Validation of Liquid Chromatography-Tandem Mass Spectrometry-Based 5-Plex Assay for Mucopolysaccharidoses

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
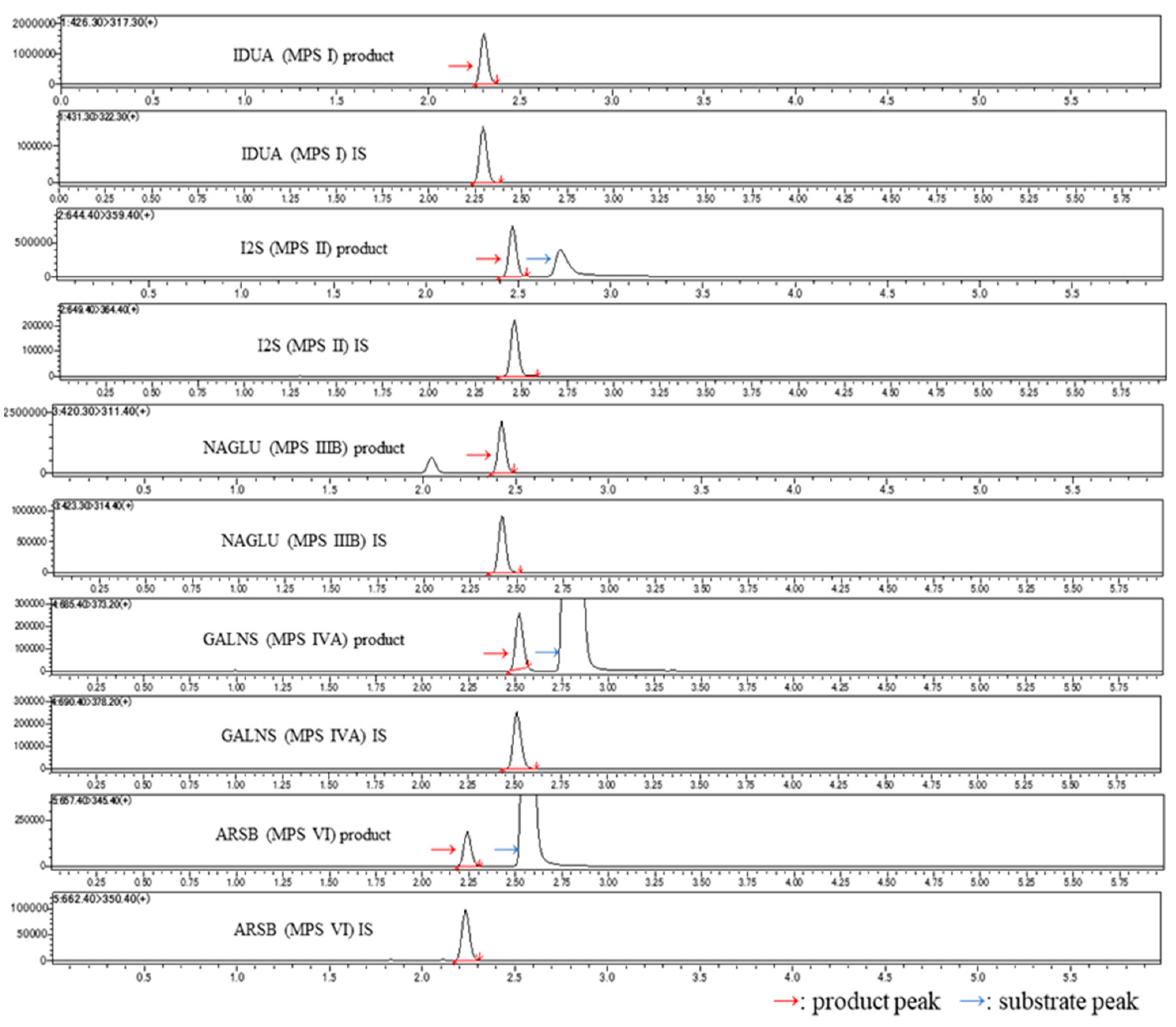
2.1. Chromatograms for Each Disease Type
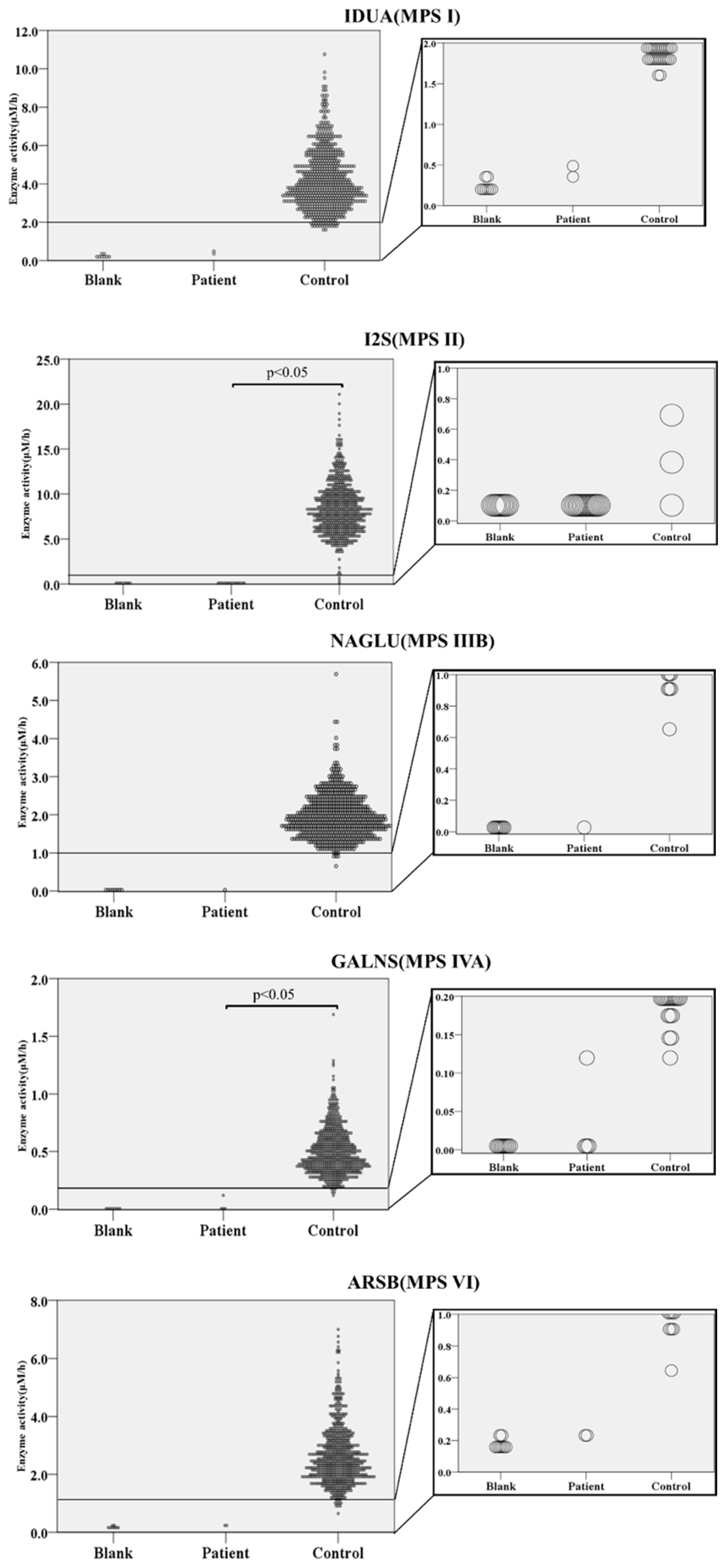
2.2. Enzyme Activities in Controls and Patients with MPS
2.3. Analysis of Stability
3. Discussion
4. Materials and Methods
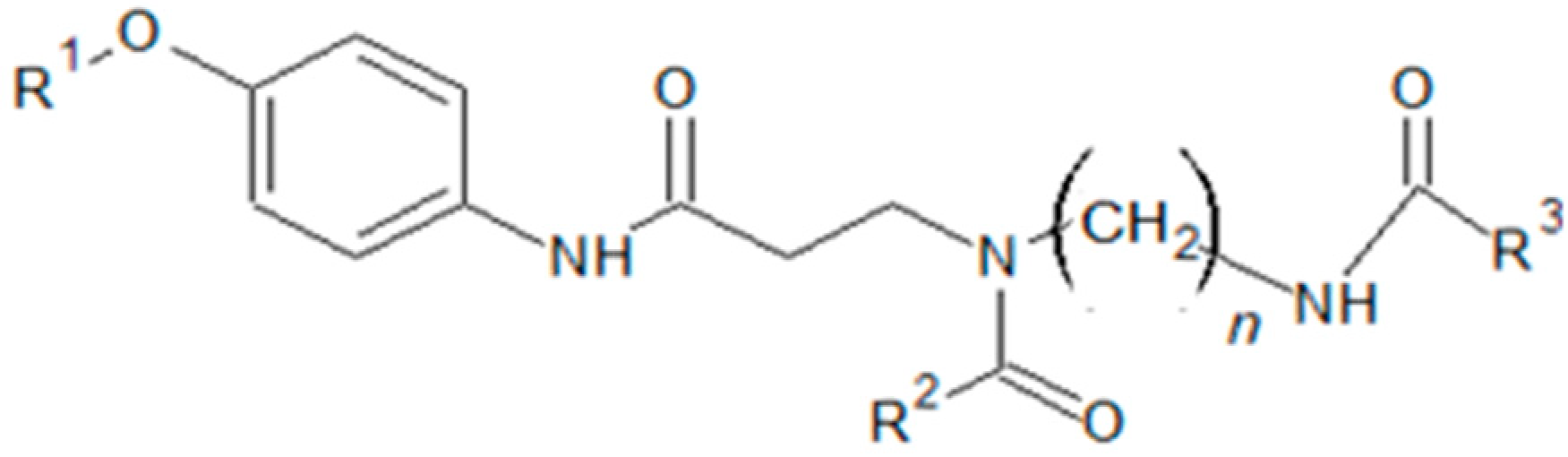
4.1. Materials
4.2. Reagents
4.3. Sample Preparation Procedure
4.4. LC-MS/MS Analysis
4.5. QC
4.6. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| MPS | mucopolysaccharidosis |
| GAG | glycosaminoglycan |
| LSD | lysosomal storage disease |
| NBS | newborn screening |
| LC-MS/MS | liquid chromatography tandem mass spectrometry |
| IDUA | α-L-iduronidase |
| I2S | iduronate-2-sulfatase |
| NAGLU | N-acetyl-α-glucosaminidase |
| GALNS | N-acetylgalactosamine-6-sulfatase |
| ARSB | N-acetylgalactosamine-4-sulfatase |
| PD | pseudo-deficiency |
References
- Stapleton, M.; Arunkumar, N.; Kubaski, F.; Mason, R.W.; Tadao, O.; Tomatsu, S. Clinical presentation and diagnosis of mucopolysaccharidoses. Mol. Genet. Metab. 2018, 125, 4–17. [Google Scholar] [CrossRef]
- Khan, S.A.; Peracha, H.; Ballhausen, D.; Wiesbauer, A.; Rohrbach, M.; Gautschi, M.; Mason, R.W.; Giugliani, R.; Suzuki, Y.; Orii, K.E.; et al. Epidemiology of mucopolysaccharidoses. Mol. Genet. Metab. 2017, 121, 227–240. [Google Scholar] [CrossRef]
- Kubaski, F.; Suzuki, Y.; Orii, K.; Giugliani, R.; Church, H.J.; Mason, R.W.; Dũng, V.C.; Ngoc, C.T.B.; Yamaguchi, S.; Kobayashi, H.; et al. Glycosaminoglycan levels in dried blood spots of patients with mucopolysaccharidoses and mucolipidoses. Mol. Genet. Metab. 2017, 120, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.A.; Mason, R.W.; Giugliani, R.; Orii, K.; Fukao, T.; Suzuki, Y.; Yamaguchi, S.; Kobayashi, H.; Orii, T.; Tomatsu, S. Glycosaminoglycans analysis in blood and urine of patients with mucopolysaccharidosis. Mol. Genet. Metab. 2018, 125, 44–52. [Google Scholar] [CrossRef]
- Kubaski, F.; Brusius-Facchin, A.C.; Mason, R.W.; Patel, P.; Burin, M.G.; Michelin-Tirelli, K.; Kessler, R.G.; Bender, F.; Leistner-Segal, S.; Moreno, C.A.; et al. Elevation of glycosaminoglycans in the amniotic fluid of a fetus with mucopolysaccharidosis VII: Prenatal diagnosis of an MPS VII fetus. Prenat. Diagn. 2017, 37, 435–439. [Google Scholar] [CrossRef]
- Baldo, G.; Matte, U.; Artigalas, O.; Schwartz, I.V.; Burin, M.G.; Ribeiro, E.; Horovitz, D.; Magalhaes, T.P.; Elleder, M.; Giugliani, R. Placenta analysis of prenatally diagnosed patients reveals early GAG storage in mucopolysaccharidoses II and VI. Mol. Genet. Metab. 2011, 103, 197–198. [Google Scholar] [CrossRef]
- Kubaski, F.; Mason, R.W.; Nakatomi, A.; Shintaku, H.; Xie, L.; van Vlies, N.N.; Church, H.; Giugliani, R.; Kobayashi, H.; Yamaguchi, S.; et al. Newborn screening for mucopolysaccharidoses: A pilot study of measurement of glycosaminoglycans by tandem mass spectrometry. J. Inherit. Metab. Dis. 2017, 40, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Tomatsu, S.; Kubaski, F.; Sawamoto, K.; Mason, R.W.; Shimada, T.; Montaño, A.M.; Yamaguchi, S.; Suzuki, Y.; Orii, T. Newborn screening and diagnosis of mucopolysaccharidoses: Application of tandem mass spectrometry. Nihon Masu Sukuriningu Gakkai Shi 2014, 24, 19–37. [Google Scholar]
- de Ruijter, J.; de Ru, M.H.; Wagemans, T.; IJlst, L.; Lund, A.M.; Orchard, P.J.; Schaefer, G.B.; Wijburg, F.A.; van Vlies, N. Heparan sulfate and dermatan sulfate derived disaccharides are sensitive markers for newborn screening for mucopolysaccharidoses types I, II and III. Mol. Genet. Metab. 2012, 107, 705–710. [Google Scholar] [CrossRef]
- Stapleton, M.; Kubaski, F.; Mason, R.W.; Shintaku, H.; Kobayashi, H.; Yamaguchi, S.; Taketani, T.; Suzuki, Y.; Orii, K.; Orii, T.; et al. Newborn screening for mucopolysaccharidoses: Measurement of glycosaminoglycans by LC-MS/MS. Mol. Genet. Metab. Rep. 2020, 22, 100563. [Google Scholar] [CrossRef]
- Taylor, M.; Khan, S.; Stapleton, M.; Wang, J.; Chen, J.; Wynn, R.; Yabe, H.; Chinen, Y.; Boelens, J.J.; Mason, R.W.; et al. Hematopoietic stem cell transplantation for mucopolysaccharidoses: Past, present, and future. Biol. Blood Marrow Transplant. 2019, 25, 226–246. [Google Scholar] [CrossRef]
- Kubaski, F.; Yabe, H.; Suzuki, Y.; Seto, T.; Hamazaki, T.; Mason, R.W.; Xie, L.; Onsten, T.G.H.; Leistner-Segal, S.; Giugliani, R.; et al. Hematopoietic stem cell transplantation for patients with mucopolysaccharidosis II. Biol. Blood Marrow Transplant. 2017, 23, 1795–1803. [Google Scholar] [CrossRef] [Green Version]
- Barth, A.L.; de Magalhães, T.S.P.C.; Reis, A.B.R.; de Oliveira, M.L.; Scalco, F.B.; Cavalcanti, N.C.; e Silva, D.S.; Torres, D.A.; Costa, A.A.P.; Bonfim, C.; et al. Early hematopoietic stem cell transplantation in a patient with severe mucopolysaccharidosis II: A 7 years follow-up. Mol. Genet. Metab. Rep. 2017, 12, 62–68. [Google Scholar] [CrossRef]
- Selvanathan, A.; Ellaway, C.; Wilson, C.; Owens, P.; Shaw, P.J.; Bhattacharya, K. Effectiveness of Early Hematopoietic Stem Cell Transplantation in Preventing Neurocognitive Decline in Mucopolysaccharidosis Type II: A Case Series; Springer: Berlin/Heidelberg, Germany, 2018; Volume 41, pp. 81–89. [Google Scholar]
- Tylki-Szymanska, A.; Jurecka, A.; Zuber, Z.; Rozdzynska, A.; Marucha, J.; Czartoryska, B. Enzyme replacement therapy for mucopolysaccharidosis II from 3 months of age: A 3-year follow-up. Acta Paediatr. 2012, 101, e42–e47. [Google Scholar] [CrossRef]
- Lampe, C.; Atherton, A.; Burton, B.K.; Descartes, M.; Giugliani, R.; Horovitz, D.D.G.; Kyosen, S.O.; Magalhães, T.S.P.C.; Martins, A.M.; Mendelsohn, N.J. Enzyme Replacement Therapy in Mucopolysaccharidosis II Patients under 1 Year of Age; Springer: Berlin/Heidelberg, Germany, 2014; Volume 14, pp. 99–113. [Google Scholar]
- Tanaka, A.; Okuyama, T.; Suzuki, Y.; Sakai, N.; Takakura, H.; Sawada, T.; Tanaka, T.; Otomo, T.; Ohashi, T.; Ishige-Wada, M.; et al. Long-term efficacy of hematopoietic stem cell transplantation on brain involvement in patients with mucopolysaccharidosis type II: A nationwide survey in Japan. Mol. Genet. Metab. 2012, 107, 513–520. [Google Scholar] [CrossRef]
- Elliott, S.; Buroker, N.; Cournoyer, J.J.; Potier, A.M.; Trometer, J.D.; Elbin, C.; Schermer, M.J.; Kantola, J.; Boyce, A.; Turecek, F.; et al. Pilot study of newborn screening for six lysosomal storage diseases using tandem mass spectrometry. Mol. Genet. Metab. 2016, 118, 304–309. [Google Scholar] [CrossRef]
- Kubaski, F.; Osago, H.; Mason, R.W.; Yamaguchi, S.; Kobayashi, H.; Tsuchiya, M.; Orii, T.; Tomatsu, S. Glycosaminoglycans detection methods: Applications of mass spectrometry. Mol. Genet. Metab. 2017, 120, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Gelb, M.H.; Scott, C.R.; Turecek, F. Newborn screening for lysosomal storage diseases. Clin. Chem. 2015, 61, 335–346. [Google Scholar] [CrossRef]
- Gelb, M.H.; Turecek, F.; Scott, C.R.; Chamoles, N.A. Direct multiplex assay of enzymes in dried blood spots by tandem mass spectrometry for the newborn screening of lysosomal storage disorders. J. Inherit. Metab. Dis. 2006, 29, 397–404. [Google Scholar] [CrossRef] [Green Version]
- Schielen, P.; Kemper, E.; Gelb, M. Newborn screening for lysosomal storage diseases: A concise review of the literature on screening methods, therapeutic possibilities and regional programs. Int. J. Neonatal Screen. 2017, 3, 6. [Google Scholar] [CrossRef]
- Bravo-Villalta, H.V.; Neto, E.C.; Schulte, J.; Pereira, J.; Sampaio-Filho, C.; Burin, M.G.; Bitencourt, F.H.; Sebastião, F.M.; Guidobono, R.R.; Brusius-Facchin, A.C.; et al. Investigation of newborns screened in a pilot program for four lysosomal diseases in Brazil. Mol. Genet. Metab. 2017, 120, S31. [Google Scholar] [CrossRef]
- Therrell, B.L.; Padilla, C.D.; Loeber, J.G.; Kneisser, I.; Saadallah, A.; Borrajo, G.J.C.; Adams, J. Current status of newborn screening worldwide: 2015. Semin. Perinatol. 2015, 39, 171–187. [Google Scholar] [CrossRef] [Green Version]
- Chuang, C.-K.; Lin, H.-Y.; Wang, T.-J.; Huang, Y.-H.; Chan, M.-J.; Liao, H.-C.; Lo, Y.-T.; Wang, L.-Y.; Tu, R.-Y.; Fang, Y.-Y.; et al. Status of newborn screening and follow up investigations for Mucopolysaccharidoses I and II in Taiwan. Orphanet J. Rare Dis. 2018, 13, 84. [Google Scholar] [CrossRef] [Green Version]
- Burlina, A.B.; Polo, G.; Salviati, L.; Duro, G.; Zizzo, C.; Dardis, A.; Bembi, B.; Cazzorla, C.; Rubert, L.; Zordan, R.; et al. Newborn screening for lysosomal storage disorders by tandem mass spectrometry in North East Italy. J. Inherit. Metab. Dis. 2018, 41, 209–219. [Google Scholar] [CrossRef]
- Burton, B.K.; Charrow, J.; Hoganson, G.E.; Waggoner, D.; Tinkle, B.; Braddock, S.R.; Schneider, M.; Grange, D.K.; Nash, C.; Shryock, H.; et al. Newborn screening for lysosomal storage disorders in Illinois: The initial 15-month experience. J. Pediatrics 2017, 190, 130–135. [Google Scholar] [CrossRef]
- Ohira, M.; Okuyama, T.; Mashima, R. Quantification of 11 enzyme activities of lysosomal storage disorders using liquid chromatography-tandem mass spectrometry. Mol. Genet. Metab. Rep. 2018, 17, 9–15. [Google Scholar] [CrossRef]
- Mashima, R.; Ohira, M.; Okuyama, T.; Tatsumi, A. Quantification of the enzyme activities of iduronate-2-sulfatase, N-acetylgalactosamine-6-sulfatase and N-acetylgalactosamine-4-sulfatase using liquid chromatography-tandem mass spectrometry. Mol. Genet. Metab. Rep. 2018, 14, 36–40. [Google Scholar] [CrossRef]
- Liu, Y.; Yi, F.; Kumar, A.B.; Kumar Chennamaneni, N.; Hong, X.; Scott, C.R.; Gelb, M.H.; Turecek, F. Multiplex tandem mass spectrometry enzymatic activity assay for newborn screening of the mucopolysaccharidoses and type 2 neuronal ceroid lipofuscinosis. Clin. Chem. 2017, 63, 1118–1126. [Google Scholar] [CrossRef] [Green Version]
- Scott, C.R.; Elliott, S.; Hong, X.; Huang, J.-Y.; Kumar, A.B.; Yi, F.; Pendem, N.; Chennamaneni, N.K.; Gelb, M.H. Newborn screening for mucopolysaccharidoses: Results of a pilot study with 100 000 dried blood spots. J. Pediatrics 2020, 216, 204–207. [Google Scholar] [CrossRef]
- Spacil, Z.; Tatipaka, H.; Barcenas, M.; Scott, C.R.; Turecek, F.; Gelb, M.H. High-Throughput Assay of 9 Lysosomal Enzymes for Newborn Screening. Clin. Chem. 2013, 59, 502–511. [Google Scholar] [CrossRef]
- Kumar, A.B.; Masi, S.; Ghomashchi, F.; Chennamaneni, N.K.; Ito, M.; Scott, C.R.; Turecek, F.; Gelb, M.H.; Spacil, Z. Tandem mass spectrometry has a larger analytical range than fluorescence assays of lysosomal enzymes: Application to newborn screening and diagnosis of mucopolysaccharidoses types II, IVA, and VI. Clin. Chem. 2015, 61, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- Supriya, M.; De, T.; Christopher, R. Effect of temperature on lysosomal enzyme activity during preparation and storage of dried blood spots. J. Clin. Lab. Anal. 2018, 32, e22220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamoles, N.A.; Blanco, M.B.; Gaggioli, D.; Casentini, C. Hurler-like Phenotype: Enzymatic Diagnosis in Dried Blood Spots on Filter Paper. Clin. Chem. 2001, 47, 2098–2102. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Day1 | Day2 | Day3 | Day4 | Day5 | Interday CV | ||
|---|---|---|---|---|---|---|---|
| IDUA (MPS I) | Low | 0.82 (15.98) | 0.88 (2.43) | 0.94 (3.04) | 1.15 (2.49) | 1.19 (13.62) | 14.65 |
| Middle | 5.02 (5.51) | 5.12 (6.46) | 6.13 (4.31) | 7.13 (3.30) | 7.04 (9.24) | 14.78 | |
| High | 10.25 (5.40) | 9.22 (5.23) | 12.12 (5.85) | 15.70 (11.19) | 13.51 (4.84) | 18.98 | |
| Control | 2.90 | 3.65 | 4.50 | 5.70 | none | - | |
| I2S (MPS II) | Low | 0.58 (8.31) | 0.54 (7.41) | 0.68 (6.44) | 0.75 (10.56) | 0.66 (13.53) | 11.82 |
| Middle | 4.86 (7.55) | 4.38 (2.73) | 5.62 (2.84) | 6.03 (5.55) | 4.88 (7.30) | 11.48 | |
| High | 10.45 (6.18) | 10.13 (3.43) | 11.86 (5.26) | 12.53 (7.26) | 8.74 (12.86) | 12.44 | |
| Control | 6.63 | 7.13 | 9.05 | 10.76 | none | - | |
| NAGLU (MPS IIIB) | Low | 0.24 (11.96) | 0.24 (6.78) | 0.23 (8.46) | 0.25 (9.49) | 0.28 (11.34) | 6.85 |
| Middle | 2.08 (6.19) | 1.85 (10.41) | 1.73 (7.76) | 2.06 (10.84) | 1.96 (7.37) | 6.85 | |
| High | 4.85 (4.59) | 4.22 (2.69) | 4.29 (16.11) | 4.84 (5.41) | 4.77 (13.38) | 6.06 | |
| Control | 1.68 | 1.98 | 1.93 | 2.25 | none | - | |
| GALNS (MPS IVA) | Low | 0.10 (4.89) | 0.18 (1.41) | 0.19 (6.15) | 0.22 (7.55) | 0.19 (14.03) | 23.13 |
| Middle | 0.87 (12.55) | 1.42 (7.66) | 1.72 (8.74) | 1.78 (9.72) | 1.39 (4.67) | 22.59 | |
| High | 1.88 (4.64) | 3.27 (10.65) | 3.86 (4.75) | 4.04 (13.23) | 2.78 (19.72) | 24.73 | |
| Control | 0.45 | 0.42 | 0.51 | 0.60 | none | - | |
| ARSB (MPS VI) | Low | 0.39 (9.40) | 0.46 (9.17) | 0.55 (6.20) | 0.55 (14.17) | 0.49 (11.55) | 11.82 |
| Middle | 2.13 (4.79) | 2.39 (3.99) | 3.20 (5.40) | 3.35 (2.33) | 2.90 (8.40) | 16.66 | |
| High | 4.79 (7.09) | 5.30 (9.60) | 6.71 (2.64) | 7.80 (12.14) | 4.60 (24.74) | 21.02 | |
| Control | 2.38 | 2.12 | 2.93 | 3.12 | none | - |
| IDUA | I2S | NAGLU | GALNS | ARSB | |
|---|---|---|---|---|---|
| This study | 4.19 | 8.39 | 1.96 | 0.5 | 2.64 |
| Other studies | 6.56 * | 19.6 ** 16.52 *** | 2.92 *** | 2.1 *** | 13.4 ** 14.6 *** |
| Molecular Weight | Final Concentration (μM) | R1 | R2 | R3 | n | ||
|---|---|---|---|---|---|---|---|
| MPS I (IDUA) | Substrate | 601.65 | 249.82 | α-Iduronosyl | Methyl | Phenyl | 6 |
| Internal Standard | 430.55 | 15.48 | H | Methyl | d5-Phenyl | 6 | |
| MPS II (IDS) | Substrate | 767.23 | 470.01 | α-Iduronosyl-2-sulfate | n-Butyl | Phenyl | 6 |
| Internal Standard | 648.34 | 5.14 | α-Iduronosyl | n-Butyl | d5-Phenyl | 6 | |
| MPS IIIB (NAGLU) | Substrate | 622.76 | 501.19 | α-N-Acetyl-glucosyl | n-Butyl | Ethyl | 6 |
| Internal Standard | 422.3 | 5.02 | H | n-Butyl | d3-Ethyl | 6 | |
| MPS IVA (GALNS) | Substrate | 786.8 | 970.56 | α-N-Acetyl-galactosyl-6-sulfate | n-Pentyl | Phenyl | 6 |
| Internal Standard | 689.39 | 4.84 | α-N-Acetyl-galactosyl | n-Pentyl | d5-Phenyl | 6 | |
| MPS VI (ARSB) | Substrate | 689.39 | 4.84 | α-N-Acetyl-galactosyl-4-sulfate | n-Pentyl | Phenyl | 5 |
| InternalStandard | 758.28 | 967.10 | α-N-Acetyl-galactosyl | n-Butyl | d5-Phenyl | 5 |
| Precursor Ion (m/z) | Product Ion (m/z) | ||
|---|---|---|---|
| MPS I (IDUA) | Product | 426.10 | 317.20 |
| Internal Standard | 431.20 | 322.20 | |
| MPS II (IDS) | Product | 644.32 | 359.23 |
| Internal Standard | 649.35 | 364.26 | |
| MPS IIIB (NAGLU) | Product | 420.20 | 311.20 |
| Internal Standard | 423.20 | 314.20 | |
| MPS IVA (GALNS) | Product | 685.38 | 373.25 |
| Internal Standard | 690.41 | 378.28 | |
| MPS VI (ARSB) | Product | 657.35 | 345.21 |
| Internal Standard | 662.38 | 350.25 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oguni, T.; Tomatsu, S.; Tanaka, M.; Orii, K.; Fukao, T.; Watanabe, J.; Fukuda, S.; Notsu, Y.; Vu, D.C.; Can, T.B.N.; et al. Validation of Liquid Chromatography-Tandem Mass Spectrometry-Based 5-Plex Assay for Mucopolysaccharidoses. Int. J. Mol. Sci. 2020, 21, 2025. https://doi.org/10.3390/ijms21062025
Oguni T, Tomatsu S, Tanaka M, Orii K, Fukao T, Watanabe J, Fukuda S, Notsu Y, Vu DC, Can TBN, et al. Validation of Liquid Chromatography-Tandem Mass Spectrometry-Based 5-Plex Assay for Mucopolysaccharidoses. International Journal of Molecular Sciences. 2020; 21(6):2025. https://doi.org/10.3390/ijms21062025
Chicago/Turabian StyleOguni, Tsubasa, Shunji Tomatsu, Misa Tanaka, Kenji Orii, Toshiyuki Fukao, Jun Watanabe, Seiji Fukuda, Yoshitomo Notsu, Dung Chi Vu, Thi Bich Ngoc Can, and et al. 2020. "Validation of Liquid Chromatography-Tandem Mass Spectrometry-Based 5-Plex Assay for Mucopolysaccharidoses" International Journal of Molecular Sciences 21, no. 6: 2025. https://doi.org/10.3390/ijms21062025