We are What We Eat: Impact of Food from Short Supply Chain on Metabolic Syndrome

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Study Approval
2.3. Data Acquisition
2.4. Blood Sample Laboratory Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Features of Study Population
3.2. Effects of SSCs on Clinical Features
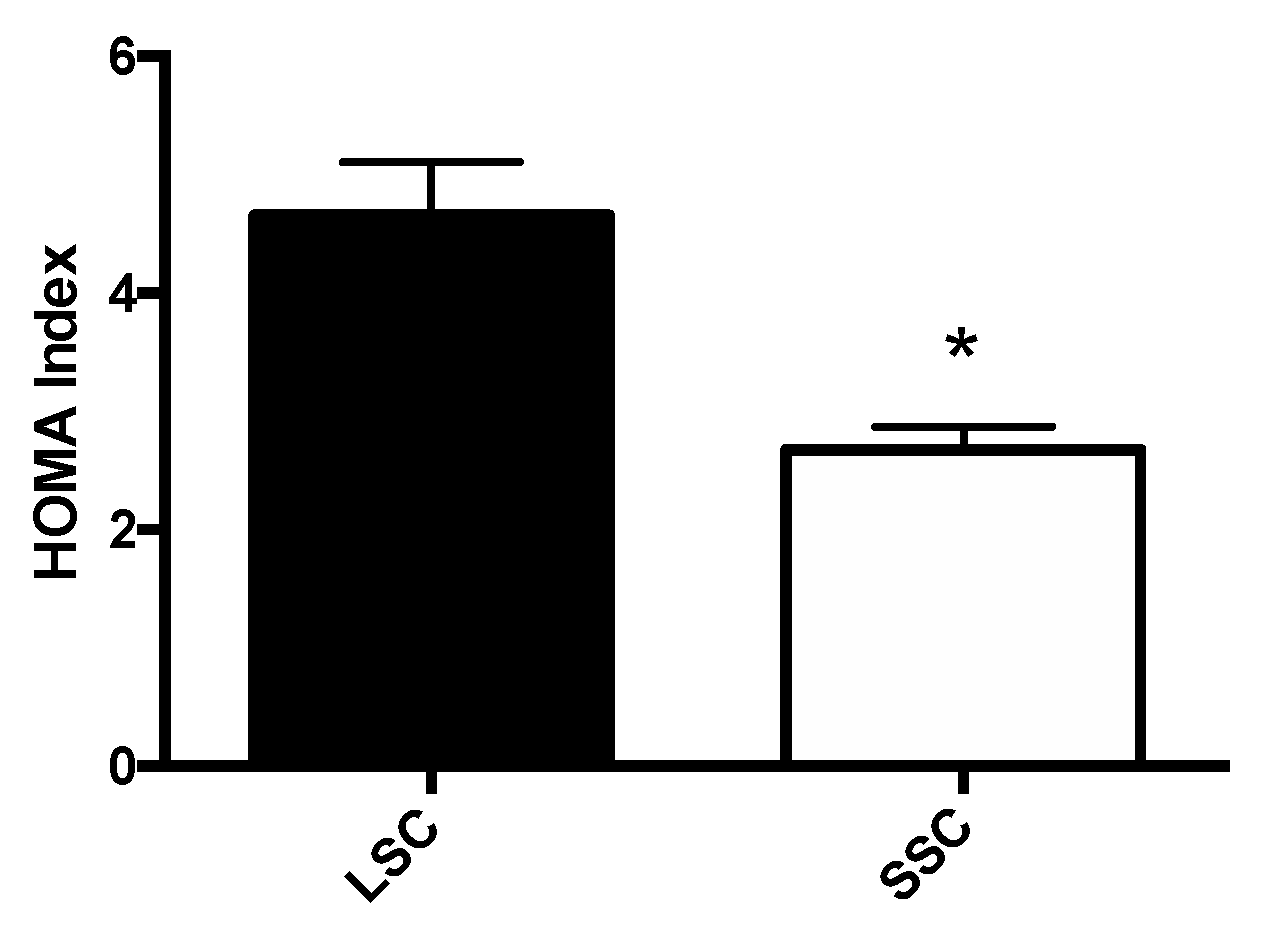
3.3. Effects of SSCs on Insulin Sensitivity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Salas-Salvado, J.; Guasch-Ferre, M.; Lee, C.H.; Estruch, R.; Clish, C.B.; Ros, E. Protective effects of the Mediterranean diet on Type 2 Diabetes and metabolic syndrome. J. Nutr. 2016, 146, 920S–927S. [Google Scholar] [CrossRef]
- Grosso, G.; Mistretta, A.; Marventano, S.; Purrello, A.; Vitaglione, P.; Calabrese, G.; Drago, F.; Galvano, F. Beneficial effects of the Mediterranean diet on metabolic syndrome. Curr. Pharm. Des. 2014, 20, 5039–5044. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 12. [Google Scholar] [CrossRef] [PubMed]
- Franquesa, M.; Pujol-Busquets, G.; Garcia-Fernandez, E.; Rico, L.; Shamirian-Pulido, L.; Aguilar-Martinez, A.; Medina, F.X.; Serra-Majem, L.; Bach-Faig, A. Mediterranean diet and cardiodiabesity: A systematic review through evidence-based answers to key clinical questions. Nutrients 2019, 11, 655. [Google Scholar] [CrossRef] [PubMed]
- Santulli, G. Dietary components and metabolic dysfunction: Translating preclinical studies into clinical practice. Nutrients. 2016, 8, 632. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Mittendorfer, B.; Klein, S. Metabolically healthy obesity: Facts and fantasies. J. Clin. Investig. 2019, 129, 3978–3989. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Hernandez-Rubio, J.; Perez-Mesa, J.C.; Piedra-Munoz, L.; Galdeano-Gomez, E. Determinants of Food Safety Level in Fruit and Vegetable Wholesalers’ Supply Chain: Evidence from Spain and France. Int. J. Environ. Res. Public Health 2018, 15, 2246. [Google Scholar] [CrossRef]
- Pettinger, C.; Holdsworth, M.; Gerber, M. ‘All under one roof?’ differences in food availability and shopping patterns in Southern France and Central England. Eur. J. Public Health 2008, 18, 109–114. [Google Scholar] [CrossRef]
- Wible, B.; Mervis, J.; Wigginton, N.S. The global supply chain. Rethinking the global supply chain. Introduction. Science 2014, 344, 1100–1103. [Google Scholar] [CrossRef]
- Gregorio, M.J.; Rodrigues, A.M.; Graca, P.; de Sousa, R.D.; Dias, S.S.; Branco, J.C.; Canhao, H. Food insecurity is associated with low adherence to the Mediterranean diet and adverse health conditions in Portuguese adults. Front. Public Health 2018, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Persichillo, M.; Zito, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Decline of the Mediterranean diet at a time of economic crisis. Results from the Moli-sani study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Agnoli, C.; Sieri, S.; Ricceri, F.; Giraudo, M.T.; Masala, G.; Assedi, M.; Panico, S.; Mattiello, A.; Tumino, R.; Giurdanella, M.C.; et al. Adherence to a Mediterranean diet and long-term changes in weight and waist circumference in the EPIC-Italy cohort. Nutr. Diabetes 2018, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.I.; Dardavessis, T.; Chourdakis, M. Food insecurity and Mediterranean diet adherence among Greek university students. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Pascale, A.V.; Finelli, R.; Giannotti, R.; Visco, V.; Fabbricatore, D.; Matula, I.; Mazzeo, P.; Ragosa, N.; Massari, A.; Izzo, R.; et al. Vitamin D, parathyroid hormone and cardiovascular risk: The good, the bad and the ugly. J. Cardiovasc. Med. (Hagerstown) 2018, 19, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Gambardella, J.; Sardu, C.; Sacra, C.; Del Giudice, C.; Santulli, G. Quit smoking to outsmart atherogenesis: Molecular mechanisms underlying clinical evidence. Atherosclerosis 2017, 257, 242–245. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. The choice of methods in determining the optimal cut-off value for quantitative diagnostic test evaluation. Stat. Methods Med. Res. 2018, 27, 2374–2383. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Haffner, S.M.; Kennedy, E.; Gonzalez, C.; Stern, M.P.; Miettinen, H. A prospective analysis of the HOMA model. The Mexico City Diabetes Study. Diabetes Care 1996, 19, 1138–1141. [Google Scholar] [CrossRef] [PubMed]
- Caserta, C.A.; Mele, A.; Surace, P.; Ferrigno, L.; Amante, A.; Messineo, A.; Vacalebre, C.; Amato, F.; Baldassarre, D.; Amato, M.; et al. Association of non-alcoholic fatty liver disease and cardiometabolic risk factors with early atherosclerosis in an adult population in Southern Italy. Ann. Ist. Super Sanita 2017, 53, 77–81. [Google Scholar] [PubMed]
- Ruggiero, E.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; Bracone, F.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M.; et al. Socioeconomic and psychosocial determinants of adherence to the Mediterranean diet in a general adult Italian population. Eur. J. Public Health 2019, 29, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef]
- Cruz, J.A. Dietary habits and nutritional status in adolescents over Europe—Southern Europe. Eur. J. Clin. Nutr. 2000, 54 (Suppl. 1), S29–S35. [Google Scholar] [CrossRef]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef]
- Maiello, M.; Zito, A.; Ciccone, M.M.; Palmiero, P. Metabolic syndrome and its components in postmenopausal women living in Southern Italy, Apulia region. Diabetes Metab. Syndr. 2017, 11, 43–46. [Google Scholar] [CrossRef]
- Martino, F.; Puddu, P.E.; Pannarale, G.; Colantoni, C.; Zanoni, C.; Martino, E.; Barilla, F. Metabolic syndrome among children and adolescents from Southern Italy: Contribution from the Calabrian Sierras Community Study (CSCS). Int. J. Cardiol. 2014, 177, 455–460. [Google Scholar] [CrossRef]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef]
- Cobb, L.K.; Appel, L.J.; Franco, M.; Jones-Smith, J.C.; Nur, A.; Anderson, C.A. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity 2015, 23, 1331–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamb, K.E.; Thornton, L.E.; Olstad, D.L.; Cerin, E.; Ball, K. Associations between major chain fast-food outlet availability and change in body mass index: A longitudinal observational study of women from Victoria, Australia. BMJ Open 2017, 7, e016594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, J.H.; Neckerman, K.; Lovasi, G.S.; Konty, K.; Quinn, J.; Arno, P.; Viola, D.; Harris, T.G.; Weiss, C.C.; Bader, M.D.; et al. Neighbourhood food environments and body mass index among New York City adults. J. Epidemiol. Community Health 2013, 67, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitt, E.; Gallegos, D.; Comans, T.; Cameron, C.; Thornton, L. Exploring the influence of local food environments on food behaviours: A systematic review of qualitative literature. Public Health Nutr. 2017, 20, 2393–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibiloni, M.D.M.; Bouzas, C.; Abbate, M.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Zomeno, M.D.; Vioque, J.; Romaguera, D.; Martinez, J.A.; et al. Nutrient adequacy and diet quality in a Mediterranean population with metabolic syndrome: A cross-sectional study. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Julibert, A.; Bibiloni, M.D.M.; Bouzas, C.; Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Corella, D.; Zomeno, M.D.; Romaguera, D.; Vioque, J.; Alonso-Gomez, A.M.; et al. Total and Subtypes of Dietary Fat Intake and Its Association with Components of the Metabolic Syndrome in a Mediterranean Population at High Cardiovascular Risk. Nutrients 2019, 11, 1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scuteri, A.; Laurent, S.; Cucca, F.; Cockcroft, J.; Cunha, P.G.; Manas, L.R.; Mattace Raso, F.U.; Muiesan, M.L.; Ryliskyte, L.; Rietzschel, E.; et al. Metabolic syndrome across Europe: Different clusters of risk factors. Eur. J. Prev. Cardiol. 2015, 22, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Lacatusu, C.M.; Grigorescu, E.D.; Floria, M.; Onofriescu, A.; Mihai, B.M. The Mediterranean Diet: From an Environment-Driven Food Culture to an Emerging Medical Prescription. Int. J. Environ. Res. Public Health 2019, 16, 942. [Google Scholar] [CrossRef] [Green Version]
- Salas-Salvado, J.; Diaz-Lopez, A.; Ruiz-Canela, M.; Basora, J.; Fito, M.; Corella, D.; Serra-Majem, L.; Warnberg, J.; Romaguera, D.; Estruch, R.; et al. Effect of a Lifestyle Intervention Program With Energy-Restricted Mediterranean Diet and Exercise on Weight Loss and Cardiovascular Risk Factors: One-Year Results of the PREDIMED-Plus Trial. Diabetes Care 2019, 42, 777–788. [Google Scholar] [CrossRef] [Green Version]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total | LSC | SSC | p | |
|---|---|---|---|---|
| N | 407 | 178 | 229 | - |
| Age (years) | 55.9 ± 0.58 | 56.4 ± 0.8 | 55.52 ± 0.8 | 0.422 |
| Sex (M, %) | 59 | 60 | 58 | 0.765 |
| Weight (Kg) | 73.8 ± 0.82 | 72.2 ± 1.2 | 75.1 ± 1.08 | 0.085 |
| Height (cm) | 163.7 ± 0.6 | 164.2 ± 0.6 | 163.3 ± 0.91 | 0.399 |
| Waist (cm) | 96.3 ± 0.74 | 96.4 ± 0.84 | 96,0 ± 1.49 | 0.803 |
| BMI (Kg/m2) | 27.6 ± 0.25 | 27.1 ± 0.39 | 27.9 ± 0.34 | 0.098 |
| SBP (mmHg) | 130.6 ± 0.9 | 131.2 ± 1.3 | 130.1 ± 1.2 | 0.523 |
| DBP (mmHg) | 79.8 ± 0.5 | 80.5 ± 0.8 | 79.2 ± 0.69 | 0.220 |
| HR (bpm) | 72.2 ± 0.6 | 72.1 ± 0.8 | 72.28 ± 0.82 | 0.877 |
| Fasting Glucose (mg/dl) | 84.4 ± 1.2 | 91.28 ± 1.7 | 79.41 ± 1.5 | 0.001 |
| Serum Insulin (μU/dl) | 17.7 ± 0.97 | 21.4 ± 1.7 | 14.9 ± 1.1 | 0.001 |
| Creatinine (mg/dl) | 0.85 ± 0.02 | 0.88 ± 0.05 | 0.82 ± 0.01 | 0.19 |
| Current Smokers (%) | 32.0 | 30.0 | 34.0 | 0.427 |
| Cholesterol (Total, mg/dl) | 201.4 ± 1.9 | 201.36 ± 3.2 | 201.48 ± 2.5 | 0.977 |
| Cholesterol (HDL, mg/dl) | 59.3 ± 0.7 | 59.03 ± 1.2 | 59.56 ± 1.0 | 0.737 |
| Cholesterol (LDL, mg/dl) | 124.6 ± 2.1 | 127.02 ± 3.9 | 123.43 ± 2.4 | 0.418 |
| TG (mg/dl) | 121.7 ± 3.6 | 136.14 ± 5.9 | 110.95 ± 4.3 | 0.001 |
| Metabolic Syndrome (%) | 24.81 | 31.46 | 19.65 | 0.007 |
| Trichopoulous Score | 4.98 ± 0.08 | 4.86 ± 0.13 | 5.08 ± 0.10 | 0.180 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santulli, G.; Pascale, V.; Finelli, R.; Visco, V.; Giannotti, R.; Massari, A.; Morisco, C.; Ciccarelli, M.; Illario, M.; Iaccarino, G.; et al. We are What We Eat: Impact of Food from Short Supply Chain on Metabolic Syndrome. J. Clin. Med. 2019, 8, 2061. https://doi.org/10.3390/jcm8122061
Santulli G, Pascale V, Finelli R, Visco V, Giannotti R, Massari A, Morisco C, Ciccarelli M, Illario M, Iaccarino G, et al. We are What We Eat: Impact of Food from Short Supply Chain on Metabolic Syndrome. Journal of Clinical Medicine. 2019; 8(12):2061. https://doi.org/10.3390/jcm8122061
Chicago/Turabian StyleSantulli, Gaetano, Valeria Pascale, Rosa Finelli, Valeria Visco, Rocco Giannotti, Angelo Massari, Carmine Morisco, Michele Ciccarelli, Maddalena Illario, Guido Iaccarino, and et al. 2019. "We are What We Eat: Impact of Food from Short Supply Chain on Metabolic Syndrome" Journal of Clinical Medicine 8, no. 12: 2061. https://doi.org/10.3390/jcm8122061