
Autonomous Quality Control of Joint Orientation Measured with Inertial Sensors

Abstract
:1. Introduction
2. Materials and Methods
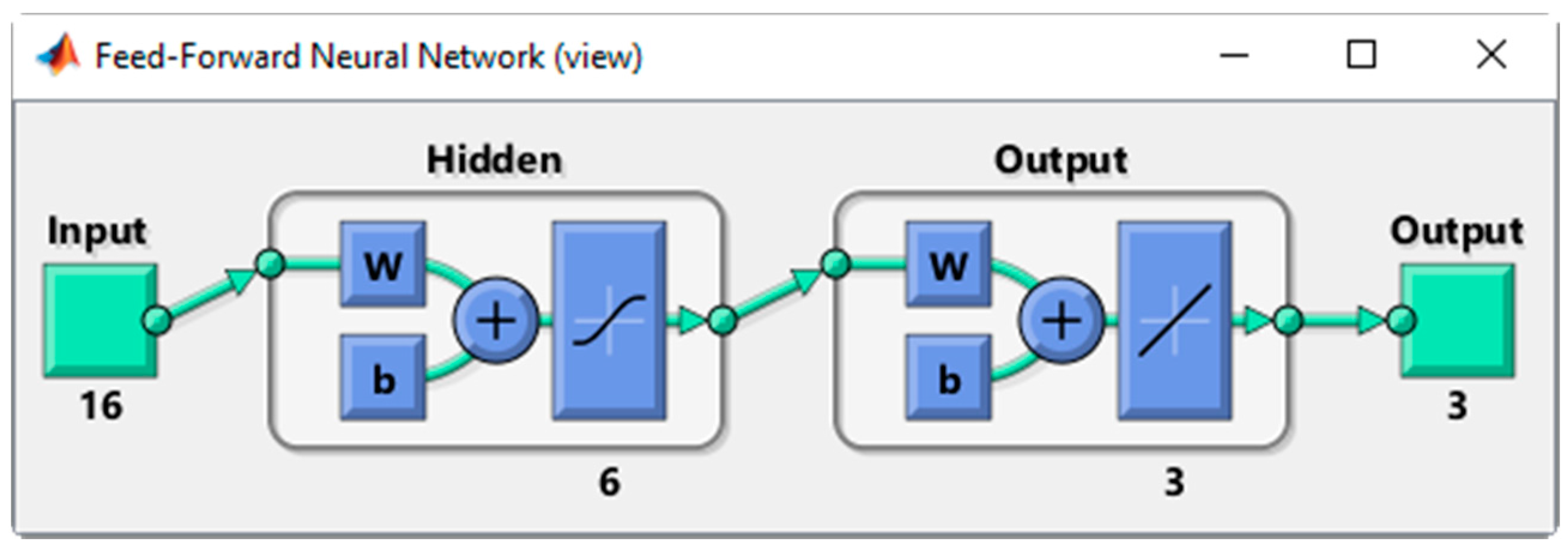
2.1. ANN Features
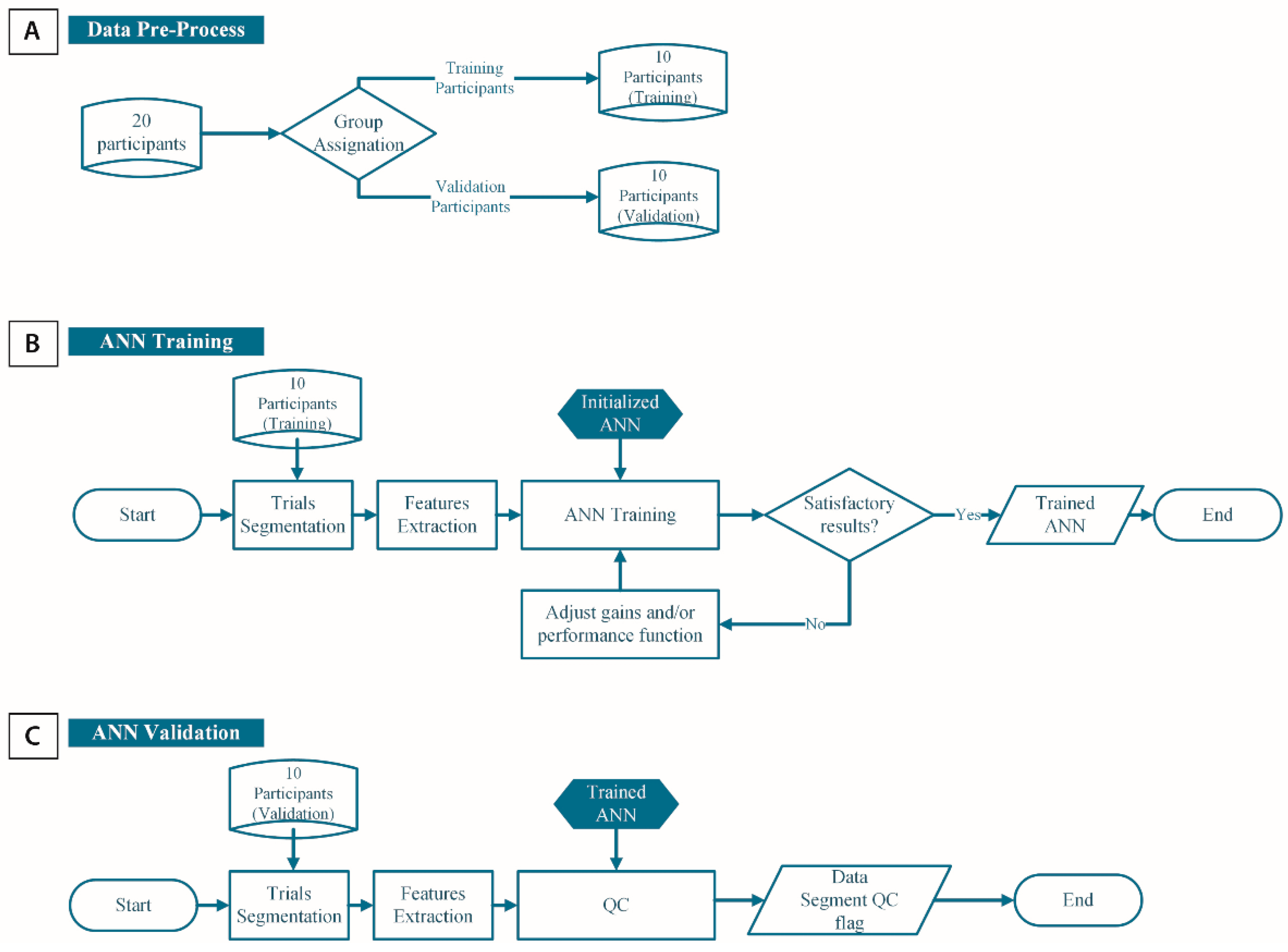
2.2. Quality Control Algorithm
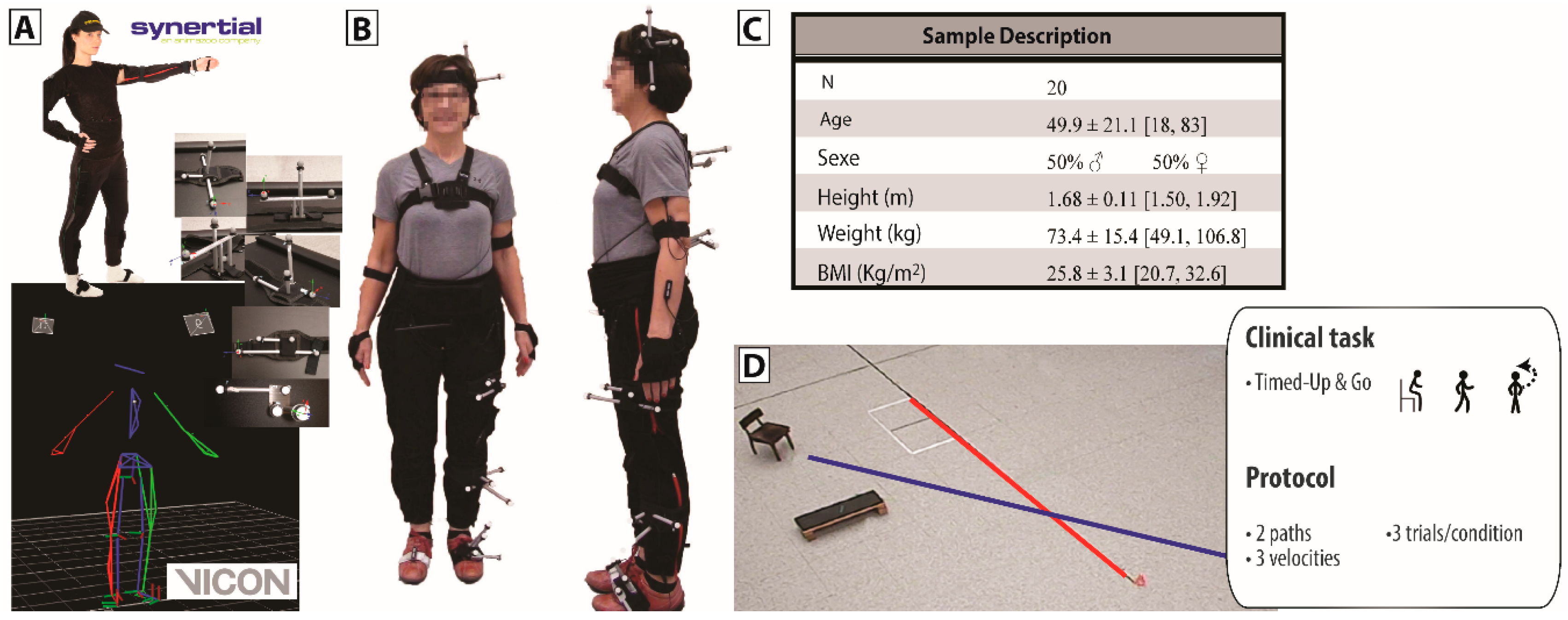
2.3. Experimental Procedure
2.4. Outcome Measures
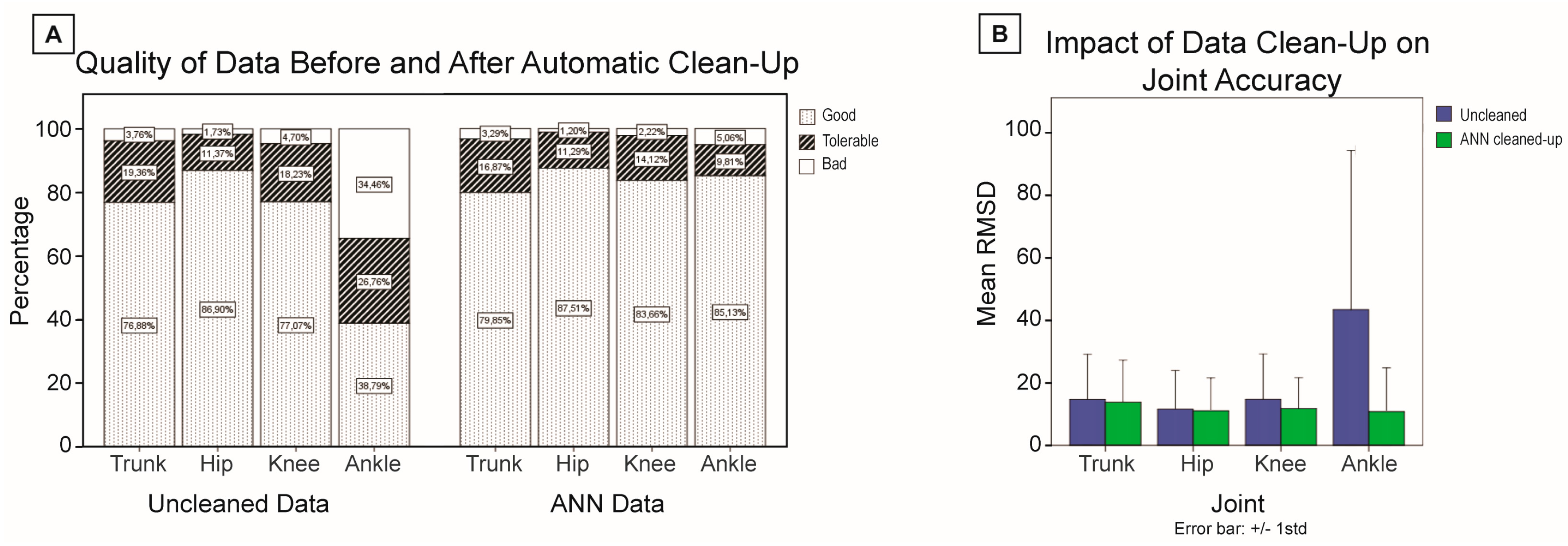
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AHRS | Attitude and Heading Reference System |
| ANN | Artificial Neural Network |
| IMU | Inertial Measurement Unit |
References
- Horak, F.; King, L.; Mancini, M. Role of body-worn movement monitor technology for balance and gait rehabilitation. Phys. Ther. 2015, 95, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Ferrari, A.; Garofalo, P.; Raggi, M.; Cappello, A. ‘Outwalk’: A protocol for clinical gait analysis based on inertial and magnetic sensors. Med. Biol. Eng. Comput. 2010, 48, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; El-Gohary, M.; Pearson, S.; McNames, J.; Schlueter, H.; Nutt, J.G.; King, L.A.; Horak, F.B. Continuous monitoring of turning in parkinson’s disease: Rehabilitation potential. NeuroRehabilitation 2015, 37, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. Itug, a sensitive and reliable measure of mobility. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Schlueter, H.; El-Gohary, M.; Mattek, N.; Duncan, C.; Kaye, J.; Horak, F.B. Continuous monitoring of turning mobility and its association to falls and cognitive function: A pilot study. J. Gerontol. A Biol. Sci. Med. Sci. 2016. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Zampieri, C.; Horak, F.B.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. Analyzing 180 degrees turns using an inertial system reveals early signs of progression of parkinson’s disease. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 224–227.
- Henderson, E.J.; Lord, S.R.; Brodie, M.A.; Gaunt, D.M.; Lawrence, A.D.; Close, J.C.T.; Whone, A.L.; Ben-Shlomo, Y. Rivastigmine for gait stability in patients with parkinson’s disease (respond): A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. 2016, 15, 249–258. [Google Scholar] [CrossRef]
- Picerno, P.; Cereatti, A.; Cappozzo, A. Joint kinematics estimate using wearable inertial and magnetic sensing modules. Gait Posture 2008, 28, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Brodie, M.A.; Walmsley, A.; Page, W. Dynamic accuracy of inertial measurement units during simple pendulum motion. Comput. Methods Biomech. Biomed. Eng. 2008, 11, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Brodie, M.A.; Walmsley, A.; Page, W. The static accuracy and calibration of inertial measurement units for 3D orientation. Comput. Methods Biomech. Biomed. Eng. 2008, 11, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Godwin, A.; Agnew, M.; Stevenson, J. Accuracy of inertial motion sensors in static, quasistatic, and complex dynamic motion. J. Biomech. Eng. 2009, 131, 114501. [Google Scholar] [CrossRef] [PubMed]
- Lebel, K.; Boissy, P.; Hamel, M.; Duval, C. Inertial measures of motion for clinical biomechanics: Comparative assessment of accuracy under controlled conditions—Effect of velocity. PLoS ONE 2013, 8, e79945. [Google Scholar] [CrossRef] [PubMed]
- Lebel, K.; Boissy, P.; Hamel, M.; Duval, C. Inertial measures of motion for clinical biomechanics: Comparative assessment of accuracy under controlled conditions—Changes in accuracy over time. PLoS ONE 2015, 10, e0118361. [Google Scholar] [CrossRef] [PubMed]
- Brückner, H.P.; Krüger, B.; Blume, H. Reliable orientation estimation for mobile motion capturing in medical rehabilitation sessions based on inertial measurement units. Microelectron. J. 2014, 45, 1603–1611. [Google Scholar] [CrossRef]
- Roetenberg, D.; Luinge, H.; Veltink, P. Inertial and magnetic sensing of human movement near ferromagnetic materials. In Proceedings of the 2nd IEEE/ACM International Symposium on Mixed and Augmented Reality, Waskington, DC, USA, 7–10 October 2003; pp. 268–269.
- Bachmann, E.R.; Yun, X.; Peterson, C.W. An investigation of the effects of magnetic variations on inertial/magnetic orientation sensors. In Proceedings of the 2004 IEEE International Conference on Robotics and Automation (ICRA ‘04), New Orleans, LA, USA, 26 April–1 May 2004; pp. 1115–1122.
- de Vries, W.H.K.; Veeger, H.E.J.; Baten, C.T.M.; van der Helm, F.C.T. Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.; Matsuoka, Y.; Wei-Tech, A. An efficient real-time human posture tracking algorithm using low-cost inertial and magnetic sensors. In Proceedings of the 2004 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2004), Sendai, Japan, 28 September–2 October 2004; pp. 2967–2972.
- Ferrari, A.; Cutti, A.G.; Garofalo, P.; Raggi, M.; Heijboer, M.; Cappello, A.; Davalli, A. First in vivo assessment of “outwalk”: A novel protocol for clinical gait analysis based on inertial and magnetic sensors. Med. Biol. Eng. Comput. 2010, 48, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Esser, P.; Dawes, H.; Collett, J.; Feltham, M.G.; Howells, K. Validity and inter-rater reliability of inertial gait measurements in Parkinson’s disease: A pilot study. J. Neurosci. Methods 2012, 205, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Rouhani, H.; Favre, J.; Crevoisier, X.; Aminian, K. Measurement of multi-segment foot joint angles during gait using a wearable system. J. Biomech. Eng. 2012, 134, 061006. [Google Scholar] [CrossRef] [PubMed]
- Seel, T.; Raisch, J.; Schauer, T. IMU-based joint angle measurement for gait analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, E.; Ligorio, G.; Summa, A.; Vannozzi, G.; Cappozzo, A.; Sabatini, A.M. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: Accuracy assessment in manual and locomotion tasks. Sensors 2014, 14, 18625–18649. [Google Scholar] [CrossRef] [PubMed]
- Roetenberg, D.; Baten, C.T.M.; Veltink, P.H. Estimating body segment orientation by applying inertial and magnetic sensing near ferromagnetic materials. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Plamondon, A.; Delisle, A.; Larue, C.; Brouillette, D.; McFadden, D.; Desjardins, P.; Larivière, C. Evaluation of a hybrid system for three-dimensional measurement of trunk posture in motion. Appl. Ergon. 2007, 38, 697–712. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Nussbaum, M.A. Performance evaluation of a wearable inertial motion capture system for capturing physical exposures during manual material handling tasks. Ergonomics 2012, 56, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Kendell, C.; Lemaire, E.D. Effect of mobility devices on orientation sensors that contain magnetometers. J. Rehabil. Res. Dev. 2009, 46, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Palermo, E.; Rossi, S.; Patanè, F.; Cappa, P. Experimental evaluation of indoor magnetic distortion effects on gait analysis performed with wearable inertial sensors. Physiol. Meas. 2014, 35, 399. [Google Scholar] [CrossRef] [PubMed]
- Roetenberg, D.; Luinge, H.J.; Baten, C.T.M.; Veltink, P.H. Compensation of magnetic disturbances improves inertial and magnetic sensing of human body segment orientation. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Yadav, N.; Bleakley, C. Accurate orientation estimation using ahrs under conditions of magnetic distortion. Sensors 2014, 14, 20008–20024. [Google Scholar] [CrossRef] [PubMed]
- Schiefer, C.; Ellegast, R.P.; Hermanns, I.; Kraus, T.; Ochsmann, E.; Larue, C.; Plamondon, A. Optimization of inertial sensor-based motion capturing for magnetically distorted field applications. J. Biomech. Eng. 2014, 136, 121008. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Giovanardi, A.; Rocchi, L.; Davalli, A. A simple test to assess the static and dynamic accuracy of an inertial sensors system for human movement analysis. In Proceedings of the 28th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS ‘06), New York, NY, USA, 30 August–3 September 2006; pp. 5912–5915.
- Boonstra, M.C.; van der Slikke, R.M.; Keijsers, N.L.; van Lummel, R.C.; de Waal Malefijt, M.C.; Verdonschot, N. The accuracy of measuring the kinematics of rising from a chair with accelerometers and gyroscopes. J. Biomech. 2006, 39, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Ayachi, F.; Nguyen, H.; Goubault, E.; Boissy, P.; Duval, C. The use of empirical mode decomposition-based algorithm and inertial measurement units to auto-detect daily living activities of healthy adults. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, PP, 1. [Google Scholar] [CrossRef] [PubMed]
- Negnevitsky, M. Artificial Intelligence: A Guide to Intelligent Systems; Addison-Wesley: New York, NY, USA, 2005. [Google Scholar]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Lebel, K.; Boissy, P.; Duval, C.; Jog, M.; Speechley, M.; Karelis, A.; Vincent, C.; Edwards, R. In Assessing the validity of attitude and heading reference systems for biomechanical evaluation of motions—A methodological proposal. In Proceedings of the International Conference on Biomedical Electronics and Devices, Angers, France, 3–6 March 2014; pp. 230–237.
- Brodie, M.A.; Psarakis, M.; Hoang, P. Gyroscopic corrections improve wearable sensor data prior to measuring dynamic sway in the gait of people with multiple sclerosis. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Ayachi, F.S.; Nguyen, H.P.; Lavigne-Pelletier, C.; Goubault, E.; Boissy, P.; Duval, C. Wavelet-based algorithm for auto-detection of daily living activities of older adults captured by multiple inertial measurement units (IMUs). Physiol. Meas. 2016, 37, 442. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.P.; Ayachi, F.; Lavigne–Pelletier, C.; Blamoutier, M.; Rahimi, F.; Boissy, P.; Jog, M.; Duval, C. Auto detection and segmentation of physical activities during a timed-up-and-go (tug) task in healthy older adults using multiple inertial sensors. J. Neuroeng. Rehabil. 2015, 12, 36. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features Category | Aspect | Input Feature |
|---|---|---|
| AHRS accuracy | Environment |
|
| Motion performed |
| |
| Direction of motion |
| |
| Joint estimation accuracy | Environment |
|
|
| Original Data | Cleaned-up Data (ANN) | |||||
|---|---|---|---|---|---|---|
| Ntotal | Ngood | RMSDtotal | Naccepted | RMSDaccepted | ||
| Sit | Trunk | 180 | 177 | 0.9° (1.4°) | 177 | 0.7° (0.6°) |
| Hip | 180 | 177 | 0.7° (2.5°) | 178 | 0.5° (0.6°) | |
| Knee | 180 | 177 | 0.9° (2.8°) | 178 | 0.7° (1.0°) | |
| Ankle | 177 | 159 | 3.4° (10.1°) | 157 | 1.2° (2.2°) | |
| STS | Trunk | 175 | 120 | 4.2° (2.5°) | 113 | 3.6° (2.0°) |
| Hip | 175 | 165 | 2.1° (1.9°) | 177 | 2.1° (1.9°) | |
| Knee | 180 | 167 | 2.4° (2.3°) | 169 | 2.2° (1.7°) | |
| Ankle | 176 | 122 | 5.8° (9.4°) | 124 | 3.8° (3.7°) | |
| Walk | Trunk | 349 | 266 | 4.3° (4.5°) | 325 | 4.2° (4.0°) |
| Hip | 349 | 301 | 3.5° (4.0°) | 331 | 3.3° (3.3°) | |
| Knee | 359 | 260 | 4.3° (2.5°) | 275 | 4.2° (2.4°) | |
| Ankle | 351 | 51 | 14.3° (12.4°) | 7 | 5.1° (2.4°) | |
| Turn | Trunk | 166 | 117 | 4.1° (2.5°) | 141 | 4.0° (2.3°) |
| Hip | 166 | 133 | 3.8° (1.8°) | 161 | 3.8° (1.9°) | |
| Knee | 180 | 108 | 4.7° (2.6°) | 81 | 4.5° (2.3°) | |
| Ankle | 176 | 18 | 15.2° (10.9°) | 2 | 6.4° (0.2°) | |
| Turn-to-sit | Trunk | 168 | 118 | 4.4° (3.5°) | 157 | 4.5° (3.6°) |
| Hip | 168 | 126 | 3.9° (2.0°) | 161 | 3.8° (1.9°) | |
| Knee | 165 | 108 | 5.6° (5.7°) | 62 | 4.1° (2.5°) | |
| Ankle | 159 | 53 | 12.5° (15.2°) | 26 | 6.0° (4.5°) | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lebel, K.; Boissy, P.; Nguyen, H.; Duval, C. Autonomous Quality Control of Joint Orientation Measured with Inertial Sensors. Sensors 2016, 16, 1037. https://doi.org/10.3390/s16071037
Lebel K, Boissy P, Nguyen H, Duval C. Autonomous Quality Control of Joint Orientation Measured with Inertial Sensors. Sensors. 2016; 16(7):1037. https://doi.org/10.3390/s16071037
Chicago/Turabian StyleLebel, Karina, Patrick Boissy, Hung Nguyen, and Christian Duval. 2016. "Autonomous Quality Control of Joint Orientation Measured with Inertial Sensors" Sensors 16, no. 7: 1037. https://doi.org/10.3390/s16071037