
Early-Life Antibiotic Exposure and Childhood Asthma Trajectories: A National Population-Based Birth Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
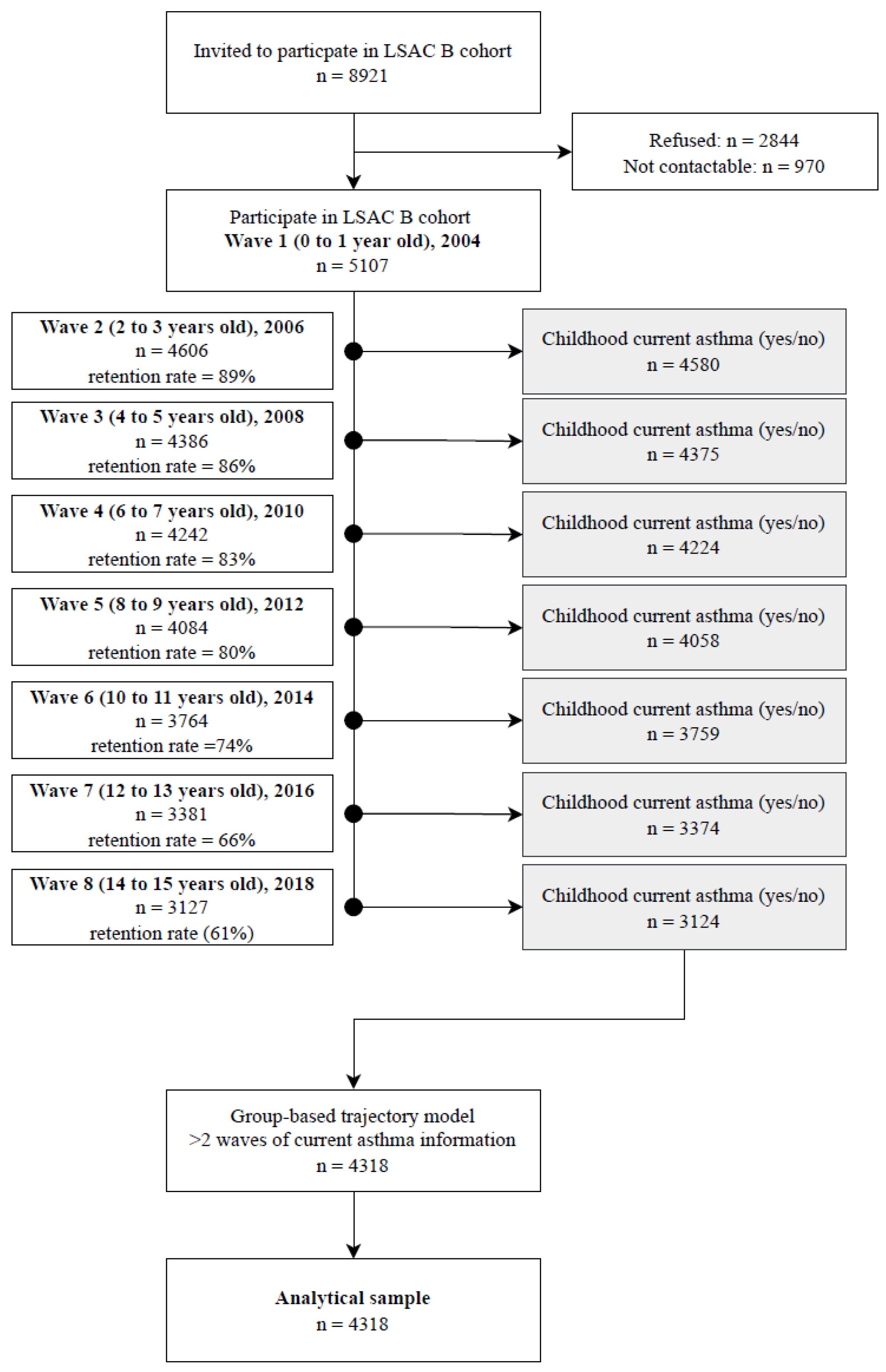
2.1. Study Design and Participants
Procedures
2.2. Measures
2.2.1. Exposure (Antibiotic Exposure in Early-Life up to 24 Months)
2.2.2. Outcome (Asthma Trajectories in Children)
2.2.3. Confounders
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics and Antibiotic Exposure
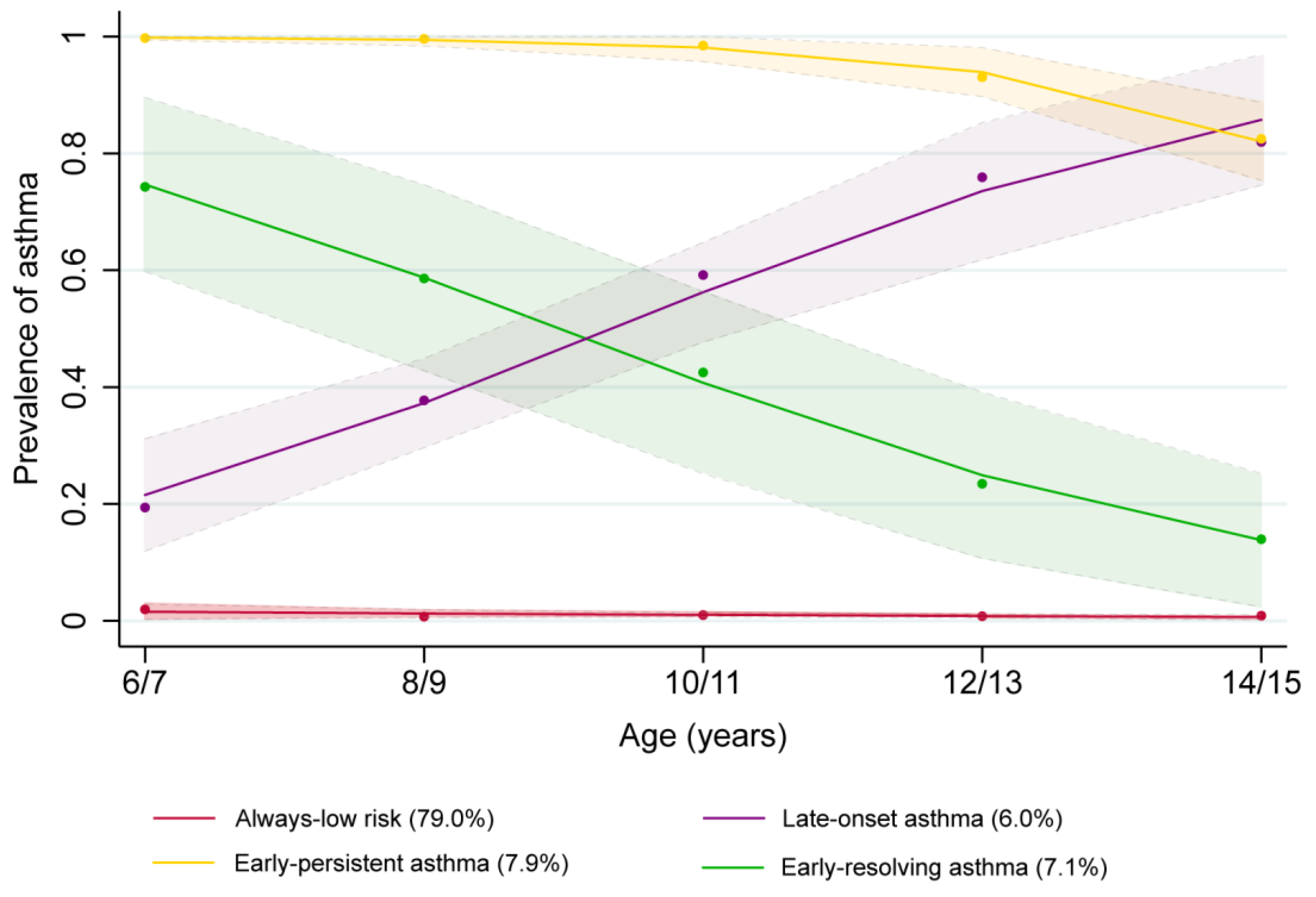
3.2. Childhood Asthma Trajectory
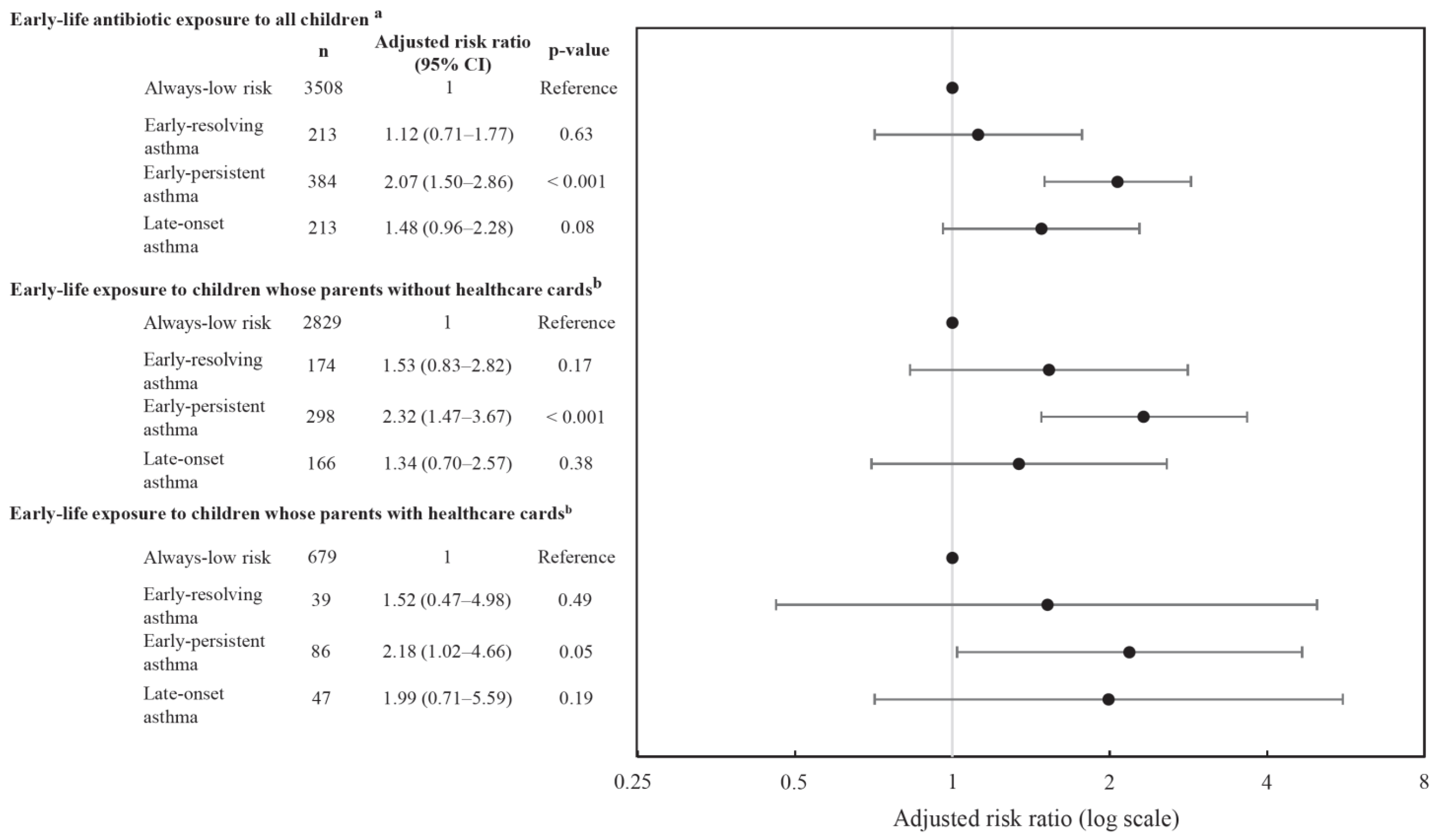
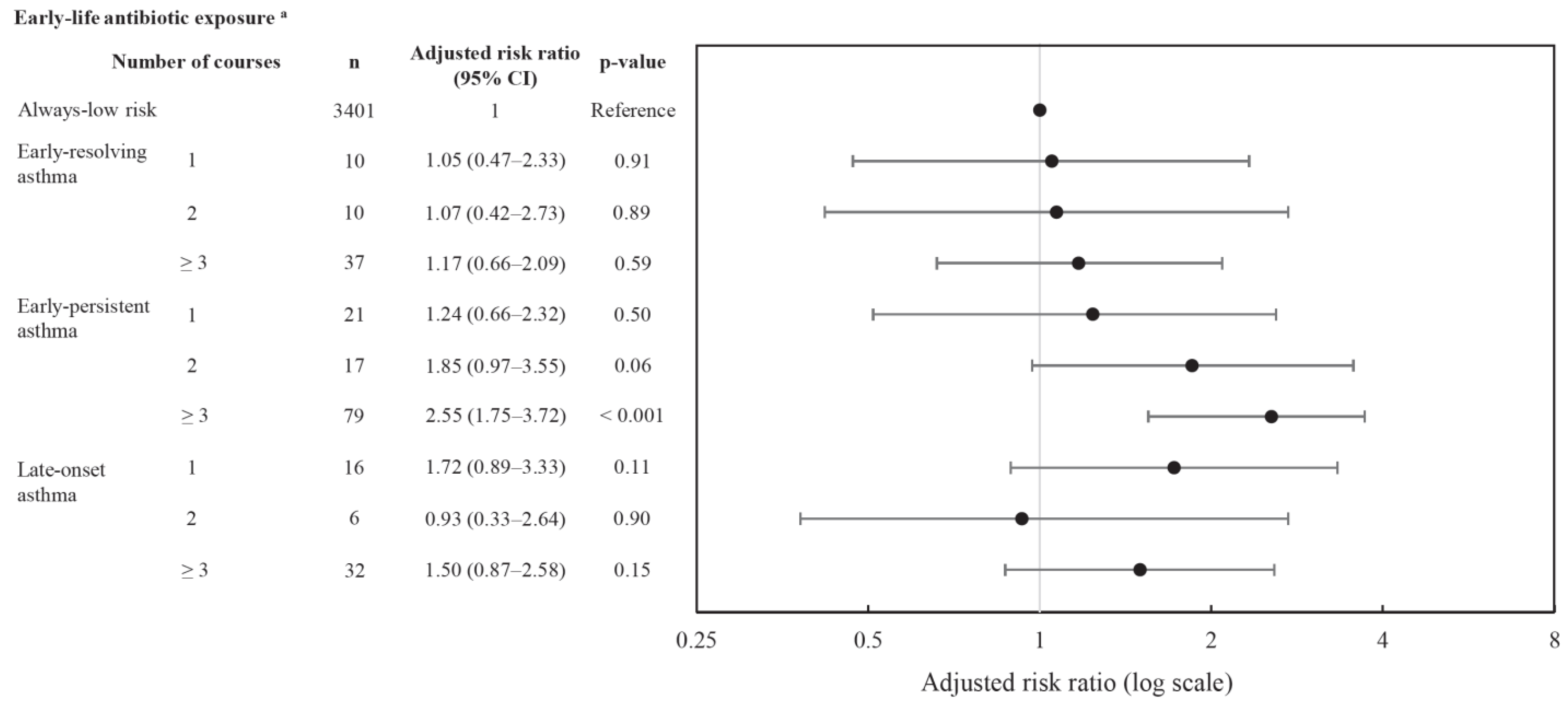
3.3. Early-Life Antibiotics Exposure Association with Childhood Asthma Trajectory
Primary Analysis
3.4. Subgroup Analyses
4. Discussion
4.1. Principal Findings
4.2. Correlation with Existing Evidence
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Asthma; AIHW: Canberra, Australia, 2020.
- Hellman, J.; Grape, M.; Ternhag, A. Antibiotic consumption among a Swedish cohort of children born in 2006. Acta Paediatr. 2015, 104, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Francino, M.P. Antibiotics and the Human Gut Microbiome: Dysbioses and Accumulation of Resistances. Front. Microbiol. 2016, 6, 1543. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.M.; Sbihi, H.; Dai, D.L.Y.; Al Mamun, A.; Rasali, D.; Rose, C.; Marra, F.; Boutin, R.C.T.; Petersen, C.; Stiemsma, L.T.; et al. Decreasing antibiotic use, the gut microbiota, and asthma incidence in children: Evidence from population-based and prospective cohort studies. Lancet Respir. Med. 2020, 8, 1094–1105. [Google Scholar] [CrossRef]
- Örtqvist, A.K.; Lundholm, C.; Kieler, H.; Ludvigsson, J.F.; Fall, T.; Ye, W.; Almqvist, C. Antibiotics in fetal and early life and subsequent childhood asthma: Nationwide population based study with sibling analysis. BMJ Br. Med. J. 2014, 349, g6979. [Google Scholar] [CrossRef] [PubMed]
- Metsälä, J.; Lundqvist, A.; Virta, L.J.; Kaila, M.; Gissler, M.; Virtanen, S.M. Prenatal and post-natal exposure to antibiotics and risk of asthma in childhood. Clin. Exp. Allergy 2015, 45, 137–145. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Mroz, E.; Flak, E.; Majewska, R.; Perera, F.; Maugeri, U.; Mroz, E.; Flak, E.; Perzanowski, M.; Majewska, R. Wheezing and asthmamay be enhanced by broad spectrum antibiotics used in early childhood. concept and results of a pharmacoepidemiology study. J. Physiol. Pharmacol. 2011, 62, 189–195. [Google Scholar]
- Loewen, K.; Monchka, B.; Mahmu, S.M.; Jong, G.; Azad, M.B. Prenatal antibiotic exposure and childhood asthma: A population-based study. Eur. Respir. J. 2018, 52, 1702070. [Google Scholar] [CrossRef]
- Yoshida, S.; Ide, K.; Takeuchi, M.; Kawakami, K. Prenatal and early-life antibiotic use and risk of childhood asthma: A retrospective cohort study. Pediatr. Allergy Immunol. 2018, 29, 490–495. [Google Scholar] [CrossRef]
- Stokholm, J.; Sevelsted, A.; Bønnelykke, K.; Bisgaard, H. Maternal propensity for infections and risk of childhood asthma: A registry-based cohort study. Lancet Respir. Med. 2014, 2, 631–637. [Google Scholar] [CrossRef]
- Martinez, F.D.; Wright, A.L.; Taussig, L.M.; Holberg, C.J.; Halonen, M.; Morgan, W.J. Asthma and Wheezing in the First Six Years of Life. N. Engl. J. Med. 1995, 332, 133–138. [Google Scholar] [CrossRef]
- Granell, R.; Henderson, A.J.; Sterne, J.A. Associations of wheezing phenotypes with late asthma outcomes in the Avon Longitudinal Study of Parents and Children: A population-based birth cohort. J. Allergy Clin. Immunol. 2016, 138, 1060–1070.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, A.L.; Taussig, L.M.; Ray, C.G.; Harrison, H.R.; Holberg, C.J. The Tucson Children’s Respiratory Study. II. Lower respiratory tract illness in the first year of life. Am. J. Epidemiol. 1989, 129, 1232–1246. [Google Scholar] [CrossRef] [PubMed]
- Panico, L.; Stuart, B.; Bartley, M.; Kelly, Y. Asthma Trajectories in Early Childhood: Identifying Modifiable Factors. PLoS ONE 2014, 9, e111922. [Google Scholar] [CrossRef] [PubMed]
- Pape, K.; Cowell, W.; Sejbaek, C.S.; Andersson, N.W.; Svanes, C.; Kolstad, H.A.; Liu, X.; Hougaard, K.S.; Wright, R.J.; Schlünssen, V. Adverse childhood experiences and asthma: Trajectories in a national cohort. Thorax 2021, 76, 547–553. [Google Scholar] [CrossRef]
- Bui, D.S.; Lodge, C.J.; Perret, J.L.; Lowe, A.; Hamilton, G.S.; Thompson, B.; Giles, G.; Tan, D.; Erbas, B.; Pirkis, J.; et al. Trajectories of asthma and allergies from 7 years to 53 years and associations with lung function and extrapulmonary comorbidity profiles: A prospective cohort study. Lancet Respir. Med. 2021, 9, 387–396. [Google Scholar] [CrossRef]
- Sbihi, H.; Koehoorn, M.; Tamburic, L.; Brauer, M. Asthma Trajectories in a Population-based Birth Cohort. Impacts of Air Pollution and Greenness. Am. J. Respir. Crit. Care Med. 2017, 195, 607–613. [Google Scholar] [CrossRef]
- Ödling, M.; Wang, G.; Andersson, N.; Hallberg, J.; Janson, C.; Bergström, A.; Melén, E.; Kull, I. Characterization of Asthma Trajectories from Infancy to Young Adulthood. J. Allergy Clin. Immunol. Pract. 2021, 9, 2368–2376.e3. [Google Scholar] [CrossRef]
- Mellish, L.; Karanges, E.A.; Litchfield, M.J.; Schaffer, A.L.; Blanch, B.; Daniels, B.J.; Segrave, A.; Pearson, S.-A. The Australian Pharmaceutical Benefits Scheme data collection: A practical guide for researchers. BMC Res. Notes 2015, 8, 634. [Google Scholar] [CrossRef]
- Mohal, L.L.C.; Howell, L.; Renda, J.; Jessup, K.; Daraganova, G. Growing Up in Australia: The Longitudinal Study of Australian Children-Data User Guide; Release 8.0.; Australian Institute of Family Studies: Melbourne, Australia, 2020. [Google Scholar]
- Wang, J.; Quach, J.; Sung, V.; Carew, P.; Wake, M. Ear Infection Trajectories and Academic, Behavioral, and Quality-of-Life Outcomes: A Population-Based Longitudinal Study. J. Dev. Behav. Pediatr. 2021, 42, 588–596. [Google Scholar] [CrossRef]
- Van Gool, K.; Kenny, P. Medicare Australia Data for Research: An Introduction Australia; University of Technology Sydney: Sydney, Australia, 2015. [Google Scholar]
- Fees, Patient Contributions and Safety Net Thresholds Canberra: Department of Health and Aged Care. 2022. Available online: https://www.pbs.gov.au/info/healthpro/explanatory-notes/front/fee (accessed on 9 October 2022).
- Loxton, D.; Tooth, L.; Harris, M.L.; Forder, P.M.; Dobson, A.; Powers, J.; Brown, W.; Byles, J.; Mishra, G. Cohort Profile: The Australian Longitudinal Study on Women’s Health (ALSWH) 1989–1995 cohort. Int. J. Epidemiol. 2017, 47, 391–392e. [Google Scholar] [CrossRef]
- Taylor, C.L.; Christensen, D.; Lawrence, D.; Mitrou, F.; Zubrick, S.R. Risk Factors for Children’s Receptive Vocabulary Development from Four to Eight Years in the Longitudinal Study of Australian Children. PLoS ONE 2013, 8, e73046. [Google Scholar] [CrossRef]
- Secretariat DUS-C. Australian Statistics on Medicines 2004–2005; Department of Health and Ageing: Canberra, Australia, 2007. [Google Scholar]
- Prescribed antibiotic use in Australian children aged 0–12 years. Aust. J. Gen. Pract. 2016, 45, 134–138.
- PBS. Expenditure and Prescriptions Twelve Months to 30 June 2004; Pharmaceutical Pricing Section Pharmaceutical Benefits Branch: Canberra, Australia, 2004.
- Therapeutic Goods Administration, Standards & Guidelines for Prescription Medicines: Department of Health, Australian Government. 2021. Available online: https://www.tga.gov.au/standards-guidelines-prescription-medicines (accessed on 2 July 2022).
- NICE NIfHaCE. Asthma: Diagnosis, Monitoring and Chronic Asthma Management (NG80). 2017. Available online: https://www.nice.org.uk/guidance/ng80 (accessed on 16 April 2022).
- Castro-Rodriguez, J.A.; Forno, E.; Celedon, J.C.; Rodriguez-Martinez, C.E. Risk and Protective Factors for Childhood Asthma: What Is the Evidence? J. Allergy Clin. Immunol. Pract. 2016, 4, 1111–1122. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef] [PubMed]
- Ellwood, P.; Asher, M.I.; Beasley, R.; Clayton, T.O.; Stewart, A.W. The international study of asthma and allergies in childhood (ISAAC): Phase three rationale and methods. Int. J. Tuberc. Lung Dis. 2005, 9, 10–16. [Google Scholar] [PubMed]
- Jones, B.L.; Nagin, D.S. A Note on a Stata Plugin for Estimating Group-based Trajectory Models. Sociol. Methods Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S. Advances in Group-Based Trajectory Modeling and an SAS Procedure for Estimating Them. Sociol. Methods Res. 2007, 35, 542–571. [Google Scholar] [CrossRef]
- Nagin, D.S.; Odgers, C.L. Group-based trajectory modeling in clinical research. Annu. Rev. Clin. Psychol. 2010, 6, 109–138. [Google Scholar] [CrossRef]
- Postma, D.S. Gender Differences in Asthma Development and Progression. Gend. Med. 2007, 4, S133–S146. [Google Scholar] [CrossRef] [PubMed]
- Ronen, O.; Malhotra, A.; Pillar, G. Influence of gender and age on upper-airway length during development. Pediatrics 2007, 120, e1028–e1034. [Google Scholar] [CrossRef]
- Strömberg Celind, F.; Wennergren, G.; Vasileiadou, S.; Alm, B.; Goksör, E. Antibiotics in the first week of life were associated with atopic asthma at 12 years of age. Acta Paediatr. 2018, 107, 1798–1804. [Google Scholar] [CrossRef]
- Murk, W.; Risnes, K.R.; Bracken, M.B. Prenatal or Early-Life Exposure to Antibiotics and Risk of Childhood Asthma: A Systematic Review. Pediatrics 2011, 127, 1125–1138. [Google Scholar] [CrossRef] [PubMed]
- Faillie, J.L. Indication bias or protopathic bias? Br. J. Clin. Pharmacol. 2015, 80, 779–780. [Google Scholar] [CrossRef]
- Bui, T.; Preuss, C.V. Cephalosporins; StatPearls Publishing: Tampa, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK551517/ (accessed on 5 July 2022).
- Hu, Y. Interventional Study to Reduce Antibiotic Over-Prescribing Among Children with Upper Respiratory Tract Infections (URIs) in Rural Guangxi; The Chinese University of Hong Kong: Hong Kong, China, 2016. [Google Scholar]
- Hu, Y.; Walley, J.; Chou, R.; Tucker, J.D.; Harwell, J.I.; Wu, X.; Yin, J.; Zou, G.; Wei, X. Interventions to reduce childhood antibiotic prescribing for upper respiratory infections: Systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 1162–1170. [Google Scholar] [CrossRef]
- Chen, I.-L.; Tsai, M.-K.; Chung, H.-W.; Hsieh, H.-M.; Huang, Y.-T.; Lin, Y.-C. The effects of antibiotic exposure on asthma in children with atopic dermatitis. Sci. Rep. 2021, 11, 8526. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Friedman, H.; Boyd, B.C.; McGurn, A.; Babinski, P.; Markossian, T.; Dugas, L.R. Early antibiotic exposure and development of asthma and allergic rhinitis in childhood. BMC Pediatr. 2019, 19, 225. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, M.-C.; Stiemsma, L.T.; Dimitriu, P.A.; Thorson, L.; Russell, S.; Yurist-Doutsch, S.; Kuzeljevic, B.; Gold, M.J.; Britton, H.M.; Lefebvre, D.L.; et al. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci. Transl. Med. 2015, 7, 307ra152. [Google Scholar] [CrossRef]
- DiMatteo, M.R. Variations in patients’ adherence to medical recommendations: A quantitative review of 50 years of research. Med. Care 2004, 42, 200–209. [Google Scholar] [CrossRef]
- Liao, Z.; Lamb, K.E.; Burgner, D.; Ranganathan, S.; Miller, J.E.; Koplin, J.J.; Dharmage, S.C.; Lowe, A.J.; Ponsonby, A.-L.; Tang, M.L.K.; et al. No obvious impact of caesarean delivery on childhood allergic outcomes: Findings from Australian cohorts. Arch. Dis. Child. 2020, 105, 664. [Google Scholar] [CrossRef]
- Morgan, B.W.; Siddharthan, T.; Grigsby, M.R.; Pollard, S.L.; Kalyesubula, R.; Wise, R.A.; Kirenga, B.; Checkley, W. Asthma and Allergic Disorders in Uganda: A Population-Based Study Across Urban and Rural Settings. J. Allergy Clin. Immunol. Pract. 2018, 6, 1580–1587.e2. [Google Scholar] [CrossRef]
- Lewis, K.M.; Ruiz, M.; Goldblatt, P.; Morrison, J.; Porta, D.; Forastiere, F.; Hryhorczuk, D.; Zvinchuk, O.; Saurel-Cubizolles, M.-J.; Lioret, S.; et al. Mother’s education and offspring asthma risk in 10 European cohort studies. Eur. J. Epidemiol. 2017, 32, 797–805. [Google Scholar] [CrossRef]
- Wu, P.; Feldman, A.S.; Rosas-Salazar, C.; James, K.; Escobar, G.; Gebretsadik, T.; Li, S.X.; Carroll, K.N.; Walsh, E.; Mitchel, E.; et al. Relative Importance and Additive Effects of Maternal and Infant Risk Factors on Childhood Asthma. PLoS ONE 2016, 11, e0151705. [Google Scholar] [CrossRef]
- Risnes, K.R.; Belanger, K.; Murk, W.; Bracken, M.B. Antibiotic exposure by 6 months and asthma and allergy at 6 years: Findings in a cohort of 1401 US children. Am. J. Epidemiol. 2011, 173, 310–318. [Google Scholar] [CrossRef]
- Greiner, T. Exclusive breastfeeding: Measurement and indicators. Int Breastfeed J. 2014, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.; Luef, B.M.; Jørgensen, J.S. Childhood inflammatory and metabolic disease following exposure to antibiotics in pregnancy, antenatally, intrapartum and neonatally. F1000Research 2020, 9, 144. [Google Scholar] [CrossRef]
- Abrahamsson, T.; Jakobsson, H.E.; Andersson, A.; Björkstén, B.; Engstrand, L.; Jenmalm, M.C. Low gut microbiota diversity in early infancy precedes asthma at school age. Clin. Exp. Allergy 2014, 44, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Dik, N.; Tate, R.B.; Manfreda, J.; Anthonisen, N.R. Risk of Physician-Diagnosed Asthma in the First 6 Years of Life. Chest 2004, 126, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Newcomb, D.C. Sex Bias in Asthma Prevalence and Pathogenesis. Front. Immunol. 2018, 9, 2997. [Google Scholar] [CrossRef] [PubMed]
- WHO. Born Too Soon, Report; World Health Organisation: Geneva, Switzerland, 2012.
- Standord_Medicine. Low Birth Weight: Standard Medicine Children’s Health. 2022. Available online: https://www.stanfordchildrens.org/en/topic/default?id=low-birthweight-90-P02382 (accessed on 3 July 2022).
- Stein, R.T.; Sherrill, D.; Morgan, W.J.; Holberg, C.J.; Halonen, M.; Taussig, L.M.; Wright, A.L.; Martinez, F.D. Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet 1999, 354, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Stern, D.A.; Morgan, W.J.; Halonen, M.; Wright, A.L.; Martinez, F.D. Wheezing and bronchial hyper-responsiveness in early childhood as predictors of newly diagnosed asthma in early adulthood: A longitudinal birth-cohort study. Lancet 2008, 372, 1058–1064. [Google Scholar] [CrossRef]
- Nyquist, A.-C.; Gonzales, R.; Steiner, J.F.; Sande, M.A. Antibiotic Prescribing for Children With Colds, Upper Respiratory Tract Infections, and Bronchitis. JAMA 1998, 279, 875–877. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.J.; Wang, J.; Harwell, J.I.; Wake, M. Association of in utero antibiotic exposure on childhood ear infection trajectories: Results from a national birth cohort study. J. Paediatr. Child Health 2021, 57, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.E.; Bunnell, H.T.; Hossain, M.J.; Wysocki, T.; Lima, J.J.; Finkel, T.H.; Bacharier, L.; Dempsey, A.; Sarzynski, L.; Test, M.; et al. Being Overweight or Obese and the Development of Asthma. Pediatrics 2018, 142, e20182119. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample,n(%) | All Children n= 5107 | Children with HCC † n= 1143 |
| Infant | ||
| Infant birthweight (g), mean ± SD | 3395.4 ± 610 | 3305.8 ± 694 |
| Gestational age weeks, mean ± SD | 39.3 ± 2.0 | 39.1 ± 2.2 |
| Infant sex, % | ||
| 2608 (51.1) 2499 (48.9) | 590 (51.6) 553 (48.4) |
| Ever had Asthma, n (%) | ||
| 1028 (32.7) 2117 (67.3) | 220 (39.3) 340 (60.7) |
| Delivery method, n (%) | ||
| 3146 (61.7) 24 (0.5) 1503 (29.5) 248 (4.9) 161 (3.2) 21 (0.4) 4 (0.08) | 760 (66.7) 3 (0.3) 306 (26.8) 35 (3.1) 33 (2.9) 3 (0.3) |
| Feeding method at 6 months, n (%) | ||
| 944 (24.9) 2845 (75.1) | 153 (17.4) 725 (82.6) |
| Ever been hospitalized for respiratory infection by 24 months, n (%) | ||
| 111 (2.6) 4975 (97.4) | 34 (3.0) 1101 (97.0) |
| Ever had ear infection by 12 months, n (%) | ||
| 200 (3.9) 4883 (96.1) | 50 (4.4) 1088 (95.6) |
| Residence location, n (%) | ||
| 4633 (90.9) 462 (9.1) | 1022 (90.0) 155 (10.0) |
| Birthweight (g), n (%) | ||
| 294 (5.8) 706 (13.9) 3438 (67.4) 656 (12.9) | 93 (8.2) 182 (16.0) 734 (64.4) 130 (11.4) |
| Preterm birth, n (%) | ||
| 334 (6.5) 4773 (93.5) | 93 (8.1) 1050 (91.9) |
| Ethnicity, n (%) | ||
| 3082 (60.3) 2025 (39.7) | 537 (47.0) 606 (53.0) |
| Maternal | ||
| Maternal age (years), mean ± SD | 30.8 ± 5.5 | 28.8 ± 6.7 |
| Quintiles of neighborhood disadvantage (SEIFA), n (%) | ||
| 1136 (22.2) 1101 (21.6) 1038 (20.3) 863 (16.9) 969 (19.0) | 359 (31.4) 306 (36.8) 222 (19.4) 145 (12.7) 111 (9.7) |
| Maternal asthma, n (%) | ||
| 185 (3.6) 4912 (96.4) | 47 (4.1) 1093 (95.9) |
| Maternal smoking, n (%) | ||
| 709 (16.7) 3530 (83.3) | 279 (32.6) 576 (67.4) |
| Maternal alcohol | ||
| 1633 (38.6) 2594 (61.4) | 216 (25.5) 631 (74.5) |
| Mother’s highest education achieved at conception, n (%) | ||
| 865 (16.9) 796 (15.6) 2764 (54.2) 679 (13.3) | 348 (30.5) 181 (15.8) 541 (47.3) 73 (6.4) |
| Antibiotic exposure during pregnancy, n (%) | ||
| 531 (10.4) 4566 (89.6) | 138 (12.1) 1002 (87.9) |
| Any Antibiotic Prescribed (PBS Records), n(%) † | |
| 1267 (24.8) 3840 (75.2) |
| Any antibiotic prescribed for children whose parents have healthcare cards, n (%) | 3395.4 ± 610 |
| 778 (68.1) 365 (31.9) |
| Number of antibiotic courses exposed during the period, n (%) | |
| 317 (25.0) 233 (18.4) 717 (56.6) |
| Class of Antibiotics Exposed by Courses, n (%) | |
| β-lactam other than cephalosporin ‡, total | 1123 (100) |
| 382 (34.0) 254 (22.6) 153 (13.6) 334 (29.8) |
| First-generation cephalosporin, total | 257 (100) |
| 165 (64.2) 50 (19.5) 25 (9.7) 17 (6.6) |
| Second-generation cephalosporin, total | 351 (100) |
| 185 (52.7) 83 (23.6) 37 (10.5) 46 (13.1) |
| Third-generation cephalosporin, total | 3 (100) |
| 3 (100) |
| Quinolone, total | 2 (100) |
| 1 (50) 1 (50) |
| Macrolide, total | 252 (100) |
| 167 (66.3) 52 (20.6) 16 (6.4) 17(6.7) |
| Aminoglycoside, total | 1 (100) |
| 1 (100) |
| Sulfonamide and Trimethoprim, total | 98 (100) |
| 71 (72.5) 13 (13.3) 7 (7.1) 7 (7.1) |
| Nitroimidazole, total | 30 (100) |
| 28 (93.3) 2 (6.7) |
| Fusidane, total | 1 (100) |
| 1 (100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.; Wang, Y.; Wang, J.; Lowe, A.J.; Grzeskowiak, L.E.; Hu, Y.J. Early-Life Antibiotic Exposure and Childhood Asthma Trajectories: A National Population-Based Birth Cohort. Antibiotics 2023, 12, 314. https://doi.org/10.3390/antibiotics12020314
Lu Y, Wang Y, Wang J, Lowe AJ, Grzeskowiak LE, Hu YJ. Early-Life Antibiotic Exposure and Childhood Asthma Trajectories: A National Population-Based Birth Cohort. Antibiotics. 2023; 12(2):314. https://doi.org/10.3390/antibiotics12020314
Chicago/Turabian StyleLu, Yankun, Yichao Wang, Jing Wang, Adrian J. Lowe, Luke E. Grzeskowiak, and Yanhong J. Hu. 2023. "Early-Life Antibiotic Exposure and Childhood Asthma Trajectories: A National Population-Based Birth Cohort" Antibiotics 12, no. 2: 314. https://doi.org/10.3390/antibiotics12020314