
Dances with Social Robots: A Pilot Study at Long-Term Care

Autonomous Systems and Biomechatronics Laboratory (ASBLab), Department of Mechanical and Industrial Engineering, University of Toronto, 5 King’s College Rd, Toronto, ON M5S 3G8, Canada
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Robotics 2022, 11(5), 96; https://doi.org/10.3390/robotics11050096
Submission received: 27 July 2022
/
Revised: 2 September 2022
/
Accepted: 8 September 2022
/
Published: 13 September 2022
(This article belongs to the Special Issue Social Robots for the Human Well-Being)
Abstract
:Dance therapy can have significant physical, emotional and cognitive benefits for older adults. In particular, social robots can be developed to autonomously facilitate dance sessions to engage these individuals with the aim of improving quality of life. To successfully integrate and promote long-term use of social robots into long-term care homes for such recreational activities, it is important to explore both residents’ and staff’s perceptions of such robots. In this paper, we present the first pilot human–robot interaction study that investigates the overall experiences and attitudes of both residents and staff in a long-term care home for robot-facilitated dance sessions. In general, the questionnaire results from our study showed that both staff and residents had positive attitudes towards the robot-facilitated dance activity. Encouraging trends showed residents had higher ratings for statements on perceived ease of use, safety, and enjoyment than the staff. However, the staff had a statistically significantly higher rating for willingness to use the robots for dance facilitation. Some key statistical differences were also determined with respect to: (1) gender within the resident group (men had higher ratings for the robots being useful in helping facilitate recreational activities), as well as between staff and residents (resident men had higher perceived safety), and (2) prior robot experience (residents with limited prior experience had higher ratings on perceived ease of use and perceived enjoyment than staff with the same level of experience). The robot-facilitated dance activity was positively received by both older adults and staff as an activity of daily living that can enhance wellbeing while also being safe, easy to use and enjoyable.
1. Introduction
Dance therapy has been shown to be beneficial for a person’s cognitive, emotional, physical and social abilities [1]. In particular, for older adults, dance can improve cognitive flexibility [2] and physical skills [3], especially in muscular strength, endurance and balance [4]. Furthermore, dance therapy has shown to improve motion control skills in the treatment of Parkinson’s disease [5,6] and has had positive effects on depression, loneliness and the moods of older adults living with mild dementia [7]. Both older adults and caregivers believe dancing is an important physical activity that is both enjoyable and keeps older adults active [8,9]. Furthermore, dancing has been found as a desirable function for robot companions by middle–older-aged adults [8].
To date, a handful of robots have been used to facilitate dance as either: (1) robot dance partners [10,11,12] and/or (2) robot dance instructors [12,13,14,15,16]. A robot dance partner engages physically in collaborative dance with a user to form a dance pair (e.g., ballroom dancing) [10] or can provide physical assistance to a user when they have difficulties in completing the dance motion (e.g., with older adults) [11]. On the other hand, a robot dance instructor can facilitate and provide guidance in a noncontact manner on a user’s dance performance in order for the user to learn specific dance steps and improve their overall dance quality [13,14]. Robot dance-based human–robot interaction (HRI) studies have shown that users perceive these robot as engaging [12,14,16], useful [11] and cognitively stimulating [17].
The majority of existing HRI research in long-term care has mainly focused on older adults perspectives as highlighted in the following survey papers [18,19]. However, it is also important to consider acceptance and attitudes of care staff before implementing any new technology to aid in improving the quality of work [20] and ensuring the successful integration of such robots in care settings [21]. Such acceptance by healthcare staff is critical to the actual prolonged use of new technology in care settings [22]. To date, only a few studies have investigated both care staffs’ attitudes and acceptance of robots in long-term care settings [23,24,25,26,27,28,29,30]. There has not yet been a study that specifically investigates and compares both residents’ and staff’s perceptions for the integration of dance therapy robots in long-term care.
Herein, we introduce an HRI study to investigate and compare the perceptions of both residents and staff in a long-term care home for dance activity sessions facilitated by social robots. In particular, we explore and compare both staff and residents overall experience with autonomous dance robots and examine whether demographic factors influence their overall acceptance of such technology.
Our aim is to provide insight into the potential integration of robots for the dance activity and explore preliminary impacts on both staff and residents. In this paper, we present the first HRI study to provide a quantitative evaluation on the deployment of social robots for the autonomous facilitation of dance sessions with older adults in long-term care. Our contributions are twofold: (1) we are the first to examine and compare the perceptions of both residents and care staff for the stimulating activity of dance facilitated by social robots, and (2) our study uniquely explores the impacts of demographic factors on acceptance of social robots by these two groups for such activities in long-term care.
The remaining sections of the paper are organized as follows. In Section 2, we summarize the existing literature on the use of dance robots for older adults, as well as general HRI studies that have considered both older adults and staff experiences in care settings. In Section 3, we present our HRI study design and implementation procedure, and in Section 4, we discuss the overall statistical results we obtained for both the staff and residents while also considering the demographic factors. In Section 5, we discuss the outcomes, impacts and design considerations of our HRI study and compare our results to existing studies. Lastly, we provide concluding remarks and future work in Section 6. Table 1 provides a summary of all the abbreviations and variables used in this paper.
2. Related Works
In this section, we present and discuss the existing literature on: (1) the deployment of dance robots for older adults and (2) general HRI studies with both older adults and staff in care settings.
2.1. Robot Dance for Older Adults
A handful of studies have been conducted on robot dance with older adults using a robot as a partner [11], performer (for entertainment purposes) [31] or instructor [15,17,32,33,34,35]. For example, in [11], a human-sized robot consisting of a wheeled base and two anthropomorphic robotic arms was used for partner dancing. The robot was led by an older adult partner in simple forward/backward walking dance steps. A study with healthy older adults showed that they considered the robot dance partner useful, easy to use and enjoyed dancing with it. In [31], a small 3D-printed expressive robot that could dance was introduced for potential homecare to provide entertainment to older adults. The focus was on the design of the robot rather than on evaluation with the intended users.
In [15,35], the Nao robot was used as a dance instructor for people living at residential care homes. Participants sat in a circle with Nao and were asked to follow the robot’s dance movements to music. The participants danced or sang along with Nao and found the robot interesting. In [32], a toy-like social robot named Matilda was used to perform multimodal interactions with older adults. The robot was used in multiple long-term care homes where older adults interacted with the robot over a period of three years in different activities, including gaming playing, dance, storytelling and reminding. The results from the study found the participants were engaged and accepted the robot for these tasks. In [33], the toy-like social robot Betty was used to interact with older adults living with dementia at home. The interactions with Betty included dance. The results showed that participants were engaged with the social robot and found it useful.
With respect to measuring health outcomes, in [17], another small robot was used for cognitive dance therapy with older adults. The dance therapy sessions consisted of singing, dancing and memorizing tasks. The cognitive evaluation test showed a significant improvement in participants’ cognitive ability. In [34], a mobile robot named SI-ROBOTICS equipped with a microphone, tablet, camera and Lidar was developed for conducting dance therapy sessions with different types of dances to help those living with Parkinson’s disease. The study is currently underway and will evaluate their gait and functional status, along with cardiorespiratory performance.
2.2. HRI Studies with Older Adults and Caregivers
Table 2 provides a summary of the only handful of HRI studies that have considered both older adults’ and care staffs’ acceptance of social robots for a range of daily activities in different care settings [25,27,28,29,30]. In [26], a survey consisting of only interviews and questionnaires on attitudes towards possible healthcare robots in a retirement village was presented. The participants included residents, staff and residents’ relatives. The statistical analysis of the questionnaires showed a more positive attitude towards robots by the residents than both the staff and relatives.
In both [25,27], robot interaction studies were conducted. For example, in [25], a 10-week study with the care robot Zora was performed in several long-term care homes. The robot’s interactive activities included physical exercises, playing music, storytelling, dancing, interactive memory and playing guessing games with older residents. Interviews were conducted with both staff and residents. The staff expressed concerns regarding training on how to properly use the robot and the added workload related to operating the robot, whereas residents considered the robot funny, entertaining and interesting. In [27], the teleoperated humanoid robot Robovie2 provided greetings and chatted with older adults in a care home. Interviews were conducted with both staff and older adults. The staff had a general positive attitude towards the robot, and older adults expressed a willingness to interact with Robovie2.
Some studies also directly compared the differences in robot acceptance between staff and older adults for tasks such as providing greetings [28], pick-up and reminders [29] and teleconferencing [30]. In [28], the mobile robot SCITOS was introduced at a care hospital. The robot was able to autonomously navigate and patrol a predefined area and greet passersby. Both interviews and questionaries were used for evaluating acceptance of the robot by staff and older adults with dementia and multimorbidity. The results showed a moderate acceptance of the robot from the staff and older adults. The staff also expressed concerns about the robot occupying their workspace and replacing them. In [29], in a home-like testing environment, the Care-O-bot robot was used to aid older adults with package pick-up and water drinking reminders. Care providers of the older adults were invited to observe this testing. The results from questionnaires and interviews found that the robot was more accepted by the older adults than their care providers. Caregivers expressed concerns about the robot not being able to operate independently without supervision and being used only as an additional helper. In [30], both staff and older adults in a long-term care home tested several functions of a telepresence robot, including navigation, vital signs measurement, video conferencing and reminders. The results from a robot acceptance questionnaire found that the staff and older adults perceived the usefulness of certain functions differently based on their own interest. Namely, the staff found vital signs measurements and reminders more useful than the older adults did, whereas the older adults found video conferencing more useful than the staff did.
In general, older adults have found robot dance useful, engaging and entertaining, and some studies have reported preliminary health outcomes. To date, HRI studies directly comparing care staffs’ and older adults’ experiences and the acceptance of social robots are still limited. No study has investigated the acceptance of robot-facilitated dance among both older adult residents and staff or considered the demographic factors that may influence this. However, dance therapy has shown significant physical and cognitive benefits for this older cohort. Furthermore, these robots can help reduce the staff workload in long-term care homes. Therefore, herein, we present an HRI study that allows both care staff and residents to directly interact with social robots during robot-facilitated dance sessions in order to investigate and compare their experiences, as well as other factors (including demographic) that may affect the uptake of this technology.
3. Robot Dance Pilot Study Methodology
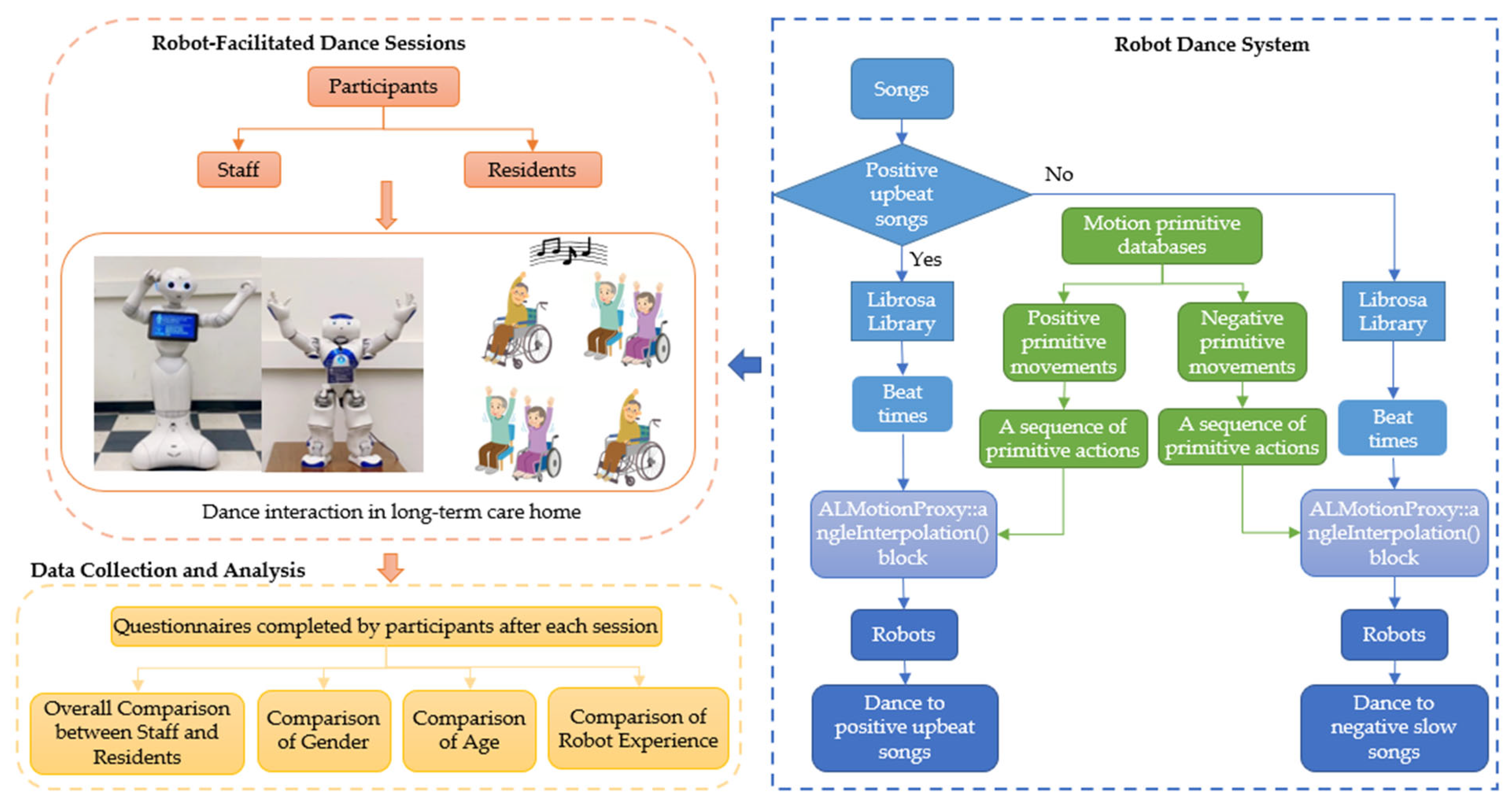
An HRI study was conducted in a recreational room of a Toronto area long-term care home for the duration of a day. The participants included both residents and staff at the home. Two robots (human-sized and toy-sized) facilitated group-based dance sessions for approximately 15–20 min a session throughout the day. Figure 1 presents the procedural flowchart of our HRI study. We investigate the following research questions: (1) Is there any difference between the staff and residents’ experiences with robot-facilitated dance? and (2) Do the demographic factors influence experience and perceptions of these two groups? The participants’ overall experiences and perceptions of the robots and the facilitated dance sessions were obtained through questionnaires.
3.1. Robot Dance Design
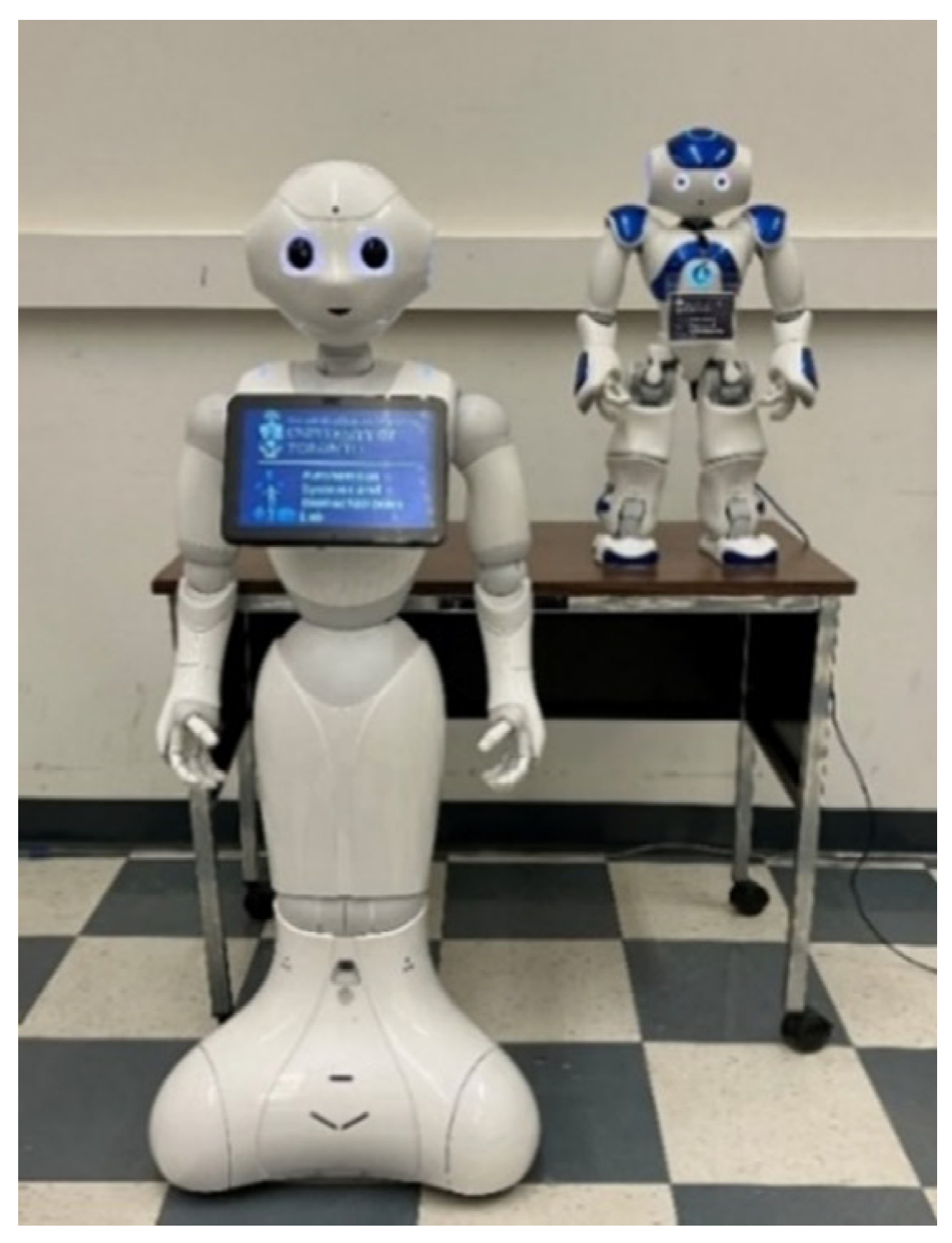
Two noncontact socially assistive robots, which we named Salt and Luke (in order to personalize the robots for the dance interactions), were introduced in this study (Figure 2). Salt is a human-sized Pepper robot, and Luke is a toy-sized Nao humanoid robot; both robots are from Softbank. The main features of the two robots used in this study are provided in Table 3.
In this study, we developed two robot motion primitive databases for the dance movements of the two robots. This allowed for the design of motion primitives that can be modularly combined in different ways to produce corresponding dance routines to generalize to multiple songs. One database includes 81 positive primitive movements, and the other includes 41 negative primitive movements. Each motion primitive was composed of a combination of arm, head and waist movements that consist of either positive or negative body expressions. The databases were used by each robot to autonomously choose their corresponding sequence of dance moves to match the type of music played by the robot, i.e., upbeat and fast motions or slow motions. To ensure all the dance motion are easy to be recognized by the users, the design of the robot’s motion primitives is adapted from [38,39], which both identified distinct correlations between human or robot body movements and positive and negative emotions through the chi-square goodness of fit and regression tests, respectively. In [38], adults (including older adults up to 78 years of age) were able to recognize the positive emotions through a series of expansive movements with stretching trunk and high movement activity/dynamics, whereas the negative emotions were identified with inexpansive movements with bowing trunk and low movement activity/dynamics. The motion primitives in our robot system are composed of a series of these specific movement types. Examples of these motion primitives are presented in Table 4. We use the Librosa Library [40] to detect beats in the audio of a song. Namely, input audio is converted into an onset strength envelope that represents hypothesized beat times [41]. This onset strength envelope is used to estimate the tempo period strength. An overall global tempo for a song is estimated to be the tempo period strength when it is the largest. Using the global tempo, a transition cost function is constructed, and dynamic programming is used to determine the best-scoring set of beat times that reflect this tempo [41]. The set of beat times in a song, D, is used to set the time duration when the robot displays each dance movement. We manually categorized several popular songs, chosen by our collaborative long-term care home, into one of two categories based on the emotional expression of the songs by their tempos: (1) positive upbeat songs and (2) negative slow songs. Slow tempos (60–76 beats per minute) are associated with negative emotions, whereas music played with fast tempos are associated with positive emotions (>120 beats per minute) [42]. One robot motion primitive database corresponds to each music category and is autonomously selected by a robot to generate the sequence of primitive actions A = {a1, …, ai, …}. An entire dance is generated by executing a sequence of ai from A along the time trajectory T = D. For this HRI study, we used the following songs: The Twist by Chubby Checker, Yesterday and A Hard Day’s Night by the Beatles and Stayin Alive by the Bee Gees.
3.2. Participants
A total of eighty-one participants volunteered for our study. Participants were recruited through poster advertisements in the home (i.e., posters were distributed on different floors of the home). Participants were divided into 2 separate groups: residents and staff. During each interaction session, all the participants were from the same group. Ethics approval was obtained from the University of Toronto Ethics Committee.
3.3. Procedure
Participants were divided into 10 sessions (5 resident and 5 staff sessions) with approximately 8 people in each session so that everyone had a clear line-of-sight of the robots. We used a counterbalanced approach for the robots, where either robot was randomly chosen to dance first in the sessions. In each session, the robots danced to all four songs and had the same dance movements. During each interaction, the noncontact robots were located at the front of the room, approximately 2 m from the participants. They would greet and invite the participants to dance along with them. Once the dance session was completed, the participants were asked to voluntarily complete a questionnaire.
3.4. Measures
To evaluate the perception and acceptance of the robots for the dance activity from both staff and residents, we designed a five-point Likert-scale short questionnaires for the staff and resident groups (Table 5). The questionnaires included statements on perceived usefulness (S1 and S2), perceived ease of use (S3), emotional adaption (S4), positive attitude (S5), reduced workload (S6), perceived safety (S7), perceived enjoyment (S8) and intent to use (S9). A number of these statements were adapted from the technology acceptance model (TAM) [43], which has been successfully used in robot studies with older adults [11,44]. We also included statements on perceived enjoyment [45] and perceived safety [46]. As job relevance has been found to significantly influence user acceptance [47], we included a statement on workload for the staff questionnaire. We also included a statement on robot functionality to evaluate its potential to enhance overall experience (S4). In the questionnaire design, a common concern is that the response burden of completing questionnaires may be particularly high for older adults [48]. Hence, we limited the questionnaire length to 9 questions to alleviate the response burden and increase the response rate of this user group [49,50]. Demographic information was also obtained from each group (gender, age and prior robot experience).
4. Results
The results were analyzed to examine and compare the staff and resident groups’ perceptions regarding the robot-facilitated dance sessions and to observe the statistical relationships with the demographic factors. We conducted nonparametric Mann–Whitney U (MWU) tests [51] to determine if statistically significant differences exist between the responses of the two independent groups: staff and residents. To investigate the influence of demographic factors, we conducted nonparametric tests to determine significant differences using: (1) the Kruskal–Wallis (KW) test [52] for the multiple age groups within the staff and residents groups and (2) MWU test [51] for gender, age and prior robot experience between the staff and residents groups and gender and prior robot experience within the staff and residents groups.
4.1. Staff and Resident Comparison
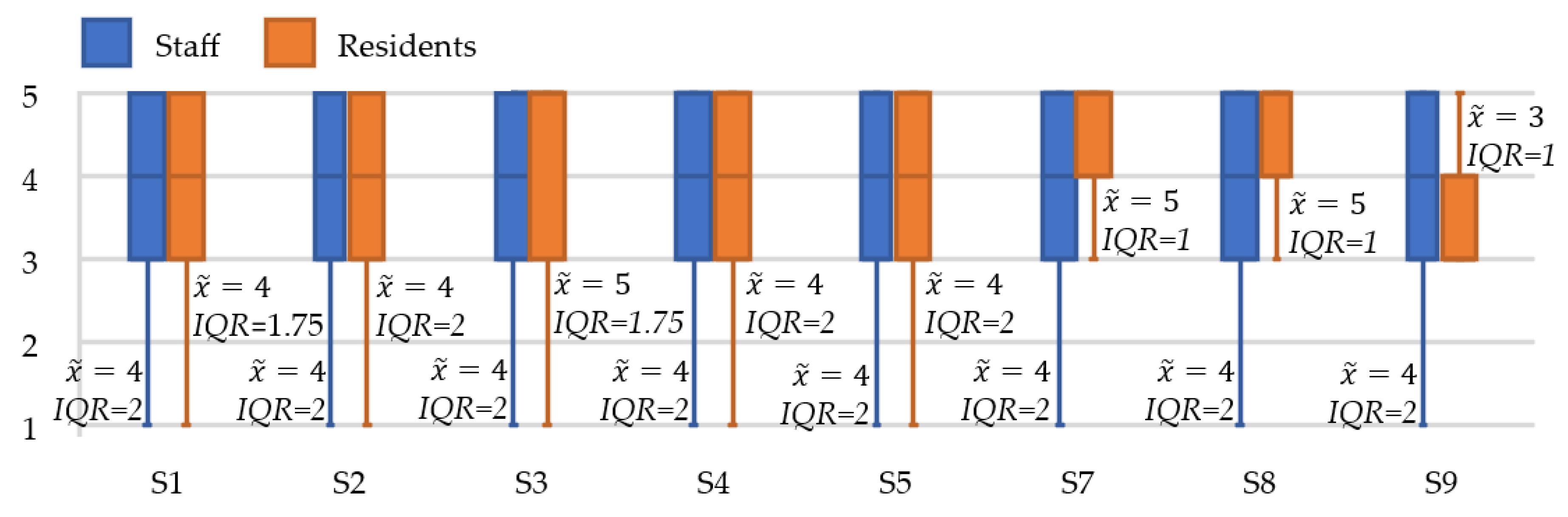
The staff participant group included fifty-four people, and the resident participant group consisted of twenty-seven people. Table 5 presents the overall descriptive statistics for both the staff and resident questionnaires, and Figure 3 shows the corresponding box and whisker plots for these groups with respect to the statements in the questionnaires. Both staff and residents positively rated the majority of statements in the questionnaires with a
= 4 or higher. Table 6 presents the statistical MWU tests results for the comparison of the staff and resident group responses. The staff ( = 4, IQR = 2) had a higher median score for their intent to use a robot for dance activities than the residents ( = 3, IQR = 1), with a statistically significant difference: MWU (U = 938.5, p = 0.019). Differences in median scores were determined between the residents and staff for statements on the perceived ease of use (S3), perceived safety (S7) and perceived enjoyment (S8). Namely, the robots were rated as easier to use ( = 5, IQR = 1.75) and safer ( = 5, IQR = 1) by the residents, and the residents thought a robot would make the dance activity more fun ( = 5, IQR = 1) than the staff group (all three statements: = 4, IQR = 2). However, these differences were not statistically significant: MWU (U = 559.5, p = 0.127), MWU (U = 585.5, p = 0.129), and (U = 602.5, p = 0.171), respectively.
4.2. Gender
Of the fifty-four participants in the staff group, 38 participants responded as women and 10 participants as men (6 did not specify gender), whereas, for the twenty-seven participants in the resident group, 12 responded as women, 12 as men and 3 did not specify.
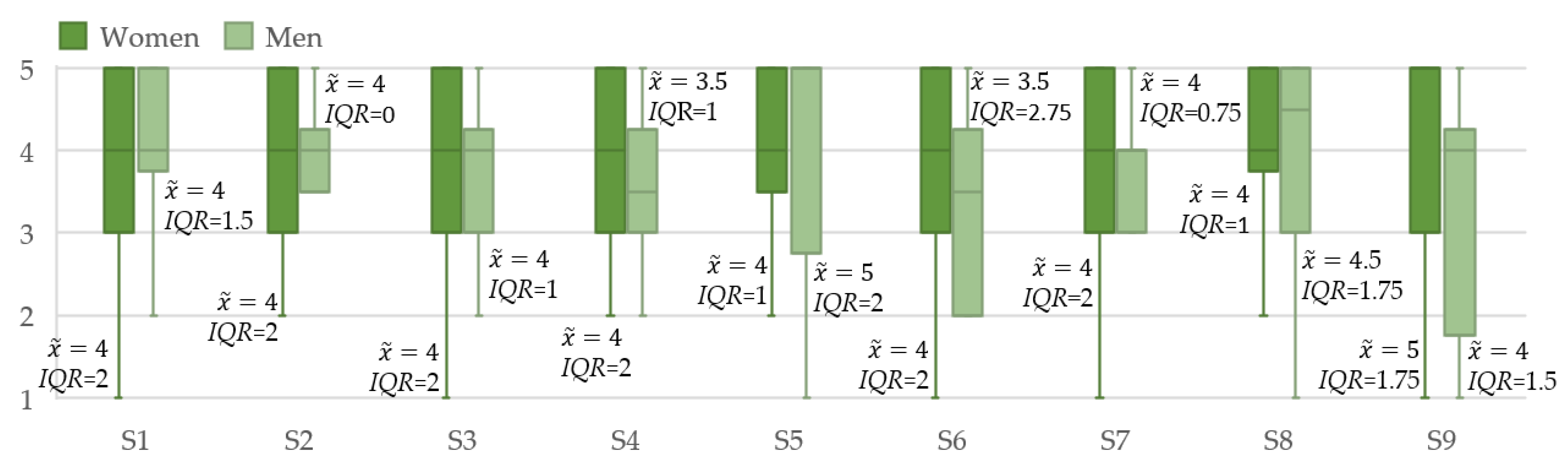
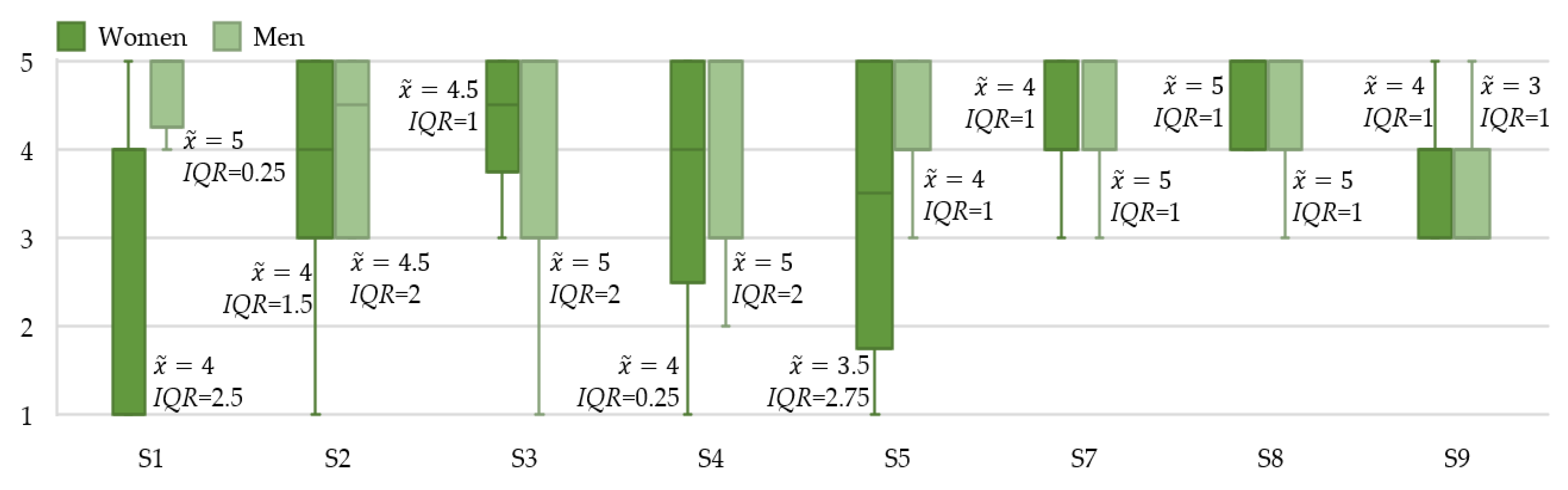
Figure 4 and Figure 5 present the box and whisker plots for gender for both the staff and residents, and Table 7 presents the nonparametric test results for the demographic factors within these two groups, including gender. For the staff group, women ( = 4) had the same median score as men ( = 4) for statements on perceived usefulness (S1: IQR = 2 and 1.5; S2: IQR = 2 and 0), perceived ease of use (S3: IQR = 2 and 1) and perceived safety (S7: IQR = 2 and 0.75); however, they ( = 5, IQR = 1.75) did rate the robots higher for intent to use (S9) than men ( = 4, IQR = 1.5) did. Staff who were men ( = 5, IQR = 2) had more positive attitudes towards the robots (S5) than the women staff ( = 4, IQR = 1) did based on their median scores. There were no statistically significant differences found between men and women for the staff group with respect to gender, as determined by the MWU tests (p > 0.05).
With respect to the resident group, men ( = 5, IQR = 0.25) thought that, in general, it was more useful to have a robot help with recreational activities than women ( = 4, IQR = 2.5), with a statistically significant difference: MWU (U = 18, p = 0.04). Residents who were men also rated S4 and S7 higher than residents who were women with respect to their median scores. Both women and men residents ( = 5, IQR = 1) rated the robot high on perceived enjoyment (S8). The only statement that women residents had a higher median score for than the men residents was intent to use a robot for dance activities (S9). However, MWU tests showed that there were no statistically significant differences for these other statements (S2–S5 and S7–S9) between women and men in the resident group (p > 0.05).
We then compared results between these two groups to determine any differences in the responses. Table 8 presents the MWU test results between the staff and resident groups for the three demographic factors. When comparing resident men and staff men, the resident group ( = 5, IQR = 1) thought that having a robot facilitate the dance activity was safer than the staff group ( = 4, IQR = 0.75), with a statistically significant difference: MWU (U = 96, p = 0.017). Men in the resident group had higher median scores than men in the staff group did for the robots with respect to perceived usefulness (S1: = 5, IQR = 0.25; S2: = 4.5, IQR = 2 versus S1: = 4, IQR = 1.5; S2: = 4, IQR = 0), perceived ease of use (S3: = 5, IQR = 2 versus = 4, IQR = 1) and emotional adaption (S4: = 5, IQR = 2 versus = 3.5, IQR = 1). However, men in the staff group rated the robots higher for positive attitude (S5: = 5, IQR = 2 versus = 4, IQR = 1) and intent to use (S9: = 4, IQR = 1.5 versus = 3, IQR = 1) than men in the resident group. The MWU tests showed that there were no statistically significant differences for these other statements between men in the resident and staff groups.
Women in the resident group had similar median scores as women in the staff group for the majority of the statements. The exception being that women in the resident group rated the robots higher for perceived enjoyment (S8) than women in the staff group ( = 5, IQR = 1 versus = 4, IQR = 1), whereas women in the staff group had higher intent to use (S9) than women in the resident group did based on the median scores ( = 5, IQR = 1.75 versus = 4, IQR = 1). However, there was no statistically significant differences found between women in the resident and staff groups, as determined by the MWU tests (p > 0.05).
4.3. Age
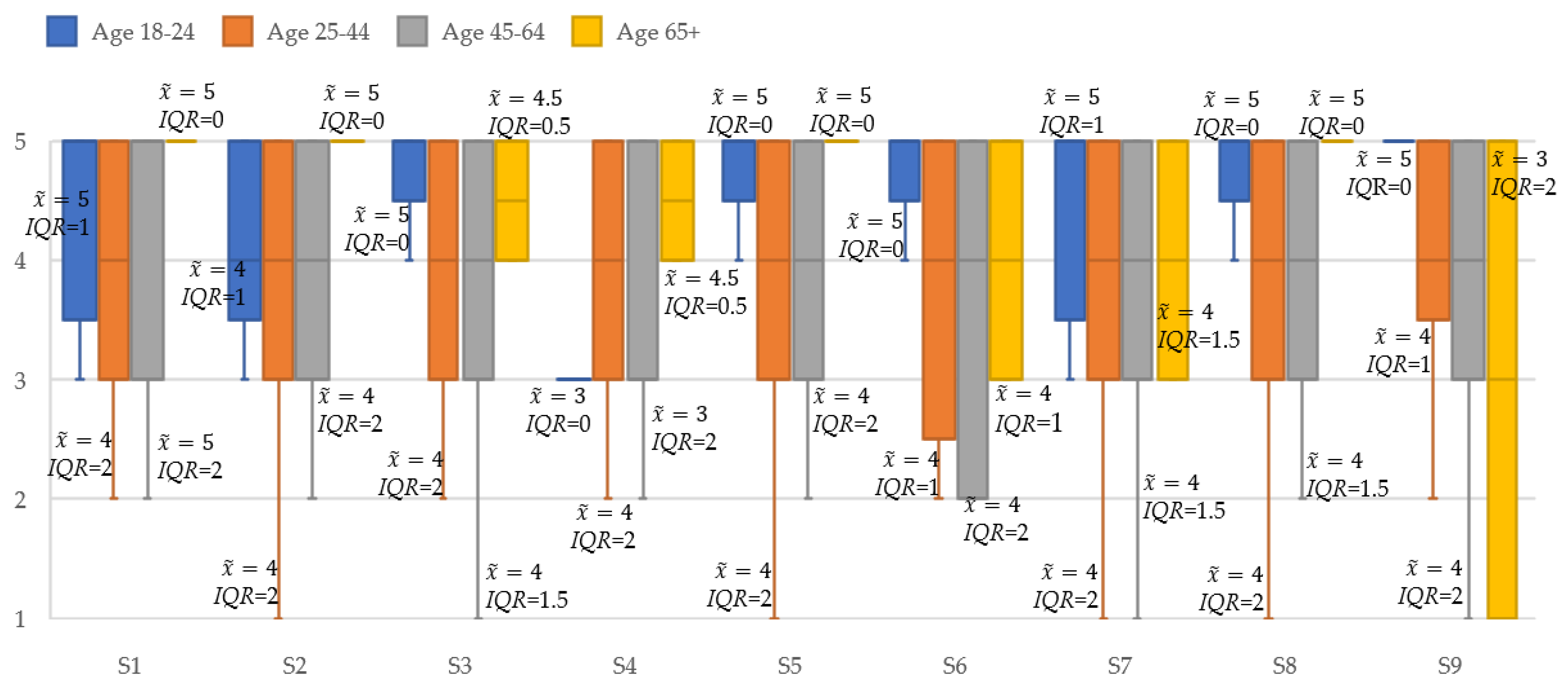
The ages of the staff ranged from 22 to 65 years (μ = 40.2, σ = 12.7), and the ages of the residents were between 57 and 93 (μ = 76.7, σ = 11). Staff ages were categorized into four common age groups for further analysis [53]: 18–24 (n = 17), 25–44 (n = 18), 45–64 (n = 11) and 65+ (n = 2). The ages of the residents were also distributed into two of these common age groups: 45–64 (n = 3), and 65+ (n = 14). Six staff and ten residents did not specify their ages. We noticed that the 65+ age group for staff and 45–64 age group for residents only consisted of two and three participants, respectively. However, this was expected, since the typical retirement age in Canada is 65 years old and over [54]. Figure 6 and Figure 7 present the box and whisker plots of the ages for staff and residents. The robots had higher median scores for the youngest staff age group for a reduced workload (S6: = 5, IQR = 0), perceived safety (S7: = 5, IQR = 1) and intent to use (S9: = 5, IQR = 0) than all other staff age groups. Both the youngest and oldest staff age groups had higher median scores for positive attitude (S5) and perceived enjoyment (S8) ( = 5, IQR = 0) than the middle staff age groups. However, the KW tests showed that there were no statistically significant differences in these statements for the staff group (p > 0.05).
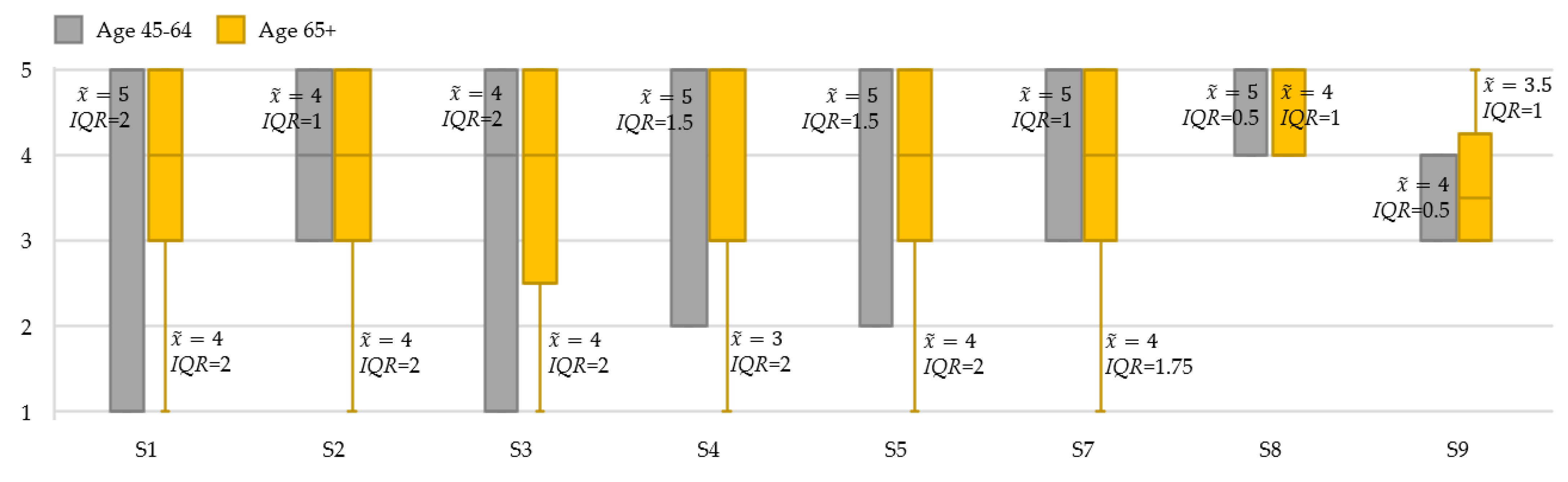
In the resident group, both age groups rated the majority of the statements as high ( ≥ 4). The only exceptions being for emotional adaption (S4) and intent to use (S9), where the 65+ group rated this statement more neutral ( = 3, IQR = 2 and = 3.5, IQR = 1), respectively. The younger (45–64 in age) resident age group ( = 5, IQR = 2) thought that it was more useful to have a robot help with recreational activities (S1) than the older (65+ in age) resident age group ( = 4, IQR = 2). The KW tests showed that there were no statistically significant differences in all the statements for the resident group (p > 0.05).
4.4. Prior Robot Experience
In the staff group, 28 people responded that they had no prior robot experience (no experience), 20 responded they had seen robots at museums, science centers or on TV (beginner experience), 2 people responded that they had seen robots used at their workplace delivering packages or medicine or interacting with residents (intermediate experience), no one responded that they had hands-on experience using a robot in a healthcare setting (advanced experience) and 4 people did not specify any prior robot experience. As the sample size was small for anyone with intermediate or advanced experience, the staff were categorized into two experience groups: no experience (n = 28) or limited experience (i.e., beginner and intermediate) (n = 22). In the resident group, 13 participants had no prior robot experience (n = 13), 12 participants had limited robot experience (n = 12) and 2 participants did not specify prior robot experience. Namely, no residents had intermediate or advanced robot experience.
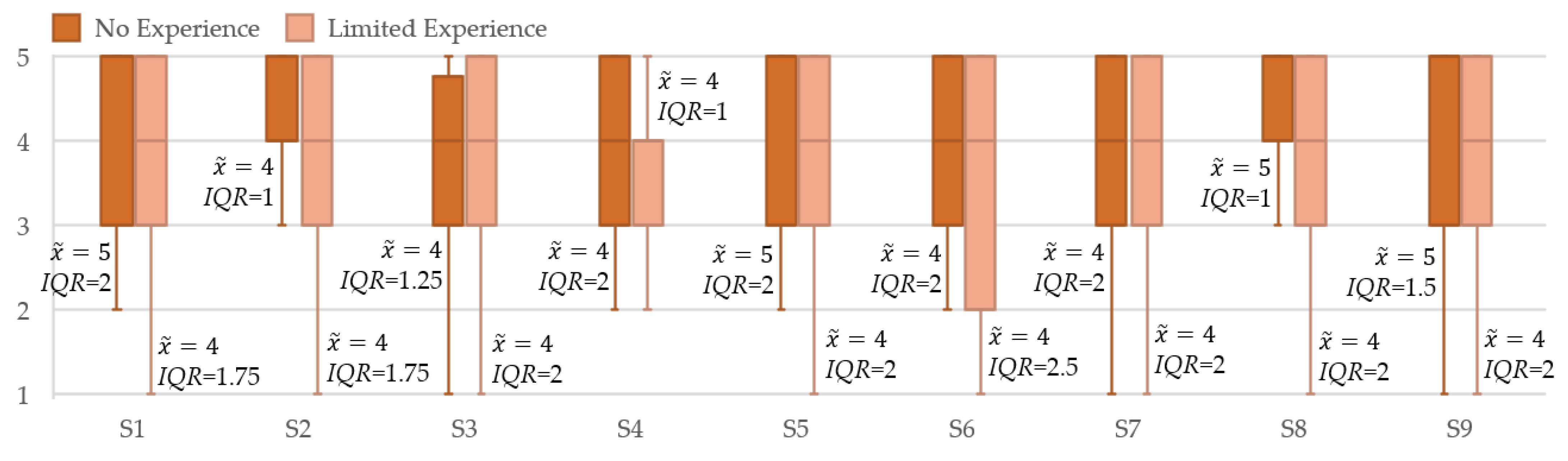
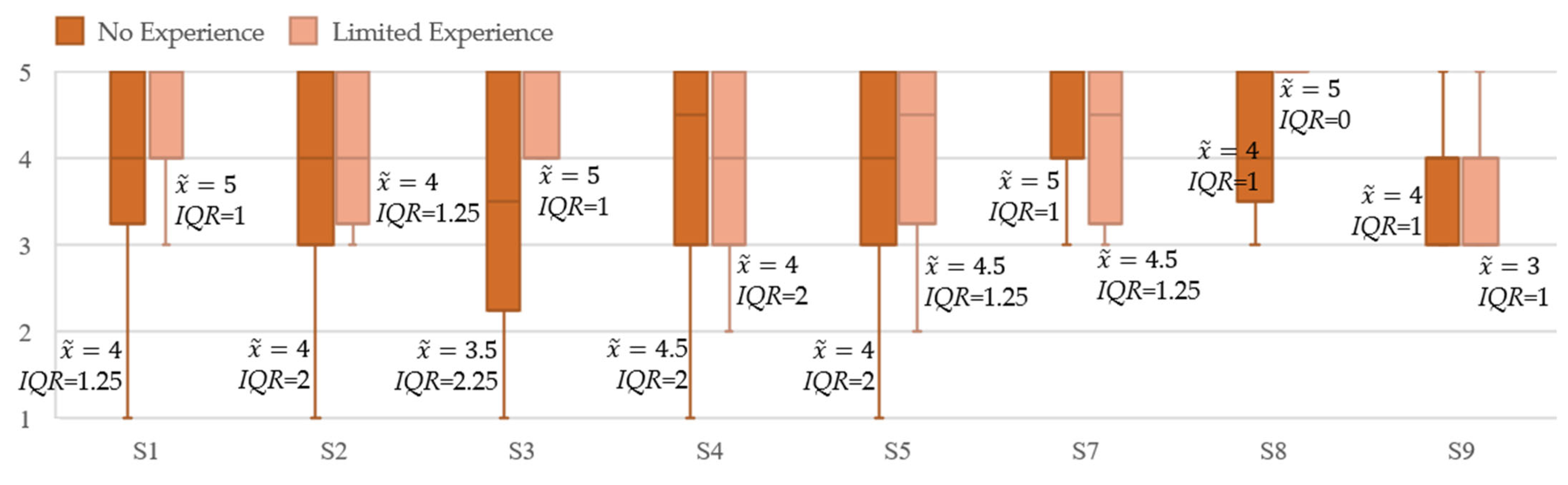
Figure 8 and Figure 9 show the box and whisker plots of robot experience for both the staff and residents. Staff who had no prior robot experience had higher median scores than the staff who had limited prior robot experience on perceived usefulness in having a robot help with recreational activities (S1: = 5, IQR = 2 versus = 4, IQR = 1.75), positive attitude (S5: = 5, IQR = 2 versus: = 4, IQR = 2), perceived enjoyment (S8: = 5, IQR = 1 versus = 4, IQR = 2) and intent to use (S9: = 5, IQR = 1.5 versus: = 4, IQR = 2). The MWU tests showed that there were no statistically significant differences between these experience levels within the staff group (p > 0.05).
Residents who had limited prior robot experiences had higher median scores than residents who had no prior robot experience for perceived usefulness in having a robot help with recreational activities (S1: = 5, IQR = 1 versus = 4, IQR = 1.25), perceived ease of use (S3: = 5, IQR = 1 versus = 3.5, IQR = 2.25) and perceived enjoyment (S8: = 5, IQR = 0 versus = 4, IQR = 1). However, residents who had no prior robot experience rated their intent to use the robots higher than residents who had limited prior robot experience (S9: = 4, IQR = 1 versus = 3, IQR = 1) based on the median scores. Both groups thought that such robot-facilitated dance activities were useful in enhancing wellbeing (S2: = 4, IQR = 2 and = 4, IQR = 1.25). The MWU tests showed that there were no statistically significant differences between these experience levels within the resident group (p > 0.05).
Comparing staff and resident responses, staff who had no robot experience had higher median scores than residents who had no robot experience for perceived usefulness in having a robot help with recreational activities (S1: = 5, IQR = 2 versus = 4, IQR = 1.25), positive attitude (S5: = 5, IQR = 2 versus = 4, IQR = 2), perceived enjoyment (S8: = 5, IQR = 1 versus = 4, IQR = 1) and intent to use (S9: = 5, IQR = 1.5 versus = 4, IQR = 1). Residents with no robot experience had higher median scores than the staff in this experience group for perceived safety (S7: = 5, IQR = 1 versus = 4, IQR = 2). However, there was no statistically significant difference found between the resident and staff groups with respect to no prior robot experience, as determined by the MWU tests (p > 0.05). Conversely, participants who had limited robot experience in the resident group ( = 5, IQR = 1) thought it would be easier for them to follow the robot during the dance sessions (S3) than participants who had limited robot experience in the staff group ( = 4, IQR = 2), with a statistically significant difference determined: MWU (U = 192, p = 0.031). Furthermore, participants who had limited robot experience in the resident group ( = 5, IQR = 0) also thought a robot would make the dance activity more fun (S8) than participants who had limited robot experience in the staff group ( = 4, IQR = 2) with a statistically significant difference: MWU (U = 202, p = 0.011).
5. Discussions
The aim of our HRI study is to explore the perceptions and attitudes of both staff and the residents in long-term care of autonomous robot-facilitated dance sessions, with the goal of providing long-term dance therapy for residents. During the interactions, we observed the older adult participants follow and mimic the robot dance movements while singing along with the music, showing the dance sessions were easy to follow and enjoyable. This is consistent with the results of the questionnaire, in which the majority of residents thought it was easy for them to follow the robots during the dance sessions. Our results suggest that, overall, both the staff and the resident groups had positive perceptions and attitudes towards the robots for the dance activity itself. Several participants also provided open feedback on the study with respect to their experience with the robots. In general, the residents provided specific positive comments about their direct interactions with the robots, such as “it was interesting and entertaining. I enjoyed the session”, “seeing the future today” and “the robots are doing a wonderful job!”. On the other hand, the staff provided comments directly related to the future deployment logistics of such robots in the home, such as they wanted to see “more funding for more robots in the home (than just the two robots used in this study)”.
5.1. Comparison of Staff and Residents
The residents had higher median scores for the robots than the staff for statements on perceived ease of use, perceived safety and perceived enjoyment, even though the results were not statistically significant. This trend is similar to other studies that have found older adults to have more positive attitudes towards social robots, such as in [25]. The staff, however, had a statistically significant higher rating for intentions to use the robots than the residents. We believe this difference between the staff and residents in terms of intentions to use may be due to the length of interactions in order to realize the potential benefits of the robot-facilitated activity. For example, in [55], older adults with mild cognitive impairments initially had lower intentions to use a companion robot; however, after several hours of interactions with the robot in one day, they started to appreciate its benefits and found the robot more acceptable.
5.2. Gender
In general, we found men and women to have similar attitudes, regardless of whether they were in the staff or resident group. This trend is consistent with other studies that have found that gender did not have a significant effect on perceptions of robots [56,57]. However, we noted two key differences in our study between (1) resident men and women and (2) men in the staff and resident groups.
Namely, we found that men in the resident group expressed statistically significant higher agreement with the robots being useful for helping with recreational activities than women in this same group. A previous study in [58] also found older adult men had a more positive perception of the usefulness of a healthcare robot than women. This difference across genders was not observed in the staff group in our study. It was noted in [59] that such a gender divide can exist within older adult populations but not necessarily younger populations.
Comparing gender between the resident and staff groups, a statistical significance was determined between the men for perceived safety, where the resident men believed robot-facilitated dance to be safer than the men in the staff group. In [60], it was reported that the staff regarded residents’ safety a primary concern and, hence, were more cautious with respect to their attitudes towards safety in general.
5.3. Age
A direct comparison for the responses between the same age groups (45–64 and 65+) for both the staff and residents did not find significant differences. However, this may be due to the small size of these specific age groups, namely, n = 2 for 65+ for staff and n = 3 for 45–64 for residents, which is expected in long-term care settings.
We did notice that the youngest staff age group had the highest median scores for the majority of the statements compared to any other staff age groups. This potentially highlights that younger staff may be more accepting of the use of robotics technology in long-term care settings. This finding is similar to other robotic studies that reported younger adults having a higher acceptance of robots for healthcare applications [61,62].
5.4. Prior Robot Experience
There was no statistically significant difference found between the no experience and limited experience groups of both the staff and residents. However, residents with limited robot experience thought it was easy to follow the robot during the dance sessions and thought that a robot would make the dance activity more fun than the staff with the same experience level. We believe that this may be due to staff having some logistical concerns with respect to having to setting up the robots on their own for resident use, as was also noted in [20,25]. Nonetheless, it is important to note that, in general, the staff agreed that the robots can free up staff time to do other tasks (Table 5: = 4, IQR = 2).
5.5. Robot Types
It is worth noting that, in this study, we did not explicitly ask participants specific questions about the two different robot types (i.e., the human-sized or toy-sized robots). Our aim in this initial pilot study was to introduce them to social robots and robot-facilitated dance. However, we did observe during the sessions that the residents danced with both robots, and in some cases, they also sang along. Therefore, we did not directly observe any differences in behaviors towards each robot. A prior study that compared these two robots with respect to their sizes by showing videos of the robots to older adults found that there was no difference in the users’ willingness to interact with either robot; however, the larger robot elicited higher positive impressions [63].
5.6. Comparisons to Previous Other HRI Studies
Our HRI study showed that older adults had positive perceptions and attitudes towards the robot-facilitated dance activity. This finding was aligned with several studies where robots were used as dance instructors with older adults. In these studies, participants also found the robots to be engaging [14,31,32] and useful [32] while also having a high acceptance of these robots [31].
Previous resident–caregiver comparison studies have found that older adults responded more positively to the potential deployment of robots than caregivers [26,29]. For example, in [26], based on the ratings of usefulness of a list of potential robot functions (e.g., detecting falls and calling for help, lifting heavy things and monitoring locations of older adults), older adults thought a potential healthcare robot would be more useful than the staff and relatives did, with statistical significance. However, in our HRI study, no statistically significant difference was found for perceived usefulness between residents and staff for dance activity. In [29], the Care-O-bot 3 robot helped older adults with package pick-ups and reminders for drinking water. Their caregivers and relatives observed these interactions. In the post-interaction interviews, older adults were more willing to accept the robot than their caregivers and relatives, as they found the robot easy to operate. From the caregivers’ and relatives’ perspective, safety concerns were expressed. In our study, staff men gave a statistically significant lower rating than the resident men for perceived safety.
5.7. Study Considerations
We conducted a short-term pilot study (approximately 15–20 min per session), where both the staff and residents had positive experiences in the use of robot-facilitated dance sessions in the long-term care home.
Our pilot study was conducted during the robot design cycle and is consistent with other similar preliminary HRI studies that also did not have bidirectional interactions or incorporate user actions, e.g., [12,35,64,65]. In our future long-term study, which will be informed from these results, our robots will autonomously recognize and classify the users’ affect in order to select the appropriate music and robot dance movements to promote user engagement and the positive affect during dancing. This feature was positively ranked for both residents and staff in our questionnaires.
We note that the novelty effect may have been present in our short-term study. For our long-term study, we will need to investigate and compare if the novelty effect contributed to our measured perception, experience and intent to use outcomes. Furthermore, we will need to explore the influence of long-term dance therapy and prolonged interactions on health (e.g., flexibility, range of motion and endurance) and affect (e.g., improving the affect over time) outcomes.
As mentioned above, we used two robots in this study; however, we did not ask participants to directly compare the two different embodiment types (toy-sized versus human-sized); instead we only observed their interactions with these robots. In the future, we will need to explore and compare robot embodiments for dance therapy activity.
6. Conclusions
In this paper, we presented the first HRI pilot study on both residents and staff perceptions of autonomous robot dance sessions in a long-term care home. Both groups had overall positive experiences with the robots, motivating the use of social robots for dance therapy with older adults. The residents had trends of higher ratings on statements related to perceived ease of use, perceived safety and perceived enjoyment. However, the staff had higher intentions to use the robots in facilitating dance activities (statistical significance was found). Some demographic influences were determined within and between the two groups. Namely, statistical differences were found between men in the resident and staff groups with respect to perceived safety, as well as between men and women residents with respect to robots being useful in helping facilitate recreational activities. There were also differences noted in perceived ease of use and perceived enjoyment for residents who had limited prior robot experience versus staff members with limited prior experience.
Our results are very promising, as they highlight an important activity of daily living that social robots can provide assistance to promote their quality of life and wellbeing. Our study provides insight for other HRI researchers with respect to the consideration of dance activity and how demographic factors may influence both the staff and other adults’ acceptance and intentions to use robots for dance therapy or other similar activities of daily living. Our HRI pilot study also emphasizes the importance of feedback from potential users on the design and use of social robot emotional dance to ensure the needs and preferences of older adults are incorporated during the design stage prior to long-term deployment. By investigating care staff perceptions, we aim to encompass the opinions of an important large group of individuals who can support the integration of social robots in care homes. Namely, with the support of the staff, HRI researchers will be able to maximize the benefits of such technologies in long-term care homes. Our future work includes conducting longitudinal robot dance therapy sessions at our partner long-term care home to investigate both the health and interaction outcomes. We will also investigate robot embodiment types to determine if any preferences exist.
Author Contributions
Conceptualization, G.N., Y.L., N.L. and M.E.; Methodology, Y.L.; Software, Y.L.; validation, Y.L. and G.N.; Formal analysis, Y.L. and G.N.; Investigation, Y.L., M.E. and N.L.; Resources, G.N.; Data Curation, Y.L.; Writing—original draft preparation, Y.L., N.L. and G.N.; Writing—review and editing, Y.L., N.L., G.N. and M.E.; Visualization, G.N.; Supervision, G.N.; Project administration, G.N. and Funding acquisition, G.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded in part by AGE-WELL Inc., the Natural Sciences and Engineering Research Council of Canada (NSERC), New Frontiers in Research Fund (NFRF)—Innovative Approaches to Research in the Pandemic Context, and the Canada Research Chairs Program.
Data Availability Statement
The data are not publicly available due to ethical and privacy restrictions.
Acknowledgments
The authors would like to thank the staff at the long-term care home for their help in conducting this pilot study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses or interpretation of the data; in the writing of the manuscript or in the decision to publish the results.
References
- Strassel, J.K.; Cherkin, D.C.; Steuten, L.; Sherman, K.J.; Vrijhoef, H.J. A Systematic Review of the Evidence for the Effectiveness of Dance Therapy. Altern. Ther. Health Med. 2011, 17, 50–59. [Google Scholar] [PubMed]
- Coubard, O.A.; Duretz, S.; Lefebvre, V.; Lapalus, P.; Ferrufino, L. Practice of Contemporary Dance Improves Cognitive Flexibility in Aging. Front. Aging Neurosci. 2011, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Hwang, P.W.-N.; Braun, K.L. The Effectiveness of Dance Interventions to Improve Older Adults’ Health: A Systematic Literature Review. Altern. Ther. Health Med. 2015, 21, 64. [Google Scholar] [PubMed]
- Alpert, P.T. The Health Benefits of Dance. Home Health Care Manag. Pract. 2011, 23, 155–157. [Google Scholar] [CrossRef]
- Earhart, G.M. Dance as Therapy for Individuals with Parkinson Disease. Eur. J. Phys. Rehabil. Med. 2009, 45, 231. [Google Scholar]
- Hackney, M.E.; Earhart, G.M. Effects of Dance on Movement Control in Parkinson’s Disease: A Comparison of Argentine Tango and American Ballroom. J. Rehabil. Med. Off. J. UEMS Eur. Board Phys. Rehabil. Med. 2009, 41, 475. [Google Scholar] [CrossRef]
- Ho, R.T.; Fong, T.C.; Chan, W.C.; Kwan, J.S.; Chiu, P.K.; Yau, J.C.; Lam, L.C. Psychophysiological Effects of Dance Movement Therapy and Physical Exercise on Older Adults with Mild Dementia: A Randomized Controlled Trial. J. Gerontol. Ser. B 2020, 75, 560–570. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Hsieh, S.; Li, C.-W. Needs and Preferences of Middle-Aged and Older Adults in Taiwan for Companion Robots and Pets: Survey Study. J. Med. Internet Res. 2021, 23, e23471. [Google Scholar] [CrossRef]
- Sefcik, J.S.; Johnson, M.J.; Yim, M.; Lau, T.; Vivio, N.; Mucchiani, C.; Cacchione, P.Z. Stakeholders’ Perceptions Sought to Inform the Development of a Low-Cost Mobile Robot for Older Adults: A Qualitative Descriptive Study. Clin. Nurs. Res. 2018, 27, 61–80. [Google Scholar] [CrossRef]
- Kosuge, K.; Hayashi, T.; Hirata, Y.; Tobiyama, R. Dance partner robot-ms dancer. In Proceedings of the 2003 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2003) (Cat. No. 03CH37453), Las Vegas, NV, USA, 27–31 October 2003; IEEE: New York, NY, USA, 2003; Volume 4, pp. 3459–3464. [Google Scholar]
- Chen, T.L.; Bhattacharjee, T.; Beer, J.M.; Ting, L.H.; Hackney, M.E.; Rogers, W.A.; Kemp, C.C. Older Adults’ Acceptance of a Robot for Partner Dance-Based Exercise. PLoS ONE 2017, 12, e0182736. [Google Scholar] [CrossRef]
- Venture, G.; Indurkhya, B.; Izui, T. Dance with me! Child-robot interaction in the wild. In Proceedings of the International Conference on Social Robotics, Golden, CO, USA, 14–18 November 2020; Springer: Berlin/Heidelberg, Germany, 2017; pp. 375–382. [Google Scholar]
- Ros, R.; Baroni, I.; Demiris, Y. Adaptive Human–Robot Interaction in Sensorimotor Task Instruction: From Human to Robot Dance Tutors. Robot. Auton. Syst. 2014, 62, 707–720. [Google Scholar] [CrossRef] [Green Version]
- Lei, X.; Rau, P.-L.P. Effect of Robot Tutor’s Feedback Valence and Attributional Style on Learners. Int. J. Soc. Robot. 2021, 13, 1579–1597. [Google Scholar] [CrossRef]
- Pedell, S.; Constantin, K.; Muñoz, D.; Sterling, L. Designing meaningful, beneficial and positive human robot interactions with older adults for increased wellbeing during care activities. In Handbook of Artificial Intelligence in Healthcare; Springer: Berlin/Heidelberg, Germany, 2022; pp. 85–108. [Google Scholar]
- Javed, H.; Park, C.H. Promoting Social Engagement with a Multi-Role Dancing Robot for In-Home Autism Care. Front. Robot. AI 2022, 4, 161. [Google Scholar] [CrossRef]
- Sawami, K.; Kimura, M.; Kitamura, T.; Kawaguchi, M.; Furusumi, M.; Suishu, C.; Morisaki, N.; Hattori, S. Cognitive Ability and Psychological Effectiveness of Brain Training Dance Robot Therapy for Elderly People. OA J. Neuropsychiatry 2019, 1, 004. [Google Scholar] [CrossRef]
- Broadbent, E.; Stafford, R.; MacDonald, B. Acceptance of Healthcare Robots for the Older Population: Review and Future Directions. Int. J. Soc. Robot. 2009, 1, 319–330. [Google Scholar] [CrossRef]
- Papadopoulos, I.; Koulouglioti, C.; Lazzarino, R.; Ali, S. Enablers and Barriers to the Implementation of Socially Assistive Humanoid Robots in Health and Social Care: A Systematic Review. BMJ Open 2020, 10, e033096. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Redmalm, D.; Iversen, C. Caregivers’ Use of Robots and Their Effect on Work Environment—A Scoping Review. J. Technol. Hum. Serv. 2021, 40, 251–277. [Google Scholar] [CrossRef]
- Franke, A.; Nass, E.; Piereth, A.-K.; Zettl, A.; Heidl, C. Implementation of Assistive Technologies and Robotics in Long-Term Care Facilities: A Three-Stage Assessment Based on Acceptance, Ethics, and Emotions. Front. Psychol. 2021, 12, 694297. [Google Scholar] [CrossRef]
- Yu, P.; Li, H.; Gagnon, M.-P. Health IT Acceptance Factors in Long-Term Care Facilities: A Cross-Sectional Survey. Int. J. Med. Inform. 2009, 78, 219–229. [Google Scholar] [CrossRef]
- Dijkers, M.P.; deBear, P.C.; Erlandson, R.F.; Kristy, K.; Geer, D.M.; Nichols, A. Patient and Staff Acceptance of Robotic Technology in Occupational Therapy: A Pilot Study. JRRD 1991, 28, 33. [Google Scholar] [CrossRef]
- Tuisku, O.; Pekkarinen, S.; Hennala, L.; Melkas, H. “Robots Do Not Replace a Nurse with a Beating Heart”: The Publicity around a Robotic Innovation in Elderly Care. Inf. Technol. People 2018, 32, 47–67. [Google Scholar] [CrossRef]
- Melkas, H.; Hennala, L.; Pekkarinen, S.; Kyrki, V. Impacts of Robot Implementation on Care Personnel and Clients in Elderly-Care Institutions. Int. J. Med. Inform. 2020, 134, 104041. [Google Scholar] [CrossRef]
- Broadbent, E.; Tamagawa, R.; Patience, A.; Knock, B.; Kerse, N.; Day, K.; MacDonald, B.A. Attitudes towards Health-Care Robots in a Retirement Village. Australas. J. Ageing 2012, 31, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Sabelli, A.M.; Kanda, T.; Hagita, N. A conversational robot in an elderly care center: An ethnographic study. In Proceedings of the 2011 6th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Lausanne, Switzerland, 6–9 March 2011; IEEE: New York, NY, USA, 2011; pp. 37–44. [Google Scholar]
- Hebesberger, D.; Koertner, T.; Gisinger, C.; Pripfl, J. A Long-Term Autonomous Robot at a Care Hospital: A Mixed Methods Study on Social Acceptance and Experiences of Staff and Older Adults. Int. J. Soc. Robot. 2017, 9, 417–429. [Google Scholar] [CrossRef]
- Bedaf, S.; Marti, P.; Amirabdollahian, F.; de Witte, L. A Multi-Perspective Evaluation of a Service Robot for Seniors: The Voice of Different Stakeholders. Disabil. Rehabil. Assist. Technol. 2018, 13, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Koceski, S.; Koceska, N. Evaluation of an Assistive Telepresence Robot for Elderly Healthcare. J. Med. Syst. 2016, 40, 121. [Google Scholar] [CrossRef]
- Potnuru, A.; Jafarzadeh, M.; Tadesse, Y. 3D printed dancing humanoid robot “buddy” for homecare. In Proceedings of the 2016 IEEE International Conference on Automation Science and Engineering (CASE), Fort Worth, TX, USA, 21–25 August 2016; IEEE: New York, NY, USA, 2016; pp. 733–738. [Google Scholar]
- Khosla, R.; Nguyen, K.; Chu, M.-T. Human Robot Engagement and Acceptability in Residential Aged Care. Int. J. Hum.–Comput. Interact. 2017, 33, 510–522. [Google Scholar] [CrossRef]
- Khosla, R.; Chu, M.-T.; Khaksar, S.M.S.; Nguyen, K.; Nishida, T. Engagement and Experience of Older People with Socially Assistive Robots in Home Care. Assist. Technol. 2021, 33, 57–71. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Benadduci, M.; Bonfigli, A.R.; Riccardi, G.R.; Melone, G.; La Forgia, A.; Macchiarulo, N.; Rossetti, L.; Marzorati, M.; Rizzo, G. Dancing With Parkinson’s Disease: The SI-ROBOTICS Study Protocol. Front. Public Health 2021, 9, 780098. [Google Scholar] [CrossRef]
- Back, I.; Kallio, J. Robot-Guided Exercise Program for the Rehabilitation of Older Nursing Home Residents. Ann. Long-Term Care 2013, 21, 6. [Google Scholar]
- Pepper-Technical Overview—Aldebaran 2.0.6.8 Documentation. Available online: http://doc.aldebaran.com/2-0/family/juliette_technical/index_juliette.html (accessed on 25 August 2022).
- NAO-Technical Overview—Aldebaran 2.0.6.8 Documentation. Available online: http://doc.aldebaran.com/2-0/family/robots/index_robots.html (accessed on 25 August 2022).
- De Meijer, M. The Contribution of General Features of Body Movement to the Attribution of Emotions. J. Nonverbal Behav. 1989, 13, 247–268. [Google Scholar] [CrossRef]
- McColl, D.; Nejat, G. Recognizing Emotional Body Language Displayed by a Human-Like Social Robot. Int. J. Soc. Robot. 2014, 6, 261–280. [Google Scholar] [CrossRef]
- Librosa. Librosa 0.9.1 Documentation. Available online: https://librosa.org/doc/latest/index.html (accessed on 10 March 2022).
- Ellis, D.P.W. Beat Tracking by Dynamic Programming. J. New Music. Res. 2007, 36, 51–60. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, G.; Wei, D.; Li, Q.; Yuan, G.; Wu, S.; Wang, G.; Zhao, X. Effects of Musical Tempo on Musicians’ and Non-Musicians’ Emotional Experience When Listening to Music. Front. Psychol. 2018, 9, 2118. [Google Scholar] [CrossRef]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Smarr, C.-A.; Mitzner, T.L.; Beer, J.M.; Prakash, A.; Chen, T.L.; Kemp, C.C.; Rogers, W.A. Domestic Robots for Older Adults: Attitudes, Preferences, and Potential. Int. J. Soc. Robot. 2014, 6, 229–247. [Google Scholar] [CrossRef]
- Heerink, M.; Kröse, B.; Wielinga, B.; Evers, V. Enjoyment intention to use and actual use of a conversational robot by elderly people. In Proceedings of the the 3rd ACM/IEEE International Conference on Human Robot Interaction, Amsterdam, The Netherlands, 12–15 March 2008; pp. 113–120. [Google Scholar]
- Bartneck, C.; Kulić, D.; Croft, E.; Zoghbi, S. Measurement Instruments for the Anthropomorphism, Animacy, Likeability, Perceived Intelligence, and Perceived Safety of Robots. Int. J. Soc. Robot. 2009, 1, 71–81. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Stone, A.; Shiffman, S.; Atienza, A.; Nebeling, L. The Science of Real-Time Data Capture: Self-Reports in Health Research; Oxford University Press: Oxford, UK, 2007; ISBN 0-19-534631-9. [Google Scholar]
- Rolstad, S.; Adler, J.; Rydén, A. Response Burden and Questionnaire Length: Is Shorter Better? A Review and Meta-Analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef]
- Kato, T.; Miura, T. The Impact of Questionnaire Length on the Accuracy Rate of Online Surveys. J. Mark. Anal. 2021, 9, 83–98. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a Test of Whether One of Two Random Variables Is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Costa, S.; Hausenblas, H.A.; Oliva, P.; Cuzzocrea, F.; Larcan, R. The Role of Age, Gender, Mood States and Exercise Frequency on Exercise Dependence. J. Behav. Addict. 2013, 2, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Canada Pension Plan—Overview. Available online: https://www.canada.ca/en/services/benefits/publicpensions/cpp.html (accessed on 30 June 2022).
- Gross, H.-M.; Schroeter, C.; Mueller, S.; Volkhardt, M.; Einhorn, E.; Bley, A.; Langner, T.; Merten, M.; Huijnen, C.; van den Heuvel, H.; et al. Further progress towards a home robot companion for people with mild cognitive impairment. In Proceedings of the 2012 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Seoul, Korea, 14–17 October 2012; pp. 637–644. [Google Scholar]
- Krakovski, M.; Kumar, S.; Givati, S.; Bardea, M.; Zafrani, O.; Nimrod, G.; Bar-Haim, S.; Edan, Y. “Gymmy”: Designing and Testing a Robot for Physical and Cognitive Training of Older Adults. Appl. Sci. 2021, 11, 6431. [Google Scholar] [CrossRef]
- Bishop, L.; van Maris, A.; Dogramadzi, S.; Zook, N. Social Robots: The Influence of Human and Robot Characteristics on Acceptance. Paladyn J. Behav. Robot. 2019, 10, 346–358. [Google Scholar] [CrossRef]
- Kuo, I.H.; Rabindran, J.M.; Broadbent, E.; Lee, Y.I.; Kerse, N.; Stafford, R.M.; MacDonald, B.A. Age and gender factors in user acceptance of healthcare robots. In Proceedings of the RO-MAN 2009—The 18th IEEE International Symposium on Robot and Human Interactive Communication, Toyama, Japan, 27 September–2 October 2009; IEEE: New York, NY, USA, 2009; pp. 214–219. [Google Scholar]
- Heerink, M. Exploring the influence of age, gender, education and computer experience on robot acceptance by older adults. In Proceedings of the 2011 6th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Lausanne, Switzerland, 8–11 March 2011; IEEE: New York, NY, USA, 2011; pp. 147–148. [Google Scholar]
- Sims-Gould, J.; McKay, H.A.; Feldman, F.; Scott, V.; Robinovitch, S.N. Autonomy, Choice, Patient-Centered Care, and Hip Protectors: The Experience of Residents and Staff in Long-Term Care. J. Appl. Gerontol. 2014, 33, 690–709. [Google Scholar] [CrossRef]
- Vichitkraivin, P.; Naenna, T. Factors of Healthcare Robot Adoption by Medical Staff in Thai Government Hospitals. Health Technol. 2021, 11, 139–151. [Google Scholar] [CrossRef]
- Hall, A.K.; Backonja, U.; Painter, I.; Cakmak, M.; Sung, M.; Lau, T.; Thompson, H.J.; Demiris, G. Acceptance and Perceived Usefulness of Robots to Assist with Activities of Daily Living and Healthcare Tasks. Assist. Technol. 2017, 31, 133–140. [Google Scholar] [CrossRef]
- Esposito, A.; Cuciniello, M.; Amorese, T.; Esposito, A.M.; Troncone, A.; Maldonato, M.N.; Vogel, C.; Bourbakis, N.; Cordasco, G. Seniors’ appreciation of humanoid robots. In Neural Approaches to Dynamics of Signal Exchanges; Springer: Berlin/Heidelberg, Germany, 2020; pp. 331–345. [Google Scholar]
- Zhumabekova, K.; Ismailova, A.; Kushkinbayev, D.; Sandygulova, A. Exploring the effects of robot gender on child-robot interaction. In Proceedings of the Companion of the 2018 ACM/IEEE International Conference on Human-Robot Interaction, New York, NY, USA, 1 March 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 287–288. [Google Scholar]
- Schneider, S.; Kummert, F. Does the user’s evaluation of a socially assistive robot change based on presence and companionship type? In Proceedings of the Companion of the 2017 ACM/IEEE International Conference on Human-Robot Interaction, New York, NY, USA, 6 March 2017; Association for Computing Machinery: New York, NY, USA, 2017; pp. 277–278. [Google Scholar]
Figure 1.
Procedural flowchart for the HRI study.

Figure 2.
The robots Salt (left) and Luke (right).

Figure 3.
Box and whisker plots for both the staff and resident groups with respect to the statements (S1–S9) in the questionnaire.
Figure 3.
Box and whisker plots for both the staff and resident groups with respect to the statements (S1–S9) in the questionnaire.

Figure 4.
Box and whisker plots of gender with respect to the statements in the staff questionnaire.
Figure 4.
Box and whisker plots of gender with respect to the statements in the staff questionnaire.

Figure 5.
Box and whisker plots of gender with respect to the statements in the resident questionnaire.
Figure 5.
Box and whisker plots of gender with respect to the statements in the resident questionnaire.

Figure 6.
Box and whisker plots of the ages with respect to the statements in the staff questionnaire.
Figure 6.
Box and whisker plots of the ages with respect to the statements in the staff questionnaire.

Figure 7.
Box and whisker plots of the ages with respect to the statements in the resident questionnaire.
Figure 7.
Box and whisker plots of the ages with respect to the statements in the resident questionnaire.

Figure 8.
Box and whisker plots of the robot experience with respect to the statements in the staff questionnaire.
Figure 8.
Box and whisker plots of the robot experience with respect to the statements in the staff questionnaire.

Figure 9.
Box and whisker plots of the robot experience with respect to the statements in the resident questionnaire.
Figure 9.
Box and whisker plots of the robot experience with respect to the statements in the resident questionnaire.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Abbreviations and variables.
| Abbreviations | Variables | ||
|---|---|---|---|
| HRI | human–robot interaction | D | The set of beat times in a song |
| TAM | technology acceptance model | ai | the ith primitive action |
| MWU | Mann-Whitney U | A | the sequence of primitive actions |
| KW | Kruskal-Wallis | T | the time trajectory |
| Si | the ith statement in the questionnaire | median value | |
| IQR | interquartile range | ||
| Min | minual value | ||
| Max | maximul value | ||
| U | the corresponding MWU statistic | ||
| H | the corresponding KW statistic | ||
| p | significance level | ||
Table 2.
Summary of HRI studies and their findings with respect to older adults and caregivers.
| Reference | Robot Platform | Participants and Environment | Tasks and Functionalities | Methods | Findings |
|---|---|---|---|---|---|
| [25] | Zora robot | Care personnel and elderly clients in care homes and a geriatric rehabilitation hospital | Physical exercises, playing music, storytelling, dancing, interactive memory and playing guessing games | Focus group semi-structured interviews and interaction observations. | Staff expressed concerns regarding training on how to properly use the robot and the increased workload related to operating the robot. Residents found the robot funny, entertaining and interesting. |
| [27] | Robovie2 robot | Older adults and staff in an elderly care center | Greetings and engaging in conversations | Semi-structured interviews and interaction observations. | In general, staff had positive attitudes towards the robot. Older adults expressed willingness to interact with Robovie2. |
| [28] | SCITOS Robot | Older adults and employees in a care hospital | Autonomous navigation indoors, patrolling an area and greeting passersby. | Semi-structured interviews, interaction observations and questionnaires. | Staff had a moderate level acceptance of the robot, whereas older adults had higher acceptance. Staff also expressed concerns about the robot occupying their workspace and replacing them. |
| [29] | Care-O-bot 3 Robot | Older adults, informal cares and professional caregivers in a home-like testing environment | Package pick-ups and reminders for drinking water | Semi-structured interviews and questionaries | The robot was accepted more by the older adults than caregivers. Caregivers expressed concerns about the robot not being able to operate independently without supervision. |
| [30] | Assistive telepresence robot | Professional caregivers and elderly residents in a nursing home | Navigation indoors, vital sign measurements, video conferencing and reminders | Questionaries | Staff found vital sign measurements and reminders more useful than the older adults did. The older adults found video conferencing more useful than the staff did. |
Table 3.
Main features of the two robots used in this study.
| Robots | Main Features | ||||
|---|---|---|---|---|---|
| Height (m) | Mobile Base | Degrees-of-Freedom | Speakers | Microphones | |
| Salt (Pepper Robot by Softbank [36]) | 1.2 (human-size) | Omnidirectional wheeled base | 20 (Head: 2; Arm: 5 × 2; Hand: 1 × 2; Hip: 2; Knee: 1; Mobile base: 3) | ×2 on both sides of the head | ×4 on the head |
| Luke (Nao Robot by Softbank [37]) | 0.574 (toy-size) | Biped | 25 (Head: 2; Arm: 5 × 2; Hand: 1 × 2; Hip: 1; Leg: 5 × 2) | ×2 on both sides of the head | ×4 on the head |
Table 4.
Examples of robot positive and negative motion primitives.
| Examples | Positive Motion Primitives for Salt and Luke | ||
|---|---|---|---|
| 1 |  |  |  |
| 2 |  |  |  |
| 3 |  |  |  |
| 4 |  |  |  |
| Examples | Negative Motion Primitives for Salt and Luke | ||
| 1 |  |  |  |
| 2 |  |  |  |
| 3 |  |  |  |
| 4 |  |  |  |
Table 5.
Descriptive statistics for the staff and resident questionnaires.
| Statements | Median () | IQR | Min | Max | ||||
|---|---|---|---|---|---|---|---|---|
| Staff | Resident | Staff | Resident | Staff | Resident | Staff | Resident | |
| S1. It is useful to have a robot help with recreational activities. | 4 | 4 | 2 | 1.75 | 1 | 1 | 5 | 5 |
| S2. I think such robot-facilitated dance activities can enhance the wellbeing of residents. | 4 | 4 | 2 | 2 | 1 | 1 | 5 | 5 |
| S3. I think it will be easy for the residents to follow the robot during the dance sessions. | 4 | 5 | 2 | 1.75 | 1 | 1 | 5 | 5 |
| S4. It would be useful for the robot to automatically detect the residents’ emotions and pick appropriate music and dance movements to match their emotions. | 4 | 4 | 2 | 2 | 1 | 1 | 5 | 5 |
| S5. I think having a robot to facilitate the older adults to dance is a good idea. | 4 | 4 | 2 | 2 | 1 | 1 | 5 | 5 |
| S6. Using a robot would free up staff time to do other tasks. * | 4 | N/A | 2 | N/A | 1 | N/A | 5 | N/A |
| S7. I think having a robot facilitate the dance activity is safe. | 4 | 5 | 2 | 1 | 1 | 1 | 5 | 5 |
| S8. I think a robot will make the dancing activity fun. | 4 | 5 | 2 | 1 | 1 | 1 | 5 | 5 |
| S9. I would use a robot to conduct dance activities. | 4 | 3 | 2 | 1 | 1 | 1 | 5 | 5 |
* Statement is only available to the staff.
Table 6.
MWU results for comparison of the staff and resident groups.
| Statements | MWU Test | |
|---|---|---|
| U | p | |
| S1 | 680 | 0.816 |
| S2 | 698.5 | 0.752 |
| S3 | 559.5 | 0.127 |
| S4 | 634 | 0.55 |
| S5 | 705 | 0.865 |
| S7 | 585.5 | 0.129 |
| S8 | 602.5 | 0.171 |
| S9 | 938.5 | 0.019 |
A statistically significant difference was found for bolded blue colored text data.
Table 7.
MWU/KW test results on the participant demographic factors within the staff and resident groups.
Table 7.
MWU/KW test results on the participant demographic factors within the staff and resident groups.
| Statements | Staff | Residents | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Age | Experience | Gender | Age | Experience | |||||||
| U | p | H | p | U | p | U | p | H | p | U | p | |
| S1 | 185.5 | 0.91 | 2.61 | 0.456 | 230.5 | 0.109 | 18 | 0.04 | 0.24 | 0.624 | 93.5 | 0.219 |
| S2 | 220 | 0.46 | 2.818 | 0.421 | 225.5 | 0.09 | 60 | 0.74 | 0.004 | 0.947 | 83 | 0.81 |
| S3 | 212.5 | 0.573 | 5.784 | 0.123 | 338 | 0.541 | 55.5 | 0.771 | 0.044 | 0.834 | 102 | 0.089 |
| S4 | 214.5 | 0.449 | 5.978 | 0.113 | 258 | 0.44 | 44 | 0.314 | 0.316 | 0.574 | 73.5 | 0.932 |
| S5 | 181 | 0.929 | 3.992 | 0.262 | 249.5 | 0.312 | 46 | 0.381 | 0.181 | 0.671 | 84 | 0.514 |
| S6 | 223.5 | 0.251 | 4.585 | 0.205 | 226 | 0.198 | N/A | N/A | N/A | N/A | N/A | N/A |
| S7 | 234 | 0.274 | 0.686 | 0.876 | 264.5 | 0.373 | 45 | 0.211 | 0.223 | 0.637 | 73.5 | 0.81 |
| S8 | 193 | 0.95 | 3.839 | 0.279 | 243 | 0.175 | 60.5 | 0.74 | 0.691 | 0.406 | 110 | 0.087 |
| S9 | 250.5 | 0.126 | 4.853 | 0.183 | 251.5 | 0.329 | 74.5 | 0.608 | 0.039 | 0.843 | 71.5 | 0.728 |
A statistically significant difference was found for bolded blue text data.
Table 8.
MWU test results on the demographic factors between the staff and resident groups.
| Statements | Gender | Age | Prior Robot Experience | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | 45–64 | 65+ | No Experience | Limited Experience | |||||||
| U | p | U | p | U | p | U | p | U | p | U | p | |
| S1 | 81.5 | 0.159 | 121.5 | 0.082 | 14 | 1 | 4 | 0.171 | 141 | 0.439 | 182 | 0.074 |
| S2 | 72 | 0.456 | 200 | 0.82 | 14.5 | 0.864 | 5 | 0.2 | 166 | 0.668 | 164.5 | 0.245 |
| S3 | 77.5 | 0.254 | 224 | 0.401 | 13 | 1 | 9 | 0.571 | 164.5 | 0.919 | 192 | 0.031 |
| S4 | 79 | 0.228 | 166.5 | 0.636 | 16.5 | 0.6 | 7 | 0.381 | 170 | 0.965 | 152.5 | 0.326 |
| S5 | 59.5 | 0.974 | 146 | 0.322 | 15.5 | 0.727 | 5 | 0.229 | 134.5 | 0.408 | 152 | 0.488 |
| S7 | 96 | 0.017 | 0.208 | 0.98 | 16.5 | 0.6 | 14.5 | 1 | 210 | 0.446 | 165 | 0.245 |
| S8 | 70.5 | 0.497 | 232 | 0.551 | 18 | 0.482 | 6 | 0.267 | 165 | 0.648 | 202 | 0.011 |
| S9 | 48 | 0.456 | 134 | 0.057 | 12 | 0.864 | 14.5 | 1 | 110.5 | 0.06 | 93.5 | 0.168 |
A statistically significant difference was found for bolded blue text data.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Li, Y.; Liang, N.; Effati, M.; Nejat, G. Dances with Social Robots: A Pilot Study at Long-Term Care. Robotics 2022, 11, 96. https://doi.org/10.3390/robotics11050096
AMA Style
Li Y, Liang N, Effati M, Nejat G. Dances with Social Robots: A Pilot Study at Long-Term Care. Robotics. 2022; 11(5):96. https://doi.org/10.3390/robotics11050096
Chicago/Turabian StyleLi, Yizhu, Nan Liang, Meysam Effati, and Goldie Nejat. 2022. "Dances with Social Robots: A Pilot Study at Long-Term Care" Robotics 11, no. 5: 96. https://doi.org/10.3390/robotics11050096
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.