
Efficacy and Safety of Continuous Infusion of Vancomycin in Children: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Results
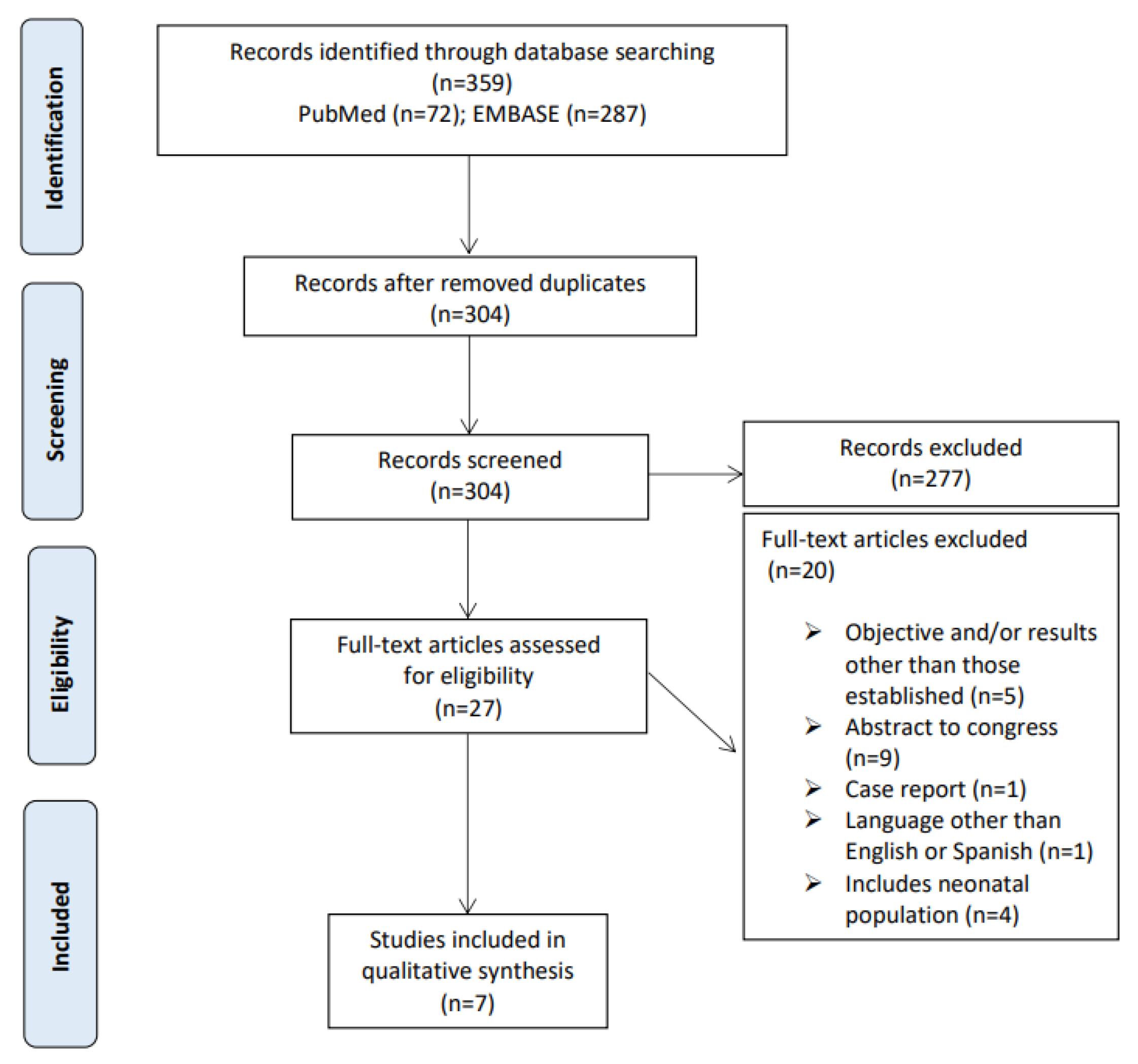
2.1. Bibliographic Search
2.2. Quality of the Included Studies
2.3. Characteristics of the Included Studies
2.4. Characteristics of Vancomycin Treatment
2.5. Target Attainment
2.6. Clinical Efficacy
2.7. Safety
3. Discussion
4. Materials and Methods
4.1. Selection Criteria
- Population: pediatric patients (age range: ≥1 month and ≤19 years) receiving treatment with vancomycin.
- Intervention: continuous infusion of vancomycin.
- Comparison: with comparator or without comparator.
- Outcomes: clinical efficacy or SVCs target attainment, the latter defined as reaching target serum concentrations.
- Study Design: clinical trials and observational studies.
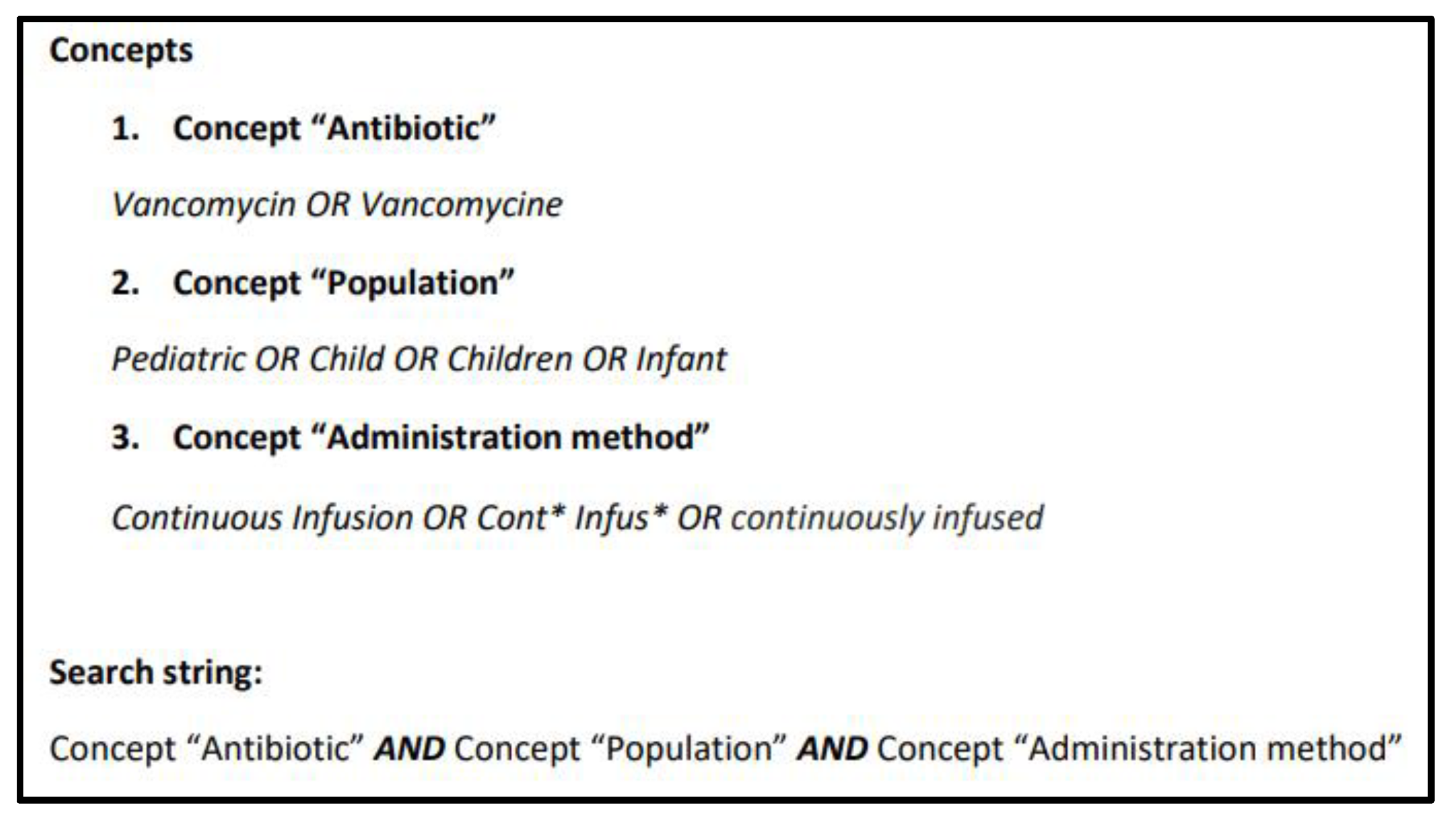
4.2. Data Sources
4.3. Study Selection
4.4. Quality Assessment
4.5. Data Extraction
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Man, S.S.K.; Carr, R.R.; Ensom, M.H.H. Comparison of Continuous and Intermittent IV Infusion of Vancomycin: Systematic Review. Can. J. Hosp. Pharm. 2010, 63, 373–381. [Google Scholar] [CrossRef] [Green Version]
- Girand, H.L. Continuous Infusion Vancomycin in Pediatric Patients: A Critical Review of the Evidence. J. Pediatr. Pharmacol. Ther. JPPT Off. J. PPAG 2020, 25, 198–214. [Google Scholar] [CrossRef] [PubMed]
- Tkachuk, S.; Collins, K.; Ensom, M.H.H. The Relationship Between Vancomycin Trough Concentrations and AUC/MIC Ratios in Pediatric Patients: A Qualitative Systematic Review. Pediatr. Drugs 2018, 20, 153–164. [Google Scholar] [CrossRef]
- Hwang, D.; Chiu, N.C.; Chang, L.; Peng, C.C.; Huang, D.T.; Huang, F.Y.; Chi, H. Vancomycin dosing and target attainment in children. J. Microbiol. Immunol. Infect. 2017, 50, 494–499. [Google Scholar] [CrossRef] [Green Version]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Pharm. 2020, 77, 835–864. [Google Scholar] [CrossRef] [Green Version]
- Fiorito, T.; Luther, M.K.; Dennehy, P.H.; LaPlante, K.; Matson, K.L. Nephrotoxicity with Vancomycin in the Pediatric Population: A Systematic Review and Meta-Analysis. Pediatr. Infect. Dis. J. 2018, 37, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children: Executive Summary. Clin. Infect. Dis. 2011, 52, 285–292. [Google Scholar] [CrossRef]
- Rybak, M.; Lomaestro, B.; Rotschafer, J.C.; Moellering, R.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am. J. Health Pharm. 2009, 66, 82–98. [Google Scholar] [CrossRef]
- Kishk, O.A.; Lardieri, A.B.; Heil, E.L.; Morgan, J.A. Vancomycin AUC/MIC and Corresponding Troughs in a Pediatric Population. J. Pediatr. Pharmacol. Ther. 2017, 22, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frymoyer, A.; Guglielmo, B.J.; Hersh, A.L. Desired Vancomycin Trough Serum Concentration for Treating Invasive Methicillin-resistant Staphylococcal Infections. Pediatr. Infect. Dis. J. 2013, 32, 1077–1079. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Luo, Y.; Quan, X.; Jiang, M.; Zhou, B. Intermittent vs. continuous vancomycin infusion for gram-positive infections: A systematic review and meta-analysis. J. Infect. Public Health 2020, 13, 591–597. [Google Scholar] [CrossRef]
- Van Maarseveen, E.M.; Gipmans, S.G.H.; Van Zanten, A.R.H. Exposure Variability and Target Attainment of Vancomycin: A Systematic Review Comparing Intermittent and Continuous Infusion. Ther. Drug Monit. 2020, 42, 381–391. [Google Scholar] [CrossRef]
- Hurst, A.L.; Baumgartner, C.; MacBrayne, C.E.; Child, J. Experience with Continuous Infusion Vancomycin Dosing in a Large Pediatric Hospital. J. Pediatr. Infect. Dis. Soc. 2018, 8, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Veluzat, S.; Pauquet, E.; Sarlangue, J. Practice survey on the use of vancomycin in pediatrics in the New Aquitaine region and guidelines of learned societies. Arch. Pédiatr. 2020, 27, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Genuini, M.; Oualha, M.; Bouazza, N.; Moulin, F.; Treluyer, J.-M.; Lesage, F.; Renolleau, S.; Benaboud, S. Achievement of Therapeutic Vancomycin Exposure with Continuous Infusion in Critically Ill Children. Pediatr. Crit. Care Med. 2018, 19, e263–e269. [Google Scholar] [CrossRef] [PubMed]
- Berthaud, R.; Benaboud, S.; Hirt, D.; Genuini, M.; Oualha, M.; Castelle, M.; Briand, C.; Artru, S.; Norsa, L.; Boyer, O.; et al. Early Bayesian Dose Adjustment of Vancomycin Continuous Infusion in Children in a Randomized Controlled Trial. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [PubMed]
- Hoegy, D.; Goutelle, S.; Garnier, N.; Rénard, C.; Faure-Conter, C.; Bergeron, C.; Bertrand, Y.; Bleyzac, N. Continuous intravenous vancomycin in children with normal renal function hospitalized in hematology-oncology: Prospective validation of a dosing regimen optimizing steady-state concentration. Fundam. Clin. Pharmacol. 2018, 32, 323–329. [Google Scholar] [CrossRef]
- Fung, L. Continuous Infusion Vancomycin for Treatment of Methicillin-Resistant Staphylococcus aureus in Cystic Fibrosis Patients. Ann. Pharmacother. 2012, 46, 1437. [Google Scholar] [CrossRef] [PubMed]
- McKamy, S.; Chen, T.; Lee, M.; Ambrose, P.J. Evaluation of a pediatric continuous-infusion vancomycin therapy guideline. Am. J. Health-Syst. Pharm. 2012, 69, 2066–2071. [Google Scholar] [CrossRef]
- Zylbersztajn, B.L.; Chicco, P.; Vega, L.; Centeno, M.; Filippini, S.; Ruvinsky, S. Continuous infusion of vancomycin in pediatric critical care. Arch. Argent. Pediatr. 2013, 111, e31-4. [Google Scholar] [CrossRef]
- Lopes, J.A.; Jorge, S. The RIFLE and AKIN classifications for acute kidney injury: A critical and comprehensive review. Clin. Kidney J. 2013, 6, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, J.E. Clinical Pharmacokinetics, 6th ed.; American Society of Health–System Pharmacists: Bethesda, MD, USA, 2016. [Google Scholar]
- Madigan, T.; Sieve, R.M.; Graner, K.K.; Banerjee, R. The Effect of Age and Weight on Vancomycin Serum Trough Concentrations in Pediatric Patients. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2013, 33, 1264–1272. [Google Scholar] [CrossRef] [Green Version]
- Le, J.; Bradley, J.S.; Murray, W.; Romanowski, G.L.; Tran, T.T.; Nguyen, N.; Cho, S.; Natale, S.; Bui, I.; Tran, T.M.; et al. Improved Vancomycin Dosing in Children Using Area Under the Curve Exposure. Pediatr. Infect. Dis. J. 2013, 32, e155–e163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waineo, M.F.; Kuhn, T.C.; Brown, D.L. The pharmacokinetic/pharmacodynamic rationale for administering vancomycin via continuous infusion. J. Clin. Pharm. Ther. 2015, 40, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Hao, J.-J.; Chen, H.; Zhou, J.-X. Continuous versus intermittent infusion of vancomycin in adult patients: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2016, 47, 28–35. [Google Scholar] [CrossRef]
- Cataldo, M.A.; Tacconelli, E.; Grilli, E.; Pea, F.; Petrosillo, N. Continuous versus intermittent infusion of vancomycin for the treatment of Gram-positive infections: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2011, 67, 17–24. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIH Study Quality Assessment Tools n.d. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 2 February 2021).



{kind=link}
{kind=link}
| Risk of Bias Due To | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Tool | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall Bias | ||
| Genuini M 2018 [15] | Robins | S | L | L | S | M | M | M | S | ||
| Hoegy D 2018 [17] | S | L | L | M | L | M | S | S | |||
| Hurst 2019 [13] | S | L | L | S | S | M | S | S | |||
| Study | Tool | Randomization Process | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall Bias | ||||
| Berthaud R 2019 [16] | ROB-2 | SC | SC | SC | L | SC | SC | ||||
| Study | Tool | Study Question | Population | Consecutive | Cases Comparable | Intervention | Measurement of Outcomes | Length of Follow up | Statistical Methods | Results | Overall |
| Fung L 2012 [18] | SQAT | Y | Y | CD | N | Y | Y | Y | NA | Y | FAIR |
| Zylbersztajn BL 2013 [20] | N | Y | N | N | Y | N | Y | NA | N | POOR | |
| McKamy S 2012 [19] | Y | Y | Y | N | Y | Y | Y | NA | Y | GOOD | |
| Reference | Type of Study | Comparator | Study Population | Main Objective | ||
|---|---|---|---|---|---|---|
| Characteristics and Number of Patients | Age | Sex | ||||
| Berthaud R 2019 [16] | single-center randomized controlled trial | yes (control group without early Bayesian dose adjustment) | 99 patients: 49 from Bayesian group 50 from control group | 3 months-old to 17 years-old | 48% (n = 48) males 52% (n = 51) females | to assess if an early Bayesian dose adjustment of vancomycin would increase the rate of target attainment in the first 24 h of treatment |
| Fung L 2012 [18] | case series study | no | 3 patients with cystic fibrosis | 3 years-old, 15 years-old and 17 years-old | 100% (n = 3) females | to achieve therapeutic serum concentrations with continuous infusions of vancomycin |
| Genuini M 2018 [15] | Retrospective observational single-center study | no | 28 critical ill patients | 1 month-old to 17 years-old | 21.42% (n = 6) males 78.58% (n = 22) females | Describe and assess a continuous infusion dosing scheme of vancomycin therapy in critically ill children |
| Hoegy D 2018 [17] | prospective study | no | 94 patients hospitalized in hematology-oncology ward | 4.3 months-old to 17.9 years-old | 50% (n = 47) males 50% (n = 47) females | to prospectively validate an age-based dosing regimen for continuous IV vancomycin |
| Hurst AL 2019 [13] | Retrospective observational single-center study | no | 240 patients (215 patients with CIV) | 1 month-old to 18 years-old | 60% (n = 144) males 40% (n = 100) females | to determine the total daily dose of CIV required to attain therapeutic serum vancomycin concentrations (SVCs) in pediatric patients according to age |
| McKamy S 2012 [19] | case series study | no | 15 patients with pneumonia (n = 10) or osteomyelitis (n = 5) | 6 months-old to 19 years-old (5.8 ± 6.1 years) | 86.66% (n = 13) males 13.34% (n = 2) females | to assess adverse effects, the achievement of target plateau SVCs at steady state and the adequacy of the empirical dosing strategy. |
| Zylbersztajn BL 2013 [20] | casa series study | no | 6 critical ill patients | 2 months-old–7 years-old | 66.66% (n = 4) males 33.33% (n = 2) females | to assess security and efficacy of CIV |
| Reference | Therapy Duration (Days) | Microorganism Isolated | Site of Infection | Empirical/Targeted Antimicrobial Therapy | Total Daily Dose on IIV before CIV | Final Total Daily Dose on CIV |
|---|---|---|---|---|---|---|
| Berthaud R 2019 [16] | At least 7 | Staphylococcus epidermidis (n = 17), Staphylococcus haemolyticus (n = 3), Staphylococcus hominis (n = 3), Staphylococcus capitis (n = 1), non-typeable CNS (n = 1), methicillin-sensitive Staphylococcus aureus (n = 3), Streptococcus mitis (n = 2), group A streptococcus (n = 1), and Enterococcus faecalis (n = 1) | blood | 34% (n = 28) targeted 72% (n = 71) empirical | NA | loading dose 14.9 (14.7–15) + 48 (44.6–59.2) mg/kg/day |
| Fung L 2012 [18] | 14–21 | MRSA | sputum | 100% targeted | 60–76 mg/kg/day | 30–50 mg/kg/day |
| Genuini M 2018 [15] | 4 (1–18) | CoNS (n = 11), Enterococcus faecalis (n = 1), Brevibacterium casei (n = 1), Staphylococcus aureus (n = 1), and Enterococcus avium (n = 1). | blood | 54% (n = 15) targeted 46% (n = 13) empirical | NA | loading dose 14.8 (12–16) mg/kg + 44 (35–61) mg/kg/day |
| Hoegy D 2018 [17] | no data | no data | no data | no data | NA | <2 years-old: 56.5 ±13.5 mg/kg/day 2–6 years-old: 51.9 ± 10.6 mg/kg/day 6–12 years-old: 46.6 ± 10.8 mg/kg/day >12 years-old: 40.7 ± 11.8 mg/kg/day |
| Hurst AL 2019 [13] | no data | Streptococcus species (n = 68), CoNs (n = 64), and MRSA (n = 31) were the most frequently isolated | blood, urine, cerebral spinal fluid, aspirate, and/or wound swab | 65% (n = 156) targeted 35% (n = 84) empirical | 10–15 mg/L: <2 years-old: 79.5 ± 9.6 mg/kg/day 2–8 years-old: 79.1 ± 8.5 mg/kg/day >8 years-old: 72.5 ± 12.6 mg/kg/day 15–20 mg/L: <2 years-old: 77.9 ± 12.4 mg/kg/day 2–8 years-old: 78.7 ± 10.9 mg/kg/day >8 years-old: 72.9 ± 13.8 mg/kg/day | 10–15 mg/L: <2 years-old: 48.4 ± 4.6 mg/kg/day 2–8 years-old: 45.6 ± 5.5 mg/kg/day >8 years-old: 39.4 ± 7.3 mg/kg/day 15–20 mg/L: <2 years-old: 47.7 ± 5.4 mg/kg/day 2–8 years-old: 46.8 ± 5.4 mg/kg/day >8 years-old: 43.6 ± 5.4 mg/kg/day |
| McKamy S 2012 [19] | 15.3 ± 23.1 | MRSA (n = 9) and Streptococcus pneumoniae (n = 3) | blood, urine | 100% targeted | 68.4 ± 5.8 mg/kg/day | 44.5 ± 12.6 mg/kg/day |
| Zylbersztajn BL 2013 [20] | 9–18 | MRSA (n = 6) | blood | 100% targeted | 40–80 mg/ kg/day | 50–60 mg/kg/day |
| Reference | Target Attaintment | Clinical Data | Safety Data | ||||
|---|---|---|---|---|---|---|---|
| SVTC (mg/L) | Measured SVC (Hours) | Therapeutic Concentrations in Range | Infra/Supratherapeutic SVC | AUC/MIC (mg·h/L) | |||
| Berthaud R 2019 [16] | 20–40 | within the first 24 h | 68% (n = 27) from the Bayesian group 38% (n = 16) from the control group | no data | AUC/MIC= 400–800: 85% (n = 34) from Bayesian group 57% (n = 27) from control group | sustainable apyrexia, C-reactive protein evolution and duration of bacteremia was not statistically different between groups (n = 43) | nephrotoxicity occurred in 12% (n = 10). Red man syndrome occurred in 4% (n = 4). |
| Fung L 2012 [18] | 15–20 | 24 h after the initiation of therapy | 0% (n = 0) | <15 mg/L: 33.33% (n = 1) >20 mg/L: 66.66% (n = 2) | AUC/MIC > 400: 66.66% (n = 2) AUC/MIC < 400: 33.33% (n = 1) | clinical improvement (n = 3) | no signs of nephrotoxicity |
| Genuini M 2018 [15] | 15–30 | within the first 48 h | first measured SVC: 43% (n = 12) second measured SVC 45% (n = 9) | no data | AUC/MIC > 400: 25% (n = 7) | no data | nephrotoxicity occurred in 11% (n = 3) |
| Hoegy D 2018 [17] | 14–21 | between 48 h and 96 h after the initiation of therapy | <2 years-old: 61.5% (n = 8) 2–6 years-old: 53.8% (n = 21) 6–12 years-old: 56.3% (n = 9) >12 years-old:65.4% (n = 17) | <14 mg/mL <2 years-old: 38.5% (n = 5) 2–6 years-old: 43.6% (n = 17) 6–12 years-old: 25.0% (n = 4) >12 years-old: 19.2% (n = 5) >21 mg/mL: < 2 years-old: 0% (n = 0) 2–6 years-old: 2.6% (n = 1) 6–12 years-old: 18.7% (n = 3) >12 years-old: 15.4% (n = 4) | no data | no data | no data |
| Hurst AL 2019 [13] | 10–15 15–20 | ≥23 h after the initiation of therapy | 10–15 mg/L: <2 years-old: 82% (n = 14) 2–8 years-old: 82% (n = 31) > 8 years-old: 67% (n = 14) 15–20 mg/L <2 years-old: 81% (n = 19) 2–8 years-old: 41% (n = 23) >years-old: 76% (n = 54) | no data | no data | no data | no signs of nephrotoxicity |
| McKamy S 2012 [19] | 15–20 | within the first 24–48 h | 27% (n = 4) | <15 mg/L: 20% (n = 3) >20 mg/L: 53% (n = 8) | no data | no data | no signs of nephrotoxicity |
| Zylbersztajn BL 2013 [20] | 10–25 | no data | 100% (n = 6) | NA | no data | clinical improvement (n = 6) and negative blood cultures (n = 4) | no signs of nephrotoxicity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Moreno, M.; Mejías-Trueba, M.; Herrera-Hidalgo, L.; Goycochea-Valdivia, W.A.; Gil-Navarro, M.V. Efficacy and Safety of Continuous Infusion of Vancomycin in Children: A Systematic Review. Antibiotics 2021, 10, 912. https://doi.org/10.3390/antibiotics10080912
Alonso-Moreno M, Mejías-Trueba M, Herrera-Hidalgo L, Goycochea-Valdivia WA, Gil-Navarro MV. Efficacy and Safety of Continuous Infusion of Vancomycin in Children: A Systematic Review. Antibiotics. 2021; 10(8):912. https://doi.org/10.3390/antibiotics10080912
Chicago/Turabian StyleAlonso-Moreno, Marta, Marta Mejías-Trueba, Laura Herrera-Hidalgo, Walter Alfredo Goycochea-Valdivia, and María Victoria Gil-Navarro. 2021. "Efficacy and Safety of Continuous Infusion of Vancomycin in Children: A Systematic Review" Antibiotics 10, no. 8: 912. https://doi.org/10.3390/antibiotics10080912