A Systematic Review and Meta-Analysis of Within-Person Changes in Cardiac Vagal Activity across the Menstrual Cycle: Implications for Female Health and Future Studies

 , ,
, ,
Abstract
:1. Introduction
2. Methods
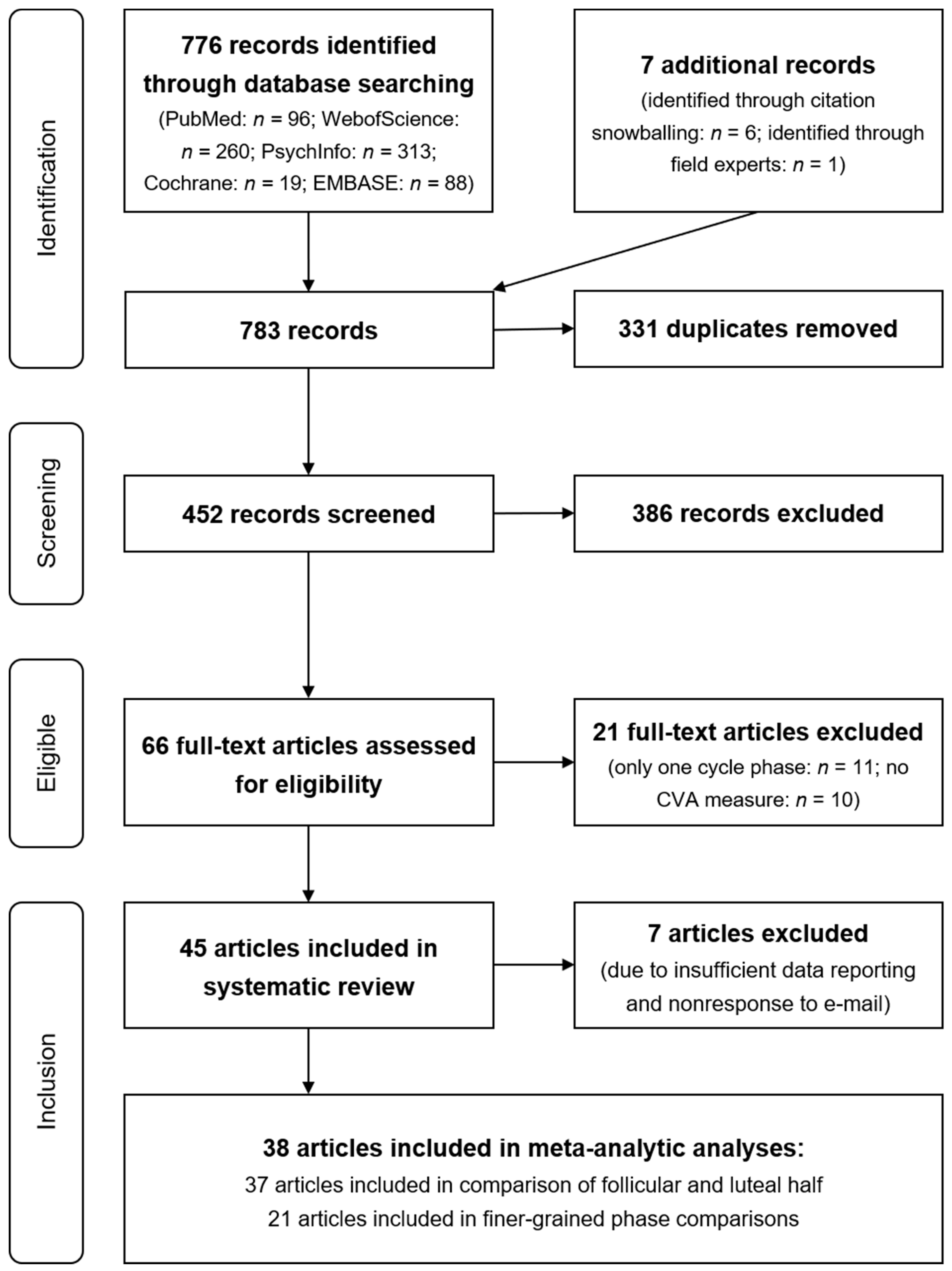
2.1. Literature Search and Screening Criteria
2.2. Study Selection
2.3. Data Extraction
2.4. Cycle Phase Reclassification
2.5. Identification of Studies with Precise Cycle Phase Determination
3. Results
3.1. Study Characteristics
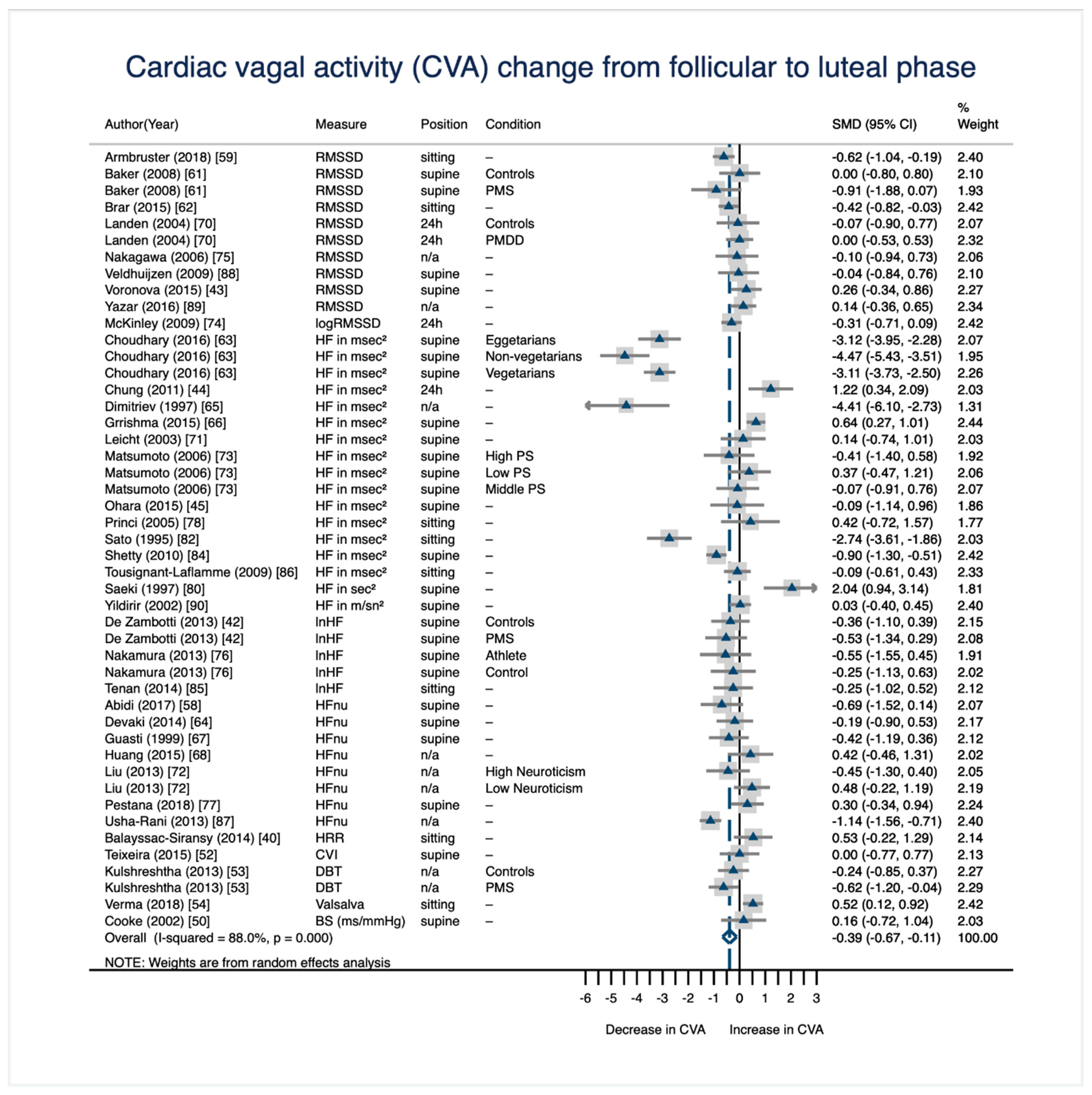
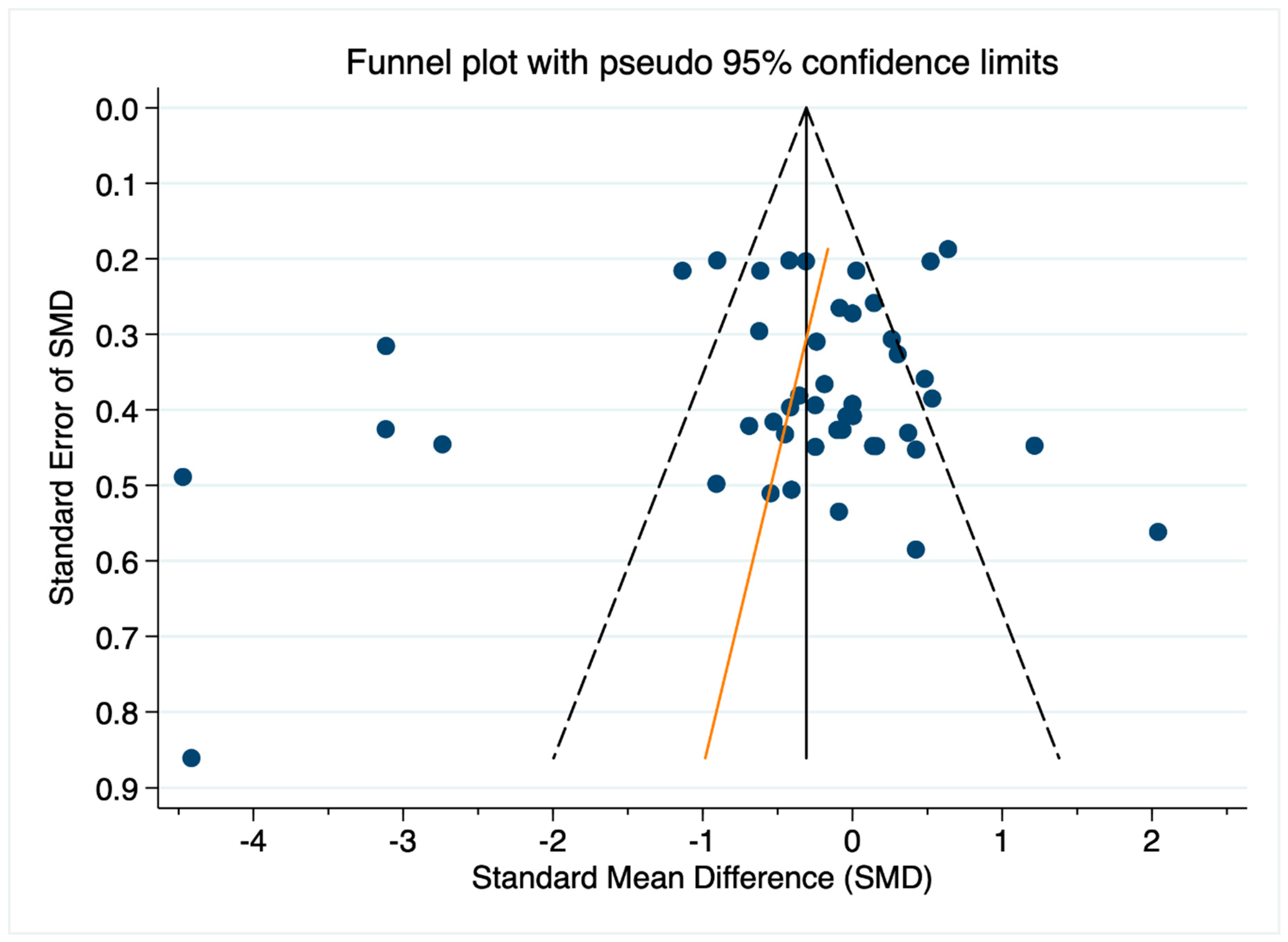
3.2. CVA Change from the Follicular Phase to the Luteal Phase
3.3. CVA Change in Finer-Grained Cycle Phase Comparisons
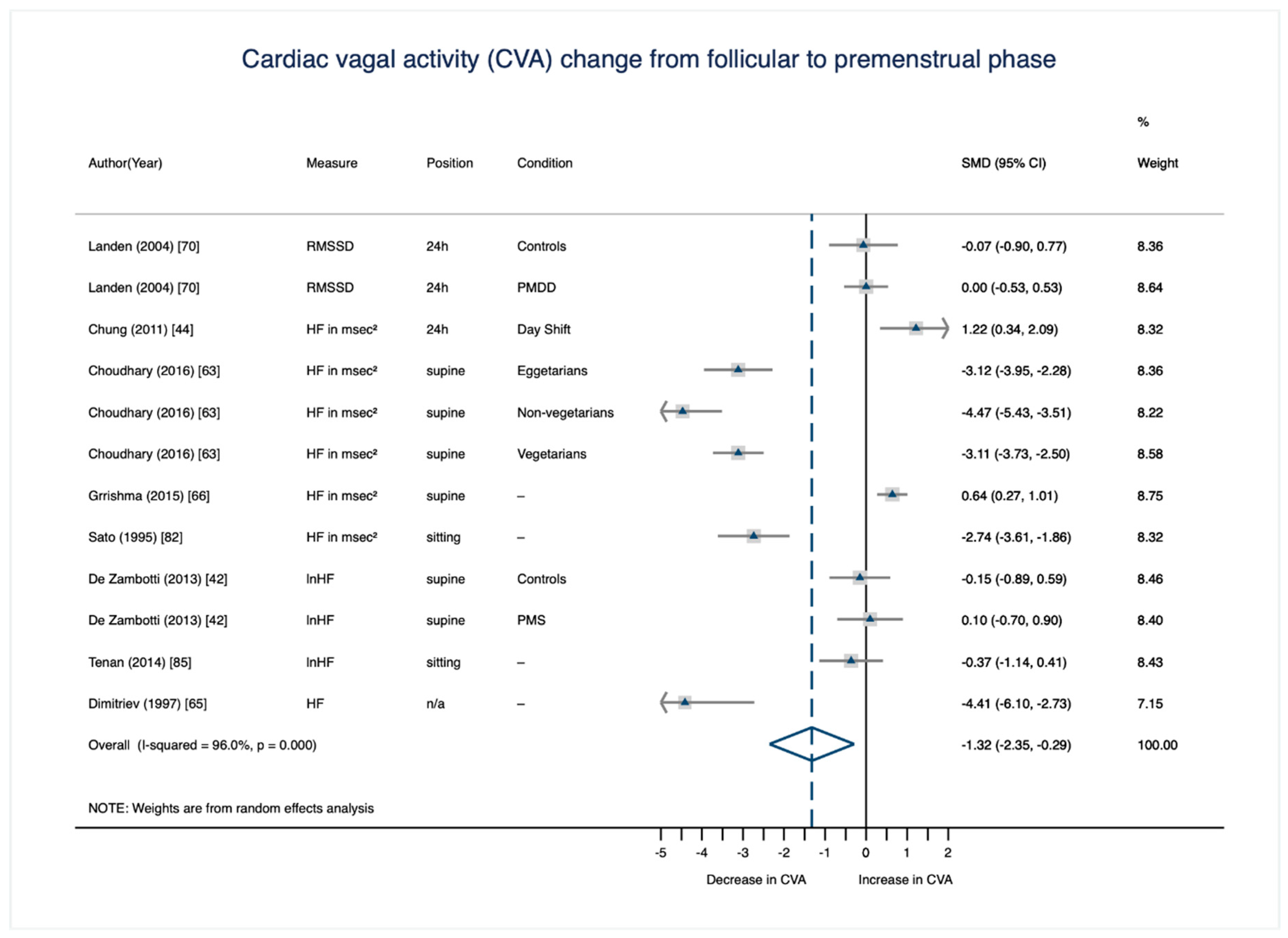
3.3.1. CVA Change from the Mid-To-Late Follicular to the Premenstrual Phase
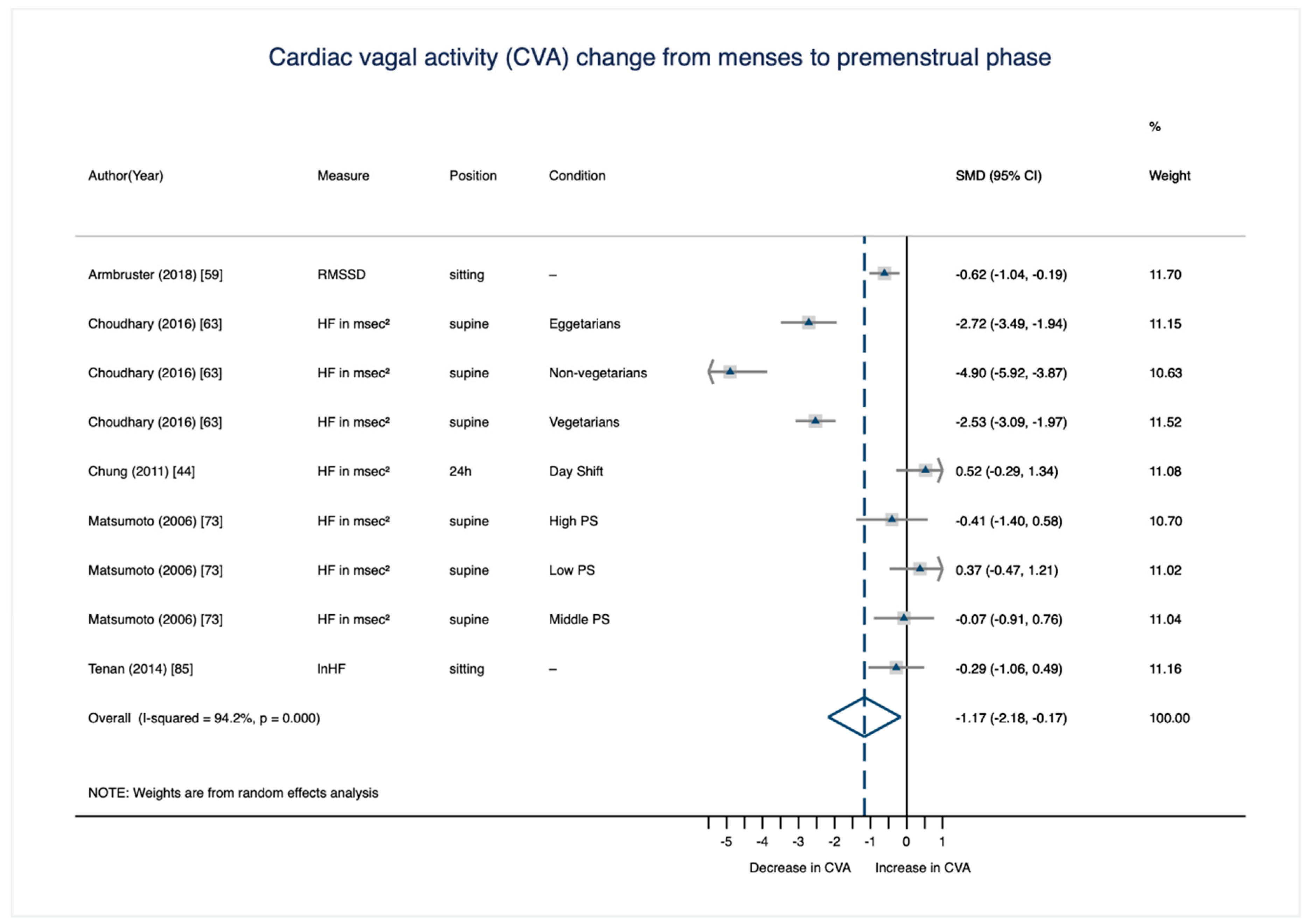
3.3.2. CVA Change from the Menstrual to the Premenstrual Phase
4. Discussion
4.1. Potential Moderators and Mediators
4.2. Underlying Mechanisms
4.3. Limitations
5. Conclusions and Recommendations
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Search terms (period until 26 October 2018)
- PubMed(“Menstrual Cycle”[Mesh] OR “Estradiol”[Mesh] OR “Progesterone”[Mesh] OR “Testosterone”[Mesh]) AND(“HRV”[tiab] OR “Heart Rate Variability”[tiab] OR “Heart Rate Variabilities”[tiab] OR “Heart Period Variability”[tiab] OR “Heart Period Variabilities”[tiab] OR “Cardiac Autonomic Activity”[tiab] OR “Cardiac Autonomic Control”[tiab] OR “Cardiac Electrophysiology”[tiab] OR “Cardiac Reactivity”[tiab] OR “Cardiac Vagal Control”[tiab] OR “Autonomic Nervous System Activity”[tiab] OR “Parasympathetic Nervous System Activity”[tiab] OR “Vagal Tone”[tiab] OR “Vagal Activity”[tiab] OR “Vagal Reactivity”[tiab] OR “Cardiac Electrophysiology”[Mesh] OR “Vagus Nerve/physiology”[Mesh]) AND(“Humans”[MeSH])
- WebOfScienceTS = (((“Menstrual Cycle”) OR (“Luteal Phase”) OR (“Follicular Phase”) OR (“Ovarian Hormones”) OR (“Gonadal Hormones”) OR (“Gonadal Sex Hormones”) OR (“Sex Hormones”) OR (“Sex Steroids”) OR(“Estrogen”) OR (“Estradiol”) OR (“Progesterone”) OR (“Testosterone”)) AND((“HRV”) OR (“Heart Rate Variability”) OR (“Heart Rate Variabilities”) OR (“Heart Period Variability”) OR (“Heart Period Variabilities”) OR (“Cardiac Autonomic Activity”) OR (“Cardiac Autonomic Control”) OR (“Cardiac Electrophysiology”) OR (“Cardiac Reactivity”) OR (“Cardiac Vagal Control”) OR (“Autonomic Nervous System Activity”) OR (“Parasympathetic Nervous System Activity”) OR (“Vagal Tone”) OR (“Vagal Activity”) OR (“Vagal Reactivity”)))Delimiters: Publication Years Timespan = All Years. Databases = SCI-EXPANDED, SSCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, CCR-EXPANDED, IC. Search language = Auto.
- PsychInfo(SU “Menstrual Cycle” OR SU “Luteal Phase” OR SU “Follicular Phase” OR “Ovarian Hormones” OR “Gonadal Hormones” OR “Gonadal Sex Hormones” OR “Sex Hormones” OR “Sex Steroids” OR “Estrogen” OR “Estradiol” OR “Progesterone” OR “Testosterone”) AND(SU “HRV” OR SU “Heart Rate Variability” OR SU “Heart Rate Variabilities” OR SU “Heart Period Variability” OR SU “Heart Period Variabilities” OR SU “Cardiac Autonomic Activity” OR SU “Cardiac Autonomic Control” OR SU “Cardiac Electrophysiology” OR SU “Cardiac Reactivity” OR SU “Cardiac Vagal Control” OR SU “Autonomic Nervous System Activity” OR SU “Parasympathetic Nervous System Activity” OR SU “Vagal Tone” OR SU “Vagal Activity” OR SU “Vagal Reactivity” OR SU “Vagus Nerve” OR SU “Parasympathetic Nervous System” OR SU “Sympathetic Nervous System”)Population Group: Human; Exclude MEDLINE records; Population Group: Human AND Apply equivalent subjects; Apply related words; Also search within the full text of the articles on 2016-07-22 07:20 AM”
- Cochrane#1 (MeSH descriptor: [Menstrual Cycle] explode all trees); #2 (MeSH descriptor: [Estradiol] explode all trees); #3 (MeSH descriptor: Progesterone] explode all trees); #4 (MeSH descriptor: [Testosterone] explode all trees); #5 (“HRV” OR “Heart Rate Variability” OR “Heart Rate Variabilities” OR “Heart Period Variability” OR “Cardiac Autonomic Activity” OR “Cardiac Autonomic Control” OR “Cardiac Electrophysiology” OR “Cardiac Reactivity” OR “Cardiac Vagal Control” OR “Autonomic Nervous System Activity” OR “Parasympathetic Nervous System Activity” OR “Vagal Tone” OR “Vagal Activity” OR “Vagal Reactivity”: ti, ab, kw (Word variations have been searched)); #6 ((#1 or #2 or #3 oe #4) and #5)
- EMBASE(‘Menstrual Cycle’/mj OR ‘Luteal Phase’/mj OR ‘Follicular Phase’/mj OR ‘Ovarian Hormones’ OR ‘Gonadal Hormones’/mj OR ‘Gonadal Sex Hormones’ OR ‘Sex Hormones’/mj OR ‘Sex Steroids’ OR ‘Estrogen’/mj OR ‘Estradiol’/mj OR ‘Progesterone’/mj OR ‘Testosterone’/mj) AND(‘HRV’ OR ‘Heart Rate Variability’/mj OR ‘Heart Rate Variabilities’ OR ‘Heart Period Variability’ OR ‘Heart Period Variabilities’ OR ‘Cardiac Autonomic Activity’ OR ‘Cardiac Autonomic Control’ OR ‘Cardiac Electrophysiology’/mj OR ‘Cardiac Reactivity’ OR ‘Cardiac Vagal Control’ OR ‘Autonomic Nervous System Activity’ OR ‘Parasympathetic Nervous System Activity’ OR ‘Vagal Tone’/mj OR ‘Vagal Activity’/mj OR ‘Vagal Reactivity’ OR ‘Vagus Nerve’/mj OR ‘Parasympathetic Nervous System’/mj OR ‘Sympathetic Nervous System’/mj) AND([Article]/lim OR [Article In Press]/lim OR [Editorial]/lim OR [Erratum]/lim OR [Letter]/lim OR [Note]/lim OR [Review]/lim OR [Short Survey]/lim) AND([Adolescent]/lim OR [Young Adult]/lim OR [Adult]/lim) AND[Embase]/lim
References
- Beauchaine, T.P.; Thayer, J.F. Heart rate variability as a transdiagnostic biomarker of psychopathology. Int. J. Psychophysiol. 2015, 98, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Balzarotti, S.; Biassoni, F.; Colombo, B.; Ciceri, M.R. Cardiac vagal control as a marker of emotion regulation in healthy adults: A review. Biol. Psychol. 2017, 130, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Lane, R.D. A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 2000, 61, 201–216. [Google Scholar] [CrossRef]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart rate variability, prefrontal neural function, and cognitive performance: The neurovisceral integration perspective on self-regulation, adaptation, and health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Geisler, F.C.; Kubiak, T.; Siewert, K.; Weber, H. Cardiac vagal tone is associated with social engagement and self-regulation. Biol. Psychol. 2013, 93, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.A.; Heathers, J.A.; Abbott, M.J.; Kemp, A.H.; Quintana, D.S. Worry is associated with robust reductions in heart rate variability: A transdiagnostic study of anxiety psychopathology. BMC Psychol. 2016, 4, 32. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Quintana, D.S. The relationship between mental and physical health: Insights from the study of heart rate variability. Int. J. Psychophysiol. 2013, 89, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Kemp, A.H.; Beauchaine, T.P.; Thayer, J.F.; Kaess, M. Depression and resting state heart rate variability in children and adolescents—A systematic review and meta-analysis. Clin. Psychol. Rev. 2016, 46, 136–150. [Google Scholar] [CrossRef] [PubMed]
- Sgoifo, A.; Carnevali, L.; Pico Alfonso, M.A.; Amore, M. Autonomic dysfunction and heart rate variability in depression. Stress 2015, 18, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Aguilar-Raab, C.; Koenig, J.; Kaess, M.; Borniger, J.C.; Nelson, R.J.; Hall, M.; Ditzen, B.; Thayer, J.F.; Fischer, J.E. The heart’s rhythm‘n’blues: Sex differences in circadian variation patterns of vagal activity vary by depressive symptoms in predominantly healthy employees. Chronobiol. Int. 2018, 35, 896–909. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Lane, R.D. Claude Bernard and the heart–brain connection: Further elaboration of a model of neurovisceral integration. Neurosci. Biobehav. Rev. 2009, 33, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Pavlov, V.A.; Chavan, S.S.; Tracey, K.J. Molecular and functional neuroscience in immunity. Ann. Rev. Immunol. 2018, 36, 783–812. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Koenig, J.; Li, J.; Mauss, D.; Hoffmann, K.; Schmidt, B.; Fischer, J.E.; Thayer, J.F. The association of work stress and glycemic status is partially mediated by autonomic nervous system function: Cross-sectional results from the Mannheim Industrial cohort study (MICS). PLoS ONE 2016, 11, e0160743. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.K.; Fischer, J.E.; Thayer, J.F.; Mauss, D.; Jarczok, M.N. Decreased heart rate variability correlates to increased cardiovascular risk. Int. J. Cardiol. 2016, 203, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Pavlov, V.A.; Tracey, K.J. The vagus nerve and the inflammatory reflex-linking immunity and metabolism. Nat. Rev. Endocrinol. 2012, 8, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.D.; Khasar, S.G.; Green, P.G. Neurogenic inflammation and arthritis. Ann. N.Y. Acad. Sci. 2006, 1069, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Van Rensburg, D.C.; Ker, J.A.; Grant, C.C.; Fletcher, L. Autonomic impairment in rheumatoid arthritis. Int. J. Rheum. Dis. 2012, 15, 419–426. [Google Scholar] [CrossRef] [PubMed]
- De Couck, M.; Caers, R.; Spiegel, D.; Gidron, Y. The role of the vagus nerve in cancer prognosis: A systematic and a comprehensive review. J. Oncol. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Woody, M.L.; McGeary, J.E.; Gibb, B.E. Brooding rumination and heart rate variability in women at high and low risk for depression: Group differences and moderation by COMT genotype. J. Abnorm. Psychol. 2014, 123, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laederach-Hofmann, K.; Mussgay, L.; Ruddel, H. Autonomic cardiovascular regulation in obesity. J. Endocrinol. 2000, 164, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, J.; Jarczok, M.N.; Fischer, J.E.; Thayer, J.F. The association of (effective and ineffective) analgesic intake, pain interference and heart rate variability in a cross-sectional occupational sample. Pain Med. 2015, 16, 2261–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanowicz, M.; Schmidt, J.E.; Bostwick, J.M.; Mrazek, D.A.; Karpyak, V.M. Changes in heart rate variability associated with acute alcohol consumption: Current knowledge and implications for practice and research. Alcohol Clin. Exp. Res. 2011, 35, 1092–1105. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Jarczok, M.N.; Kuhn, W.; Morsch, K.; Schäfer, A.; Hillecke, T.K.; Thayer, J.F. Impact of caffeine on heart rate variability: A systematic review. J. Caffeine Res. 2013, 3, 22–37. [Google Scholar] [CrossRef]
- Koenig, J.; Menke, B.; Hillecke, T.K.; Thayer, J.F.; Jarczok, M.N. Heart rate variability and cocaine: A systematic review of human studies. Arch. Neurosci. 2015, 2, e60035. [Google Scholar] [CrossRef] [Green Version]
- Koenig, J.; Jarczok, M.N.; Wasner, M.; Hillecke, T.K.; Thayer, J.F. Heart rate variability and swimming. Sports Med. 2014, 44, 1377–1391. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Jarczok, M.; Mauss, D.; Koenig, J.; Li, J.; Herr, R.M.; Thayer, J.F. Autonomic nervous system activity and workplace stressors—A systematic review. Neurosci. Biobehav. Rev. 2013, 37, 1810–1823. [Google Scholar] [CrossRef] [PubMed]
- Bilan, A.; Witczak, A.; Palusiński, R.; Myśliński, W.; Hanzlik, J. Circadian rhythm of spectral indices of heart rate variability in healthy subjects. J. Electrocardiol. 2005, 38, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, J.J.; Le, F.K.; Lahiri, M.; Kannankeril, P.J.; Ng, J.; Kadish, A.H. Assessment of parasympathetic reactivation after exercise. Am. J. Physiol Heart Circ. Physiol 2006, 290, H2446–H2452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaikkonen, P.; Nummela, A.; Rusko, H. Heart rate variability dynamics during early recovery after different endurance exercises. Eur. J. Appl. Physiol. 2007, 102, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, R.; Melillo, P.; Bracale, U.; Caserta, M.; Triassi, M.; Pecchia, L. Acute mental stress assessment via short term HRV analysis in healthy adults: A systematic review with meta-analysis. Biomed. Signal Proces. Control 2015, 18, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Mihm, M.; Gangooly, S.; Muttukrishna, S. The normal menstrual cycle in women. Anim. Reprod. Sci. 2011, 124, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Lenton, E.A.; Landgren, B.M.; Sexton, L. Normal variation in the length of the luteal phase of the menstrual cycle: Identification of the short luteal phase. BJOG Int. J. Obstet. Gynaecol. 1984, 91, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Sundström Poromaa, I.; Gingnell, M. Menstrual cycle influence on cognitive function and emotion processing—From a reproductive perspective. Front. Neurosci. 2014, 8, 380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinton, R.D.; Thompson, R.F.; Foy, M.R.; Baudry, M.; Wang, J.; Finch, C.E.; Morgan, T.E.; Pike, C.J.; Mack, W.J.; Stanczyk, F.Z.; et al. Progesterone receptors: Form and function in brain. Front. Neuroendocrinol. 2008, 29, 313–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruber, C.J.; Tschugguel, W.; Schneeberger, C.; Huber, J.C. Production and actions of estrogens. N. Engl. J. Med. 2002, 346, 340–352. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, E.; D’Esposito, M. Estrogen shapes dopamine-dependent cognitive processes: Implications for women’s health. J. Neurosci. 2011, 31, 5286–5293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balayssac-Siransy, E.; Ouattara, S.; Adoubi, A.; Kouame, A.; Sall, F.; Bogui, R. Effects of menstrual cycle on vagal reactivation in post-exercise recovery among young black African women. Sci. Sport 2014, 29, 196–202. [Google Scholar] [CrossRef]
- Lahiri, M.K.; Kannankeril, P.J.; Goldberger, J.J. Assessment of autonomic function in cardiovascular disease: Physiological basis and prognostic implications. J. Am. Coll. Cardiol. 2008, 51, 1725–1733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Zambotti, M.; Nicholas, C.L.; Colrain, I.M.; Trinder, J.A.; Baker, F.C. Autonomic regulation across phases of the menstrual cycle and sleep stages in women with premenstrual syndrome and healthy controls. Psychoneuroendocrinology 2013, 38, 2618–2627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voronova, N.; Meigal, A.Y.; Yelaeva, L.; Kuzmina, G. Heart rate variability in women during various seasons and phases of the menstrual cycle. Ekologiia Cheloveka 2015, 2, 20–26. [Google Scholar]
- Chung, M.-H.; Yang, C.C. Heart rate variability across the menstrual cycle in shift work nurses. J. Exp. Clin. Med. 2011, 3, 121–125. [Google Scholar] [CrossRef]
- Ohara, K.; Okita, Y.; Kouda, K.; Mase, T.; Miyawaki, C.; Nakamura, H. Cardiovascular response to short-term fasting in menstrual phases in young women: An observational study. BMC Womens Health 2015, 15, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research–recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, R.J.; Deeks, J.J.; Altman, D.G.; Bradburn, M.J.; Harbord, R.M.; Sterne, J.A. Metan: Fixed-and random-effects meta-analysis. Stata J. 2008, 8, 3–28. [Google Scholar] [CrossRef] [Green Version]
- Harbord, R.M.; Harris, R.J.; Sterne, J.A. Updated tests for small-study effects in meta-analyses. Stata J. 2009, 9, 197–210. [Google Scholar] [CrossRef]
- Lüthi, M.; Roach, D.E.; Beaudin, A.E.; Debert, C.T.; Sheldon, R.S.; Poulin, M.J. Effects of ovarian hormones and aging on respiratory sinus arrhythmia and breathing patterns in women. Clin. Auton. Res. 2008, 18, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Cooke, W.H.; Ludwig, D.A.; Eckberg, D.L.; Convertino, V.A. Does the menstrual cycle influence the sensitivity of vagally mediated baroreflexes? Clin. Sci. 2002, 102, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Minson, C.T.; Halliwill, J.R.; Young, T.M.; Joyner, M.J. Influence of the menstrual cycle on sympathetic activity, baroreflex sensitivity, and vascular transduction in young women. Circulation 2000, 101, 862–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, A.L.; Ramos, P.S.; Vianna, L.C.; Ricardo, D.R. Effects of ovarian hormones and oral contraceptive pills on cardiac vagal withdrawal at the onset of dynamic exercise. PLoS ONE 2015, 10, e0119626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulshreshtha, M.; Kumar, Y.; Agarwal, V.; Dhama, V. Symathovagal imbalance in premenstrual syndrome. Ind. J. Physiol. Pharmacol. 2013, 57, 443–447. [Google Scholar]
- Verma, S.; Khuraiya, P.; Soni, R. A comparative study of parasympathetic function tests during different phases of menstrual cycle in young healthy females. Int. J. Res. Med. Sci 2018, 6, 1197–1202. [Google Scholar] [CrossRef] [Green Version]
- Edler, C.; Lipson, S.F.; Keel, P.K. Ovarian hormones and binge eating in bulimia nervosa. Psychol. Med. 2007, 37, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Eisenlohr-Moul, T.A.; Schmalenberger, K.M.; Owens, S.A.; Peters, J.R.; Dawson, D.N.; Girdler, S.S. Perimenstrual exacerbation of symptoms in borderline personality disorder: Evidence from multilevel models and the Carolina Premenstrual Assessment Scoring System. Psychol. Med. 2018, 48, 2085–2095. [Google Scholar] [CrossRef] [PubMed]
- Weissman, A.; Lowenstein, L.; Tal, J.; Ohel, G.; Calderon, I.; Lightman, A. Modulation of heart rate variability by estrogen in young women undergoing induction of ovulation. Eur. J. Appl. Physiol. 2009, 105, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Abidi, S.; Nili, M.; Serna, S.; Kim, S.; Hazlett, C.; Edgell, H. Influence of sex, menstrual cycle, and oral contraceptives on cerebrovascular resistance and cardiorespiratory function during Valsalva or standing. J. Appl. Physiol. 2017, 123, 375–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armbruster, D.; Grage, T.; Kirschbaum, C.; Strobel, A. Processing emotions: Effects of menstrual cycle phase and premenstrual symptoms on the startle reflex, facial EMG and heart rate. Behav. Brain Res. 2018, 351, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Li, J.; Zhou, L.; Li, X. Influence of the menstrual cycle on nonlinear properties of heart rate variability in young women. Am. J. Physiol Heart Circ. Physiol 2009, 297, H765–H774. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.C.; Colrain, I.M.; Trinder, J. Reduced parasympathetic activity during sleep in the symptomatic phase of severe premenstrual syndrome. J. Psychosom. Res. 2008, 65, 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brar, T.K.; Singh, K.D.; Kumar, A. Effect of different phases of menstrual cycle on heart rate variability (HRV). J. Clin. Diagn. Res. 2015, 9, CC01–CC04. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, A.K.; Alam, T.; Jiwane, R.; Kishanrao, S.S. A comparative analysis of dietary habits on sensory motor association and heart rate variability during menstrual cycle. J. Clin. Diagn. Res. 2016, 10, CC04–CC08. [Google Scholar] [CrossRef] [PubMed]
- Devaki, P.; Saikumar, P.; Prabhu, K.; Prasannavenkatesh, E.; Kalaiselvi, V. Heartrate variability across different phases menstrual cycle in adolescent females. Res. J. Pharm. Biol. Chem. Sci. 2014, 5, 6. [Google Scholar]
- Dimitriev, D.; Saperova, E.; Dimitriev, A.; Karpenko, I. Features of cardiovascular functioning during different phases of the menstrual cycle. Rossiiskii Fiziologicheskii Zhurnal Imeni IM Sechenova 2007, 93, 300–305. [Google Scholar]
- Grrishma, B.; Gaur, G.; Chaturvedula, L.; Velkumary, S.; Subramanian, S.K.; Gurunandan, U. Assessment of cardiovascular autonomic functions and baroreceptor reactivity in women with premenstrual syndrome. Ind. J. Physiol. Pharmacol. 2015, 59, 148–154. [Google Scholar]
- Guasti, L.; Grimoldi, P.; Mainardi, L.T.; Petrozzino, M.R.; Piantanida, E.; Garganico, D.; Diolisi, A.; Zanotta, D.; Bertolini, A.; Ageno, W.; et al. Autonomic function and baroreflex sensitivity during a normal ovulatory cycle in humans. Acta Cardiol. 1999, 54, 209–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.-C.; Wong, A.M.; Ho, C.-W.; Weng, T.-P.; Cheng, S.-C.; Wang, J.-S. Comparison of cardiac autonomic nervous system disturbed by sleep deprivation in sex and menstrual phase. Chin. J. Physiol. 2015, 58, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Konishi, K.; Kumashiro, M.; Izumi, H.; Higuchi, Y. Effects of the menstrual cycle on working memory: Comparison of postmenstrual and premenstrual phases. Ind. Health 2008, 46, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landén, M.; Wennerblom, B.; Tygesen, H.; Modigh, K.; Sörvik, K.; Ysander, C.; Ekman, A.; Nissbrandt, H.; Olsson, M.; Eriksson, E. Heart rate variability in premenstrual dysphoric disorder. Psychoneuroendocrinology 2004, 29, 733–740. [Google Scholar] [CrossRef]
- Leicht, A.S.; Hirning, D.A.; Allen, G.D. Heart rate variability and endogenous sex hormones during the menstrual cycle in young women. Exp. Physiol. 2003, 88, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; Zhou, R.; Oei, T.P.; Wang, Q.; Zhao, Y.; Liu, Y. Variation in the stress response between high-and low-neuroticism female undergraduates across the menstrual cycle. Stress 2013, 16, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Ushiroyama, T.; Morimura, M.; Moritani, T.; Hayashi, T.; Suzuki, T.; Tatsumi, N. Autonomic nervous system activity in the late luteal phase of eumenorrheic women with premenstrual symptomatology. J. Psychosom. Obst. Gyn. 2006, 27, 131–139. [Google Scholar] [CrossRef] [PubMed]
- McKinley, P.S.; King, A.R.; Shapiro, P.A.; Slavov, I.; Fang, Y.; Chen, I.S.; Jamner, L.D.; Sloan, R.P. The impact of menstrual cycle phase on cardiac autonomic regulation. Psychophysiology 2009, 46, 904–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagawa, M.; Ooie, T.; Takahashi, N.; Taniguchi, Y.; Anan, F.; Yonemochi, H.; Saikawa, T. Influence of menstrual cycle on QT interval dynamics. Pacing Clin. Electrophysiol. 2006, 29, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Hayashi, K.; Aizawa, K.; Mesaki, N.; Kono, I. Effects of regular aerobic exercise on post-exercise vagal reactivation in young female. Eur. J. Sport Sci. 2013, 13, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Pestana, E.R.; Mostarda, C.T.; Silva-Filho, A.C.; Salvador, E.P.; de Carvalho, W.R.G. Effect of different phases of menstrual cycle in heart rate variability of physically active women. Sport Sci. Health 2018, 14, 297–303. [Google Scholar] [CrossRef]
- Princi, T.; Parco, S.; Radillo, O.; De Seta, F.; Ulcigrai, L.; Accardo, A. Heart rate variability and menstrual cycle in eumenorrheic young women. Biomed. Sci. Instrum. 2005, 41, 340–345. [Google Scholar] [PubMed]
- Rawal, K.; Saini, I. Comparative analysis of measuring heart rate variability during different phases of menstrual cycle in young healthy women. Int. J. Inf. Electron. Eng. 2014, 4, 62–64. [Google Scholar] [CrossRef]
- Saeki, Y.; Atogami, F.; Takahashi, K.; Yoshizawa, T. Reflex control of autonomic function induced by posture change during the menstrual cycle. J. Auton. Nerv. Syst. 1997, 66, 69–74. [Google Scholar] [CrossRef]
- Sato, N.; Miyake, S. Cardiovascular reactivity to mental stress: Relationship with menstrual cycle and gender. J. Physiol. Anthropol. Appl. Hum. Sci. 2004, 23, 215–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, N.; Miyake, S.; Akatsu, J.I.; Kumashiro, M. Power spectral analysis of heart rate variability in healthy young women during the normal menstrual cycle. Psychosom. Med. 1995, 57, 331–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seebauer, M.; Frühwirth, M.; Moser, M. Changes of respiratory sinus arrhythmia during the menstrual cycle depend on average heart rate. Eur. J. Appl. Physiol. 2002, 87, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.; Pai, S.R.; Nayanatara, A.; Bhat, M.R.; Shetty, B.A. Comparative study of time and frequency domain analysis of heart rate variability in different phases of menstrual cycle. J. Chin. Clin. Med. 2010, 5, 469–473. [Google Scholar]
- Tenan, M.S.; Brothers, R.M.; Tweedell, A.J.; Hackney, A.C.; Griffin, L. Changes in resting heart rate variability across the menstrual cycle. Psychophysiology 2014, 51, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Tousignant-Laflamme, Y.; Marchand, S. Autonomic reactivity to pain throughout the menstrual cycle in healthy women. Clin. Auton. Res. 2009, 19, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Usha Rani, Y.S.; Manjunath, P.; Desai, R.D. Comparative study of heart rate variability, heart rate and blood pressure in different phases of menstrual cycle in healthy young women aged 18–22 years. J. Phys. Pharm. Adv. 2013, 3, 188–192. [Google Scholar]
- Veldhuijzen van Zanten, J.J.; Carroll, D.; Ring, C. Mental stress-induced haemoconcentration in women: Effects of menstrual cycle phase. Br. J. Health Psychol. 2009, 14, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Yazar, Ş. Impact of menstrual cycle on cardiac autonomic function assessed by heart rate variability and heart rate recovery. Med. Prin. Pract. 2016, 25, 374–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yildirir, A.; Kabakci, G.; Akgul, E.; Tokgozoglu, L.; Oto, A. Effects of menstrual cycle on cardiac autonomic innervation as assessed by heart rate variability. Ann. Noninvasive Electrocardiol. 2001, 7, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Approximate power and sample size determination for common one-sample and two-sample hypothesis tests. Educ. Psychol. Meas. 1970, 30, 811–831. [Google Scholar] [CrossRef]
- Egger, M.G.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Schmidt, P.J.; Nieman, L.K.; Danaceau, M.A.; Adams, L.F.; Rubinow, D.R. Differential behavioral effects of gonadal steroids in women with and in those without premenstrual syndrome. N. Engl. J. Med. 1998, 338, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Koenig, J.; Thayer, J.F. From psychological moments to mortality: A multidisciplinary synthesis on heart rate variability spanning the continuum of time. Neurosci. Biobehav. Rev. 2017, 83, 547–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thayer, J.F.; Åhs, F.; Fredrikson, M.; Sollers, J.J., III; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Dubey, N.; Hoffman, J.F.; Schuebel, K.; Yuan, Q.; Martinez, P.E.; Nieman, L.K.; Rubinow, D.R.; Schmidt, P.J.; Goldman, D. The ESC/E (Z) complex, an effector of response to ovarian steroids, manifests an intrinsic difference in cells from women with premenstrual dysphoric disorder. Mol. Psychiatry 2017, 22, 1172–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, L.; Straub, R.E.; Roca, C.; Schmidt, P.J.; Shi, K.; Vakkalanka, R.; Weinberger, D.R.; Rubinow, D.R. Risk for premenstrual dysphoric disorder is associated with genetic variation in ESR1, the estrogen receptor α gene. Biol. Psychiatry 2007, 62, 925–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenlohr-Moul, T.A.; Rubinow, D.R.; Schiller, C.E.; Johnson, J.L.; Leserman, J.; Girdler, S.S. Histories of abuse predict stronger within-person covariation of ovarian steroids and mood symptoms in women with menstrually related mood disorder. Psychoneuroendocrinology 2016, 67, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girdler, S.S.; Thompson, K.S.; Light, K.C.; Leserman, J.; Pedersen, C.A.; Prange, A.J., Jr. Historical sexual abuse and current thyroid axis profiles in women with premenstrual dysphoric disorder. Psychosom. Med. 2004, 66, 403–410. [Google Scholar] [PubMed]
- Perkonigg, A.; Yonkers, K.A.; Pfister, H.; Lieb, R.; Wittchen, H.-U. Risk factors for premenstrual dysphoric disorder in a community sample of young women: The role of traumatic events and posttraumatic stress disorder. J. Clin. Psychiatry 2004, 65, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Gollenberg, A.L.; Hediger, M.L.; Mumford, S.L.; Whitcomb, B.W.; Hovey, K.M.; Wactawski-Wende, J.; Schisterman, E.F. Perceived stress and severity of perimenstrual symptoms: The BioCycle Study. J. Womens Health 2010, 19, 959–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahromi, B.N.; Pakmehr, S.; Hagh-Shenas, H. Work stress, premenstrual syndrome and dysphoric disorder: Are there any associations? Iran. Red Crescent Med. J. 2011, 13, 199–202. [Google Scholar]
- Eisenlohr-Moul, T.A.; Girdler, S.S.; Schmalenberger, K.M.; Dawson, D.N.; Surana, P.; Johnson, J.L.; Rubinow, D.R. Toward the reliable diagnosis of DSM-5 premenstrual dysphoric disorder: The Carolina Premenstrual Assessment Scoring System (C-PASS). Am. J. Psychiatry 2017, 174, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salerni, S.; Di Francescomarino, S.; Cadeddu, C.; Acquistapace, F.; Maffei, S.; Gallina, S. The different role of sex hormones on female cardiovascular physiology and function: Not only oestrogens. Eur. J. Clin. Investig. 2015, 45, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Brunton, P.J.; Donadio, M.V.; Yao, S.T.; Greenwood, M.; Seckl, J.R.; Murphy, D.; Russell, J.A. 5α-reduced neurosteroids sex-dependently reverse central prenatal programming of neuroendocrine stress responses in rats. J. Neurosci. 2015, 35, 666–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hut, R.A.; van der Zee, E.A. The cholinergic system, circadian rhythmicity, and time memory. Behav. Brain Res. 2011, 221, 466–480. [Google Scholar] [CrossRef] [PubMed]
- Oikawa, S.; Kai, Y.; Mano, A.; Ohata, H.; Nemoto, T.; Kakinuma, Y. Various regulatory modes for circadian rhythmicity and sexual dimorphism in the non-neuronal cardiac cholinergic system. J. Cardiovas. Transl. Res. 2017, 10, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Riese, H.; Su, S.; Zhu, H.; Dong, Y.; Ding, X.; Thayer, J.F.; Treiber, F.; Snieder, H. A gene-wide association study of heart rate variability at rest and during stress: 8 genes in the parasympathetic pathway. In Abstracts From the 2009 Joint Conference-Nutrition, Physical Activity and Metabolism and 49th Cardiovascular Disease Epidemiology and Prevention, Proceedings of the 2009 Joint Conference-Nutrition, Physical Activity and Metabolism and 49th Cardiovascular Disease Epidemiology and Prevention, Palm Harbor, FL, USA, 11–14 March 2009; American Heart Association: Dallas, TX, USA, 2009. [Google Scholar] [CrossRef] [Green Version]
- Nolte, I.M.; Munoz, M.L.; Tragante, V.; Amare, A.T.; Jansen, R.; Vaez, A.; Von Der Heyde, B.; Avery, C.L.; Bis, J.C.; Dierckx, B.; et al. Genetic loci associated with heart rate variability and their effects on cardiac disease risk. Nat. Commun. 2017, 8, 15805. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Jarczok, M.N.; Warth, M.; Ellis, R.; Bach, C.; Hillecke, T.; Thayer, J.F. Body mass index is related to autonomic nervous system activity as measured by heart rate variability—A replication using short term measurements. J. Nutr. Health Aging 2014, 18, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Windham, B.; Ferrucci, L.; Sonntag, D.; Fischer, J.; Thayer, J.F.; Jarczok, M.N. Association strength of three adiposity measures with autonomic nervous system function in apparently healthy employees. J. Nutr. Health Aging 2015, 19, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.B.; Mitchell, D.; Musey, P.I.; Collins, D.C. The relationship of exercise to anovulatory cycles in female athletes: Hormonal and physical characteristics. Obstet. Gynecol. 1984, 63, 452–456. [Google Scholar] [PubMed]
- Schmalenberger, K.M.; Eisenlohr-Moul, T.A. Studying the menstrual cycle as an independent variable: Practical recommendations and tools for getting started. OSF Preprints 2019. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CVA Measure | Definition |
|---|---|
| RMSSD | Root mean square of successive differences between adjacent R–R intervals in milliseconds or log-transformed values |
| HF | High frequency component in the power spectrum range between 0.15 and 0.4 Hz in milliseconds squared, seconds squared, normalized units, or log-transformed values to the basis of 10 (log) or e (ln) |
| RSA | Respiratory sinus arrhythmia, defined as heart rate variability (HRV) in synchrony with respiration, by which the R–R interval is shortened during inspiration and prolonged during expiration [49]. |
| BS | Baroreflex slope, defined as the resulting changes in R–R intervals from modulated carotid baroreceptor (sequential neck pressure and suction; [50]). |
| CBS | Cardiovagal baroreflex sensitivity, defined as the slope relating R–R interval and systolic blood pressure [51]. |
| CVI | Cardiac vagal index, defined as the ratio of the longest and shortest R–R interval during a 4 s exercise test [52]. |
| HRR | Heart rate (HR) reactivity, defined as the difference between peak HR during 3 min exercise and HR at the first minute post exercise (i.e., recovery; [40]). |
| DBT | Deep breathing test, defined as the difference between the longest and shortest R–R interval while breathing at resonance frequency (6 breath/min; inhale and exhale phase lasting each for 5 s). This can be also described as expiration to inspiration ratio at resonance frequency [53]. |
| Valsalva | Valsalva ratio, defined as the ratio of the maximum R–R interval after strain and the shortest R–R interval during strain. Under the Valsalva maneuver, participants’ nostrils were closed by nose clip and participants were asked to blow by doing forceful expiration into the rubber tube of a mercury sphygmomanometer, raise the mercury column to 40 mm Hg and maintain that level for at least 15 s. HR was recorded continuously during the whole procedure [54]. |
| Menstrual Cycle | Cycle-Day-Based Phase Determination | Ovulation-Based Phase Determination | |||
|---|---|---|---|---|---|
| Menstrual cycle half | Menstrual cycle phase | Forward-count method in cycle days (assuming a 28-day cycle) | Backward-count method in cycle days | LH testing | Basal body temperature |
| Follicular | Menstrual | Day 1 to 7 | |||
| Mid-to-late follicular | Day 8 to 12 | ||||
| Ovulatory | Day 13 to 16 | Day –15 to –12 | Day of and day +1 following positive LH test | Nadir just before temperature rise in the luteal phase and day +1 | |
| Luteal | Early-to-mid luteal | Day 17 to 21 | Day −11 to −8 | Day +2 to +7 following positive LH test | Day +2 to +7 following nadir |
| Premenstrual | Day 22 to 28 | Day −7 to −1 | Day +8 to +14 following positive LH test | Day +8 to +14 following nadir | |
| Names of the Authors (Year of Publication) | Sample Size | Potential Sub-Sampling of Sample of Interest (Between-Person) | Experi-mental Condition (Within-Person) | Cycle Phases Compared | Potential Validation Of Cycle Phase | Measure Indexing CVA | Body Position During CVA Assessment | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Menstrual | Mid-To-Late Follicular | Ovulatory | Early-To-Mid Luteal | Premenstrual | |||||||
| Abidi et al. (2017) [58] | 12 | - | - | “Low hormone”: Day 2–5 | “High hormone”: Day 18–24 | HFnu | Supine | ||||
| Armbruster et al. (2018) [59] | 45 | - | - | “Early follicular”: Day 1–7 | “Late luteal”: Day 6–1 before menstrual onset | Saliva hormone analyses of E2, P4, Testosterone | RMSSD | Sitting | |||
| Bai et al. (2009) [60] | 16 | - | - | “Follicular”: Day = 11.9 ± 1.4; range 10–14 | “Luteal”: Day = 22.0 ± 1.4; range 20–24 | Blood hormone analyses of E2 and P4 | HF in ms2 | Supine | |||
| Baker et al. (2008) [61] | 21 | PMS versus Controls | - | “Mid-follicular” Day 6–12 | “Late-luteal” Day 9–13 after LH-surge | Blood hormone analyses of P4 | RMSSD | Supine | |||
| Balayssac-Siransy et al. (2014) [40] | 14 | - | Active Recovery 3rd min | “Menstrual”: Day = 2.9 ± 0.6; range 1–5 | “Follicular”: Day = 13.0 ± 1.4; 4 days preceding ovulation | “Luteal”: Day = 23.1 “Luteal” 1.4; 6–10 days after ovulation | Blood hormone analyses of E2 and P4 | HRR | Sitting | ||
| Brar et al. (2015) [62] | 50 | - | - | “Menstrual”: Day = 2 | “Proliferative”: Day = 10 | “Secretory”: Day = 21 | RMSSD | Sitting | |||
| Choudhary et al. (2016) [63] | 100 | Eggetarians versus Non-vegetarians versus Vegetarians | - | “Menses”: Day 1–2 | “Follicular”: Day 7–10 | “Luteal”: Day 7–3 days before menstrual onset | HF in ms2 | Supine | |||
| Chung & Yang (2011) [44] | 12 | - | Day Shift | “Menses”: Day 1–2 | “Follicular”: Day 7–10 | “Luteal”: Day 7–3 before menstrual onset | Blood hormone analyses of E2 and P4 | HF in ms2 | 24 h | ||
| Cooke et al. (2002) [50] | 10 | - | - | Day 0–8 | Day 9–14 | Day 15–20 | Day 21–25 | Blood hormone analyses of E2 and P4 | BS | Supine | |
| De Zambotti et al. (2013) [42] | 26 | PMS versus Controls | REM sleep | “Mid-follicular”: Day 6–11 | “Mid-luteal”: Day 5–9 after LH-surge on average 8 ± 2 days before menstrual onset | “Late-luteal”: Day 10–14 after LH-surge on average 3 ± 2 days before menstrual onset | Blood hormone analyses of E2 and P4 | lnHF | Supine | ||
| Devaki et al. (2014) [64] | 15 | - | - | “Menstrual”: Day 1–5 | “Proliferative”: Day 9–12 | “Secretory”: Day 19–22 | HFnu | Supine | |||
| Dimitriev et al. (2007) [65] | 10 | - | - | “Follicular”: Day 7–11 | “Luteal”: Day 7–3 before menstrual onset | HF in ms2 | n/a | ||||
| Grrishma et al. (2015) [66] | 60 | - | - | “Follicular”: Day 8–10 | “Luteal”: Day 5–1 before menstrual onset | HF in ms2 | Supine | ||||
| Guasti et al. (1999) [67] | 13 | - | - | “Follicular” Day 4–6 | “Luteal”: Day 20–26 | HFnu | Supine | ||||
| Huang et al. (2015) [68] | 10 | - | - | “Mid-follicular”: n/a | “Mid-luteal”: n/a | Blood hormone analyses of P4 | HFnu | n/a | |||
| Konishi et al. (2008) [69] | 12 | - | - | “Postmenstrual”: Day 3–7 after cessation of bleeding | “Premenstrual”: Day 10–3 before menstrual onset | HF in ms2 | Seated | ||||
| Kulshreshtha et al. (2013) [53] | 45 | PMS versus Controls | - | “Follicular”: Day = 7 | “Luteal”: Day = 21 | DBT | n/a | ||||
| Landén et al. (2004) [70] | 39 | PMDD versus Controls | - | “Follicular”: Day 6–10 | “Luteal”: Day 5–0 before menstrual onset | RMSSD | 24 h | ||||
| Leicht et al. (2003) [71] | 10 | - | - | “Menses”: Day = 3.8 ± 0.5; range 1–5 | “Ovulation”: Day = 15.8 ± 0.7; range 11–21 | “Luteal”: Day = 22.1 ± 0.4; range 21–24 | Blood hormone analyses of E2 and P4 | HF in ms2 | Supine | ||
| Liu et al. (2013) [72] | 27 | High versus Low Neuroticism | - | “Menstruation”: Day 1–4 | “Ovulation”: Day 11–13 | “Luteal”: Day 21–22 | HFnu | n/a | |||
| Lüthi et al. (2008) [49] | 10 | - | - | “Follicular”: Day 3–6 | “Mid-cycle”: Day of/day after LH-surge | “Luteal”: Day 6–8 after LH-surge | Blood hormone analyses of E2 and P4 | RSA | Seated | ||
| Matsumoto et al. (2006) [73] | 30 | High versus Middle versus Low Premenstrual Symptomatology | - | “Follicular”: Day 1–5 | “Late luteal”: Day 7–1 before menstrual onset | Urinary hormone analyses of E2 and P4 | HF in ms2 | Supine | |||
| McKinley et al. (2009) [74] | 49 | - | - | “Early-to-mid-follicular”: Day 4–10 | “Mid-luteal”: Day 3 after LH-surge–5 days before menstrual onset | logRMSSD | 24 h | ||||
| Minson et al. (2000) [51] | 9 | - | - | “Early follicular”: Day 2–4 | “Midluteal”: Day 8–10 after LH-surge | Blood hormone analyses of E2, P4, LH, follicle stimulating hormone | CBS | Supine | |||
| Nakagawa et al. (2006) [75] | 11 | - | - | “Follicular”: Day = 9.5 ± 0.5; range 7–12 | “Luteal”: Day = 23.2 ± 0.8; range 18–26 | Blood hormone analyses of E2 and P4 | RMSSD | n/a | |||
| Nakamura et al. (2013) [76] | 18 | Athlete versus Control | - | “Early follicular”: Day 4–8 | “Middle luteal”: Day 5–10 after ovulation | lnHF | Supine | ||||
| Ohara et al. (2015) [45] | 7 | - | Eating Trial | “Follicular”: n/a | “Luteal”: n/a | HF in ms2 | Supine | ||||
| Pestana et al. (2018) [77] | 19 | - | - | “Menstrual”: Day 1–9 | “Luteal”: Day 15-day before menstrual onset | HFnu | Supine | ||||
| Princi et al. (2005) [78] | 6 | - | - | “Menstrual”: Day 3“Follicular”: Day 7 | “Luteal”: Day 21 | Blood hormone analyses of E2 and P4 | HF in ms2 | Sitting | |||
| Rawal & Saini (2014) [79] | 20 | - | - | “Menstrual”: n/a | “Follicular”: n/a | “Luteal”: n/a | RMSSD | Supine | |||
| Saeki et al. (1997) [80] | 10 | - | - | “Menstrual”: Day 1–3 | “Follicular”: Period between menstrual and ovulatory phases | “Ovulatory”: Period of 4 days beginning 3 days prior to the day of ovuluation | “Luteal”: Period between ovulatory and premenstrual phases | “Premenstrual”: Days 7–1 before menstrual onset | Blood hormone analyses of E2 and P4 | HF in sec2 | Supine |
| Sato & Miyake (2004) [81] | 14 | - | - | “Follicular”: Day 7–11 | “Luteal”: Days 7–3 before menstrual onset | HF in ms2 | Sitting | ||||
| Sato et al. (1995) [82] | 20 | - | - | “Follicular”: Day 7–10 | “Luteal”: Days 7–3 before menstrual onset | Blood hormone analyses of P4 | HF in ms2 | Sitting | |||
| Seebauer et al. (2002) [83] | 26 | Low versus medium versus high average HR | “Menstruation”: Day 1–4 | “Early follicular”: Remaining days between end of menses and mid-follicular phase “Mid-follicular”: 3 days preceding late follicular phase “Late follicular”: 3 days preceding ovulation phase | “Ovulation”: Positive test result ± 1 day (duration 3 days) | “Early luteal”: 4 days following ovulation phase “Mid-luteal”: 4 days following ovulation phase | “Late-luteal”: Remaining days between end of mid-luteal phase and onset of menses | logRSA | Supine | ||
| Shetty et al. (2010) [84] | 54 | - | - | “Menstrual”: Day 1–5 | “Follicular”: Day 6–14 | “Luteal”: Day 15–28 or menstrual onset | HF in ms2 | Supine | |||
| Teixeira et al. (2015) [52] | 13 | - | - | “Early follicular”: Day = 3.6 ± 1.2; range 1–5 | “Ovulatory”: Day = 14.3 ± 08; range 13–16 | “Mid-luteal”: Day = 21.3 ± 0.8; range 20–24 | Blood hormone analyses of E2 and P4 | CVI | Supine | ||
| Tenan et al. (2014) [85] | 13 | - | - | “Early follicular”: Equally spaced with late follicular phase from menstrual onset until ovulatory phase | “Late follicular”: Equally spaced with early follicular phase from menstrual onset until ovulatory phase | “Ovulatory”: 3-day period | “Midluteal”: Equally spaced with late luteal phase from end of ovulatory phase until menstrual onset | “Late luteal”: Equally spaced with early luteal phase from end of ovulatory phase until menstrual onset | lnHF | Sitting | |
| Tousignant-Laflamme & Marchand (2009) [86] | 29 | - | - | “Menstrual”: Day 1–3 | “Ovulatory”: Day 12–14 | “Luteal”: Day 19–23 | Blood hormone analyses of E2 and P4 | HF in ms2 | Sitting | ||
| Usha Rani et al. (2013) [87] | 50 | - | - | “Menstrual”: Day 1–5 | “Follicular”: Day 6–14 | “Luteal”: Day 15–28 | HFnu | n/a | |||
| Veldhuijzen von Zanten et al. (2009) [88] | 12 | - | - | “Follicular”: Day 4–9 | “Luteal”: Day 19–25 | Blood hormone analyses of E2 and P4 | RMSSD | Supine | |||
| Verma et al. (2018) [54] | 50 | - | - | “Menstrual”: Day 1–5 | “Follicular”: Day 9–12 | “Luteal phase”: Day 19–25 | Valsalva | Sitting | |||
| Voronova et al. (2015) [43] | 21 | - | Spring | “Early follicular”: Day 7 | “Late follicular”: Day 13 “Ovulation”: Day 16 | “Luteal”: Day 24 | RMSSD | Supine | |||
| Weissman et al. (2009) [57] | 14 | “Early follicular”: Day 2–3 | “Preovulatory”: Just before ovulation | Blood hormone analyses of E2 | HFnu | Supine | |||||
| Yazar (2016) [89] | 30 | - | - | “Late follicular”: Day 9–13 | “Mid-luteal”: Day 19–23 | RMSSD | n/a | ||||
| Yildirir et al. (2001) [90] | 43 | - | - | “Follicular”: Day 10–12 | “Luteal”: Day 19–23 | HF in m/sn2 | Supine | ||||
| To From | Mid-To-Late Follicular | Ovulatory | Early-To-Mid Luteal | Premenstrual |
|---|---|---|---|---|
| Menstrual | d = 0.23 95% CI (−0.08, 0.55) nstudies = 10; nindividuals = 349 | d = 0.35 95% CI (−0.45, 1.16) nstudies = 4; nindividuals = 47 | d = 0.28 95% CI (−0.52, 1.08) nstudie; = 4; nindividuals = 86 | d = −1.17 95% CI (−2.18, −0.17) nstudies = 5; nindividuals = 200 |
| Mid-to-late follicular | nstudies = 1; nindividuals = 13 | d = −0.14 95% CI (−0.60, 0.32) nstudies = 3; nindividuals = 53 | d = −1.32 95% CI (−2.35, −0.29) nstudies = 8; nindividuals = 280 | |
| Ovulatory | d = −0.06 95% CI (−0.64, 0.51) nstudies = 2; nindividuals = 23 | nstudies = 1; nindividuals = 13 | ||
| Early-to-mid luteal | d = 0.20 95% CI (−0.25, 0.64) nstudies = 2; nindividuals = 39 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmalenberger, K.M.; Eisenlohr-Moul, T.A.; Würth, L.; Schneider, E.; Thayer, J.F.; Ditzen, B.; Jarczok, M.N. A Systematic Review and Meta-Analysis of Within-Person Changes in Cardiac Vagal Activity across the Menstrual Cycle: Implications for Female Health and Future Studies. J. Clin. Med. 2019, 8, 1946. https://doi.org/10.3390/jcm8111946
Schmalenberger KM, Eisenlohr-Moul TA, Würth L, Schneider E, Thayer JF, Ditzen B, Jarczok MN. A Systematic Review and Meta-Analysis of Within-Person Changes in Cardiac Vagal Activity across the Menstrual Cycle: Implications for Female Health and Future Studies. Journal of Clinical Medicine. 2019; 8(11):1946. https://doi.org/10.3390/jcm8111946
Chicago/Turabian StyleSchmalenberger, Katja M., Tory A. Eisenlohr-Moul, Lena Würth, Ekaterina Schneider, Julian F. Thayer, Beate Ditzen, and Marc N. Jarczok. 2019. "A Systematic Review and Meta-Analysis of Within-Person Changes in Cardiac Vagal Activity across the Menstrual Cycle: Implications for Female Health and Future Studies" Journal of Clinical Medicine 8, no. 11: 1946. https://doi.org/10.3390/jcm8111946