
The Assessment of Multiplex PCR in Identifying Bacterial Infections in Patients Hospitalized with SARS-CoV-2 Infection: A Systematic Review


 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
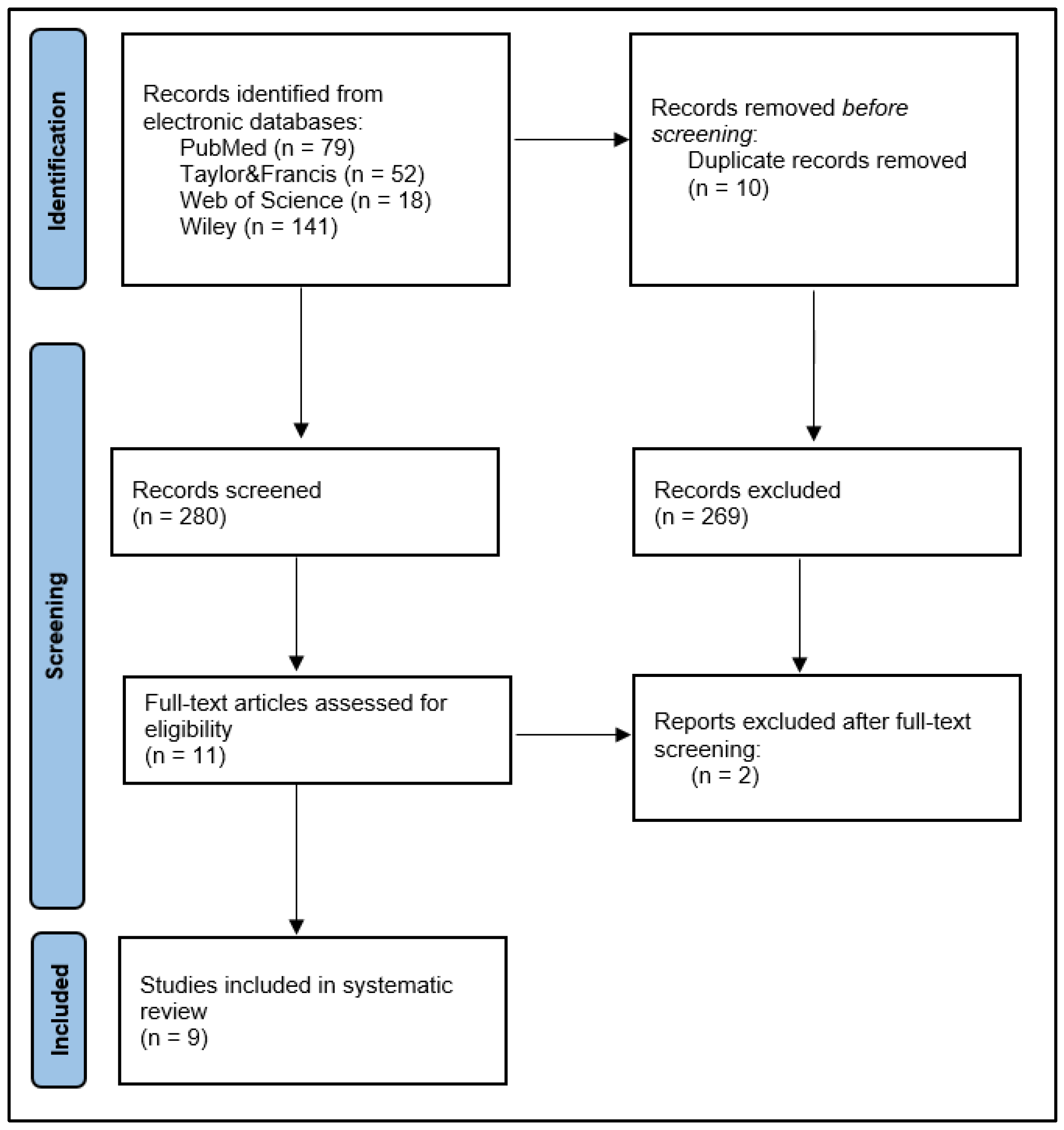
2. Materials and Methods
3. Results
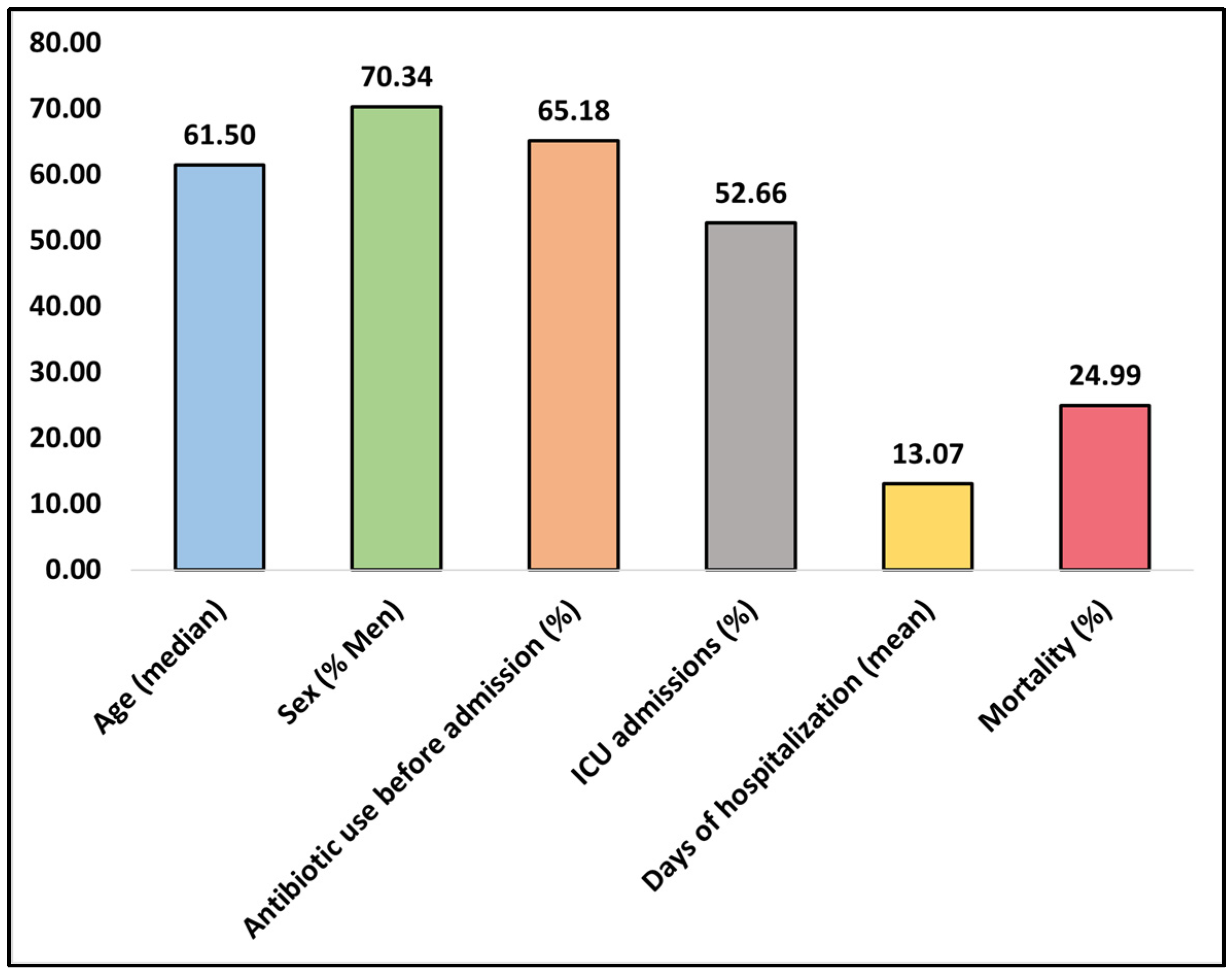
3.1. Study Characteristics and Clinical Outcomes
3.2. Bacterial Pathogen Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dao, T.L.; Hoang, V.T.; Colson, P.; Million, M.; Gautret, P. Co-Infection of SARS-CoV-2 and Influenza Viruses: A Systematic Review and Meta-Analysis. J. Clin. Virol. Plus 2021, 1, 100036. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://covid19.who.int (accessed on 23 December 2022).
- Citu, C.; Gorun, F.; Motoc, A.; Ratiu, A.; Gorun, O.M.; Burlea, B.; Neagoe, O.; Citu, I.M.; Rosca, O.; Bratosin, F.; et al. Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania. Diagnostics 2022, 12, 703. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-Infections in People with COVID-19: A Systematic Review and Meta-Analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Pilut, C.N.; Citu, C.; Gorun, F.; Bratosin, F.; Gorun, O.M.; Burlea, B.; Citu, I.M.; Grigoras, M.L.; Manolescu, D.; Gluhovschi, A. The Utility of Laboratory Parameters for Cardiac Inflammation in Heart Failure Patients Hospitalized with SARS-CoV-2 Infection. Diagnostics 2022, 12, 824. [Google Scholar] [CrossRef]
- Cerbu, B.; Grigoras, M.L.; Bratosin, F.; Bogdan, I.; Citu, C.; Bota, A.V.; Timircan, M.; Bratu, M.L.; Levai, M.C.; Marincu, I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. J. Clin. Med. 2022, 11, 652. [Google Scholar] [CrossRef]
- Sah, S.N.; Ghimire, A.; Sah, R.K.; Sah, P.K.; Caplash, N.; Sharma, P. Potential Lethal Co-Infections in COVID-19: A Study Based on Literature Review. Nepal J. Sci. Technol. 2021, 19, 125–129. [Google Scholar] [CrossRef]
- Citu, C.; Burlea, B.; Gorun, F.; Motoc, A.; Gorun, O.M.; Malita, D.; Ratiu, A.; Margan, R.; Grigoras, M.L.; Bratosin, F.; et al. Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania. J. Clin. Med. 2022, 11, 2831. [Google Scholar] [CrossRef]
- Stefanini, I.; De Renzi, G.; Foddai, E.; Cordani, E.; Mognetti, B. Profile of Bacterial Infections in COVID-19 Patients: Antimicrobial Resistance in the Time of SARS-CoV-2. Biology 2021, 10, 822. [Google Scholar] [CrossRef]
- Marincu, I.; Citu, C.; Bratosin, F.; Bogdan, I.; Timircan, M.; Gurban, C.V.; Bota, A.V.; Braescu, L.; Grigoras, M.L. Clinical Characteristics and Outcomes of COVID-19 Hospitalized Patients: A Comparison between Complete mRNA Vaccination Profile and Natural Immunity. J. Pers. Med. 2022, 12, 259. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and Outcomes of Co-Infection and Superinfection with SARS-CoV-2 and Other Pathogens: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, W.; Tang, Y.-W. Clinical Microbiology in Detection and Identification of Emerging Microbial Pathogens: Past, Present, and Future. Emerg. Microbes Infect. 2022, 11, 2579–2589. [Google Scholar] [CrossRef]
- Henegariu, O.; Heerema, N.A.; Dlouhy, S.R.; Vance, G.H.; Vogt, P.H. Multiplex PCR: Critical Parameters and Step-by-Step Protocol. BioTechniques 1997, 23, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Bahceci, I.; Yildiz, I.E.; Duran, O.F.; Soztanaci, U.S.; Harbawi, Z.K.; Senol, F.F.; Demiral, G. Secondary Bacterial Infection Rates Among Patients With COVID-19. Cureus 2022, 14, e22363. [Google Scholar] [CrossRef]
- Mohammadnejad, E.; Manshadi, S.A.D.; Mohammadi, M.T.B.; Abdollai, A.; Seifi, A.; Salehi, M.R.; Gheshlagh, R.G. Prevalence of nosocomial infections in COVID-19 patients admitted to the intensive care unit of Imam Khomeini complex hospital in Tehran. Iran. J. Microbiol. 2021, 13, 764–768. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Gao, Y.; Wang, X.; Liu, R.; Du, P.; Wang, X.; Zhang, X.; Lu, S.; Wang, Z.; Shi, Q.; et al. COVID-19 Evidence and Recommendations Working Group. Nosocomial infections among patients with COVID-19, SARS and MERS: A rapid review and meta-analysis. Ann. Transl. Med. 2020, 8, 629. [Google Scholar] [CrossRef] [PubMed]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502. [Google Scholar] [CrossRef]
- Elnifro, E.M.; Ashshi, A.M.; Cooper, R.J.; Klapper, P.E. Multiplex PCR: Optimization and Application in Diagnostic Virology. Clin. Microbiol. Rev. 2000, 13, 559–570. [Google Scholar] [CrossRef]
- Budea, C.M.; Pricop, M.; Bratosin, F.; Bogdan, I.; Saenger, M.; Ciorica, O.; Braescu, L.; Domuta, E.M.; Grigoras, M.L.; Citu, C.; et al. Antibacterial and Antifungal Management in Relation to the Clinical Characteristics of Elderly Patients with Infective Endocarditis: A Retrospective Analysis. Antibiotics 2022, 11, 956. [Google Scholar] [CrossRef]
- Panchali, M.J.L.; Oh, H.J.; Lee, Y.M.; Kim, C.M.; Tariq, M.; Seo, J.W.; Kim, D.Y.; Yun, N.R.; Kim, D.M. Accuracy of Real-Time Polymerase Chain Reaction in COVID-19 Patients. Microbiol. Spectr. 2022, 10, e0059121. [Google Scholar] [CrossRef]
- Manolescu, D.; Timar, B.; Bratosin, F.; Rosca, O.; Citu, C.; Oancea, C. Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study. Diagnostics 2022, 12, 1397. [Google Scholar] [CrossRef]
- Baldanti, F.; Ganguly, N.K.; Wang, G.; Möckel, M.; O’Neill, L.A.; Renz, H.; Dos Santos Ferreira, C.E.; Tateda, K.; Van Der Pol, B. Choice of SARS-CoV-2 diagnostic test: Challenges and key considerations for the future. Crit. Rev. Clin. Lab. Sci. 2022, 59, 445–459. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial Co-Infection, and Secondary Infection in Patients with COVID-19: A Living Rapid Review and Meta-Analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Teymouri, M.; Mollazadeh, S.; Mortazavi, H.; Naderi Ghale-Noie, Z.; Keyvani, V.; Aghababaei, F.; Hamblin, M.R.; Abbaszadeh-Goudarzi, G.; Pourghadamyari, H.; Hashemian, S.M.R.; et al. Recent advances and challenges of RT-PCR tests for the diagnosis of COVID-19. Pathol. Res. Pract. 2021, 221, 153443. [Google Scholar] [CrossRef]
- Markoulatos, P.; Siafakas, N.; Moncany, M. Multiplex polymerase chain reaction: A practical approach. J. Clin. Lab. Anal. 2002, 16, 47–51. [Google Scholar] [CrossRef]
- Lazic, I.; Feihl, S.; Prodinger, P.M.; Banke, I.J.; Trampuz, A.; von Eisenhart-Rothe, R.; Suren, C. Diagnostic accuracy of multiplex polymerase chain reaction on tissue biopsies in periprosthetic joint infections. Sci. Rep. 2021, 11, 19487. [Google Scholar] [CrossRef]
- Rakiro, J.; Shah, J.; Waweru-Siika, W.; Wanyoike, I.; Riunga, F. Microbial coinfections and superinfections in critical COVID-19: A Kenyan retrospective cohort analysis. IJID Reg. 2021, 1, 41–46. [Google Scholar] [CrossRef]
- Suranadi, I.W.; Sucandra, I.M.A.K.; Fatmawati, N.N.D.; Wisnawa, A.D.F. A Retrospective Analysis of the Bacterial Infections, Antibiotic Use, and Mortality Predictors of COVID-19 Patients. Int. J. Gen. Med. 2022, 15, 3591–3603. [Google Scholar] [CrossRef]
- Alqahtani, A.; Alamer, E.; Mir, M.; Alasmari, A.; Alshahrani, M.M.; Asiri, M.; Ahmad, I.; Alhazmi, A.; Algaissi, A. Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 2424. [Google Scholar] [CrossRef]
- Kwok, K.O.; Wei, W.I.; Ma, B.H.M.; Ip, M.; Cheung, H.; Hui, E.; Tang, A.; Mcneil, E.B.; Wong, S.Y.S.; Yeoh, E.K. Antibiotic use among COVID-19 patients in Hong Kong, January 2018 to March 2021. J. Infect. 2022, 84, e129–e132. [Google Scholar] [CrossRef]
- Mohamad, I.N.; Wong, C.K.; Chew, C.C.; Leong, E.L.; Lee, B.H.; Moh, C.K.; Chenasammy, K.; Lim, S.C.; Ker, H.B. The landscape of antibiotic usage among COVID-19 patients in the early phase of pandemic: A Malaysian national perspective. J. Pharm. Policy Pract. 2022, 15, 4. [Google Scholar] [CrossRef]
- Cong, W.; Stuart, B.; AIhusein, N.; Liu, B.; Tang, Y.; Wang, H.; Wang, Y.; Manchundiya, A.; Lambert, H. Antibiotic Use and Bacterial Infection in COVID-19 Patients in the Second Phase of the SARS-CoV-2 Pandemic: A Scoping Review. Antibiotics 2022, 11, 991. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Alosaimi, B.; Naeem, A.; Hamed, M.E.; Alkadi, H.S.; Alanazi, T.; Al Rehily, S.S.; Almutairi, A.Z.; Zafar, A. Influenza Co-Infection Associated with Severity and Mortality in COVID-19 Patients. Virol. J. 2021, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef]
- Cohen, R.; Babushkin, F.; Finn, T.; Geller, K.; Alexander, H.; Datnow, C.; Uda, M.; Shapiro, M.; Paikin, S.; Lellouche, J. High Rates of Bacterial Pulmonary Co-Infections and Superinfections Identified by Multiplex PCR among Critically Ill COVID-19 Patients. Microorganisms 2021, 9, 2483. [Google Scholar] [CrossRef]
- Foschi, C.; Zignoli, A.; Gaibani, P.; Vocale, C.; Rossini, G.; Lafratta, S.; Liberatore, A.; Turello, G.; Lazzarotto, T.; Ambretti, S. Respiratory Bacterial Co-Infections in Intensive Care Unit-Hospitalized COVID-19 Patients: Conventional Culture VS BioFire FilmArray Pneumonia plus Panel. J. Microbiol. Methods 2021, 186, 106259. [Google Scholar] [CrossRef]
- Huang, C.-P.; Tsai, C.-S.; Su, P.-L.; Huang, T.-H.; Ko, W.-C.; Lee, N.-Y. Respiratory Etiological Surveillance among Quarantined Patients with Suspected Lower Respiratory Tract Infection at a Medical Center in Southern Taiwan during COVID-19 Pandemic. J. Microbiol. Immunol. Infect. 2022, 55, 428–435. [Google Scholar] [CrossRef]
- Karolyi, M.; Pawelka, E.; Hind, J.; Baumgartner, S.; Friese, E.; Hoepler, W.; Neuhold, S.; Omid, S.; Seitz, T.; Traugott, M.T.; et al. Detection of Bacteria via Multiplex PCR in Respiratory Samples of Critically Ill COVID-19 Patients with Suspected HAP/VAP in the ICU. Wien. Klin. Wochenschr. 2021, 134, 385–390. [Google Scholar] [CrossRef]
- Maataoui, N.; Chemali, L.; Patrier, J.; Tran Dinh, A.; Le Fèvre, L.; Lortat-Jacob, B.; Marzouk, M.; d’Humières, C.; Rondinaud, E.; Ruppé, E.; et al. IMPACT OF RAPID Multiplex PCR on Management of Antibiotic Therapy in COVID-19-Positive Patients Hospitalized in Intensive Care Unit. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2227–2234. [Google Scholar] [CrossRef]
- Rothe, K.; Spinner, C.D.; Panning, M.; Pletz, M.W.; Rohde, G.; Rupp, J.; Witzenrath, M.; Erber, J.; Eberhardt, F.; Essig, A.; et al. Evaluation of a Multiplex PCR Screening Approach to Identify Community-Acquired Bacterial Co-Infections in COVID-19: A Multicenter Prospective Cohort Study of the German Competence Network of Community-Acquired Pneumonia (CAPNETZ). Infection 2021, 49, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Soto, A.; Quiñones-Laveriano, D.M.; Valdivia, F.; Juscamayta-López, E.; Azañero-Haro, J.; Chambi, L.; Horna, H.; Patiño, G.; Guzman, E.; De la Cruz-Vargas, J.A. Detection of Viral and Bacterial Respiratory Pathogens Identified by Molecular Methods in COVID-19 Hospitalized Patients and Its Impact on Mortality and Unfavorable Outcomes. Infect. Drug Resist. 2021, 14, 2795–2807. [Google Scholar] [CrossRef]
- Lai, C.C.; Wang, C.Y.; Hsueh, P.R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, E.D.; Feemster, K.; Rello, J. Protecting Adults at Risk of Pneumococcal Infection and Influenza from Exposure to SARS-CoV-2. Hum. Vaccines Immunother. 2021, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and Fungal Coinfection among Hospitalized Patients with COVID-19: A Retrospective Cohort Study in a UK Secondary-Care Setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of Co-Infections and Superinfections in Hospitalized Patients with COVID-19: A Retrospective Cohort Study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Allou, N.; Larsen, K.; Dubernet, A.; Traversier, N.; Masse, L.; Foch, E.; Bruneau, L.; Maillot, A.; André, M.; Lagrange-Xelot, M.; et al. Co-Infection in Patients with Hypoxemic Pneumonia Due to COVID-19 in Reunion Island. Medicine 2021, 100, e24524. [Google Scholar] [CrossRef]
- Caméléna, F.; Moy, A.-C.; Dudoignon, E.; Poncin, T.; Deniau, B.; Guillemet, L.; Le Goff, J.; Budoo, M.; Benyamina, M.; Chaussard, M.; et al. Performance of a Multiplex Polymerase Chain Reaction Panel for Identifying Bacterial Pathogens Causing Pneumonia in Critically Ill Patients with COVID-19. Diagn. Microbiol. Infect. Dis. 2021, 99, 115183. [Google Scholar] [CrossRef]
- Lapa, S.A.; Miftakhov, R.A.; Klochikhina, E.S.; Ammur, Y.I.; Blagodatskikh, S.A.; Shershov, V.E.; Zasedatelev, A.S.; Chudinov, A.V. Development of Multiplex RT-PCR with Immobilized Primers for Identification of Infectious Human Pneumonia Pathogens. Mol. Biol. 2021, 55, 828–838. [Google Scholar] [CrossRef]
- Sahajpal, N.S.; Mondal, A.K.; Ananth, S.; Njau, A.; Jones, K.; Ahluwalia, P.; Oza, E.; Ross, T.M.; Kota, V.; Kothandaraman, A.; et al. Clinical Validation of a Multiplex PCR-Based Detection Assay Using Saliva or Nasopharyngeal Samples for SARS-CoV-2, Influenza A and B. Sci. Rep. 2022, 12, 3480. [Google Scholar] [CrossRef]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-Infection with Respiratory Pathogens among COVID-2019 Cases. Virus Res. 2020, 285, 198005. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Country | Study Year | Study Design | Sample Size |
|---|---|---|---|---|
| 1. [35] Alosaimi, B.; Naeem, A.; Hamed, M. E.; Alkadi, H. S.; Alanazi, T.; Al Rehily, S. S.; Almutairi, A. Z.; Zafar, A. Influenza Co-Infection Associated with Severity and Mortality in COVID-19 Patients. Virology Journal 2021, 18 (1). | Saudi Arabia | 2021 | Retrospective observational | 48 |
| 2. [36] Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C. V.; Bota, A. V.; Turaiche, M.; Bratu, M. L.; Pilut, C. N.; Marincu, I. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11 (4), 437. | Romania | 2022 | Cross-sectional | 489 |
| 3. [37] Cohen, R.; Babushkin, F.; Finn, T.; Geller, K.; Alexander, H.; Datnow, C.; Uda, M.; Shapiro, M.; Paikin, S.; Lellouche, J. High Rates of Bacterial Pulmonary Co-Infections and Superinfections Identified by Multiplex PCR among Critically Ill COVID-19 Patients. Microorganisms 2021, 9 (12), 2483. | Israel | 2021 | Retrospective observational | 93 |
| 4. [38] Foschi, C.; Zignoli, A.; Gaibani, P.; Vocale, C.; Rossini, G.; Lafratta, S.; Liberatore, A.; Turello, G.; Lazzarotto, T.; Ambretti, S. Respiratory Bacterial Co-Infections in Intensive Care Unit-Hospitalized COVID-19 Patients: Conventional Culture vs. BioFire FilmArray Pneumonia plus Panel. Journal of Microbiological Methods 2021, 186, 106259. | Italy | 2021 | Retrospective observational | 178 |
| 5. [39] Huang, C.-P.; Tsai, C.-S.; Su, P.-L.; Huang, T.-H.; Ko, W.-C.; Lee, N.-Y. Respiratory Etiological Surveillance among Quarantined Patients with Suspected Lower Respiratory Tract Infection at a Medical Center in Southern Taiwan during COVID-19 Pandemic. Journal of Microbiology, Immunology and Infection 2022, 55 (3), 428–435. | Taiwan | 2022 | Retrospective observational | 201 |
| 6. [40] Karolyi, M.; Pawelka, E.; Hind, J.; Baumgartner, S.; Friese, E.; Hoepler, W.; Neuhold, S.; Omid, S.; Seitz, T.; Traugott, M. T.; Wenisch, C.; Zoufaly, A. Detection of Bacteria via Multiplex PCR in Respiratory Samples of Critically Ill COVID-19 Patients with Suspected HAP/VAP in the ICU. Wiener klinische Wochenschrift 2021, 134 (9–10), 385–390. | Austria | 2021 | Retrospective observational | 60 |
| 7. [41] Maataoui, N.; Chemali, L.; Patrier, J.; Tran Dinh, A.; Le Fèvre, L.; Lortat-Jacob, B.; Marzouk, M.; d’Humières, C.; Rondinaud, E.; Ruppé, E.; Montravers, P.; Timsit, J.-F.; Armand-Lefèvre, L. IMPACT OF RAPID Multiplex PCR on Management of Antibiotic Therapy in COVID-19-Positive Patients Hospitalized in Intensive Care Unit. European Journal of Clinical Microbiology & Infectious Diseases 2021, 40 (10), 2227–2234. | France | 2021 | Retrospective observational | 191 |
| 8. [42] Rothe, K.; Spinner, C. D.; Panning, M.; Pletz, M. W.; Rohde, G.; Rupp, J.; Witzenrath, M.; Erber, J.; Eberhardt, F.; Essig, A.; Schneider, J. Evaluation of a Multiplex PCR Screening Approach to Identify Community-Acquired Bacterial Co-Infections in COVID-19: A Multicenter Prospective Cohort Study of the German Competence Network of Community-Acquired Pneumonia (CAPNETZ). Infection 2021, 49 (6), 1299–1306. | Germany and Switzerland | 2021 | Prospective observational multicenter | 200 |
| 9. [43] Soto, A.; Quiñones-Laveriano, D. M.; Valdivia, F.; Juscamayta-López, E.; Azañero-Haro, J.; Chambi, L.; Horna, H.; Patiño, G.; Guzman, E.; De la Cruz-Vargas, J. A. Detection of Viral and Bacterial Respiratory Pathogens Identified by Molecular Methods in COVID-19 Hospitalized Patients and Its Impact on Mortality and Unfavorable Outcomes. Infection and Drug Resistance 2021, Volume 14, 2795–2807. | Peru | 2021 | Prospective observational | 93 |
| Study | Age (Median) | Gender (% Female–Male) | ICU Admissions (%) | Duration of Hospitalization (Median) | Mortality Rate (%) |
|---|---|---|---|---|---|
| Alosaimi [35] | 52.0 | 33.0–77.0% | 29.0 | ND | 19.0 |
| Bogdan [36] | >18.0 | 49.0–51.0% | 6.7 | 12.4 | 5.5 |
| Cohen [37] | 67.0 | 30.0–70.0% | ND | 24.0 | 38.7 |
| Foschi [38] | >18.0 | ND | 100 | ND | ND |
| Huang [39] | 72.0 | 31.8–68.2% | 9.5 | 7.0 | 8.5 |
| Karolyi [40] | 62.5 | 20.0–80.0% | 100 | 7.0 | 36.7 |
| Maataoui [41] | 57.0 | 18.0–82.0% | 100 | 19.0 | 56.0 |
| Rothe [42] | 58.5 | 36.5–63.5% | 23.4 | 9.0 | 4.5 |
| Soto [43] | 61.7 | 29.0–71.0% | ND | ND | 31.0 |
| Study | Most Frequent Bacteria | Community-Acquired | Antibiotic Usage Prior to Admission (%) | PCR Assay and Panels | Sensitivity/Specificity (%) |
|---|---|---|---|---|---|
| 1 [35] | Chlamydophila pneumonia, S. aureus | ND | ND | Multiplex PCR assay, Superscript III panel | ND |
| 2 [36] | Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella spp. | 25.5% | 40.4 | Multiplex RT-PCR assay | ND |
| 3 [37] | H. influenzae, S. pneumoniae, M. catarrhalis, E. cloacae, P. aeruginosa, S. aureus | 17.0% (31.5% K. pneumoniae, 17.3% H. influenzae, S. pneumoniae 13.0%) | ND | Biofire®, FilmArray® Pneumonia Panel | 78.4/98.1 |
| 4 [38] | Pseudomonas aeruginosa, Klebsiella pneumoniae, Staphylococcus aureus | ND | ND | FilmArray Pneumonia Plus panel | 89.6/98.3 |
| 5 [39] | Pseudomonas aeruginosa, Klebsiella pneumoniae, Staphylococcus aureus | 23.4% | ND | FilmArray TM Respiratory Panel | ND |
| 6 [40] | Staphylococcus aureus, Klebsiella pneumoniae, H. influenzae | 0.0% (20% hospital-acquired, 80% ventilator-acquired) | 73.0 | BioFire® Pneumonia Panel | ND |
| 7 [41] | P. aeruginosa, E. coli, Klebsiella spp. | ND | 79.0 | BioFire® FilmArray® Pneumonia plus Panel | 89.3/99.1 |
| 8 [42] | Staphylococcus aureus, H. influenzae, Streptococcus pneumoniae, Moraxella catarrhalis, Legionella pneumophila | 100% (S. aureus 27.0%, H. influenzae 13.5%, S. pneumoniae 5.5%) | 51.5 | Multiplex RT-PCR | ND |
| 9 [43] | Staphylococcus aureus, Streptococcus agalactiae, H. influenzae, Klebsiella pneumoniae | ND | 82.0 | Biofire Filmarray Pneumonia plus® panel | 96.3/97.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogdan, I.; Gadela, T.; Bratosin, F.; Dumitru, C.; Popescu, A.; Horhat, F.G.; Negrean, R.A.; Horhat, R.M.; Mot, I.C.; Bota, A.V.; et al. The Assessment of Multiplex PCR in Identifying Bacterial Infections in Patients Hospitalized with SARS-CoV-2 Infection: A Systematic Review. Antibiotics 2023, 12, 465. https://doi.org/10.3390/antibiotics12030465
Bogdan I, Gadela T, Bratosin F, Dumitru C, Popescu A, Horhat FG, Negrean RA, Horhat RM, Mot IC, Bota AV, et al. The Assessment of Multiplex PCR in Identifying Bacterial Infections in Patients Hospitalized with SARS-CoV-2 Infection: A Systematic Review. Antibiotics. 2023; 12(3):465. https://doi.org/10.3390/antibiotics12030465
Chicago/Turabian StyleBogdan, Iulia, Tejaswi Gadela, Felix Bratosin, Catalin Dumitru, Alin Popescu, Florin George Horhat, Rodica Anamaria Negrean, Razvan Mihai Horhat, Ion Cristian Mot, Adrian Vasile Bota, and et al. 2023. "The Assessment of Multiplex PCR in Identifying Bacterial Infections in Patients Hospitalized with SARS-CoV-2 Infection: A Systematic Review" Antibiotics 12, no. 3: 465. https://doi.org/10.3390/antibiotics12030465