Dietary Restrictions and Depressive Symptoms: Longitudinal Results from the Constances Cohort

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Population
2.2. Variables
2.2.1. Depressive Symptoms at Baseline and during the Follow-Up
2.2.2. Dietary Exclusions Measured at Baseline and during the Follow-Up
2.2.3. Covariates Measured at Baseline
Anemia
Physical Activity
Other Covariates
Missing Data
2.3. Statistical Analyses
2.3.1. Depressive Symptoms at Follow-Up
2.3.2. Dietary Exclusions at Follow-Up
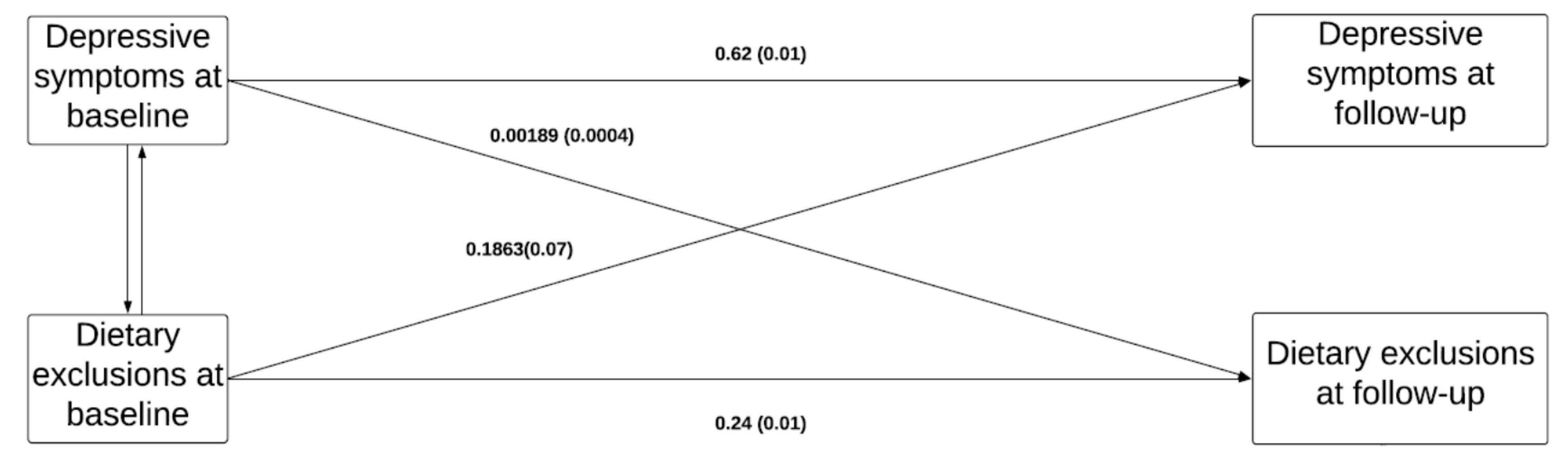
2.3.3. Path Analysis
2.3.4. Supplementary Analyses
Specificity Analyses
Sensitivity Analyses
3. Results
Supplementary Analyses
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Explanatory Hypotheses
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Sánchez-Villegas, A.; Delgado-Rodríguez, M.; Alonso, A.; Schlatter, J.; Lahortiga, F.; Majem, L.S.; Martínez-González, M.A. Association of the Mediterranean dietary pattern with the incidence of depression: The Seguimiento Universidad de Navarra/University of Navarra follow-up (SUN) cohort. Arch. Gen. Psychiatry 2009, 66, 1090–1098. [Google Scholar] [CrossRef]
- Kim, T.-H.; Choi, J.-Y.; Lee, H.-H.; Park, Y. Associations between dietary pattern and depression in Korean adolescent girls. J. Pediatr. Adolesc. Gynecol. 2015, 28, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef] [Green Version]
- Gougeon, L.; Payette, H.; Morais, J.; Gaudreau, P.; Shatenstein, B.; Gray-Donald, K. Dietary patterns and incidence of depression in a cohort of community-dwelling older Canadians. J. Nutr. Health Aging 2015, 19, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, E.; Knüppel, A.; Shipley, M.J.; Brouwer, I.A.; Visser, M.; Akbaraly, T.; Brunner, E.J.; Nicolaou, M. High-sugar, high-saturated-fat dietary patterns are not associated with depressive symptoms in middle-aged adults in a prospective study. J. Nutr. 2018, 148, 1598–1604. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, M.-R.; Wei, Y.-J.; Sun, L.; Zhang, J.-X.; Zhang, H.-G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Matta, J.; Czernichow, S.; Kesse-Guyot, E.; Hoertel, N.; Limosin, F.; Goldberg, M.; Zins, M.; Lemogne, C. Depressive symptoms and vegetarian diets: Results from the constances cohort. Nutrients 2018, 10, 1695. [Google Scholar] [CrossRef] [Green Version]
- Michalak, J.; Zhang, X.C.; Jacobi, F. Vegetarian diet and mental disorders: Results from a representative community survey. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 67. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.J.; Sanderson, K.; McNaughton, S.A.; Gall, S.L.; Dwyer, T.; Venn, A.J. Longitudinal associations between fish consumption and depression in young adults. Am. J. Epidemiol. 2014, 179, 1228–1235. [Google Scholar] [CrossRef]
- Kingsbury, M.; Dupuis, G.; Jacka, F.; Roy-Gagnon, M.-H.; McMartin, S.E.; Colman, I. Associations between fruit and vegetable consumption and depressive symptoms: Evidence from a national Canadian longitudinal survey. J. Epidemiol. Community Health 2016, 70, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Elstgeest, L.E.; Visser, M.; Penninx, B.W.; Colpo, M.; Bandinelli, S.; Brouwer, I.A. Bidirectional associations between food groups and depressive symptoms: Longitudinal findings from the Invecchiare in Chianti (InCHIANTI) study. Br. J. Nutr. 2019, 121, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Lavallee, K.; Zhang, X.C.; Michalak, J.; Schneider, S.; Margraf, J. Vegetarian diet and mental health: Cross-sectional and longitudinal analyses in culturally diverse samples. J. Affect. Disord. 2019, 248, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Puccio, F.; Fuller-Tyszkiewicz, M.; Ong, D.; Krug, I. A systematic review and meta-analysis on the longitudinal relationship between eating pathology and depression. Int. J. Eat. Disord. 2016, 49, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Voderholzer, U.; Hessler-Kaufmann, J.B.; Lustig, L.; Läge, D. Comparing severity and qualitative facets of depression between eating disorders and depressive disorders: Analysis of routine data. J. Affect. Disord. 2019, 257, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Vulser, H.; Wiernik, E.; Hoertel, N.; Thomas, F.; Pannier, B.; Czernichow, S.; Hanon, O.; Simon, T.; Simon, J.M.; Danchin, N.; et al. Association between depression and anemia in otherwise healthy adults. Acta Psychiatr. Scand. 2016, 134, 150–160. [Google Scholar] [CrossRef]
- Goetz, L.G.; Valeggia, C. The ecology of anemia: Anemia prevalence and correlated factors in adult indigenous women in Argentina. Am. J. Hum. Biol. 2017, 29, e22947. [Google Scholar] [CrossRef]
- Vulser, H.; Lemogne, C.; Boutouyrie, P.; Côté, F.; Perier, M.-C.; Van Sloten, T.; Hoertel, N.; Danchin, N.; Limosin, F.; Jouven, X. Depression, antidepressants and low hemoglobin level in the Paris Prospective Study III: A cross-sectional analysis. Prev. Med. 2020, 135, 106050. [Google Scholar] [CrossRef]
- Zins, M.; Goldberg, M. The French CONSTANCES population-based cohort: Design, inclusion and follow-up. Eur. J. Epidemiol. 2015, 30, 1317–1328. [Google Scholar] [CrossRef] [Green Version]
- Morin, A.J.; Moullec, G.; Maiano, C.; Layet, L.; Just, J.L.; Ninot, G. Psychometric properties of the Center for Epidemiologic Studies Depression Scale (CES-D) in French clinical and nonclinical adults. Rev. D’épidémiologie St. Publique 2011, 59, 327–340. [Google Scholar] [CrossRef]
- Hercberg, S.; Chat-Yung, S.; Chauliac, M. The French national nutrition and health program: 2001–2006–2010. Int. J. Public Health 2008, 53, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Plessz, M.; Kesse-Guyot, E.; Zins, M.; Matta, J.; Czernichow, S. Poverty does not modify the association between perceived diet healthiness and adherence to nutritional guidelines in the Constances cohort (France). Appetite 2019, 138, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Koyanagi, A.; Schuch, F.B.; Firth, J.; Rosenbaum, S.; Veronese, N.; Solmi, M.; Mugisha, J.; Vancampfort, D. Physical activity and depression: A large cross-sectional, population-based study across 36 low-and middle-income countries. Acta Psychiatr. Scand. 2016, 134, 546–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, A.; Simon, C.; Evans, A.; Ferrières, J.; Montaye, M.l.; Ducimetière, P.; Arveiler, D. Physical activity and coronary event incidence in Northern Ireland and France: The Prospective Epidemiological Study of Myocardial Infarction (PRIME). Circulation 2002, 105, 2247–2252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pino, E.C.; Damus, K.; Jack, B.; Henderson, D.; Milanovic, S.; Kalesan, B. Adolescent socioeconomic status and depressive symptoms in later life: Evidence from structural equation models. J. Affect. Disord. 2018, 225, 702–708. [Google Scholar] [CrossRef]
- Stage, F.K.; Carter, H.C.; Nora, A. Path analysis: An introduction and analysis of a decade of research. J. Educ. Res. 2004, 98, 5–13. [Google Scholar] [CrossRef]
- Blanco, C.; Hoertel, N.; Wall, M.M.; Franco, S.; Peyre, H.; Neria, Y.; Helpman, L.; Limosin, F. Toward Understanding Sex Differences in the Prevalence of Posttraumatic Stress Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2018, 79, 16m11364. [Google Scholar] [CrossRef]
- Wolfe, A.R.; Ogbonna, E.M.; Lim, S.; Li, Y.; Zhang, J. Dietary linoleic and oleic fatty acids in relation to severe depressed mood: 10 years follow-up of a national cohort. Prog. NeuroPsychopharmacol. Biol. Psychiatry 2009, 33, 972–977. [Google Scholar] [CrossRef]
- Wang, J.; Um, P.; Dickerman, B.A.; Liu, J. Zinc, magnesium, selenium and depression: A review of the evidence, potential mechanisms and implications. Nutrients 2018, 10, 584. [Google Scholar] [CrossRef] [Green Version]
- Molendijk, M.; Molero, P.; Sánchez-Pedreño, F.O.; Van der Does, W.; Martínez-González, M.A. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef] [Green Version]
- Appleton, K.; Woodside, J.; Yarnell, J.; Arveiler, D.; Haas, B.; Amouyel, P.; Montaye, M.; Ferrieres, J.; Ruidavets, J.; Ducimetiere, P. Depressed mood and dietary fish intake: Direct relationship or indirect relationship as a result of diet and lifestyle? J. Affect. Disord. 2007, 104, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Assmann, K.; Deschasaux, M.; Andreeva, V.; Lemogne, C.; Charnaux, N.; Sutton, A.; Hercberg, S.; Galan, P.; Touvier, M. Statut en vitamine D et symptômes dépressifs récurrents dans la cohorte française SU. VI. MAX. Nutr. Clin. Métabolisme 2017, 31, 60–61. [Google Scholar] [CrossRef]
- Andreeva, V.A.; Galan, P.; Torres, M.; Julia, C.; Hercberg, S.; Kesse-Guyot, E. Supplementation with B vitamins or n–3 fatty acids and depressive symptoms in cardiovascular disease survivors: Ancillary findings from the SUpplementation with FOLate, vitamins B-6 and B-12 and/or OMega-3 fatty acids (SU. FOL. OM3) randomized trial. Am. J. Clin. Nutr. 2012, 96, 208–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| All (%) | No Depressive Symptoms at Follow-Up (CES-D Score <19) | Depressive Symptoms at Follow-Up (CES-D Score ≥19) | p-Value (Depressive Symptoms versus No Depressive Symptoms) | |
|---|---|---|---|---|
| Women, N (%) | 15,671 (53.42) | 12,223 (50.57) | 3448 (66.74) | <0.0001 |
| Age, mean (SD) | 49.14 (12.91) | 47.88 (12.49) | 49.41 (12.98) | <0.0001 |
| Household income, N (%) | <0.0001 | |||
| <1500 euros or does not want to answer | 3562 (12.14) | 2544 (10.53) | 1018 (19.71) | |
| 1500 to less than 2800 euros | 7419 (25.29) | 5793 (23.97) | 1626 (31.48) | |
| ≥2800 euros | 18,356 (62.57) | 15,834 (65.51) | 2522 (48.82) | |
| Education level, N (%) | <0.0001 | |||
| ≤ high school diploma or other diploma | 11,515 (39.25) | 9225 (38.17) | 2290 (44.33) | |
| Undergraduate degree | 10,622 (36.21) | 8749 (36.20) | 1873 (36.26) | |
| Postgraduate degree | 7200 (24.54) | 6197 (26.64) | 1003 (19.42) | |
| Depressive symptoms (CES-D score ≥19), N (%) | 4066 (13.86) | 1614 (6.68) | 2452 (47.46) | <0.0001 |
| Dietary exclusions, N (%) | <0.0001 | |||
| No exclusion | 21,844 (74.16) | 18,305 (75.73) | 3539 (68.51) | |
| 1 exclusion | 5716 (19.48) | 4538 (18.77) | 1178(22.80) | |
| 2 exclusions | 1342 (4.57) | 1039 (4.30) | 303 (5.87) | |
| 3 exclusions | 309 (1.05) | 214 (0.89) | 95 (1.84) | |
| ≥4 exclusions | 126 (0.43) | 75 (0.31) | 51 (0.99) | |
| Alcohol intake, N (%) | <0.0001 | |||
| 1/week or more | 18,372 (62.62) | 15,453 (63.93) | 2919 (56.50) | |
| 2–3/months | 5987 (20.41) | 4916 (20.34) | 1071 (20.73) | |
| 1/month or less | 3857 (13.15) | 2980 (12.33) | 877 (16.98) | |
| Never | 1121 (3.82) | 822 (3.40) | 299 (5.79) | |
| Smoking status, N (%) | <0.0001 | |||
| Non-Smokers | 13,561 (46.22) | 11,365 (47.02) | 2196 (42.51) | |
| Smokers | 4915 (16.75) | 3721 (15.39) | 1194 (23.11) | |
| Ex-smokers | 10,861 (37.02) | 9085 (37.59) | 1776 (34.38) | |
| Physical activity level, N (%) | <0.0001 | |||
| Low | 7615 (25.95) | 5918 (24.48) | 1697 (32.85) | |
| Moderate | 13,569 (46.25) | 11,260 (46.58) | 2309 (44.70) | |
| High | 8153 (27.79) | 6993 (28.93) | 1160 (22.45) | |
| Anemia, N (%) | 818 (2.78) | 644 (2.66) | 174 (3.37) | 0.005 |
| All (%) | No Exclusion | 1 Exclusion | 2 Exclusions | 3 Exclusions | ≥4 Exclusions | p-Value | |
|---|---|---|---|---|---|---|---|
| Women, N (%) | 13,580 (53.5) | 11,957 (53.32) | 1284 (56.44) | 261 (55.18) | 62 (48.06) | 16 (30.19) | 0.0002 |
| Age, mean (SD) | 49.9 (12.8) | 50.60 (12.65) | 45.73 (12.90) | 43.46 (13.07) | 45.25 (13.06) | 41.75 (12.12) | <0.0001 |
| Household income, N (%) | <0.0001 | ||||||
| <1500 euros or does not want to answer | 2902 (11.4) | 2365 (10.55) | 375 (16.48) | 107 (22.62) | 38 (29.46) | 17 (32.08) | |
| 1500 to less than 2800 euros | 6354 (25.0) | 5407 (24.11) | 724 (31.82) | 161 (34.04) | 40 (31.01) | 22 (41.51) | |
| ≥2800 euros | 16,100 (63.4) | 14,654 (65.34) | 1176 (51.69) | 205 (43.34) | 51 (39.53) | 14 (26.42) | |
| Education level, N (%) | <0.0001 | ||||||
| ≤ high school diploma or other diploma | 10,005 (39.4) | 8699 (38.79) | 992 (43.60) | 213 (45.03) | 66 (51.16) | 35 (66.04) | |
| Undergraduate degree | 9069 (35.7) | 8023 (35.78) | 824 (36.22) | 170 (35.94) | 36 (27.91) | 16 (30.19) | |
| Postgraduate degree | 6282 (24.7) | 5704 (25.43) | 459 (20.18) | 90 (19.03) | 27 (20.93) | 2 (3.77) | |
| Depressive symptoms (CES-D score ≥19), N (%) | 3350 (12.2) | 2771 (12.36) | 431 (18.95) | 96 (20.30) | 31 (24.03) | 21 (39.62) | <0.0001 |
| Dietary exclusions at baseline, N (%) | <0.0001 | ||||||
| No exclusion | 19,069 (75.2) | 17,852 (79.60) | 1012 (44.48) | 167 (35.31) | 30 (23.26) | 8 (15.09) | |
| 1 exclusion | 4829 (19.0) | 3787 (16.89) | 856 (37.63) | 137 (28.96) | 40 (31.01) | 9 (16.98) | |
| 2 exclusions | 1126 (4.4) | 657 (2.93) | 309 (13.58) | 117 (24.74) | 29 (22.48) | 14 (26.42) | |
| 3 exclusions | 251 (0.98) | 106 (0.47) | 84 (3.69) | 33 (6.98) | 15 (11.63) | 13 (24.53) | |
| ≥4 exclusions | 81 (0.31) | 24 (0.11) | 14 (0.62) | 19 (4.02) | 15 (11.63) | 9 (16.98) | |
| Alcohol intake, N (%) | <0.0001 | ||||||
| 1/week or more | 15,911 (62.7) | 14,330 (63.90) | 1245 (54.73) | 243 (51.37) | 66 (51.16) | 27 (50.94) | |
| 2–3/months | 5214 (20.5) | 4573 (20.39) | 495 (21.76) | 105 (22.20) | 29 (22.48) | 12 (22.64) | |
| 1/month or less | 3302 (13.0) | 2785 (12.42) | 400 (17.58) | 83 (17.55) | 23 (17.83) | 11 (20.75) | |
| Never | 929 (3.6) | 738 (3.29) | 135 (5.93) | 42 (8.88) | 11 (8.53) | 3 (5.66) | |
| Smoking status, N (%) | <0.0001 | ||||||
| Non-Smokers | 11,937 (47.0) | 10,671 (47.58) | 976 (42.90) | 206 (43.55) | 63 (48.84) | 21 (39.62) | |
| Smokers | 3916 (15.4) | 3264 (14.55) | 493 (21.67) | 106 (22.41) | 31 (24.03) | 22 (41.51) | |
| Ex-smokers | 9503 (37.4) | 8491 (37.86) | 806 (35.43) | 161 (34.04) | 35 (27.13) | 10 (18.87) | |
| Physical activity level, N (%) | <0.0001 | ||||||
| Low | 6368 (25.1) | 5391 (24.04) | 737 (32.40) | 152 (32.14) | 56 (43.41) | 32 (60.38) | |
| Moderate | 11,721 (46.2) | 10,403 (46.39) | 1059 (46.55) | 199 (42.07) | 45 (34.88) | 15 (28.30) | |
| High | 7267 (28.6) | 6632 (22.57) | 479 (21.05) | 122 (25.79) | 28 (21.71) | 6 (11.32) | |
| Anemia, N (%) | 694 (2.73) | 580 (2.59) | 86 (3.78) | 21 (4.44) | 5 (3.88) | 2 (3.77) | 0.0018 |
| Exclusions at Baseline | Model 1 | Model 2 |
|---|---|---|
| No dietary exclusions | Ref | Ref |
| One exclusion | 1.30 (1.19–1.38) | 1.18 (1.09–1.27) |
| Two exclusions | 1.47 (1.28–1.68) | 1.23 (1.07–1.42) |
| Three exclusions | 2.30 (1.79–2.95) | 1.64 (1.27–2.11) |
| Four and more | 3.47 (2.41–4.99) | 2.35 (1.62–3.40) |
| Exclusions | No Dietary Exclusionsat Follow-Up | One Exclusion at Follow-Up | Two Exclusions at Follow-Up | Three Exclusions at Follow-Up | Four and More at Follow-Up |
|---|---|---|---|---|---|
| Model 1 | Ref | 1.62 (1.45–1.82) | 1.79 (1.42–2.25) | 2.34 (1.55–3.52) | 5.56 (3.18–9.74) |
| Model 2 | Ref | 1.37 (1.22–1.54) | 1.42 (1.12–1.79) | 1.68 (1.10–2.57) | 3.45 (1.93–6.16) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matta, J.; Hoertel, N.; Airagnes, G.; Czernichow, S.; Kesse-Guyot, E.; Limosin, F.; Goldberg, M.; Zins, M.; Lemogne, C. Dietary Restrictions and Depressive Symptoms: Longitudinal Results from the Constances Cohort. Nutrients 2020, 12, 2700. https://doi.org/10.3390/nu12092700
Matta J, Hoertel N, Airagnes G, Czernichow S, Kesse-Guyot E, Limosin F, Goldberg M, Zins M, Lemogne C. Dietary Restrictions and Depressive Symptoms: Longitudinal Results from the Constances Cohort. Nutrients. 2020; 12(9):2700. https://doi.org/10.3390/nu12092700
Chicago/Turabian StyleMatta, Joane, Nicolas Hoertel, Guillaume Airagnes, Sebastien Czernichow, Emmanuelle Kesse-Guyot, Frederic Limosin, Marcel Goldberg, Marie Zins, and Cédric Lemogne. 2020. "Dietary Restrictions and Depressive Symptoms: Longitudinal Results from the Constances Cohort" Nutrients 12, no. 9: 2700. https://doi.org/10.3390/nu12092700