
Correlation between Previous Antibiotic Exposure and COVID-19 Severity. A Population-Based Cohort Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
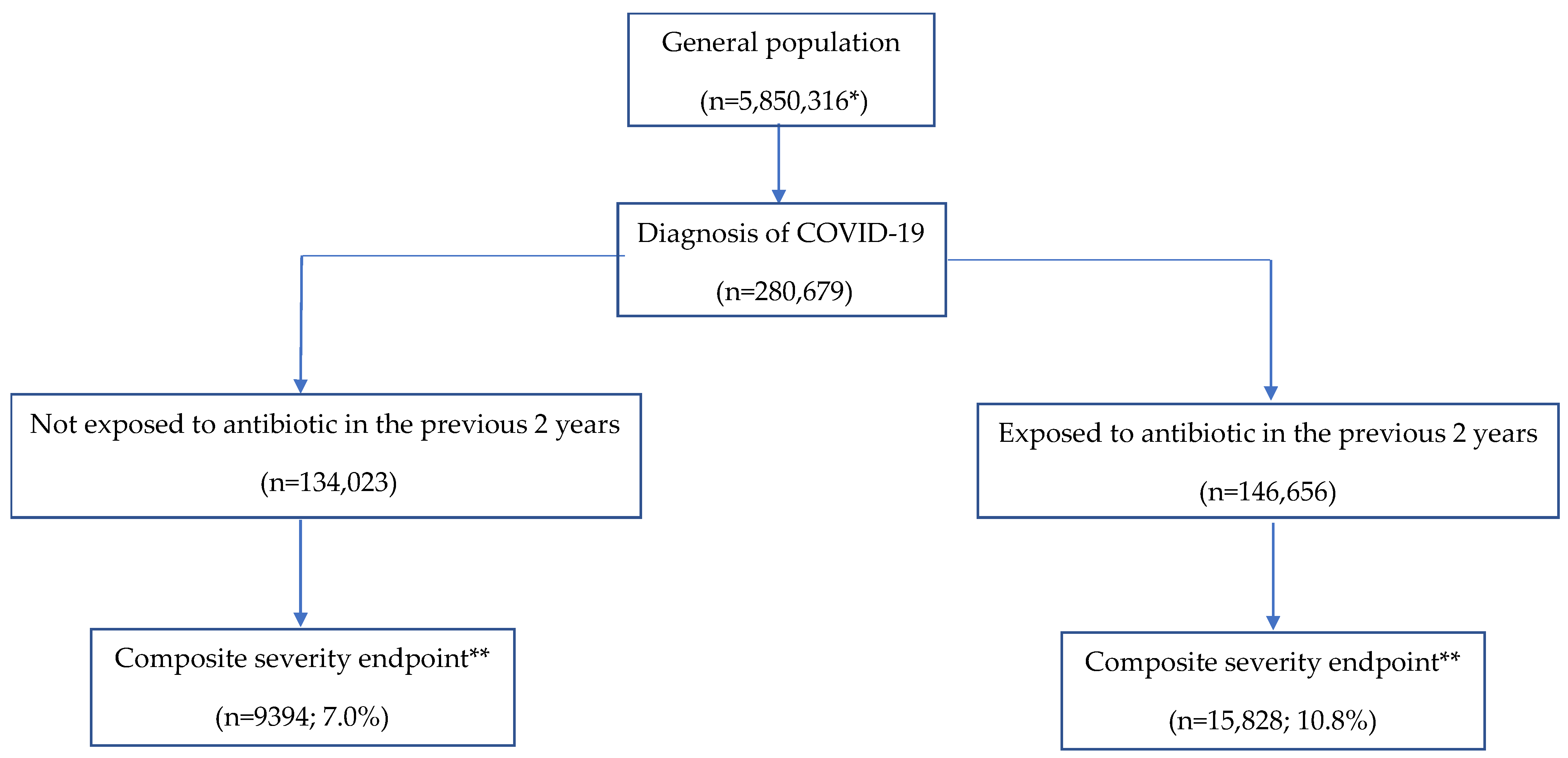
2.1. Study Population
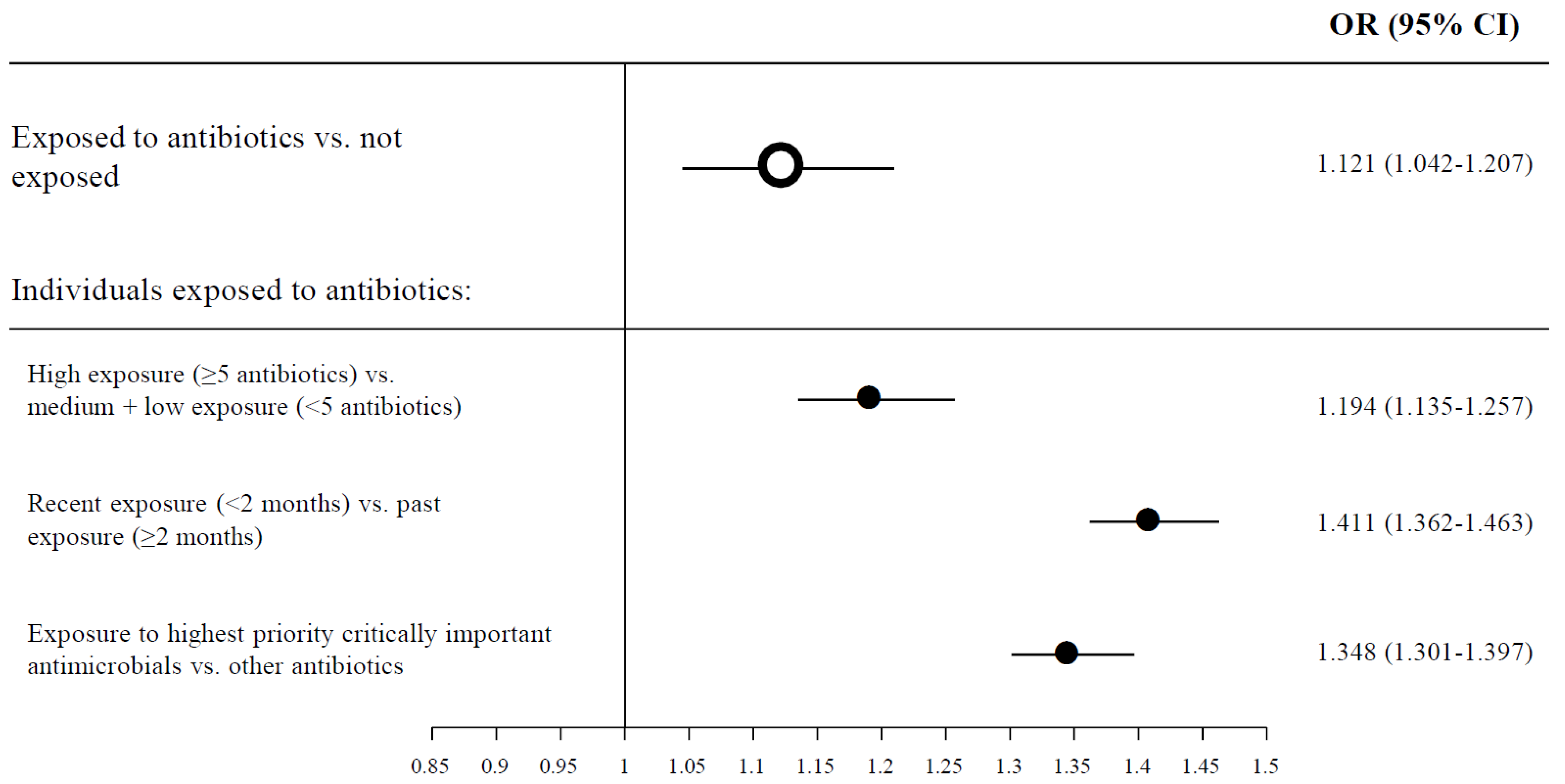
2.2. The Correlation between Previous Use of Antibiotics and COVID-19 Severity
3. Discussion
4. Methods
4.1. Study Design, Setting and Participants
4.2. Data Collection
4.3. Drug Exposure
4.4. Variables and Outcomes
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mallah, S.I.; Ghorab, O.K.; Al-Salmi, S.; Abdellatif, O.S.; Tharmaratnam, T.; Iskandar, M.A.; Nassef Sefen, J.A.; Sidhu, P.; Atallah, B.; El-Lababidi, R.; et al. COVID-19: Breaking down a global health crisis. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1942. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.A. COVID-19: Risk groups, mechanistic insights and challenges. Int. J. Clin. Pract. 2020, 74, e13512. [Google Scholar] [CrossRef] [Green Version]
- Islam, N.; Shkolnikov, V.M.; Acosta, R.J.; Klimkin, I.; Kawachi, I.; Irizarry, R.A.; Alicandro, G.; Khunti, K.; Yates, T.; Jdanov, D.A.; et al. Excess deaths associated with COVID-19 pandemic in 2020: Age and sex disaggregated time series analysis in 29 high income countries. BMJ 2021, 373, n1137. [Google Scholar] [CrossRef]
- Vaughn, V.M.; Gandhi, T.N.; Petty, L.A.; Patel, P.K.; Prescott, H.C.; Malani, A.N.; Ratz, D.; McLaughlin, E.; Chopra, V.; Flanders, S.A. Empiric antibacterial therapy and community-onset bacterial coinfection in patients hospitalized with coronavirus disease 2019 (COVID-19): A multi-hospital cohort study. Clin. Infect. Dis. 2021, 72, e533–e541. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.U.; Zaura, E.; Buijs, M.J.; Keijser, B.J.; Crielaard, W.; Nord, C.E.; Weintraub, A. Determining the long-term effect of antibiotic administration on the human normal intestinal microbiota using culture and pyrosequencing methods. Clin. Infect. Dis. 2015, 60 (Suppl. 2), S77–S84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panda, S.; El Khader, I.; Casellas, F.; López Vivancos, J.; García Cors, M.; Santiago, A.; Cuenca, S.; Guarner, F.; Manichanh, C. Short-term effect of antibiotics on human gut microbiota. PLoS ONE 2014, 9, e954764. [Google Scholar] [CrossRef] [PubMed]
- Vogt, S.L.; Finlay, B.B. Gut microbiota-mediated protection against diarrheal infections. J. Travel. Med. 2017, 24 (Suppl. 1), S39–S43. [Google Scholar] [CrossRef] [PubMed]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M.; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollef, M.H. Broad-spectrum antimicrobials and the treatment of serious bacterial infections: Getting it right up front. Clin. Infect. Dis. 2008, 47 (Suppl. 1), S3–S13. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Perez, G.; Hicks, A.L.; Tekieli, T.M.; Radens, C.M.; Williams, B.L.; Lamousé-Smith, E.S.N. Maternal antibiotic treatment impacts development of the neonatal intestinal microbiome and antiviral immunity. J. Immunol. 2016, 196, 3768–3779. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Zhou, Y.; Liu, B.; Jin, Z.; Zhuang, X.; Dai, W.; Yang, Z.; Feng, Z.; Zhou, Q.; Liu, Y.; et al. Perinatal antibiotic exposure affects the transmission between maternal and neonatal microbiota and is associated with early-onset sepsis. mSphere 2020, 5, e00984-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.E.; Kim, B.C.; Chang, D.H.; Kwon, M.; Young Lee, S.; Kang, D.; Kim, J.Y.; Hwang, I.; Yu, J.W.; Nakae, S.; et al. Dysbiosis-induced IL-33 contributes to impaired antiviral immunity in the genital mucosa. Proc. Natl. Acad. Sci. USA 2016, 113, E762–E771. [Google Scholar] [CrossRef] [Green Version]
- Harper, A.; Vijayakumar, V.; Ouwehand, A.C.; Ter Haar, J.; Obis, D.; Espadaler, J.; Binda, S.; Desiraju, S.; Day, R. Viral infections, the microbiome, and probiotics. Front. Cell. Infect. Microbiol. 2021, 10, 925. [Google Scholar] [CrossRef] [PubMed]
- Burn, E.; Tebé, C.; Fernández-Bertolin, S.; Aragon, M.; Recalde, M.; Roel, E.; Prats-Uribe, A.; Prieto-Alhambra, D.; Duarte-Salles, T. The natural history of symptomatic COVID-19 during the first wave in Catalonia. Nat. Commun. 2021, 12, 777. [Google Scholar] [CrossRef]
- Durack, J.; Lynch, S.V. The gut microbiome: Relationships with disease and opportunities for therapy. J. Exp. Med. 2019, 216, 20–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collignon, P.C.; Conly, J.M.; Andremont, A.; McEwen, S.A.; Aidara-Kane, A. For the World Health Organization. World Health Organization ranking of antimicrobials according to their importance in human medicine: A critical step for developing risk management strategies to control antimicrobial resistance from food animal production. Clin. Infect. Dis. 2016, 63, 1087–1093. [Google Scholar]
- Dethlefsen, L.; Huse, S.; Sogin, M.L.; Relman, D.A. The pervasive effects of an antibiotic on the human gut microbiota, as revealed by deep 16S rRNA sequencing. PLoS Biol. 2008, 6, e280. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence COVID-19 Rapid Guideline: Managing Suspected or Confirmed Pneumonia in Adults in the Community NG165 (NICE, London). Available online: https://www.nice.org.uk/guidance/ng165 (accessed on 7 October 2021).
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Khor, W.P.; Olaoye, O.; D’Arcy, N.; Krochow, E.M.; Elshanawy, R.A.; Rutter, V.; Ashiru-Oredope, D. The need for ongoing antimicrobial stewardship during the COVID-19 pandemic and actionable recommendations. Antibiotics 2020, 9, 904. [Google Scholar] [CrossRef] [PubMed]
- SIDIAP. Information System for Research in Primary Care. SIDIAP. 2020. Available online: http://www.sidiap.org/index.php/en (accessed on 7 October 2021).
- World Health Organization. ICD-10 Version: 2019. International Statistical Classification of Diseases and Related Health Problems 10th Revision. 2019. Available online: https://icd.who.int/browse10/2019/en (accessed on 7 October 2021).
- World Health Organization Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2019. 2019. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 7 October 2021).
- CatSalut. Servei Català de la Salut. Conjunt Mínim Bàsic de Dades (CMBD). 2019. Available online: http://catsalut.gencat.cat/ca/proveidors-professionals/registres-catalegs/registres/cmbd/ (accessed on 10 September 2021).
- Catalan Agency for Health Quality and Evaluation (AQuAS). Upadted SARS-CoV-2 Data. Updated SARS-CoV-2 Data. Available online: https://aquas.gencat.cat/ca/actualitat/ultimes-dades-coronavirus/index.html#googtrans(ca|en) (accessed on 7 October 2021).
- Bolíbar, B.; Fina Avilés, F.; Morros, R.; Garcia-Gil, M.M.; Hermosilla, E.; Ramos, R.; Rosell, M.; Rodríguez, J.; Medina, M.; Calero, S.; et al. Base de datos SIDIAP: La historia clínica informatizada de Atención Primaria como fuente de información para la investigación epidemiológica. Med. Clin. 2012, 138, 617–621. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Advisory Group on Integrated Surveillance of Antimicrobial Resistance (AGISAR). WHO Critically Important Antimicrobials for Human Medicine 6th Revision, November 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/325036/WHO-NMH-FOS-FZD-19.1-eng.pdf (accessed on 7 October 2021).
- Domínguez-Berjón, M.F.; Borrell, C.; Cano-Serral, G.; Esnaola, S.; Nolasco, A.; Pasarín, M.I.; Ramis, R.; Saurina, C.; Escolar-Pujolaret, A. Constructing a deprivation index based on census data in large Spanish cities (the MEDEA project). Gac. Sanit. 2008, 22, 179–187. [Google Scholar] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Overall (n: 280,679) | Non-Exposed to Antibiotics (n: 134,023) | Exposed to Antibiotics (n: 146,656) | p-Value | |
|---|---|---|---|---|
| Sociodemographic Data * | ||||
| Gender | <0.0001 | |||
| Female, n (%) | 153,034 (54.5) | 67,039 (50.0) | 85,995 (58.6) | |
| Male, n (%) | 127,645 (45.5) | 66,984 (50.0) | 60,661 (41.4) | |
| Age, mean (SD) | 46.3 (20.4) | 44.5 (19.0) | 48.0 (21.5) | <0.0001 |
| Age (categorical) | <0.0001 | |||
| <60 yr., n (%) | 215,699 (76.8) | 109,979 (82.1) | 105,720 (72.1) | |
| ≥60 yr., n (%) | 64,980 (23.2) | 24,044 (17.9) | 40,936 (27.9) | |
| Deprivation index score (%) | <0.0001 | |||
| Unknown, n (%) | 71,311 (25.4) | 33,967 (25.3) | 37,344 (25.5) | |
| Urban 1st quintile (least deprived), n (%) | 39,861 (14.2) | 21,207 (15.8) | 18,654 (12.7) | |
| Urban 2nd quintile, n (%) | 42,795 (15.2) | 21,094 (15.7) | 21,701 (14.8) | |
| Urban 3rd quintile, n (%) | 42,511 (15.1) | 20,497 (15.3) | 22,014 (15.0) | |
| Urban 4th quintile, n (%) | 42,402 (15.1) | 19,181 (14.3) | 23,221 (15.8) | |
| Urban 5th quintile (most deprived), n (%) | 41,799 (14.9) | 18,077 (13.5) | 23,722 (16.2) | |
| Associated Comorbidity and Risk Factors * | ||||
| Smoking habit, n (%) | 110,781 (39.5) | 47,788 (35.7) | 62,993 (43.0) | <0.0001 |
| Obesity, n (%) | 75,739 (27.0) | 29,882 (22.3) | 45,857 (31.3) | <0.001 |
| Ischemic heart disease, n (%) | 7706 (2.7) | 2452 (1.8) | 5254 (3.6) | <0.0001 |
| Diabetes mellitus, n (%) | 23,604 (8.4) | 8167 (6.1) | 15,437 (10.5) | <0.0001 |
| High blood pressure, n (%) | 57,773 (20.6) | 21,828 (16.3) | 35,945 (24.5) | <0.0001 |
| Heart failure, n (%) | 5256 (1.9) | 1213 (0.9) | 4043 (2.8) | <0.0001 |
| Chronic kidney disease, n (%) | 11,915 (4.2) | 3467 (2.6) | 8448 (5.8) | <0.0001 |
| Respiratory disease, n (%) | 45,931 (16.4) | 14,060 (10.5) | 31,871 (21.7) | <0.0001 |
| Thromboembolism, n (%) | 896 (0.3) | 260 (0.2) | 636 (0.4) | <0.0001 |
| Concomitant Medication * | ||||
| NSAIDs, n (%) | 66,764 (23.8) | 22,092 (16.5) | 44,672 (30.5) | <0.0001 |
| Antithrombotic medication, n (%) | 15,150 (5.4) | 5052 (3.8) | 10,098 (6.9) | <0.0001 |
| Corticosteroids, n (%) | 14,663 (5.2) | 3765 (2.8) | 10,898 (7.4) | <0.0001 |
| Low molecular weight heparin, n (%) | 2122 (0.8) | 666 (0.5) | 1456 (1.0) | <0.0001 |
| Antibiotic Exposure | ||||
| Antibiotic exposure intensity † | - | |||
| None, n (%) | 134,023 (47.7) | 134,023 (100.0) | - | |
| Low (1–2 prescriptions), n (%) | 104,873 (37.4) | - | 104,873 (71.5) | |
| Medium (3–4 prescriptions), n (%) | 26,868 (9.6) | - | 26,868 (18.3) | |
| High (≥5 prescriptions), n (%) | 14,915 (5.3) | - | 14,915 (10.2) | |
| Last antibiotic course taken | ||||
| <2 months before COVID-19 infection | 59,176 (40.4) | - | 59,176 (40.4) | |
| ≥2 months before COVID-19 infection | 87,480 (59.6) | - | 87,480 (59.6) | |
| Days to last antibiotic prescription, mean (SD) | 198.8 (214.6) | - | 198.8 (214.6) | - |
| Highest priority critically important antimicrobials, n (%) | 47,477 (32.4) | - | 47,477 (32.4) | - |
| COVID-Related Severity Events ‡ | ||||
| Death, hospitalization and/or pneumonia (%) | 25,222 (9.0) | 9394 (7.0) | 15,828 (10.8) | <0.0001 |
| Hospitalization, n (%) | 16,437 (5.9) | 6258 (4.7) | 10,179 (6.9) | <0.0001 |
| Pneumonia (%) | 5154 (1.8) | 2079 (1.6) | 3075 (2.1) | <0.0001 |
| Death (%) | 7975 (2.8) | 2721 (2.0) | 5254 (3.6) | <0.0001 |
| Patients Diagnosed with Non-Severe COVID-19 (n: 255,457) | Patients Diagnosed with COVID-19 with the Composite Severity Endpoint (n: 25,222) | Univariable | Multivariable * | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |||
| Exposed to antibiotics | 130,828 (51.2) | 15,828 (62.8) | 1.50 (1.40–1.60) | <0.0001 | 1.12 (1.04–1.21) | 0.0022 |
| High exposure (≥5 antibiotics) † | 12,395 (4.9) | 2520 (10.0) | 1.81 (1.73–1.90) | <0.0001 | 1.19 (1.14–1.26) | <0.0001 |
| Recent exposure (<2 months) † | 51,069 (39.0) | 8107 (51.2) | 1.64 (1.59–1.70) | <0.0001 | 1.41 (1.36–1.46) | <0.0001 |
| Past exposure (≥2 months) † | 79,759 (61.0) | 7721 (48.8) | 1.35 (1.24–1.46) | <0.0001 | 1.03 (0.95–1.13) | 0.4722 |
| Exposed to HPCIAs † | 40,891 (31.3) | 6586 (41.6) | 1.57 (1.51–1.62) | <0.0001 | 1.35 (1.30–1.40) | <0.0001 |
| Covariables | ||||||
| Smoking | 100,143 (39.2) | 10,638 (42.2) | 1.22 (1.14–1.30) | <0.0001 | ||
| Obesity | 65,194 (25.5) | 10,545 (41.8) | 1.58 (1.48–1.69) | <0.0001 | ||
| Ischemic heart disease | 5453 (2.1) | 2253 (8.9) | 2.57 (2.31–2.86) | <0.0001 | 1.26 (1.11–1.42) | 0.0003 |
| Diabetes mellitus | 17,704 (6.9) | 5900 (23.4) | 2.58 (2.39–2.80) | <0.0001 | 1.53 (1.41–1.66) | <0.0001 |
| High blood pressure | 45,614 (17.9) | 12,159 (48.2) | 2.92 (2.73–3.13) | <0.0001 | 1.89 (1.75–2.04) | <0.0001 |
| Heart failure | 3257 (1.3) | 1999 (7.9) | 3.44 (3.05–3.87) | <0.0001 | 1.61 (1.42–1.84) | <0.0001 |
| Chronic kidney disease | 7864 (3.1) | 4051 (16.1) | 3.23 (2.96–3.52) | <0.0001 | 1.72 (1.56–1.89) | <0.0001 |
| Respiratory disease | 39,608 (15.5) | 6323 (25.1) | 1.65 (1.53–1.77) | <0.0001 | 1.18 (1.09–1.28) | <0.0001 |
| Thromboembolism | 628 (0.2) | 268 (1.1) | 2.65 (1.93–3.64) | <0.0001 | 1.61 (1.15–2.26) | 0.0056 |
| Use of NSAIDs | 59,216 (23.2) | 7548 (29.9) | 1.21 (1.13–1.30) | <0.0001 | 1.30 (1.20–1.42) | <0.0001 |
| Antithrombotic medication | 11,290 (4.4) | 3860 (15.3) | 2.25 (2.07–2.45) | <0.0001 | 1.48 (1.33–1.65) | <0.0001 |
| Use of corticosteroids | 13,122 (5.1) | 1541 (6.1) | 1.10 (0.97–1.25) | 0.1513 | 1.14 (0.99–1.31) | 0.0773 |
| Low molecular weight heparin | 1147 (0.4) | 975 (3.9) | 4.62 (3.70–5.78) | <0.0001 | 4.54 (3.59–5.76) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llor, C.; Ouchi, D.; Giner-Soriano, M.; García-Sangenís, A.; Bjerrum, L.; Morros, R. Correlation between Previous Antibiotic Exposure and COVID-19 Severity. A Population-Based Cohort Study. Antibiotics 2021, 10, 1364. https://doi.org/10.3390/antibiotics10111364
Llor C, Ouchi D, Giner-Soriano M, García-Sangenís A, Bjerrum L, Morros R. Correlation between Previous Antibiotic Exposure and COVID-19 Severity. A Population-Based Cohort Study. Antibiotics. 2021; 10(11):1364. https://doi.org/10.3390/antibiotics10111364
Chicago/Turabian StyleLlor, Carl, Dan Ouchi, Maria Giner-Soriano, Ana García-Sangenís, Lars Bjerrum, and Rosa Morros. 2021. "Correlation between Previous Antibiotic Exposure and COVID-19 Severity. A Population-Based Cohort Study" Antibiotics 10, no. 11: 1364. https://doi.org/10.3390/antibiotics10111364