A Metabolomics Analysis of Adiposity and Advanced Prostate Cancer Risk in the Health Professionals Follow-Up Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Population Characteristics
2.2. Metabolites Associated with Adiposity
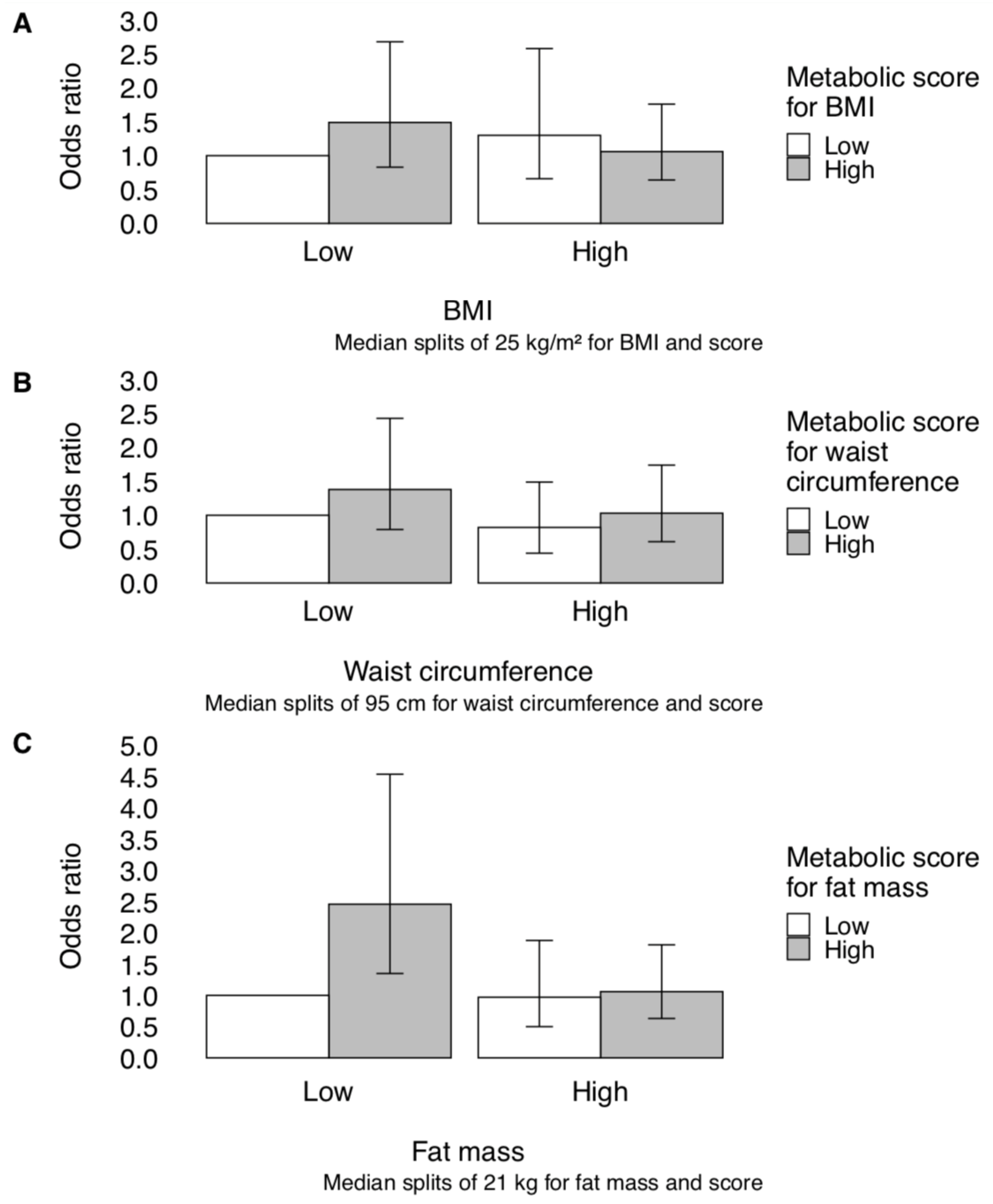
2.3. Metabolically Defined Obesity and Advanced Prostate Cancer Risk
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Adiposity Measures and Covariates
4.3. Metabolite Profiling
4.4. Statistical Analysis
4.4.1. Subgroup Analyses
4.4.2. Sensitivity Analyses
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cao, Y.; Ma, J. Body mass index, prostate cancer-specific mortality, and biochemical recurrence: A systematic review and meta-analysis. Cancer Prev Res. 2011, 4, 486–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, N.; Schick, F.; Haring, H.U. Causes, characteristics, and consequences of metabolically unhealthy normal weight in humans. Cell Metab. 2017, 26, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Batch, B.C.; Shah, S.H.; Newgard, C.B.; Turer, C.B.; Haynes, C.; Bain, J.R.; Muehlbauer, M.; Patel, M.J.; Stevens, R.D.; Appel, L.J.; et al. Branched chain amino acids are novel biomarkers for discrimination of metabolic wellness. Metabolism. 2013, 62, 961–969. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.E.; Larson, M.G.; Ghorbani, A.; Cheng, S.; Chen, M.H.; Keyes, M.; Rhee, E.P.; Clish, C.B.; Vasan, R.S.; Gerszten, R.E.; et al. Metabolomic profiles of body mass index in the Framingham Heart Study reveal distinct cardiometabolic phenotypes. PLoS ONE. 2016, 11, e0148361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildman, R.P.; Muntner, P.; Reynolds, K.; McGinn, A.P.; Rajpathak, S.; Wylie-Rosett, J.; Sowers, M.R. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: Prevalence and correlates of 2 phenotypes among the US population (NHANES 19992–004). Arch. Intern. Med. 2008, 168, 1617–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.; Rhee, E.P.; Larson, M.G.; Lewis, G.D.; McCabe, E.L.; Shen, D.; Palma, M.J.; Roberts, L.D.; Dejam, A.; Souza, A.L.; et al. Metabolite profiling identifies pathways associated with metabolic risk in humans. Circulation. 2012, 125, 2222–2231. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.C.; Matthews, C.E.; Sampson, J.N.; Stolzenberg-Solomon, R.Z.; Zheng, W.; Cai, Q.; Tan, Y.T.; Chow, W.H.; Ji, B.T.; Liu, D.K.; et al. Human metabolic correlates of body mass index. Metabolomics. 2014, 10, 259–269. [Google Scholar] [CrossRef]
- Moore, S.C.; Playdon, M.C.; Sampson, J.N.; Hoover, R.N.; Trabert, B.; Matthews, C.E.; Ziegler, R.G. A metabolomics analysis of body mass index and postmenopausal breast cancer risk. J. Natl Cancer Inst. 2018, 110, 588–597. [Google Scholar] [CrossRef]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef] [Green Version]
- Ottosson, F.; Brunkwall, L.; Ericson, U.; Nilsson, P.M.; Almgren, P.; Fernandez, C.; Melander, O.; Orho-Melander, M. Connection between BMI-related plasma metabolite profile and gut microbiota. J. Clin Endocrinol Metab. 2018, 103, 1491–1501. [Google Scholar] [CrossRef] [Green Version]
- Boulet, M.M.; Chevrier, G.; Grenier-Larouche, T.; Pelletier, M.; Nadeau, M.; Scarpa, J.; Prehn, C.; Marette, A.; Adamski, J.; Tchernof, A. Alterations of plasma metabolite profiles related to adipose tissue distribution and cardiometabolic risk. Am. J. Physiol Endocrinol Metab. 2015, 309, E736–E746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foerster, J.; Hyotylainen, T.; Oresic, M.; Nygren, H.; Boeing, H. Serum Lipid and Serum Metabolite Components in relation to anthropometric parameters in EPIC-Potsdam participants. Metabolism. 2015, 64, 1348–1358. [Google Scholar] [CrossRef] [PubMed]
- Wang-Sattler, R.; Yu, Z.; Herder, C.; Messias, A.C.; Floegel, A.; He, Y.; Heim, K.; Campillos, M.; Holzapfel, C.; Thorand, B.; et al. Novel biomarkers for pre-diabetes identified by metabolomics. Mol. Syst. Biol. 2012, 8, 615. [Google Scholar] [CrossRef] [PubMed]
- Rebouche, C. Carnitine. In Modern Nutrition in Health and Disease, 10th ed.; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 537–544. [Google Scholar]
- Rebouche, C.J. Kinetics, pharmacokinetics, and regulation of L-carnitine and acetyl-L-carnitine metabolism. Ann. N Y Acad Sci. 2004, 1033, 30–41. [Google Scholar] [CrossRef]
- Mihalik, S.J.; Goodpaster, B.H.; Kelley, D.E.; Chace, D.H.; Vockley, J.; Toledo, F.G.; DeLany, J.P. Increased levels of plasma acylcarnitines in obesity and type 2 diabetes and identification of a marker of glucolipotoxicity. Obesity 2010, 18, 1695–1700. [Google Scholar] [CrossRef] [Green Version]
- Baek, S.H.; Kim, M.; Kim, M.; Kang, M.; Yoo, H.J.; Lee, N.H.; Kim, Y.H.; Song, M.; Lee, J.H. Metabolites distinguishing visceral fat obesity and atherogenic traits in individuals with overweight. Obesity 2017, 25, 323–331. [Google Scholar] [CrossRef]
- Floegel, A.; Stefan, N.; Yu, Z.; Muhlenbruch, K.; Drogan, D.; Joost, H.G.; Fritsche, A.; Haring, H.U.; Hrabe de Angelis, M.; Peters, A.; et al. Identification of serum metabolites associated with risk of type 2 diabetes using a targeted metabolomic approach. Diabetes 2013, 62, 639–648. [Google Scholar] [CrossRef] [Green Version]
- Greenfield, J.R.; Farooqi, I.S.; Keogh, J.M.; Henning, E.; Habib, A.M.; Blackwood, A.; Reimann, F.; Holst, J.J.; Gribble, F.M. Oral glutamine increases circulating glucagon-like peptide 1, glucagon, and insulin concentrations in lean, obese, and type 2 diabetic subjects. Am. J. Clin Nutr. 2009, 89, 106–113. [Google Scholar] [CrossRef]
- Discacciati, A.; Orsini, N.; Wolk, A. Body mass index and incidence of localized and advanced prostate cancer--a dose-response meta-analysis of prospective studies. Ann. Oncol. 2012, 23, 1665–1671. [Google Scholar] [CrossRef]
- Scott, R.A.; Fall, T.; Pasko, D.; Barker, A.; Sharp, S.J.; Arriola, L.; Balkau, B.; Barricarte, A.; Barroso, I.; Boeing, H.; et al. Common genetic variants highlight the role of insulin resistance and body fat distribution in type 2 diabetes, independent of obesity. Diabetes 2014, 63, 4378–4387. [Google Scholar] [CrossRef] [Green Version]
- Giovannucci, E.; Michaud, D. The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology 2007, 132, 2208–2225. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Stampfer, M.J.; Colditz, G.A.; Chute, C.G.; Litin, L.B.; Willett, W.C. Validity of self-reported waist and hip circumferences in men and women. Epidemiology 1990, 1, 466–473. [Google Scholar] [CrossRef]
- Townsend, M.K.; Clish, C.B.; Kraft, P.; Wu, C.; Souza, A.L.; Deik, A.A.; Tworoger, S.S.; Wolpin, B.M. Reproducibility of metabolomic profiles among men and women in 2 large cohort studies. Clin Chem. 2013, 59, 1657–1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.H.; Keum, N.; Hu, F.B.; Orav, E.J.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Giovannucci, E.L. Development and validation of anthropometric prediction equations for lean body mass, fat mass and percent fat in adults using the National Health and Nutrition Examination Survey (NHANES) 1999-2006. Br. J. Nutr. 2017, 118, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Paynter, N.P.; Balasubramanian, R.; Giulianini, F.; Wang, D.D.; Tinker, L.F.; Gopal, S.; Deik, A.A.; Bullock, K.; Pierce, K.A.; Scott, J.; et al. Metabolic predictors of incident coronary heart disease in women. Circulation 2018, 137, 841–853. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Statist. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic, Mean (SD) or % | Amyotrophic Lateral Sclerosis Study | Parkinson’s Disease Study | Prostate Cancer Study | |
|---|---|---|---|---|
| Controls (n = 52) | Controls (n = 184) | Controls (n = 212) | Advanced Cases (n = 212) | |
| Age (years) | 62.7 (8.3) | 65.3 (8.0) | 65.3 (8.4) | 65.4 (8.5) |
| Body mass index (kg/m2) | 25.9 (2.5) | 25.5 (2.8) | 25.8 (3.6) | 25.8 (4.1) |
| Waist circumference (cm) | 94.7 (8.1) | 95.5 (8.5) | 96.5 (10.3) | 95.7 (9.8) |
| Derived fat mass (kg) b | 21.9 (4.3) | 21.6 (5.2) | 22.5 (6.4) | 21.7 (5.9) |
| Total physical activity (MET hours/week) | 39.7 (29.3) | 34.4 (27.4) | 32.5 (25.6) | 31.1 (28.9) |
| Year of blood donation | ||||
| 1993–1994 | 87 | 94 | 97 | 97 |
| 1995–1996 | 14 | 6 | 3 | 3 |
| Fasting ≥ 8 h | 50 | 55 | 62 | 67 |
| Race/ethnicity, White | 94 | 98 | 97 | 99 |
| Smoking status | ||||
| Never | 50 | 39 | 46 | 43 |
| Former | 46 | 58 | 50 | 51 |
| Current | 4 | 3 | 4 | 7 |
| History of diabetes mellitus | 4 | 4 | 6 | 7 |
| Family history of prostate cancer | -- | -- | 9 | 9 |
| Recent prostate-specific antigen testing c | -- | -- | 60 | 62 |
| HMDB ID b | Metabolite Name | Body Mass Index | Waist Circumference | Derived Fat Mass | |||
|---|---|---|---|---|---|---|---|
| Pearson Correlation Coefficient c | FDR p-value | Pearson Correlation Coefficient c | FDR p-value | Pearson Correlation Coefficient c | FDR p-value | ||
| Amino acids | |||||||
| HMDB00123 | glycine | −0.29 | <0.001 | −0.20 | 0.02 | −0.25 | 0.01 |
| HMDB00641 | glutamine | −0.19 | 0.02 | −0.19 | 0.03 | −0.19 | 0.04 |
| Carnitines | |||||||
| HMDB06347 | C26 carnitine | 0.18 | 0.03 | 0.18 | 0.04 | -- | -- |
| HMDB00688 | C5 carnitine | 0.18 | 0.03 | -- | -- | -- | -- |
| HMDB00705 | C6 carnitine | 0.18 | 0.03 | 0.18 | 0.03 | -- | -- |
| HMDB02013 | C4 carnitine | 0.16 | 0.05 | -- | -- | -- | -- |
| HMDB13326 | C12:1 carnitine | -- | -- | 0.17 | 0.04 | -- | -- |
| HMDB00222 | C16 carnitine | -- | -- | -- | -- | 0.18 | 0.04 |
| Lipids | |||||||
| CE | |||||||
| HMDB10375 | C22:5 CE | −0.20 | 0.01 | −0.22 | 0.01 | −0.23 | 0.01 |
| HMDB06733 | C22:6 CE | -- | -- | -- | -- | −0.19 | 0.03 |
| DAG | |||||||
| Saturated | |||||||
| HMDB07098 | C32:0 DAG | 0.23 | 0.01 | 0.21 | 0.01 | 0.22 | 0.01 |
| Unsaturated | |||||||
| HMDB07102 | C34:1 DAG | 0.24 | <0.01 | 0.24 | 0.01 | 0.24 | 0.01 |
| HMDB07099 | C32:1 DAG | 0.23 | 0.01 | 0.24 | 0.01 | 0.24 | 0.01 |
| HMDB07103 | C34:2 DAG | 0.22 | 0.01 | 0.23 | 0.01 | 0.23 | 0.01 |
| HMDB07132 | C34:3 DAG | 0.22 | 0.01 | 0.23 | 0.01 | 0.22 | 0.01 |
| HMDB07218 | C36:2 DAG | 0.21 | 0.01 | 0.23 | 0.01 | 0.22 | 0.01 |
| HMDB07216 | C36:1 DAG | 0.21 | 0.01 | 0.22 | 0.01 | 0.23 | 0.01 |
| HMDB07219 | C36:3 DAG | 0.20 | 0.02 | 0.21 | 0.01 | 0.20 | 0.02 |
| HMDB07248 | C36:4 DAG | 0.17 | 0.04 | 0.17 | 0.04 | -- | -- |
| HMDB07199 | C38:5 DAG | 0.16 | 0.05 | -- | -- | -- | -- |
| LPC | |||||||
| HMDB10386 | C18:2 LPC | −0.34 | <0.0001 | −0.23 | 0.01 | −0.29 | <0.001 |
| HMDB10397 | C20:5 LPC | −0.34 | <0.0001 | −0.24 | 0.01 | −0.29 | <0.001 |
| HMDB02815 | C18:1 LPC | −0.29 | <0.001 | −0.21 | 0.01 | −0.26 | 0.01 |
| HMDB10404 | C22:6 LPC | −0.25 | <0.01 | −0.18 | 0.03 | −0.26 | 0.01 |
| LPE | |||||||
| HMDB11503 | C16:0 LPE | −0.29 | <0.001 | −0.17 | 0.04 | −0.23 | 0.01 |
| HMDB11507 | C18:2 LPE | −0.26 | <0.01 | -- | -- | -- | -- |
| HMDB11506 | C18:1 LPE | −0.22 | 0.01 | -- | -- | −0.18 | 0.04 |
| HMDB11130 | C18:0 LPE | −0.20 | 0.02 | -- | -- | -- | -- |
| HMDB11526 | C22:6 LPE | −0.19 | 0.02 | -- | -- | -- | -- |
| PC | |||||||
| HMDB11210 | C34:2 PC plasmalogen | −0.16 | 0.05 | -- | -- | -- | -- |
| HMDB08047 | C38:3 PC | 0.20 | 0.01 | 0.20 | 0.02 | -- | -- |
| HMDB08057 | C40:6 PC | 0.19 | 0.02 | 0.19 | 0.03 | -- | -- |
| HMDB08511 | C40:10 PC | −0.16 | 0.05 | -- | -- | −0.18 | 0.04 |
| TAG | |||||||
| Unsaturated | |||||||
| HMDB05369 | C52:2 TAG | 0.23 | 0.01 | 0.23 | 0.01 | 0.23 | 0.01 |
| HMDB05360 | C50:1 TAG | 0.23 | 0.01 | 0.21 | 0.01 | 0.22 | 0.01 |
| HMDB05384 | C52:3 TAG | 0.22 | 0.01 | 0.22 | 0.01 | 0.21 | 0.02 |
| HMDB05433 | C50:3 TAG | 0.22 | 0.01 | 0.23 | 0.01 | 0.22 | 0.01 |
| HMDB05377 | C50:2 TAG | 0.22 | 0.01 | 0.21 | 0.01 | 0.22 | 0.01 |
| HMDB05367 | C52:1 TAG | 0.20 | 0.01 | 0.20 | 0.02 | 0.21 | 0.01 |
| HMDB05376 | C48:2 TAG | 0.19 | 0.02 | 0.20 | 0.02 | 0.21 | 0.02 |
| HMDB05432 | C48:3 TAG | 0.18 | 0.03 | 0.20 | 0.02 | 0.20 | 0.02 |
| HMDB10412 | C46:1 TAG | 0.18 | 0.03 | 0.17 | 0.04 | 0.20 | 0.02 |
| HMDB05403 | C54:2 TAG | 0.18 | 0.03 | 0.20 | 0.02 | 0.20 | 0.02 |
| HMDB05363 | C52:4 TAG | 0.18 | 0.03 | 0.18 | 0.03 | -- | -- |
| HMDB05359 | C48:1 TAG | 0.17 | 0.04 | 0.17 | 0.04 | 0.18 | 0.04 |
| HMDB10419 | C46:2 TAG | 0.17 | 0.05 | 0.17 | 0.04 | 0.19 | 0.04 |
| HMDB05435 | C50:4 TAG | -- | -- | 0.17 | 0.04 | -- | -- |
| HMDB05405 | C54:3 TAG | -- | -- | 0.18 | 0.04 | -- | -- |
| Purine nucleosides | |||||||
| HMDB03331 | 1-methyladenosine | -- | -- | 0.18 | 0.03 | 0.18 | 0.04 |
| Adiposity Measure | Self-reported or Derived | Metabolic Score | ||||
|---|---|---|---|---|---|---|
| Cases/ Total | Odds Ratio | 95% CI | Cases/ Total | Odds Ratio | 95% CI | |
| Body mass index (kg/m2) b | ||||||
| per 5 kg/m2 increase | 201/409 | 0.96 | (0.73, 1.27) | 201/409 | 1.18 | (0.57, 2.48) |
| Quartile 1 | 46/104 | 1.00 | -- | 49/103 | 1.00 | -- |
| Quartile 2 | 60/102 | 1.78 | (1.02, 3.13) | 40/102 | 0.71 | (0.40, 1.23) |
| Quartile 3 | 49/102 | 1.14 | (0.65, 1.98) | 60/102 | 1.57 | (0.90, 2.75) |
| Quartile 4 | 46/101 | 1.04 | (0.60, 1.82) | 52/102 | 1.12 | (0.64, 1.97) |
| p-trend | 0.72 | 0.20 | ||||
| Waist circumference (cm) c | ||||||
| per 1 SD increase | 200/408 | 0.90 | (0.73, 1.10) | 200/408 | 0.99 | (0.81, 1.21) |
| Quartile 1 | 53/110 | 1.00 | -- | 45/102 | 1.00 | -- |
| Quartile 2 | 52/96 | 1.25 | (0.72, 2.19) | 52/102 | 1.35 | (0.77, 2.36) |
| Quartile 3 | 52/110 | 0.93 | (0.54, 1.60) | 53/102 | 1.38 | (0.79, 2.43) |
| Quartile 4 | 43/92 | 0.90 | (0.50, 1.59) | 50/102 | 1.19 | (0.67, 2.12) |
| p-trend | 0.52 | 0.54 | ||||
| Derived fat mass (kg) d | ||||||
| per 1 SD increase | 193/388 | 0.89 | (0.73, 1.10) | 193/388 | 1.07 | (0.82, 1.39) |
| Quartile 1 | 49/97 | 1.00 | -- | 42/97 | 1.00 | -- |
| Quartile 2 | 54/97 | 1.20 | (0.68, 2.13) | 51/97 | 1.45 | (0.82, 2.58) |
| Quartile 3 | 44/97 | 0.78 | (0.44, 1.38) | 54/97 | 1.63 | (0.92, 2.91) |
| Quartile 4 | 46/97 | 0.84 | (0.47, 1.50) | 46/97 | 1.15 | (0.64, 2.06) |
| p-trend | 0.30 | 0.54 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dickerman, B.A.; Ebot, E.M.; Healy, B.C.; Wilson, K.M.; Eliassen, A.H.; Ascherio, A.; Pernar, C.H.; Zeleznik, O.A.; Vander Heiden, M.G.; Clish, C.B.; et al. A Metabolomics Analysis of Adiposity and Advanced Prostate Cancer Risk in the Health Professionals Follow-Up Study. Metabolites 2020, 10, 99. https://doi.org/10.3390/metabo10030099
Dickerman BA, Ebot EM, Healy BC, Wilson KM, Eliassen AH, Ascherio A, Pernar CH, Zeleznik OA, Vander Heiden MG, Clish CB, et al. A Metabolomics Analysis of Adiposity and Advanced Prostate Cancer Risk in the Health Professionals Follow-Up Study. Metabolites. 2020; 10(3):99. https://doi.org/10.3390/metabo10030099
Chicago/Turabian StyleDickerman, Barbra A., Ericka M. Ebot, Brian C. Healy, Kathryn M. Wilson, A. Heather Eliassen, Alberto Ascherio, Claire H. Pernar, Oana A. Zeleznik, Matthew G. Vander Heiden, Clary B. Clish, and et al. 2020. "A Metabolomics Analysis of Adiposity and Advanced Prostate Cancer Risk in the Health Professionals Follow-Up Study" Metabolites 10, no. 3: 99. https://doi.org/10.3390/metabo10030099