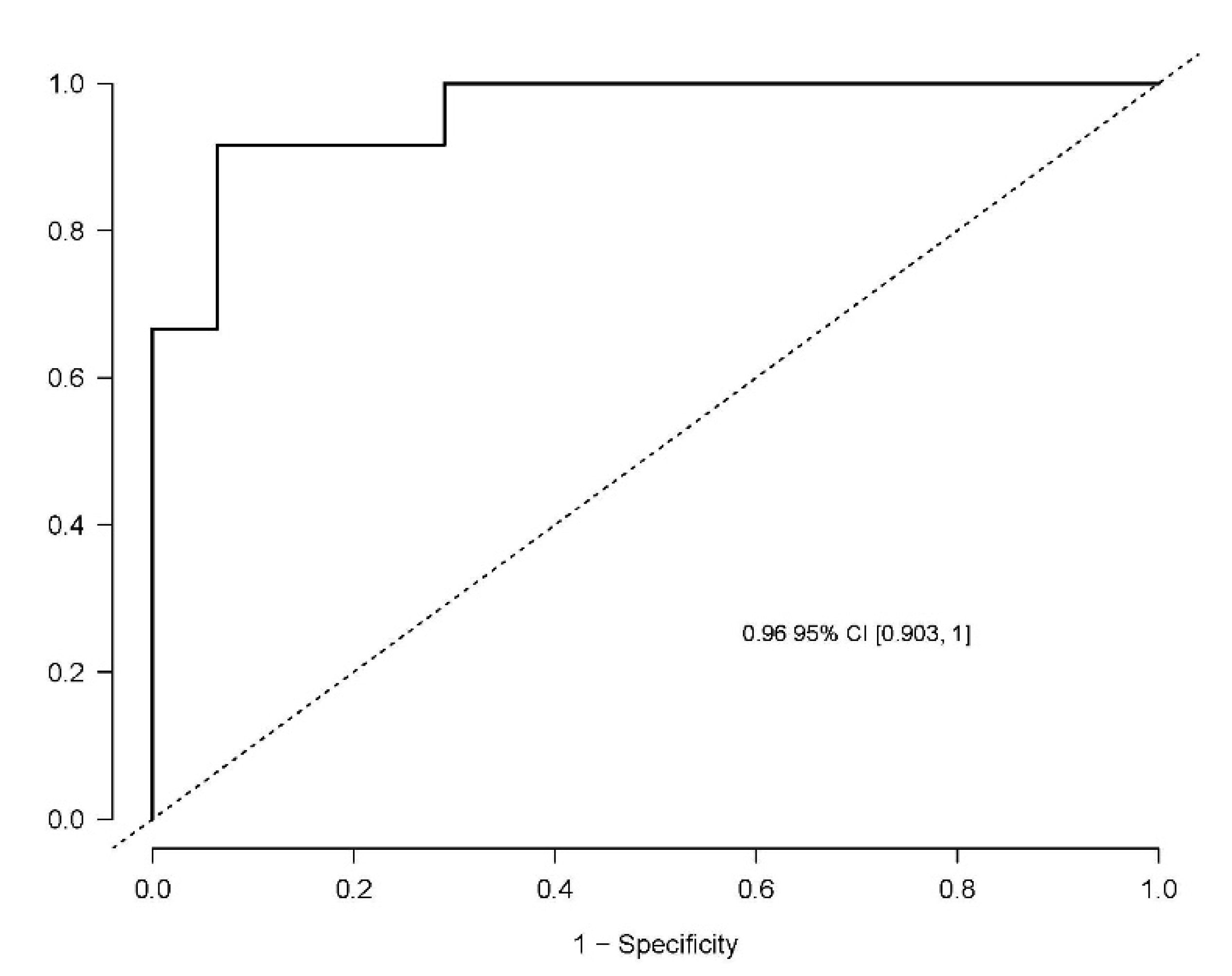
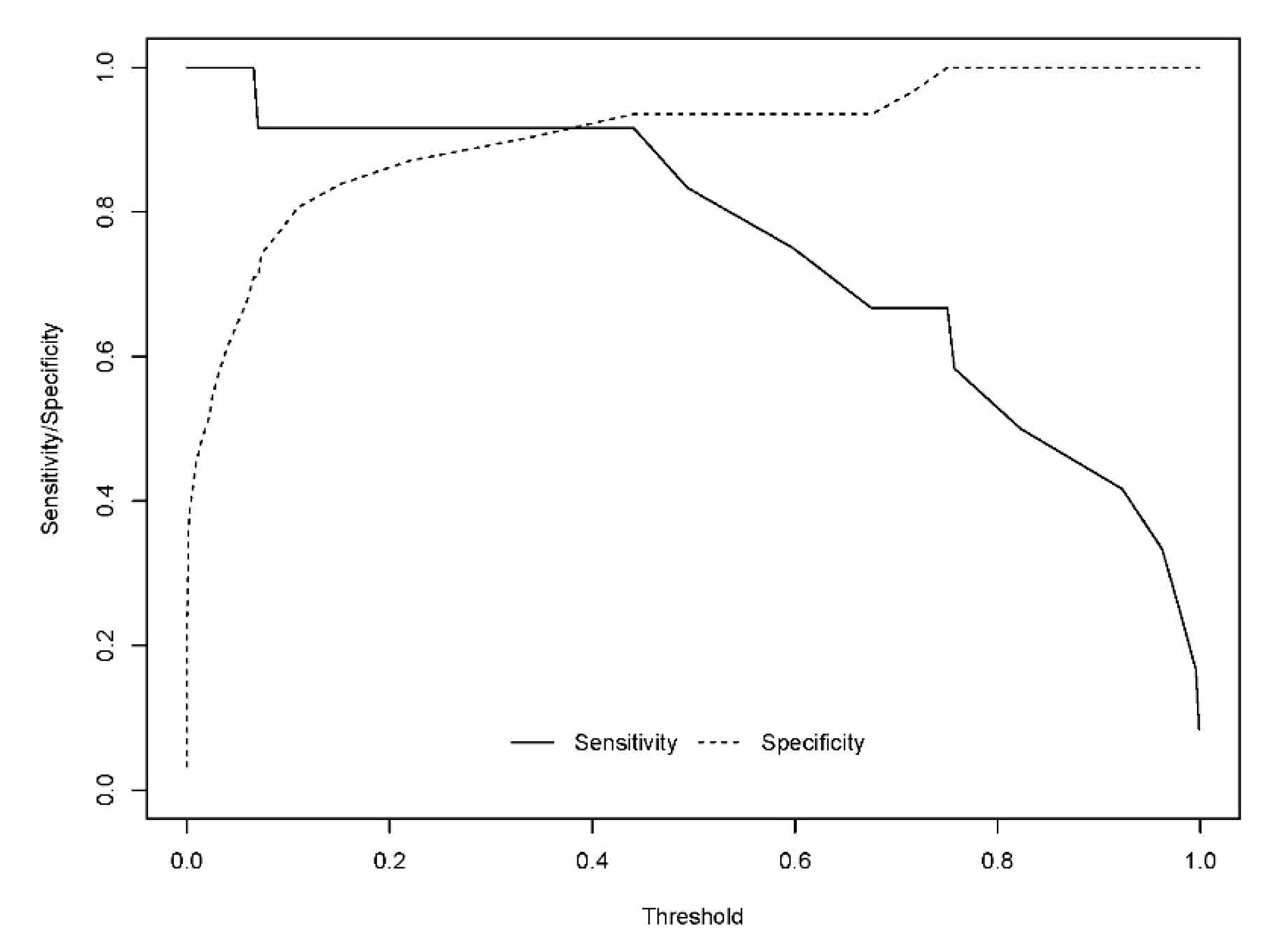
3.3. Potential Diagnosis Model
- A: 15-epi-15-F2t-IsoP
- B: PGE2
- C: 15-keto-15-E2t-IsoP
- D: 15-keto-15-F2t-IsoP
- E: 15-E2t-IsoP
- F: PGF2α
- G: 4(RS)-4-F4t-NeuroP
- H: 1a,1b-dihomo-PGF2α
- I: 10-epi-10-F4t-NeuroP
- J: 14(RS)-14-F4t-NeuroP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niedowicz, D.M.; Nelson, P.T.; Paul Murphy, M. Alzheimers Disease: Pathological Mechanisms and Recent Insights. Curr. Neuropharmacol. 2011, 9, 674–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheltens, P.; Blennow, K.; Breteler, M.M.B.; de Strooper, B.; Frisoni, G.B.; Salloway, S.; Van de Flier, W.M. Alzheimer’s disease. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- Hu, H.; Tan, L.; Bi, Y.-L.; Xu, W.; Tan, L.; Shen, X.-N.; Hou, X.-H.; Ma, Y.-H.; Dong, Q.; Yu, J.-T. Association between methylation of BIN1 promoter in peripheral blood and preclinical Alzheimer’s disease. Transl. Psychiatry 2021, 11, 89. [Google Scholar] [CrossRef]
- Keshavan, A.; Pannee, J.; Karikari, T.K.; Lantero Rodriguez, J.; Ashton, N.J.; Nicholas, J.M.; Cash, D.M.; Coath, W.; Lane, C.A.; Parker, T.D.; et al. Population-based blood screening for preclinical Alzheimer’s disease in a British birth cohort at age 70. Brain 2020, 144, 434–449. [Google Scholar] [CrossRef]
- Janelidze, S.; Berron, D.; Smith, R.; Strandberg, O.; Proctor, N.K.; Dage, J.L.; Stomrud, E.; Palmqvist, S.; Mattsson-Carlgren, N.; Hansson, O. Associations of Plasma Phospho-Tau217 Levels With Tau Positron Emission Tomography in Early Alzheimer Disease. JAMA Neurol. 2021, 78, 149. [Google Scholar] [CrossRef]
- Suárez-Calvet, M.; Karikari, T.K.; Ashton, N.J.; Gispert, J.D.; Salvado, G.; Fauria, K.; Shekari, M.; Grau-Rivera, O.; Stoops, E.; Blennow, K.; et al. Novel tau biomarkers phosphorylated at T181, T217 or T231 rise in the initial stages of the preclinical Alzheimer’s continuum when only subtle changes in Aβ pathology are detected. EMBO Mol. Med. 2020, 12, e12921. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.Y.; Maruff, P.; Kaneko, N.; Doecke, J.; Fowler, C.; Kato, T.; Rowe, C.C.; Arahata, Y.; Ito, K.; Masters, C.L.; et al. Plasma Amyloid-β Biomarker Associated with Cognitive Decline in Preclinical Alzheimer’s Disease. J. Alzheimer’s Dis. 2020, 77, 1057–1065. [Google Scholar] [CrossRef]
- Eruysal, E.; Ravdin, L.; Kamel, H.; Iadecola, C.; Ishii, M. Plasma lipocalin-2 levels in the preclinical stage of Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 646–653. [Google Scholar] [CrossRef]
- Fiandaca, M.S.; Zhong, X.; Cheema, A.K.; Orquiza, M.H.; Taan, M.T.; Gresenz, C.R.; Nalls, M.A.; Singleton, A.B.; Mapstone, M.; Chidambaram, S.; et al. Plasma 24-metabolite Panel Predicts Preclinical Transition to Clinical Stages of Alzheimer’s Disease. Front. Neurol. 2015, 6, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, L.; Zhu, M.; Kong, C.; Pang, Y.; Zhang, H.; Qiu, Q.; Wei, C.; Tang, Y.; Wang, Q.; Li, Y.; et al. Blood neuro-exosomal synaptic proteins predict Alzheimer’s disease at the asymptomatic stage. Alzheimer’s Dement. 2021, 17, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Goetzl, E.J.; Boxer, A.; Schwartz, J.B.; Abner, E.L.; Petersen, R.C.; Miller, B.L.; Kapogiannis, D. Altered lysosomal proteins in neural-derived plasma exosomes in preclinical Alzheimer disease. Neurology 2015, 85, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, A.L.; Walker, K.A.; Moghekar, A.R.; Pettigrew, C.; Soldan, A.; Albert, M.S.; Walston, J.D. Plasma Markers of Inflammation Linked to Clinical Progression and Decline During Preclinical AD. Front. Aging Neurosci. 2019, 11, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plascencia-Villa, G.; Perry, G. Preventive and Therapeutic Strategies in Alzheimer’s Disease: Focus on Oxidative Stress, Redox Metals, and Ferroptosis. Antioxid. Redox Signal. 2021, 34, 591–610. [Google Scholar] [CrossRef] [PubMed]
- García-Blanco, A.; Baquero, M.; Vento, M.; Gil, E.; Bataller, L.; Cháfer-Pericás, C. Potential oxidative stress biomarkers of mild cognitive impairment due to Alzheimer disease. J. Neurol. Sci. 2017, 373, 295–302. [Google Scholar] [CrossRef]
- Peña-Bautista, C.; Vento, M.; Baquero, M.; Cháfer-Pericás, C. Lipid peroxidation in neurodegeneration. Clin. Chim. Acta 2019, 497, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Chmatalova, Z.; Vyhnalek, M.; Laczo, J.; Hort, J.; Pospisilova, R.; Pechova, M.; Skoumalova, A. Relation of Plasma Selenium and Lipid Peroxidation End Products in Patients with Alzheimer’s Disease. Physiol. Res. 2017, 66, 1049–1056. [Google Scholar] [CrossRef]
- Montagne, A.; Zhao, Z.; Zlokovic, B.V. Alzheimer’s disease: A matter of blood-brain barrier dysfunction? J. Exp. Med. 2017, 214, 3151–3169. [Google Scholar] [CrossRef]
- Peña-Bautista, C.; Baquero, M.; Lopez-Nogueores, M.; Vento, M.; Hervas, D.; Cháfer-Pericás, C. Isoprostanoids Levels in Cerebrospinal Fluid Do Not Reflect Alzheimer’s Disease. Antioxidants 2020, 9, 407. [Google Scholar] [CrossRef]
- Peña-Bautista, C.; Vigor, C.; Galano, J.-M.; Oger, C.; Durand, T.; Ferrer, I.; Cuevas, A.; Vento, M.; Baquero, M.; Cháfer-Pericás, C.; et al. Plasma lipid peroxidation biomarkers for early and non-invasive Alzheimer Disease detection. Free Radic. Biol. Med. 2018, 124, 388–394. [Google Scholar] [CrossRef]
- Peña-Bautista, C.; Alvarez, L.; Baquero, M.; Ferrer, I.; Garcia, L.; Hervas-Marin, D.; Cháfer-Pericás, C. Plasma isoprostanoids assessment as Alzheimer’s disease progression biomarkers. J. Neurochem. 2020, 157, 2187–2194. [Google Scholar] [CrossRef]
- Hughes, C.P.; Berg, L.; Danziger, W.; Coben, L.A.; Martin, R.L. A New Clinical Scale for the Staging of Dementia. Br. J. Psychiatry 1982, 140, 566–572. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Peña-Bautista, C.; Avarez, L.; Durand, T.; Vigor, C.; Cuevas, A.; Baquero, M.; Vento, M.; Hervas, D.; Cháfer-Pericás, C. Clinical Utility of Plasma Lipid Peroxidation Biomarkers in Alzheimer’s Disease Differential Diagnosis. Antioxidants 2020, 9, 649. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Peña-Bautista, C.; Roca, M.; Hervas, D.; Cuevas, A.; Lopez-Cuevas, R.; Vento, M.; Baquero, M.; Garcia-Blanco, A.; Cháfer-Pericás, C. Plasma metabolomics in early Alzheimer’s disease patients diagnosed with amyloid biomarker. J. Proteom. 2019, 200, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Proitsi, P.; Kim, M.; Whiley, L.; Simmons, A.; Lupton, M.K.; Soininen, H.; Tsolaki, M.; Vellas, B.; Lovestone, S.; Powell, J.F.; et al. Association of blood lipids with Alzheimer’s disease: A comprehensive lipidomics analysis. Alzheimer’s Dement. 2017, 13, 140–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mapstone, M.; Cheema, A.K.; Fiandaca, M.S.; Zhong, X.; Mhyre, T.R.; Hall, W.J.; Fisher, S.G.; Peterson, D.R.; Haley, J.M.; Tan, M.T.; et al. Plasma phospholipids identify antecedent memory impairment in older adults. Nat. Med. 2014, 20, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Elmi, M.; Goozee, K.; Shah, T.; Sohrabi, H.R.; Dias, C.B.; Pedrini, S.; Shen, K.; Asih, P.R.; Dave, P.; et al. Ultrasensitive Detection of Plasma Amyloid-β as a Biomarker for Cognitively Normal Elderly Individuals at Risk of Alzheimer’s Disease. J. Alzheimer’s Dis. 2019, 71, 775–783. [Google Scholar] [CrossRef] [Green Version]
- Hilal, S.; Wolters, F.J.; Verbeek, M.M.; Vanderstichele, H.; Ikram, M.K.; Stoopes, E.; Ikram, M.A.; Vernooij, M.W. Plasma amyloid-β levels, cerebral atrophy and risk of dementia: A population-based study. Alzheimer’s Res. Ther. 2018, 10, 63. [Google Scholar] [CrossRef]
- Lövheim, H.; Elgh, F.; Johansson, A.; Zetterberg, H.; Blennow, K.; Hallmans, G.; Eriksson, S. Plasma concentrations of free amyloid β cannot predict the development of Alzheimer’s disease. Alzheimer’s Dement. 2017, 13, 778–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karikari, T.K.; Benedet, A.L.; Ashton, N.J.; Rodriguez, J.L.; Snellman, A.; Lussier, F.; Rial, A.M.; Pascoal, T.A.; Andeasson, U.; Blennow, K.; et al. Diagnostic performance and prediction of clinical progression of plasma phospho-tau181 in the Alzheimer’s Disease Neuroimaging Initiative. Mol. Psychiatry 2021, 26, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Wang, M.; Li, J.-L.; Cairns, N.J.; Han, X. Specific changes of sulfatide levels in individuals with pre-clinical Alzheimer’s disease: An early event in disease pathogenesis. J. Neurochem. 2013, 127, 733–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Shen, X.N.; Xu, W.; Huang, Y.-Y.; Li, H.-Q.; Tan, L.; Dong, Q.; Tan, L.; Yu, Y.-T. A panel of blood lipids associated with cognitive performance, brain atrophy, and Alzheimer’s diagnosis: A longitudinal study of elders without dementia. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12041. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Assessment | Classification of Participants | |
|---|---|---|
| Control | Preclinical AD | |
| RBANS.DM 1 | ≥85 | ≥85 |
| FAQ 2 | <9 | <9 |
| CDR 3 | 0-0.5 | 0–0.5 |
| MMSE 4 | ≥27 | ≥27 |
| CSF t-tau (pg mL−1) | <485 | >485 |
| CSF p-tau (pg mL−1) | <56 | >56 |
| CSF β-amyloid42 (pg mL−1) | >725 | <725 |
| CSF t-tau/β-amyloid42 | <0.51 | >0.51 |
| Variable | Control Group (n = 31) Median (1st, 3rd Quartile) | Preclinical Group (n = 12) Median (1st, 3rd Quartile) | |
|---|---|---|---|
| Age (years) | 62 (58.5, 67) | 70 (60.75, 74) | |
| Gender (Female, n (%)) | 19 (61.29%) | 6 (50%) | |
| Smoke (Yes, n (%)) | 6 (27.27%) | 1 (14.29%) | |
| Alcohol (Yes, n (%)) | 6 (27.27%) | 0 (0%) | |
| RBANS.DM (score) | 98 (94, 102) | 94.5 (87, 100.25) | |
| RBANS.A (score) | 91 (82, 98.5) | 85 (78, 91) | |
| RBANS.L (score) | 90 (83, 94) | 88.5 (82.5, 94.25) | |
| RBANS.VC (score) | 92 (84, 105) | 87 (75, 105) | |
| RBANS.IM (score) | 87 (83, 98.5) | 85 (81.75, 94) | |
| CDR (score) | 0.5 (0, 0.5) | 0.5 (0, 0.5) | |
| CSF β-amyloid-42 (pg mL−1) | 1224 (975.5, 1409.5) | 571.5 (407, 683.29) | |
| CSF t-tau (pg mL−1) | 212 (181.5, 259) | 443.5 (256.75, 607.75) | |
| CSF p-tau (pg mL−1) | 34 (26.5, 38.5) | 74 (40.75, 86) | |
| CSF t-tau/β-amyloid-42 | 0.18 (0.16–0.21) | 0.70 (0.51–0.97) | |
| FAQ (score) | 1 (0, 3.5) | 1 (0, 3) | |
| GDS (score) | 11 (5.5, 13) | 5 (3.75, 9) | |
| Educational level | Basic/primary | 10 (32.26%) | 4 (33.33%) |
| Secondary | 7 (22.58%) | 2 (16.67%) | |
| Universitary | 14 (45.16%) | 6 (50%) | |
| Medication (n, (%)) | |||
| Statins | 9 (40.91%) | 3 (42.86%) | |
| Fibrates | 0 (0%) | 1 (14.29%) | |
| Morphics | 0 (0%) | 0 (0%) | |
| ACEI | 1 (4.55%) | 0 (0%) | |
| Neuroleptics | 2 (9.09%) | 0 (0%) | |
| Benzodiazepines | 6 (27.27%) | 2 (28.57%) | |
| Antiepileptics | 1 (4.55%) | 0 (0%) | |
| Anticoagulants | 0 (0%) | 0 (0%) | |
| Antihipertensives | 7 (31.82%) | 2 (28.57%) | |
| Corticoids | 1 (4.55%) | 0 (0%) | |
| Anti-inflammatory | 3 (13.64%) | 0 (0%) | |
| Comorbidity (n, (%)) | |||
| Dyslipidemia | 11 (50%) | 3 (42.86%) | |
| Diabetes | 9 (40.91%) | 1 (14.29%) | |
| Hypertension | 8 (36.36%) | 2 (28.57%) | |
| Heart Disease | 1 (4.55%) | 0 (0%) | |
| Cerebrovascular | 1 (4.55%) | 0 (0%) | |
| Depression | 4 (18.18%) | 2 (28.57%) | |
| Anxiety | 3 (13.64%) | 2 (28.57%) | |
| Variable (nmol L−1) | Control (n = 31) | Preclinical (n = 12) | p Value |
|---|---|---|---|
| Median (1st, 3rd Quartile) | Median (1st, 3rd Quartile) | ||
| 15-epi-15-F2t-IsoP | 0.62 (0.48, 0.82) | 0.51 (0.34, 0.74) | 0.414 |
| PGE2 | 0.3 (0.26, 0.38) | 0.29 (0.27, 0.36) | 0.738 |
| 2,3-dinor-15-epi-15-F2t-IsoP | 0.03 (0, 0.03) | 0.03 (0.02, 0.03) | 0.602 |
| 15-keto-15-E2t-IsoP | 1.02 (0.72, 1.35) | 0.94 (0.69, 1.27) | 0.384 |
| 15-keto-15-F2t-IsoP | 0.65 (0.45, 0.85) | 0.66 (0.34, 0.89) | 0.926 |
| 15-E2t-IsoP | 1.05 (0.8, 1.39) | 1.26 (0.89, 1.46) | 0.478 |
| 5-F2t-IsoP | 2.75 (2.16, 3.19) | 2.35 (1.63, 2.9) | 0.414 |
| 15-F2t-IsoP | 0.05 (0.05, 0.05) | 0.05 (0.05, 0.07) | 0.430 |
| PGF2α | 0.32 (0.25, 0.51) | 0.34 (0.22, 0.65) | 0.968 |
| 4(RS)-4-F4t-NeuroP | 3.62 (2.72, 4.9) | 3.45 (2.36, 4.58) | 0.800 |
| 1a,1b-dihomo-PGF2α | 3.67 (3.06, 4.43) | 3.14 (2.31, 4.34) | 0.478 |
| 10-epi-10-F4t-NeuroP | 0.17 (0.11, 0.26) | 0.15 (0.07, 0.25) | 0.698 |
| 14(RS)-14-F4t-NeuroP | 1.77 (1.29, 2.31) | 1.35 (1.03, 2.08) | 0.355 |
| ent-7(RS)-7-F2t-dihomo-IsoP | 0 (0, 0) | 0 (0, 0.01) | 0.414 |
| 17-F2t-dihomo-IsoP | 0 (0, 0) | 0 (0, 0) | 1.000 |
| 17-epi-17-F2t-dihomo-IsoP | 0 (0, 0) | 0 (0, 0) | 1.000 |
| 17(RS)-10-epi-SC-Δ15-11-dihomo-IsoF | 0 (0, 0) | 0 (0, 0) | 0.679 |
| 7(RS)-ST-Δ8-11-dihomo-IsoF | 0 (0, 0.22) | 0 (0, 0) | 0.165 |
| Neurofurans | 0.27 (0.19, 0.37) | 0.24 (0.21, 0.41) | 0.679 |
| Isofurans | 0.52 (0.4, 0.65) | 0.5 (0.41, 0.69) | 0.718 |
| Dihomo-isoprostanes | 0.15 (0.14, 0.17) | 0.15 (0.13, 0.17) | 0.883 |
| Dihomo-isofurans | 0.01 (0.01, 0.02) | 0.01 (0.01, 0.02) | 0.883 |
| Neuroprostanes | 0.64 (0.49, 0.76) | 0.59 (0.45, 0.77) | 0.679 |
| Isoprostanes | 1.5 (1.25, 1.84) | 1.32 (1.14, 1.67) | 0.328 |
| Variables | Estimate | Exponential Estimate. (e Estimate) |
|---|---|---|
| (Intercept) | −6.566 | 0.001 |
| Gender (Females) | −0.153 | 0.858 |
| Age | 0.164 | 1.178 |
| 15-epi-15-F2t-IsoP | −11.622 | 0 |
| PGE2 | −28.241 | 0 |
| 15-keto-15-E2t-IsoP | −3.277 | 0.038 |
| 15-keto-15-F2t-IsoP | 2.457 | 11.671 |
| 15-E2t-IsoP | 6.391 | 596.158 |
| PGF2α | 8.988 | 8003.721 |
| 4(RS)-4-F4t-NeuroP | −0.174 | 0.841 |
| 1a,1b-dihomo-PGF2α | 0.315 | 1.371 |
| 10-epi-10-F4t-NeuroP | 9.289 | 10,823.421 |
| 14(RS)-14-F4t-NeuroP | −0.323 | 0.724 |
| Lambda | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña-Bautista, C.; Álvarez-Sánchez, L.; Ferrer, I.; López-Nogueroles, M.; Cañada-Martínez, A.J.; Oger, C.; Galano, J.-M.; Durand, T.; Baquero, M.; Cháfer-Pericás, C. Lipid Peroxidation Assessment in Preclinical Alzheimer Disease Diagnosis. Antioxidants 2021, 10, 1043. https://doi.org/10.3390/antiox10071043
Peña-Bautista C, Álvarez-Sánchez L, Ferrer I, López-Nogueroles M, Cañada-Martínez AJ, Oger C, Galano J-M, Durand T, Baquero M, Cháfer-Pericás C. Lipid Peroxidation Assessment in Preclinical Alzheimer Disease Diagnosis. Antioxidants. 2021; 10(7):1043. https://doi.org/10.3390/antiox10071043
Chicago/Turabian StylePeña-Bautista, Carmen, Lourdes Álvarez-Sánchez, Inés Ferrer, Marina López-Nogueroles, Antonio José Cañada-Martínez, Camille Oger, Jean-Marie Galano, Thierry Durand, Miguel Baquero, and Consuelo Cháfer-Pericás. 2021. "Lipid Peroxidation Assessment in Preclinical Alzheimer Disease Diagnosis" Antioxidants 10, no. 7: 1043. https://doi.org/10.3390/antiox10071043