
An Evaluation of the Impact of an OPEN Stewardship Generated Feedback Intervention on Antibiotic Prescribing among Primary Care Veterinarians in Canada and Israel
 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Recruitment
2.3. Intervention
2.4. Data Extraction and Aggregation
2.5. Outcome
2.6. Statistical Analysis
3. Results
3.1. Study Participants
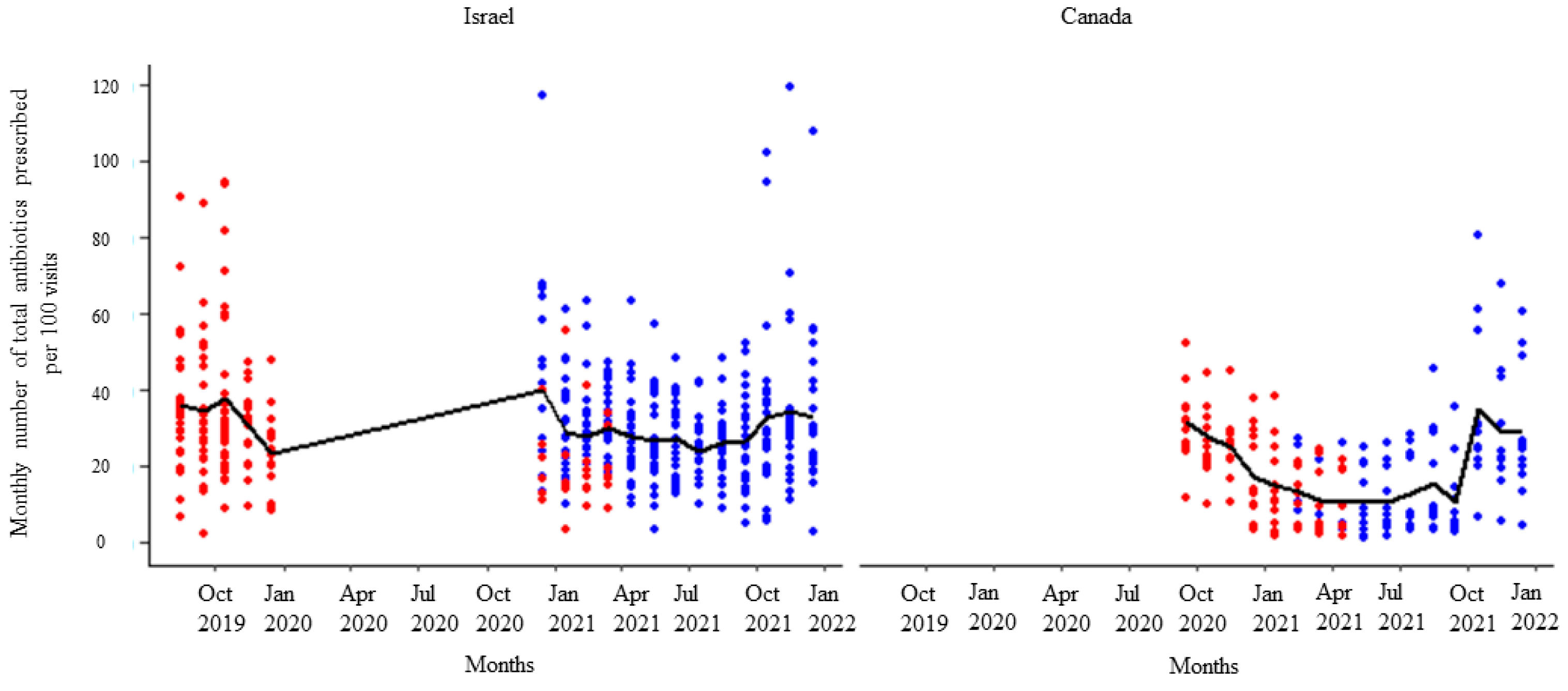
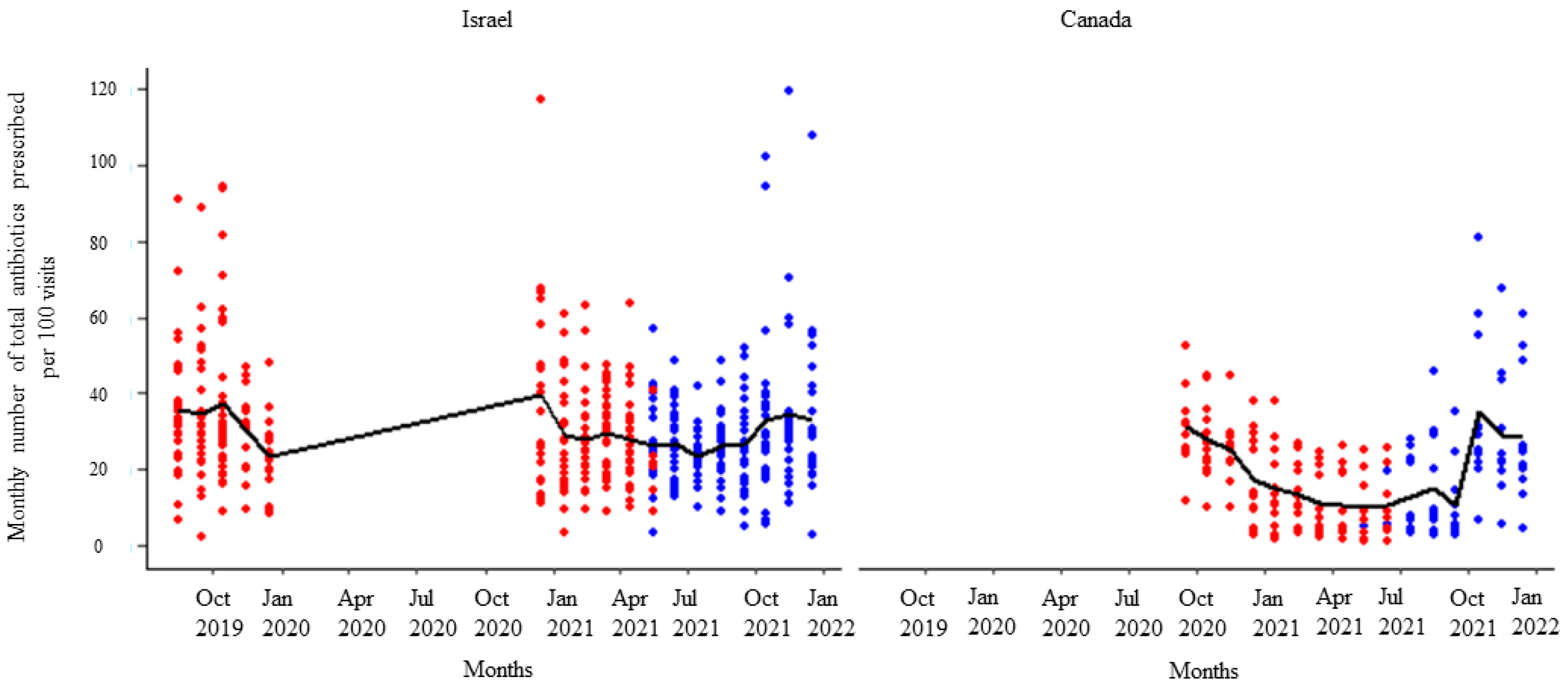
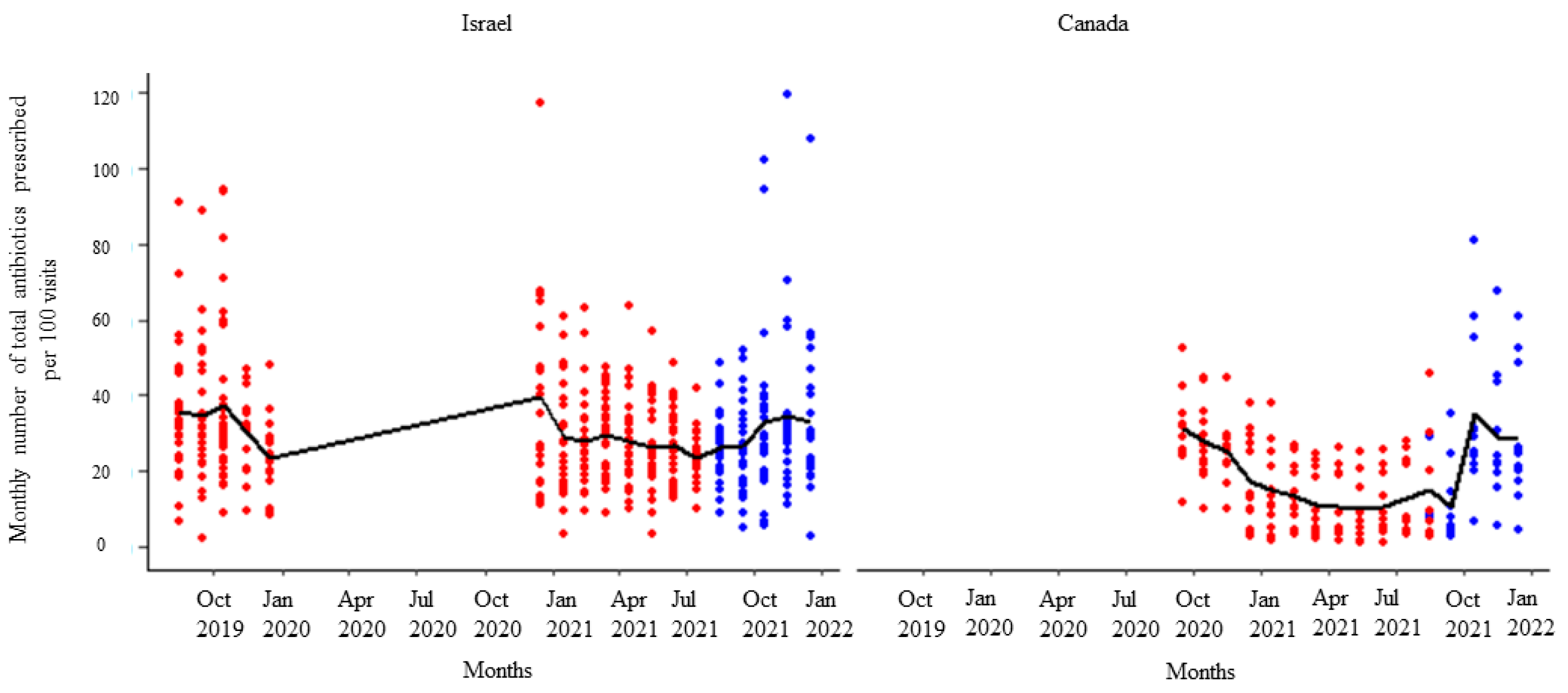
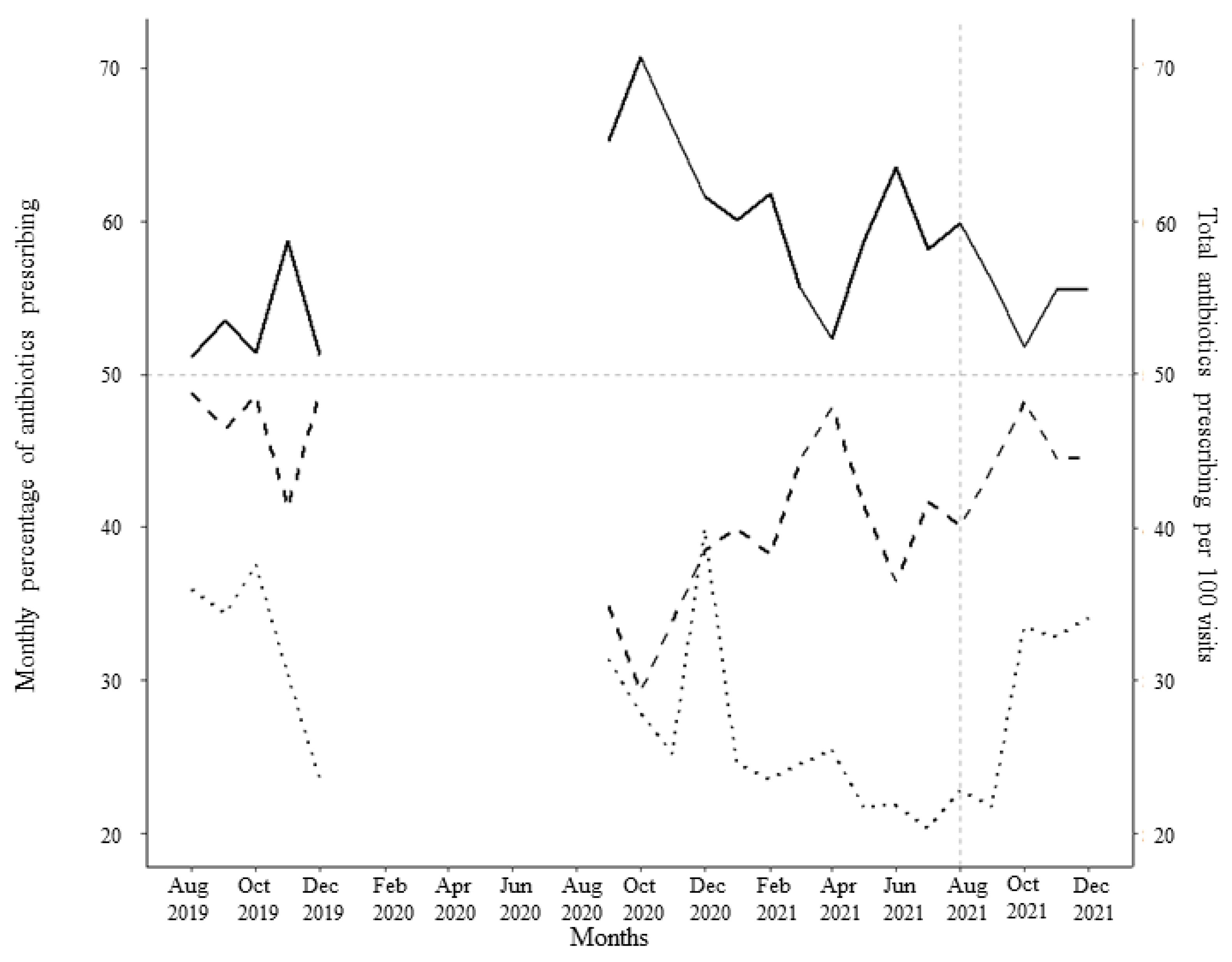
3.2. Antibiotic Prescribing
3.3. Multi-Level Generalized Linear Mixed Effect Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- World Organisation for Animal Health (OIE). OIE Annual Report on the Use of Antimicrobial Agents Intended for Use in Animals. Available online: http://www.oie.int/fileadmin/Home/eng/Our_scientific_expertise/docs/pdf/AMR/Annual_Report_AMR_3.pdf (accessed on 21 May 2019).
- Cockburn, R.; Newton, P.N.; Agyarko, E.K.; Akunyili, D.; White, N.J. The Global Threat of Counterfeit Drugs: Why Industry and Governments Must Communicate the Dangers. PLoS Med. 2005, 2, 0302–0308. [Google Scholar] [CrossRef]
- How Fake Animal Medicines Threaten African Livestock | World Economic Forum. Available online: https://www.weforum.org/agenda/2015/02/how-fake-animal-medicines-threaten-african-livestock/ (accessed on 25 November 2019).
- Buckley, G.J.; Gostin, L.O. Countering the Problem of Falsified and Substandard Drugs; National Academies Press: Washington, DC, USA, 2013; ISBN 0309269393. [Google Scholar]
- Hardefeldt, L.Y.; Browning, G.F.; Thursky, K.A.; Gilkerson, J.R.; Billman-Jacobe, H.; Stevenson, M.A.; Bailey, K.E. Cross-Sectional Study of Antimicrobials Used for Surgical Prophylaxis by Bovine Veterinary Practitioners in Australia. Vet. Rec. 2017, 181, 426. [Google Scholar] [CrossRef] [PubMed]
- IACG. No Time to Wait: Securing the Future from Drug-Resistant Infections. Available online: https://www.who.int/antimicrobial-resistance/interagency-coordination-group/IACG_final_report_EN.pdf?ua=1 (accessed on 13 June 2019).
- Holmes, A.H.; Moore, L.S.P.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J.V. V Understanding the Mechanisms and Drivers of Antimicrobial Resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, V.O.; Duffy, B. Use of Antibiotics in Plant Agriculture. Rev Sci Tech. 2012, 31, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Mcmanus, P.S.; Stockwell, V.O.; Sundin, G.W.; Jones, A.L. Antibiotic Use in Plant Agriculture. Annu. Rev. Phytopathol. 2002, 40, 443–465. [Google Scholar] [CrossRef] [PubMed]
- Larsson, D.G.J.; de Pedro, C.; Paxeus, N. Effluent from Drug Manufactures Contains Extremely High Levels of Pharmaceuticals. J. Hazard. Mater. 2007, 148, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.; Shen, Q.; Liu, F.; Ma, J.; Xu, G.; Wang, Y.; Wu, M. Antibiotic Resistance Gene Abundances Associated with Antibiotics and Heavy Metals in Animal Manures and Agricultural Soils Adjacent to Feedlots in Shanghai; China. J. Hazard. Mater. 2012, 235–236, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Diwan, V.; Tamhankar, A.J.; Khandal, R.K.; Sen, S.; Aggarwal, M.; Marothi, Y.; Iyer, R.V.; Sundblad-Tonderski, K.; Stålsby- Lundborg, C. Antibiotics and Antibiotic-Resistant Bacteria in Waters Associated with a Hospital in Ujjain, India. BMC Public Health 2010, 10, 414. [Google Scholar] [CrossRef] [PubMed]
- Price, L.B.; Stegger, M.; Hasman, H.; Aziz, M.; Larsen, J.; Andersen, P.S.; Pearson, T.; Waters, A.E.; Foster, J.T.; Schupp, J.; et al. Staphylococcus Aureus CC398: Host Adaptation and Emergence of Methicillin Resistance in Livestock. MBio 2012, 3, 1–6. [Google Scholar] [CrossRef]
- Robinson, T.P.; Wertheim, H.F.L.; Kakkar, M.; Kariuki, S.; Bu, D.; Price, L.B. Animal Production and Antimicrobial Resistance in the Clinic. Lancet 2016, 387, e1–e3. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global Increase and Geographic Convergence in Antibiotic Consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Brower, C.; Gilbert, M.; Grenfell, B.T.; Levin, S.A.; Robinson, T.P.; Teillant, A.; Laxminarayan, R.; Van Boeckel, T.P.; Brower, C.; et al. Global Trends in Antimicrobial Use in Food Animals. Proc. Natl. Acad. Sci. USA 2015, 112, 5649–5654. [Google Scholar] [CrossRef]
- Tang, K.L.; Caffrey, N.P.; Nóbrega, D.B.; Cork, S.C.; Ronksley, P.E.; Barkema, H.W.; Polachek, A.J.; Ganshorn, H.; Sharma, N.; Kellner, J.D.; et al. Restricting the Use of Antibiotics in Food-Producing Animals and Its Associations with Antibiotic Resistance in Food-Producing Animals and Human Beings: A Systematic Review and Meta-Analysis. Lancet Planet. Heal. 2017, 1, e316–e327. [Google Scholar] [CrossRef]
- Theuretzbacher, U.; Gottwalt, S.; Beyer, P.; Butler, M.; Czaplewski, L.; Lienhardt, C.; Moja, L.; Paul, M.; Paulin, S.; Rex, J.H.; et al. Analysis of the Clinical Antibacterial and Antituberculosis Pipeline. Lancet Infect. Dis. 2019, 19, e40–e50. [Google Scholar] [CrossRef]
- Butler, M.S.; Blaskovich, M.A.; Cooper, M.A. Antibiotics in the Clinical Pipeline at the End of 2015. J. Antibiot. 2017, 70, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Pan-Canadian Public Health Network. Antimicrobial Stewardship. Available online: http://www.phn-rsp.ca/pubs/anstew-gestan/index-eng.php#fnb5 (accessed on 5 February 2024).
- Mölstad, S.; Löfmark, S.; Carlin, K.; Erntell, M.; Aspevall, O.; Blad, L.; Hanberger, H.; Hedin, K.; Hellman, J.; Norman, C.; et al. Lessons Learnt during 20 Years of the Swedish Strategic Programme against Antibiotic Resistance. Bull. World Health Organ. 2017, 95, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Mateus, A.L.P.; Brodbelt, D.C.; Barber, N.; Stärk, K.D.C. Qualitative Study of Factors Associated with Antimicrobial Usage in Seven Small Animal Veterinary Practices in the UK. Prev. Vet. Med. 2014, 117, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Brown, E.; Charani, E.; Fenelon, L.; Gould, I.M.; Holmes, A.; Ramsay, C.R.; Wiffen, P.J.; Wilcox, M. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2013, 2013, 870. [Google Scholar] [CrossRef]
- Drekonja, D.M.; Filice, G.A.; Greer, N.; Olson, A.; MacDonald, R.; Rutks, I.; Wilt, T.J. Antimicrobial Stewardship in Outpatient Settings: A Systematic Review. Infect. Control Hosp. Epidemiol. 2015, 36, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Kliemann, B.S.; Levin, A.S.; Moura, M.L.; Boszczowski, I.; Lewis, J.J. Socioeconomic Determinants of Antibiotic Consumption in the State of São Paulo, Brazil: The Effect of Restricting Over-The-Counter Sales. PLoS ONE 2016, 11, e0167885. [Google Scholar] [CrossRef] [PubMed]
- Gould, I. Benefits of Antimicrobial Stewardship in Hospitals: Evidence from a Recent Cochrane Review. J. Microbiol. Immunol. Infect. 2015, 48, S24. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [PubMed]
- Wierup, M. The Swedish Experience of the 1986 Year Ban of Antimicrobial Growth Promoters, with Special Reference to Animal Health, Disease Prevention, Productivity, and Usage of Antimicrobials. Microb Drug Resist. 2001, 2, 183–190. [Google Scholar] [CrossRef]
- Aarestrup, F.M.; Seyfarth, A.M.; Emborg, H.-D.; Pedersen, K.; Hendriksen, R.S.; Bager, F. Effect of Abolishment of the Use of Antimicrobial Agents for Growth Promotion on Occurrence of Antimicrobial Resistance in Fecal Enterococci from Food Animals in Denmark. Antimicrob. Agents Chemother. 2001, 45, 2054–2059. [Google Scholar] [CrossRef] [PubMed]
- Dutil, L.; Irwin, R.; Finley, R.; Ng, L.K.; Avery, B.; Boerlin, P.; Bourgault, A.M.; Cole, L.; Daignault, D.; Desruisseau, A.; et al. Ceftiofur Resistance in Salmonella Enterica Serovar Heidelberg from Chicken Meat and Humans, Canada. Emerg. Infect. Dis. 2010, 16, 48–54. [Google Scholar] [CrossRef]
- Ivers, N.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.D.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and Feedback: Effects on Professional Practice and Healthcare Outcomes. Cochrane Database Syst. Rev. 2012, 6, CD000259. [Google Scholar] [CrossRef]
- Chung, G.W.; Wu, J.E.; Yeo, C.L.; Chan, D.; Hsu, L.Y. Antimicrobial Stewardship: A Review of Prospective Audit and Feedback Systems and an Objective Evaluation of Outcomes. Virulence 2013, 4, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Grimshaw, J.M.; Shirran, L.; Thomas, R.; Mowatt, G.; Fraser, C.; Bero, L.; Grilli, R.; Harvey, E.; Oxman, A.; O’Brien, M.A. Changing Provider Behavior: An Overview of Systematic Reviews of Interventions. Med. Care 2001, 39, II-2–II-45. [Google Scholar] [CrossRef]
- Sanchez, G.V.; Fleming-Dutra, K.E.; Roberts, R.M.; Hicks, L.A. Core Elements of Outpatient Antibiotic Stewardship. MMWRRecomm. Rep. 2016, 65, 1–12. [Google Scholar] [CrossRef]
- Acharya, K.R.; Brankston, G.; Soucy, J.P.R.; Cohen, A.; Hulth, A.; Löfmark, S.; Davidovitch, N.; Ellen, M.; Fisman, D.N.; Moran-Gilad, J.; et al. Evaluation of an OPEN Stewardship Generated Feedback Intervention to Improve Antibiotic Prescribing among Primary Care Veterinarians in Ontario, Canada and Israel: Protocol for Evaluating Usability and an Interrupted Time-Series Analysis. BMJ Open. 2021, 11, e039760. [Google Scholar] [CrossRef]
- Hardefeldt, L.Y.; Gilkerson, J.R.; Billman-Jacobe, H.; Stevenson, M.A.; Thursky, K.; Bailey, K.E.; Browning, G.F. Barriers to and Enablers of Implementing Antimicrobial Stewardship Programs in Veterinary Practices. J. Vet. Intern. Med. 2018, 32, 1092–1099. [Google Scholar] [CrossRef]
- Doherty, C. Reaching New Heights: Results of the 2018 CVMA Practice Owners Economic Survey. Can. Vet. J. 2019, 60, 315–318. [Google Scholar]
- Hulth, A.; Löfmark, S.; Andre, J.; Chorney, R.; Cohn, E.; Ellen, M.; Davidovitch, N.; Moran-Gilad, J.; Greer, A.; Fisman, D.; et al. A Tool for Promoting Responsible Antibiotic Prescribing across Settings and Sectors. Online J. Public Health Inform. 2019, 11, e322. [Google Scholar] [CrossRef]
- Bernam, T. Promoting Intelligent Use of Antibiotics in Farm Animals: Strengthening Regulation on Preparations Veterinary Literature Review, Mapping of Regulatory Processes and Recommendations for Action; Department of Pharmacy and the Environment Health at the Ministry of Health: Jerusalem, Israel, 2020.
- Canadian Veterinary Medical Association. Antimicrobial Resistance, Surveillance and Stewardship. Available online: https://www.canadianveterinarians.net/policy-and-outreach/priority-areas/antimicrobial-resistance-surveillance-and-stewardship/ (accessed on 5 February 2024).
- Health Canada. Responsible Use of Medically Important Antimicrobials in Animals. Available online: https://www.canada.ca/en/public-health/services/antibiotic-antimicrobial-resistance/animals/actions/responsible-use-antimicrobials.html (accessed on 11 March 2022).
- Public Health Agency of Canada. Canadian Integrated Program for Antimicrobial Resistance Surveillance (CIPARS) 2018: Integrated Findings. Available online: https://www.canada.ca/en/public-health/services/surveillance/canadian-integrated-program-antimicrobial-resistance-surveillance-cipars/cipars-reports/2018-annual-report-integrated-findings.html (accessed on 28 May 2022).
- Public Health Agency of Canada. Veterinary Antimicrobial Sales Reporting. Available online: https://www.canada.ca/en/public-health/services/antibiotic-antimicrobial-resistance/animals/veterinary-antimicrobial-sales-reporting.html (accessed on 5 February 2024).
- Soucy, J.P.R.; Low, M.; Acharya, K.R.; Ellen, M.; Hulth, A.; Löfmark, S.; Garber, G.E.; Watson, W.; Moran-Gilad, J.; Fisman, D.N.; et al. Evaluation of an Automated Feedback Intervention to Improve Antimicrobial Prescribing among Primary Care Physicians (OPEN Stewardship): Protocol for an Interrupted Time-Series and Usability Analysis in Ontario, Canada and Southern Israel. BMJ Open 2021, 11, e039810. [Google Scholar] [CrossRef]
- OIE. OIE List of Antimicrobial Agents of Veterinary Importance. Available online: https://www.oie.int/fileadmin/Home/eng/Our_scientific_expertise/docs/pdf/AMR/A_OIE_List_antimicrobials_July2019.pdf (accessed on 28 October 2020).
- WHO. WHO List of Critically Important Antimicrobials for Human Medicine (WHO CIA List). Available online: https://www.who.int/foodsafety/publications/antimicrobials-sixth/en/ (accessed on 21 May 2019).
- Weese, J.S.; Blondeau, J.; Boothe, D.; Guardabassi, L.G.; Gumley, N.; Papich, M.; Jessen, L.R.; Lappin, M.; Rankin, S.; Westropp, J.L.; et al. International Society for Companion Animal Infectious Diseases (ISCAID) Guidelines for the Diagnosis and Management of Bacterial Urinary Tract Infections in Dogs and Cats. Vet. J. 2019, 247, 8–25. [Google Scholar] [CrossRef]
- Lappin, M.R.; Blondeau, J.; Boothe, D.; Breitschwerdt, E.B.; Guardabassi, L.; Lloyd, D.H.; Papich, M.G.; Rankin, S.C.; Sykes, J.E.; Turnidge, J.; et al. Antimicrobial Use Guidelines for Treatment of Respiratory Tract Disease in Dogs and Cats: Antimicrobial Guidelines Working Group of the International Society for Companion Animal Infectious Diseases. J. Vet. Intern. Med. 2017, 31, 279–294. [Google Scholar] [CrossRef]
- Health Canada. Drug Product Database Online Query. Available online: https://health-products.canada.ca/dpd-bdpp/index-eng.jsp (accessed on 30 March 2022).
- Lopez Bernal, J.; Cummins, S.; Gasparrini, A. Interrupted Time Series Regression for the Evaluation of Public Health Interventions: A Tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Gelman, A.; Hill, J. Data Analysis Using Regression and Multilevel/Hierarchical Models; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar] [CrossRef]
- Taljaard, M.; McKenzie, J.E.; Ramsay, C.R.; Grimshaw, J.M. The Use of Segmented Regression in Analysing Interrupted Time Series Studies: An Example in Pre-Hospital Ambulance Care. Implement. Sci. 2014, 9, 77. [Google Scholar] [CrossRef]
- Gebski, V.; Ellingson, K.; Edwards, J.; Jernigan, J.; Kleinbaum, D.D. Modelling Interrupted Time Series to Evaluate Prevention and Control of Infection in Healthcare. Epidemiol. Infect. 2019, 140, 2131–2141. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Mächler, M.; Bolker, B.M.; Walker, S.C. Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis, 2nd, ed.; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Ryu, S.; Lau, C.L.; Chun, B.C. The Impact of Livestock Manure Control Policy on Human Leptospirosis in Republic of Korea Using Interrupted Time Series Analysis. Epidemiol. Infect. 2017, 145, 1320–1325. [Google Scholar] [CrossRef] [PubMed]
- CDC. The Core Elements of Hospital Antibiotic Stewardship Programs: 2019. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html. (accessed on 28 May 2022).
- Murphy, C.P.; Reid-Smith, R.J.; Boerlin, P.; Weese, J.S.; Prescott, J.F.; Janecko, N.; McEwen, S.A. Out-Patient Antimicrobial Drug Use in Dogs and Cats for New Disease Events from Community Companion Animal Practices in Ontario. Can. Vet. J. 2012, 53, 291–298. [Google Scholar] [PubMed]
- Oliveira, L.; Ruegg, P.L. Treatments of Clinical Mastitis Occurring in Cows on 51 Large Dairy Herds in Wisconsin. J. Dairy Sci. 2014, 97, 5426–5436. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Prescription Drug List. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/prescription-drug-list/list.html#a2 (accessed on 5 February 2024).
- Saini, V.; McClure, J.T.; Léger, D.; Dufour, S.; Sheldon, A.G.; Scholl, D.T.; Barkema, H.W. Antimicrobial Use on Canadian Dairy Farms. J. Dairy Sci. 2012, 95, 1209–1221. [Google Scholar] [CrossRef]
- McIsaac, W.; Kukan, S.; Huszti, E.; Szadkowski, L.; O’Neill, B.; Virani, S.; Ivers, N.; Lall, R.; Toor, N.; Shah, M.; et al. A Pragmatic Randomized Trial of a Primary Care Antimicrobial Stewardship Intervention in Ontario, Canada. BMC Fam. Pract. 2021, 22, 185. [Google Scholar] [CrossRef] [PubMed]
- McKay, R.M.; Vrbova, L.; Fuertes, E.; Chong, M.; David, S.; Dreher, K.; Purych, D.; Blondel-Hill, E.; Henry, B.; Marra, F.; et al. Evaluation of the Do Bugs Need Drugs? Program in British Columbia: Can We Curb Antibiotic Prescribing? Can. J. Infect. Dis. Med. Microbiol. 2011, 22, 19–24. [Google Scholar] [CrossRef]
- Mair, T.S.; Lockett, E. The Impact of COVID-19 on Equine Veterinary Practice and Mental Wellbeing. Equine Vet. Educ. 2021, 33, 6–9. [Google Scholar] [CrossRef]
- Morris, A.; Wu, H.; Morales, C. Barriers to Care in Veterinary Services: Lessons Learned From Low-Income Pet Guardians’ Experiences at Private Clinics and Hospitals During COVID-19. Front. Vet. Sci. 2021, 8, 1227. [Google Scholar] [CrossRef]
- Lardé, H.; Dufour, S.; Archambault, M.; Léger, D.; Loest, D.; Roy, J.-P.; Francoz, D. Assignment of Canadian Defined Daily Doses and Canadian Defined Course Doses for Quantification of Antimicrobial Usage in Cattle. Front. Vet. Sci. 2020, 7, 10. [Google Scholar] [CrossRef]
- Sanders, P.; Mevius, D.; Veldman, K.; van Geijlswijk, I.; Wagenaar, J.A.; Bonten, M.; Heederik, D. Comparison of Different Antimicrobial Use Indicators and Antimicrobial Resistance Data in Food-Producing Animals. JAC-Antimicrob. Resist. 2021, 3, dlab172. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Summary Statistics | Monthly Antibiotics Prescribing | Days Worked per Month | Total Visits per Month | ||||
|---|---|---|---|---|---|---|---|---|
| Critical | Other | Total | Broad-Spectrum | Narrow-Spectrum | ||||
| Israel | Min | 0.00 | 0.00 | 1.00 | 0.00 | 0.00 | 1.00 | 5.00 |
| First quartile | 7.00 | 3.00 | 11.00 | 4.00 | 5.00 | 12.00 | 39.00 | |
| median | 12.00 | 6.00 | 18.00 | 8.00 | 10.00 | 16.00 | 70.00 | |
| Mean | 14.32 | 7.45 | 21.78 | 10.30 | 11.48 | 15.35 | 77.00 | |
| Third quartile | 19.00 | 10.00 | 30.00 | 14.00 | 16.00 | 19.00 | 109.00 | |
| Max | 78.00 | 34.00 | 98.00 | 78.00 | 64.00 | 26.00 | 225.00 | |
| Canada | Min | 1.00 | 0.00 | 3.00 | 0.00 | 1.00 | 6.00 | 24.00 |
| First quartile | 4.00 | 4.00 | 9.00 | 2.00 | 5.00 | 17.00 | 90.00 | |
| median | 7.00 | 8.00 | 18.00 | 4.00 | 10.00 | 21.00 | 131.00 | |
| Mean | 11.69 | 13.41 | 25.10 | 6.24 | 18.86 | 20.64 | 156.92 | |
| Third quartile | 16.00 | 16.00 | 35.00 | 9.00 | 24.00 | 25.00 | 216.00 | |
| Max | 103.00 | 68.00 | 160.00 | 29.00 | 139.00 | 31.00 | 488.00 | |
| Fixed Effects | Incidence Rate Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Intercept | 0.32 (0.27, 0.37) | <0.01 |
| Region | <0.01 | |
| Israel | 1.00 | |
| Canada | 0.56 (0.41, 0.76) | |
| Feedback 1 | 0.88 (0.79, 0.98) | 0.02 |
| Feedback 2 | 0.85 (0.75, 0.97) | 0.01 |
| Feedback 3 | 1.38 (1.23, 1.56) | <0.01 |
| Fixed Effects | Incidence Rate Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Intercept | 0.21 (0.18, 0.24) | <0.01 |
| Region | <0.01 | |
| Israel | 1.00 | |
| Canada | 0.39 (0.29, 0.52) | |
| Feedback 1 | 0.87 (0.77, 0.98) | 0.02 |
| Feedback 2 | 0.80 (0.70, 0.93) | <0.01 |
| Feedback 3 | 1.49 (1.30, 1.70) | <0.01 |
| Fixed Effects | Incidence Rate Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Intercept | 0.15 (0.12, 0.18) | <0.01 |
| Region | <0.01 | |
| Israel | 1.00 | |
| Canada | 0.30 (0.21, 0.43) | |
| Feedback 1 | 0.86 (0.76, 0.98) | 0.02 |
| Feedback 2 | 0.81 (0.69, 0.94) | 0.01 |
| Feedback 3 | 1.48 (1.28, 1.71) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acharya, K.R.; Cohen, A.; Brankston, G.; Soucy, J.-P.R.; Hulth, A.; Löfmark, S.; Brownstein, J.S.; Davidovich, N.; Ellen, M.E.; Fisman, D.N.; et al. An Evaluation of the Impact of an OPEN Stewardship Generated Feedback Intervention on Antibiotic Prescribing among Primary Care Veterinarians in Canada and Israel. Animals 2024, 14, 626. https://doi.org/10.3390/ani14040626
Acharya KR, Cohen A, Brankston G, Soucy J-PR, Hulth A, Löfmark S, Brownstein JS, Davidovich N, Ellen ME, Fisman DN, et al. An Evaluation of the Impact of an OPEN Stewardship Generated Feedback Intervention on Antibiotic Prescribing among Primary Care Veterinarians in Canada and Israel. Animals. 2024; 14(4):626. https://doi.org/10.3390/ani14040626
Chicago/Turabian StyleAcharya, Kamal R., Adar Cohen, Gabrielle Brankston, Jean-Paul R. Soucy, Anette Hulth, Sonja Löfmark, John S. Brownstein, Nadav Davidovich, Moriah E. Ellen, David N. Fisman, and et al. 2024. "An Evaluation of the Impact of an OPEN Stewardship Generated Feedback Intervention on Antibiotic Prescribing among Primary Care Veterinarians in Canada and Israel" Animals 14, no. 4: 626. https://doi.org/10.3390/ani14040626