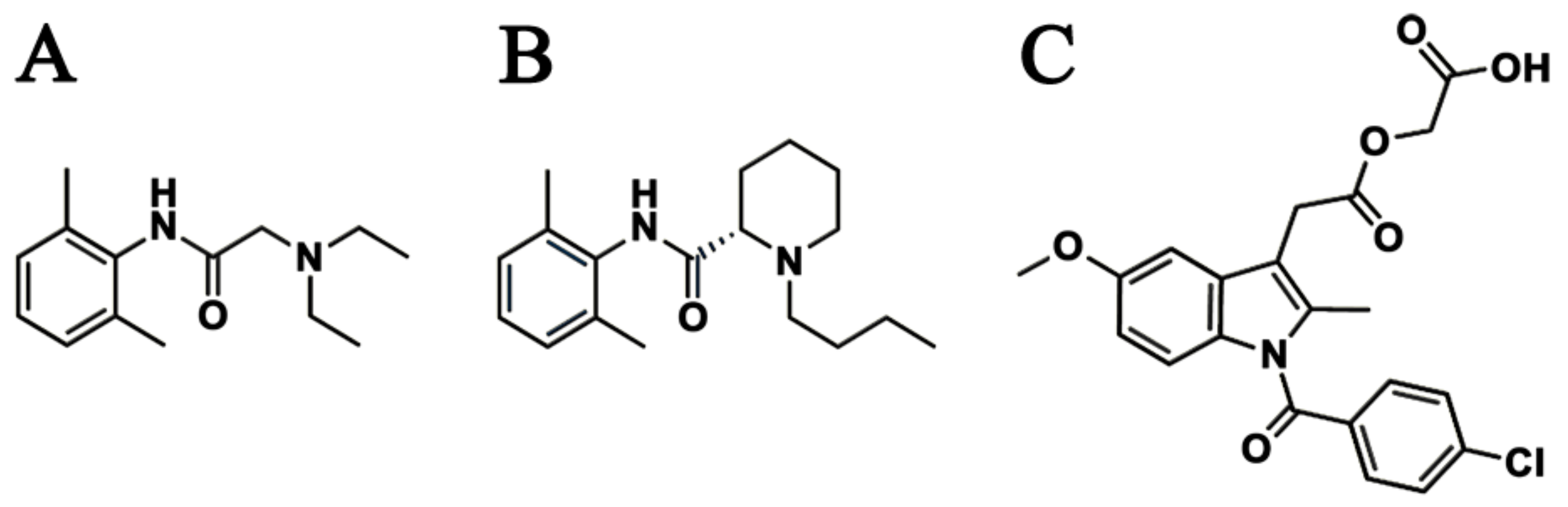
Sustained Release of Levobupivacaine, Lidocaine, and Acemetacin from Electrosprayed Microparticles: In Vitro and In Vivo Studies


Abstract
:1. Introduction
2. Results
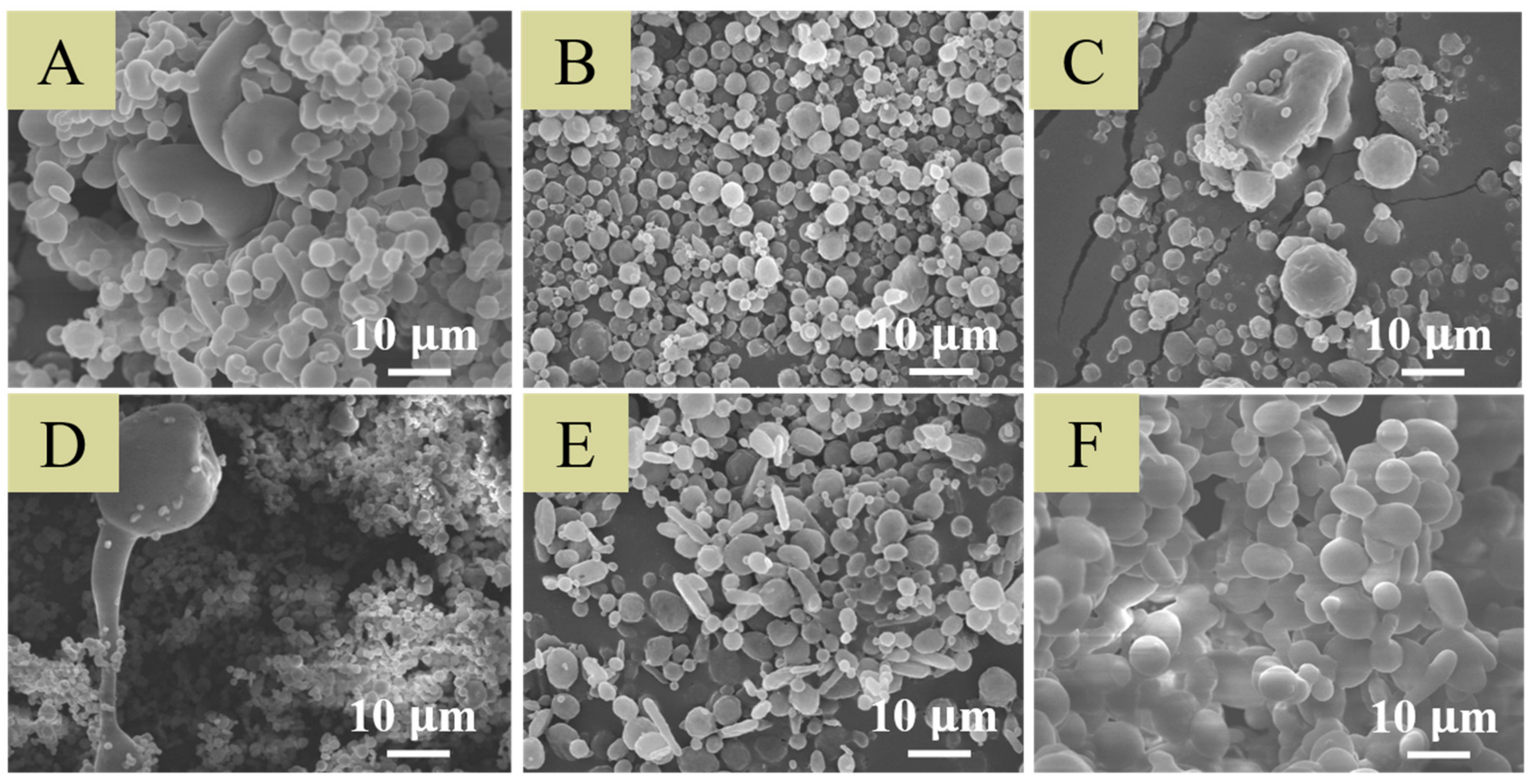
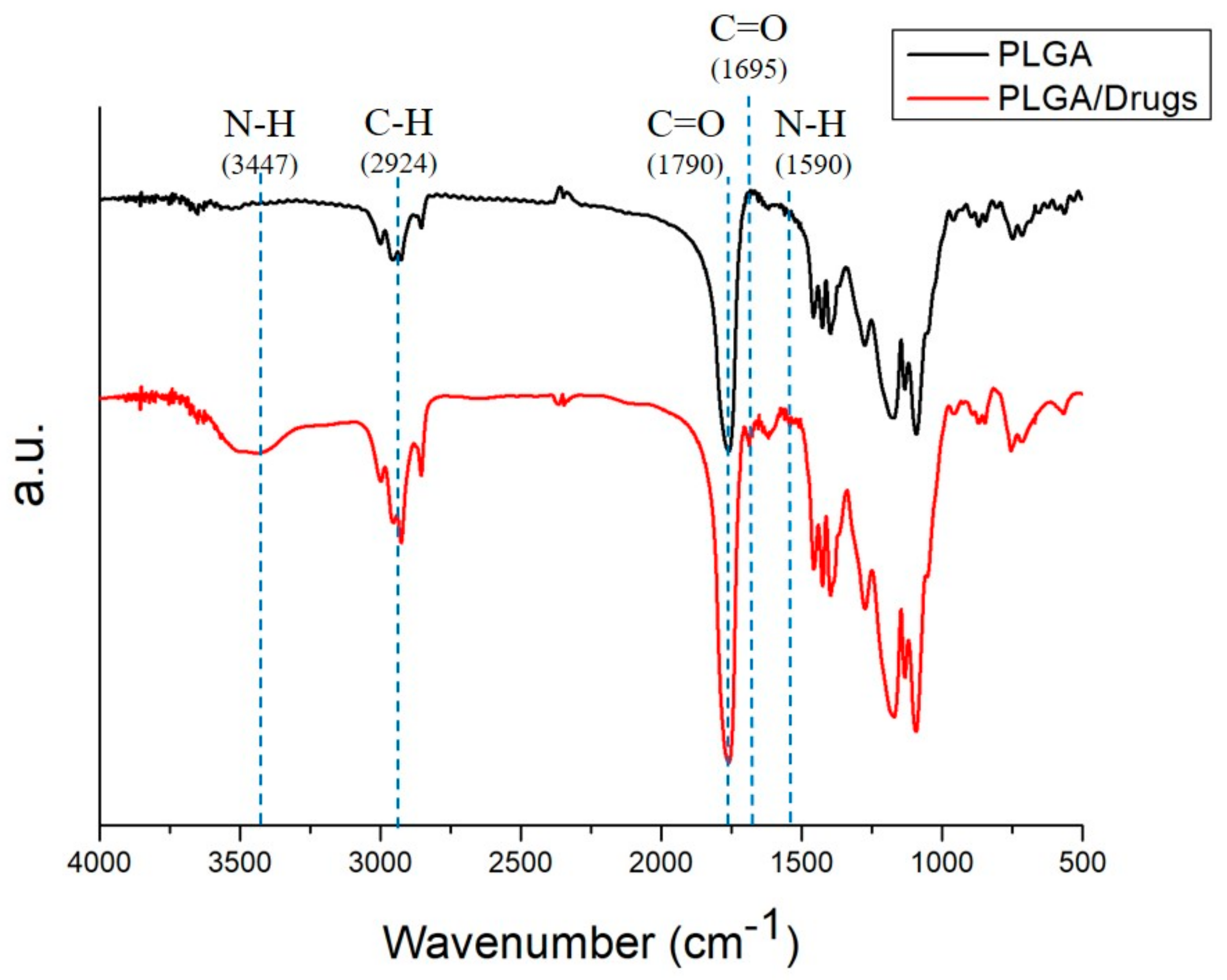
2.1. Characterization of Electrosprayed Particles
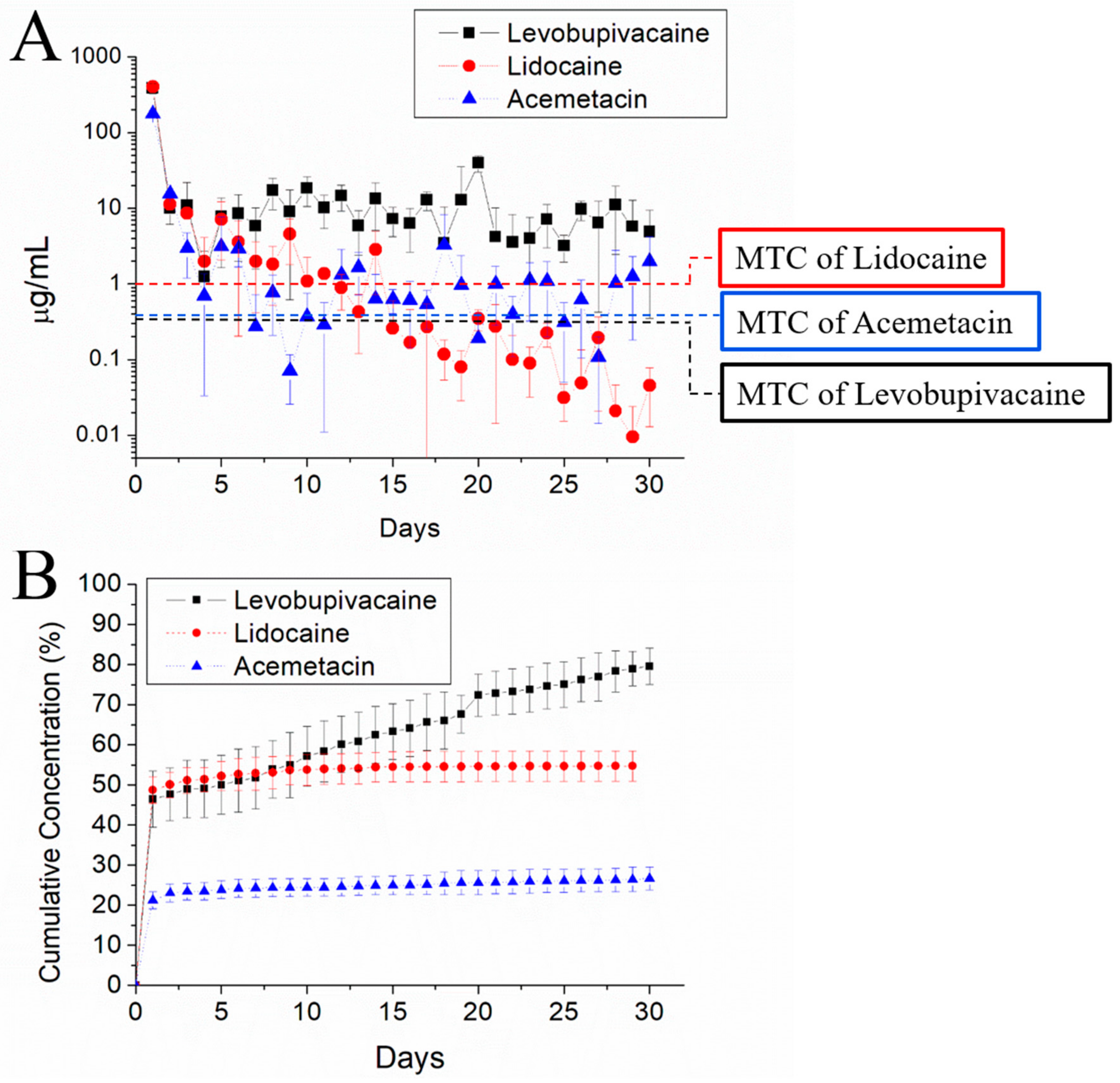
2.2. In Vitro Release of Analgesic-Eluting Microparticles
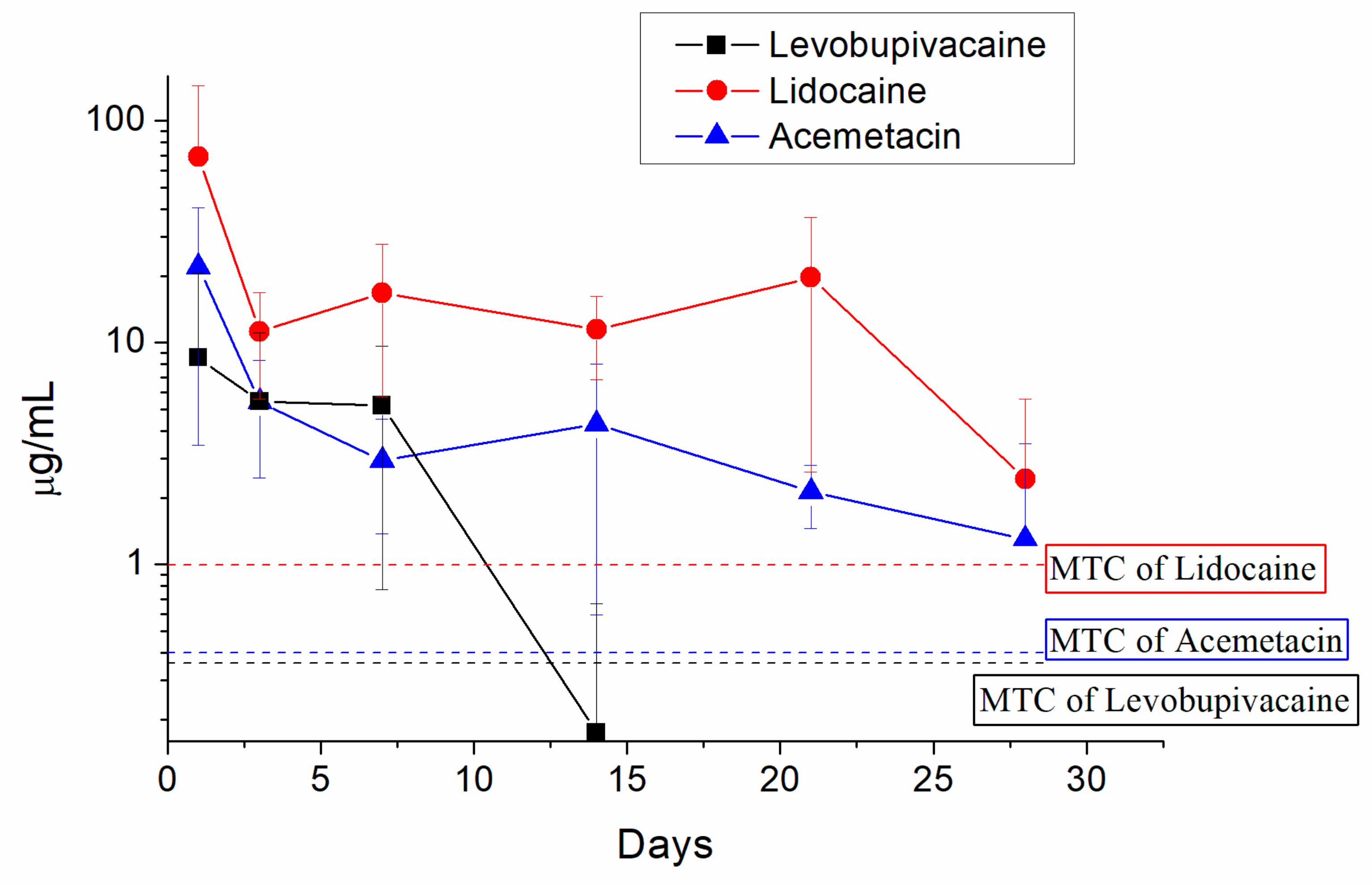
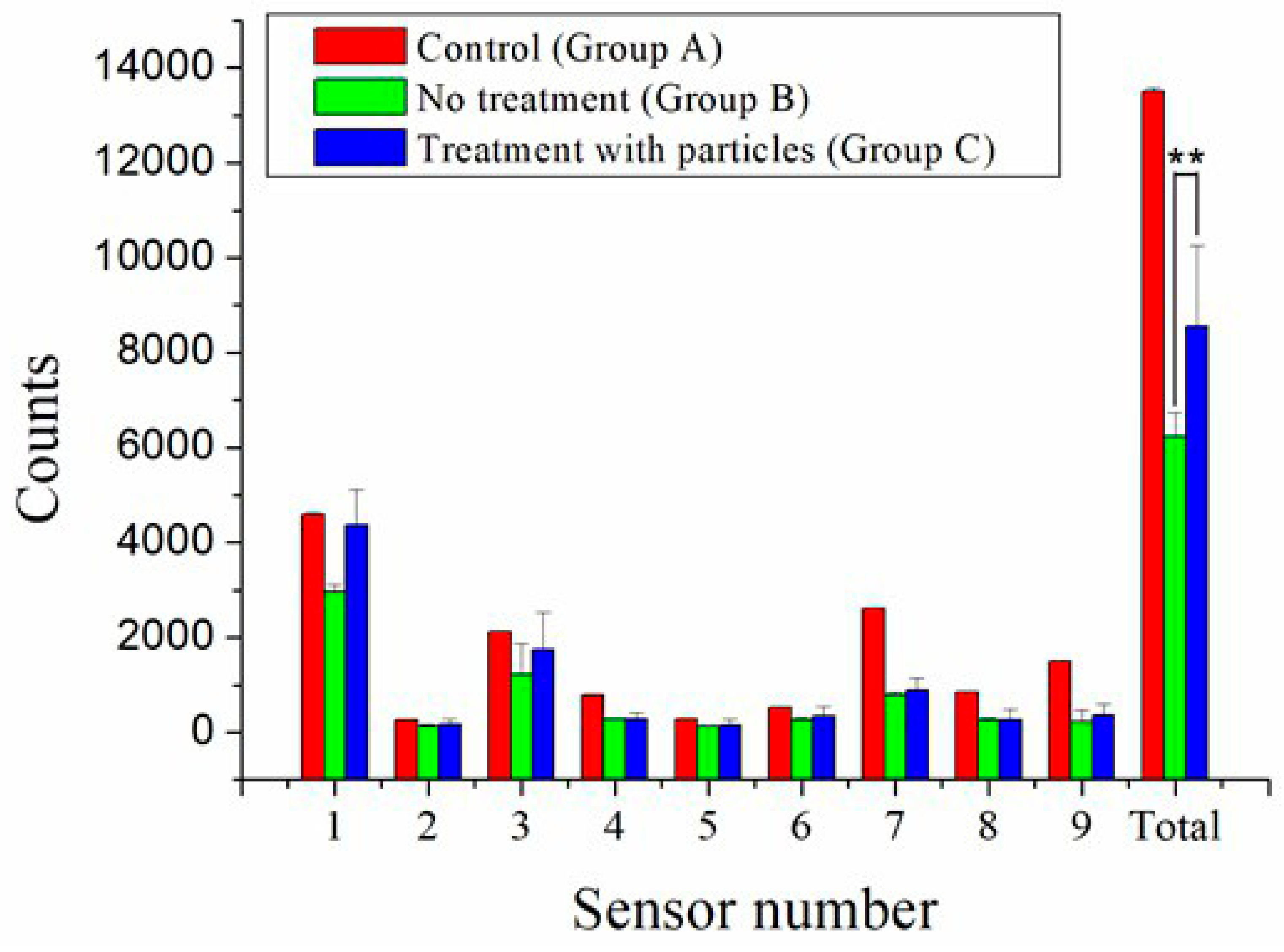
2.3. In Vivo Release and Pain Relief
3. Discussion
4. Materials and Methods
4.1. Production of Biodegradable Analgesic-Eluting Microparticles
4.2. Scanning Electron Microscopy
4.3. Fourier-Transform Infrared Spectrometry
4.4. In Vitro Release of Analgesics
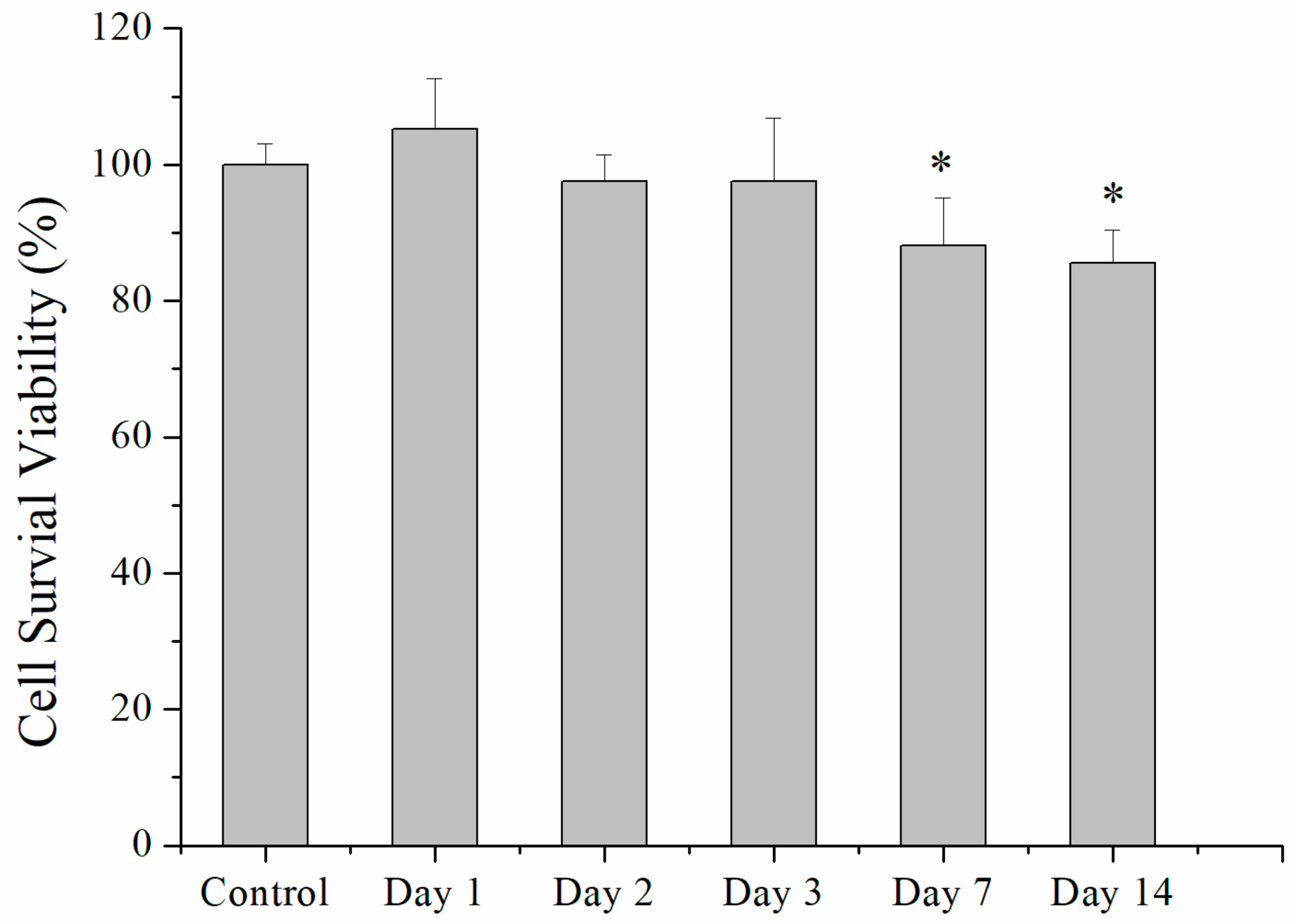
4.5. Cell Culture
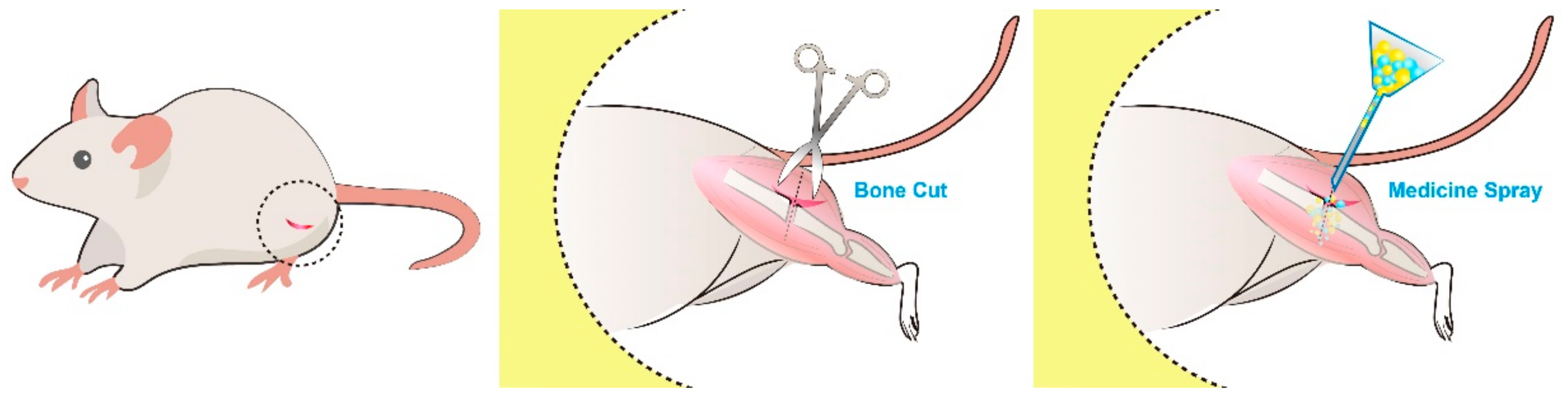
4.6. Rat Femur Shaft Fracture Model: Surgical Procedure and Animal Care
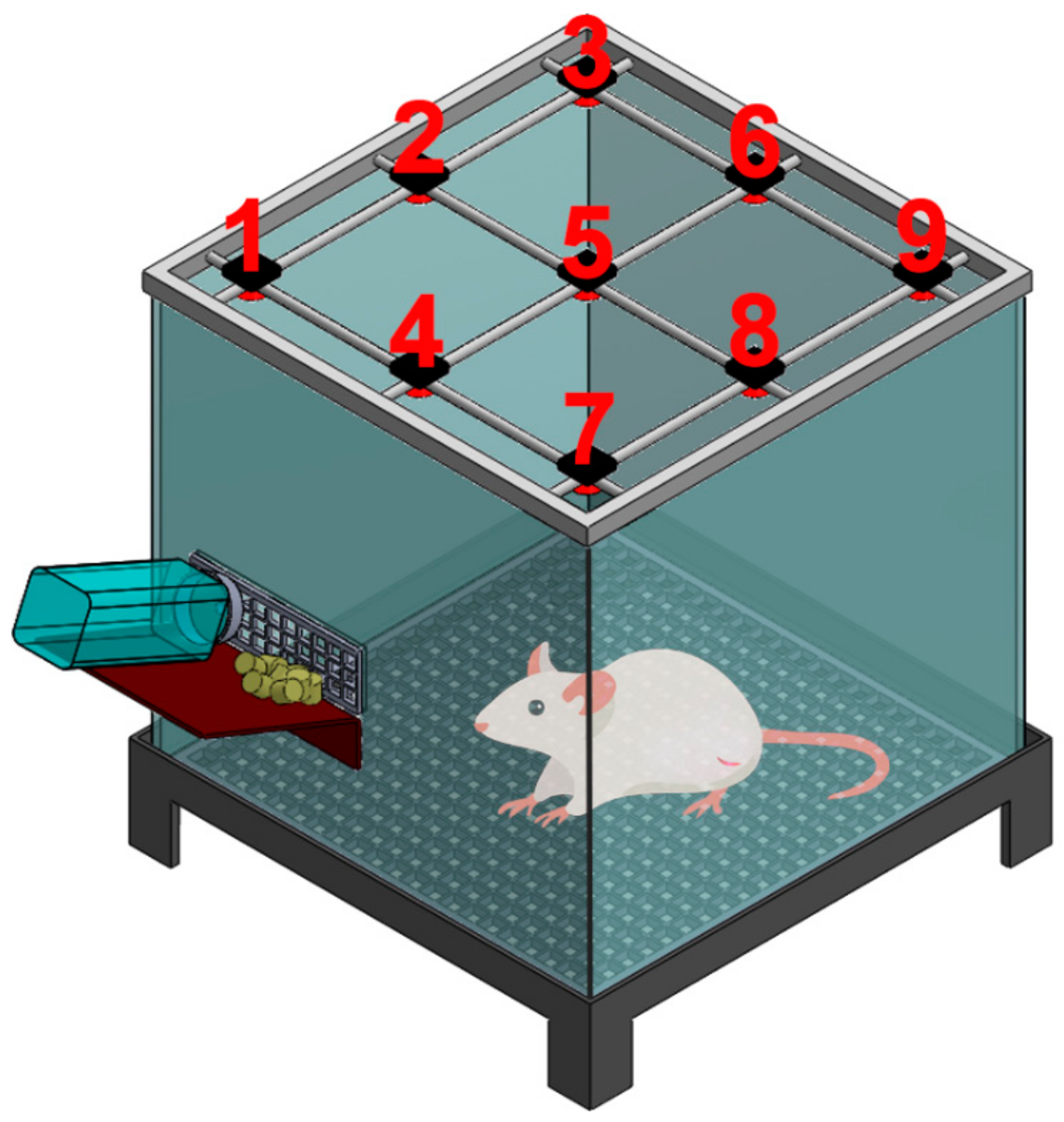
4.7. Post-Surgery Activity Assessment
4.8. Statistics and Data Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alves, C.J.; Neto, E.; Sousa, D.M.; Leitao, L.; Vasconcelos, D.M.; Ribeiro-Silva, M.; Alencastre, I.S.; Lamghari, M. Fracture pain-Traveling unknown pathways. Bone 2016, 85, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, C.B.; Sietsema, D.L. Analysis of operative versus nonoperative treatment of displaced scapular fractures. Clin. Orthop. Relat. Res. 2011, 469, 3379–3389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appelboam, A.; McLauchlan, C.A.; Murdoch, J.; MacIntyre, P.A. Delivery of local anaesthetic via a sternal catheter to reduce the pain caused by sternal fractures: First case series using the new technique. Emerg. Med. J. 2006, 23, 791–793. [Google Scholar] [CrossRef] [PubMed]
- Ko, F.C.; Morrison, R.S. Hip fracture: A trigger for palliative care in vulnerable older adults. JAMA Int. Med. 2014, 174, 1281–1282. [Google Scholar] [CrossRef]
- Sesay, M.; Dousset, V.; Liguoro, D.; Pehourcq, F.; Caille, J.M.; Maurette, P. Intraosseous lidocaine provides effective analgesia for percutaneous vertebroplasty of osteoporotic fractures. Can. J. Anesth. 2002, 49, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Zink, K.A.; Mayberry, J.C.; Peck, E.G.; Schreiber, M.A. Lidocaine patches reduce pain in trauma patients with rib fractures. Am. Surg. 2011, 77, 438–442. [Google Scholar]
- Cheng, Y.J. Lidocaine Skin Patch (Lidopat(R) 5%) Is Effective in the Treatment of Traumatic Rib Fractures: A Prospective Double-Blinded and Vehicle-Controlled Study. Med. Princ. Pract. 2016, 25, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Farrokhi, M.R.; Alibai, E.; Maghami, Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J. Neurosurg. Spine 2011, 14, 561–569. [Google Scholar] [CrossRef] [Green Version]
- Ingalls, N.K.; Horton, Z.A.; Bettendorf, M.; Frye, I.; Rodriguez, C. Randomized, double-blind, placebo-controlled trial using lidocaine patch 5% in traumatic rib fractures. J. Am. Coll. Surg. 2010, 210, 205–209. [Google Scholar] [CrossRef]
- Jain, R.; Basinski, A.; Kreder, H.J. Nonoperative treatment of hip fractures. Int. Orthop. 2003, 27, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.; Ha, Y.C.; Kim, J.Y.; Woo, Y.C.; Lee, J.S.; Jang, E.C. Effectiveness of multimodal pain management after bipolar hemiarthroplasty for hip fracture: A randomized, controlled study. J. Bone Jt. Surg. Am. 2013, 95, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Kang, B.S.; Kim, C.S.; Choi, H.J. Ultrasound-guided regional anesthesia for the pain management of elderly patients with hip fractures in the emergency department. Clin. Exp. Emerg. Med. 2014, 1, 49–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tay, E. Hip fractures in the elderly: Operative versus nonoperative management. Singap. Med. J. 2016, 57, 178–181. [Google Scholar] [CrossRef]
- Cram, P.; Yan, L.; Bohm, E.; Kuzyk, P.; Lix, L.M.; Morin, S.N.; Majumdar, S.R.; Leslie, W.D. Trends in Operative and Nonoperative Hip Fracture Management 1990–2014: A Longitudinal Analysis of Manitoba Administrative Data. J. Am. Geriatr. Soc. 2017, 65, 27–34. [Google Scholar] [CrossRef]
- Holloway, G.B.; Schenk, T.; Williams, G.R.; Ramsey, M.L.; Iannotti, J.P. Arthroscopic Capsular Release for the Treatment of Refractory Postoperative or Post-Fracture Shoulder Stiffness. J. Bone Jt. Surg. Am. 2001, 83, 1682–1687. [Google Scholar] [CrossRef]
- Reahl, G.B.; Marinos, D.; O’Hara, N.N.; Howe, A.; Degani, Y.; Wise, B.; Maceroli, M.; O’Toole, R.V. Risk Factors for Knee Stiffness Surgery After Tibial Plateau Fracture Fixation. J. Orthop. Trauma 2018, 32, e339–e343. [Google Scholar] [CrossRef]
- Yu, Y.H.; Hsu, Y.H.; Chou, Y.C.; Fan, C.L.; Ueng, S.W.; Kau, Y.C.; Liu, S.J. Sustained relief of pain from osteosynthesis surgery of rib fracture by using biodegradable lidocaine-eluting nanofibrous membranes. Nanomedicine 2016, 12, 1785–1793. [Google Scholar] [CrossRef]
- Kao, C.W.; Lee, D.; Wu, M.H.; Chen, J.K.; He, H.L.; Liu, S.J. Lidocaine/ketorolac-loaded biodegradable nanofibrous anti-adhesive membranes that offer sustained pain relief for surgical wounds. Int. J. Nanomed. 2017, 12, 5893–5901. [Google Scholar] [CrossRef] [Green Version]
- Alves, I.P.G.; Nicácio, G.M.; Diniz, M.S.; Rocha, T.L.A.; Kanashiro, G.P.; Cassu, R.N. Analgesic comparison of systemic lidocaine, morphine or lidocaine plus morphine infusion in dogs undergoing fracture repair. Acta Cir. Bras. 2014, 29, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.L.; Cleeman, E.; Auerbach, J.; Flatow, E.L. Comparison of Intra-Articular Lidocaine and Intravenous Sedation for Reduction of Shoulder Dislocations. J. Bone Jt. Surg. Am. 2002, 84, 2135–2139. [Google Scholar] [CrossRef] [Green Version]
- Godoy Monzon, D.; Vazquez, J.; Jauregui, J.R.; Iserson, K.V. Pain treatment in post-traumatic hip fracture in the elderly: Regional block vs. systemic non-steroidal analgesics. Int. J. Emerg. Med. 2010, 3, 321–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frenkel, O.; Mansour, K.; Fischer, J.W. Ultrasound-guided femoral nerve block for pain control in an infant with a femur fracture due to nonaccidental trauma. Pediatr. Emerg. Care 2012, 28, 183–184. [Google Scholar] [CrossRef] [PubMed]
- Brandt, F.; Bank, D.; Cross, S.L.; Weiss, R. A lidocaine-containing formulation of large-gel particle hyaluronic acid alleviates pain. Dermatol. Surg. 2010, 36 (Suppl. 3), 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Mooney, D.J. Designing hydrogels for controlled drug delivery. Nat. Rev. Mater. 2016, 1, 16071. [Google Scholar] [CrossRef] [PubMed]
- Thambi, T.; Li, Y.; Lee, D.S. Injectable hydrogels for sustained release of therapeutic agents. J. Control. Release 2017, 267, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Phan, V.H.G.; Duong, H.T.T.; Thambi, T.; Nugyen, T.L.; Turabee, M.H.; Yin, Y.; Kim, S.H.; Kim, J.; Jeong, J.H.; Lee, D.S. Modularly engineered injectable hybrid hydrogels based on protein-polymer network as potent immunologic adjuvant in vivo. Biomaterials 2019, 195, 100–110. [Google Scholar] [CrossRef]
- Thambi, T.; Phan, V.H.G.; Kim, S.H.; Le, T.M.D.; Duong, H.T.T.; Lee, D.S. Smart injectable biogels based on hyaluronic acid bioconjugates finely substituted with poly(β-amino ester urethane) for cancer therapy. Biomat. Sci. 2019, 7, 5424–5437. [Google Scholar] [CrossRef]
- Kim, S.H.; Thambi, T.; Phan, V.H.G.; Lee, D.S. Modularly engineered alginate bioconjugate hydrogel as biocompatible injectable scaffold for in situ biomineralization. Carbohy. Polym. 2020, 233, 115832. [Google Scholar] [CrossRef]
- Manvelian, G.; Hochberg, M.C.; Daniels, S.E.; Altman, R.D.; Young, C.L. A phase 2 study of lower-dose, indomethacin submicron particle capsules demonstrates early onset of acute pain relief. Clin. J. Pain 2014, 30, 846–851. [Google Scholar] [CrossRef]
- Sun, X.; Xu, C.; Wu, G.; Ye, Q.; Wang, C. Poly(Lactic-co-Glycolic Acid): Applications and Future Prospects for Periodontal Tissue Regeneration. Polymers 2017, 9, 189. [Google Scholar] [CrossRef]
- Makadia, H.K.; Siegel, S.J. Poly Lactic-co-Glycolic Acid (PLGA) as Biodegradable Controlled Drug Delivery Carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef] [PubMed]
- Bock, N.; Woodruff, M.A.; Hutmacher, D.W.; Dargaville, T.R. Electrospraying, a Reproducible Method for Production of Polymeric Microspheres for Biomedical Applications. Polymers 2011, 3, 131–149. [Google Scholar] [CrossRef] [Green Version]
- Correia, D.M.; Gonçalves, R.; Ribeiro, C.; Sencadas, V.; Botelho, G.; Ribelles, J.L.G.; Lanceros-Méndez, S. Electrosprayed poly(vinylidene fluoride) microparticles for tissue engineering applications. RSC Adv. 2014, 4, 33013–33021. [Google Scholar] [CrossRef] [Green Version]
- Yazicioglu, D.; Akkaya, T.; Sonmez, E.; Gumus, H. Addition of lidocaine to levobupivacaine reduces intrathecal block duration: Randomized controlled trial. Revista Brasileira de Anestesiologia 2014, 64, 159–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botros, J.M. Comparative study between a combination of lidocaine and levobupivacaine and that of lidocaine, levobupivacaine, and dexmedetomidine during peribulbar anesthesia for phacoemulsifi cation cataract surgery. Ain-Shams J. Anaesthesiol. 2017, 10, 224–229. [Google Scholar]
- Kao, C.W.; Tseng, Y.Y.; Liu, K.S.; Liu, Y.W.; Chen, J.C.; He, H.L.; Kau, Y.C.; Liu, S.J. Anesthetics and human epidermal growth factor incorporated into anti-adhesive nanofibers provide sustained pain relief and promote healing of surgical wounds. Int. J. Nanomed. 2019, 14, 4007–4016. [Google Scholar] [CrossRef] [Green Version]
- Niederwanger, V.; Gozzo, F.; Griesser, U.J. Characterization of four crystal polymorphs and a monohydrate of s-bupivacaine hydrochloride (levobupivacaine hydrochloride). J. Pharm. Sci. 2009, 98, 1064–1074. [Google Scholar] [CrossRef]
- Fraceto, L.F.; Pinto, L.D.M.A.; Franzoni, L.; Braga, A.A.C.; Spisni, A.; Schreier, S.; de Paula, E. Spectroscopic evidence for a preferential location of lidocaine inside phospholipid bilayers. Biophys. Chem. 2002, 99, 229–243. [Google Scholar] [CrossRef]
- Sanphui, P.; Bolla, G.; Nangia, A.; Chernyshev, V. Acemetacin cocrystals and salts: Structure solution from powder X-ray data and form selection of the piperazine salt. IUCrJ 2014, 1, 136–150. [Google Scholar] [CrossRef] [Green Version]
- Dhakad, R.K.; Panwar, M.; Gupta, S. Plating versus conservative treatment in mid shaft fractures of clavicle: A comparative study. J. Clin. Orthop. Trauma 2016, 7, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Shetty, S.K.; Chandran, R.; Ballal, A.; Mathias, L.J.; Hegde, A.; Shetty, A. To operate or not to operate the Mid-Shaft Fractures of the Clavicle: A Comparative Study of Functional Outcomes of the Two Methods of Management. J. Clin. Diagn. Res. 2017, 11, RC01–RC03. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.G.; Whittle, A.P.; Wood, G.W. Nonoperative treatment of ipsilateral fractures of the scapula and clavicle. J. Bone Jt. Surg. Am. 2000, 82, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Cole, P.A.; Freeman, G.; Dubin, J.R. Scapula fractures. Curr. Rev. Musculoskelet. Med. 2013, 6, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, M.-Y.; Feng, C.-H.; Liu, Y.-W.; Liu, S.-J. An Orthogonal Model to Study the Effect of Electrospraying Parameters on the Morphology of poly (d,l)-lactide-co-glycolide (PLGA) Particles. Appl. Sci. 2019, 9, 1077. [Google Scholar] [CrossRef] [Green Version]
- Mir, M.; Ahmed, N.; Rehman, A.U. Recent applications of PLGA based nanostructures in drug delivery. Colloids Surf. B Biointerface 2017, 159, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.; Heard, K.; Foran, M.; Koyfman, A. Intravenous lipid emulsion in the emergency department: A systematic review of recent literature. J. Emerg. Med. 2015, 48, 387–397. [Google Scholar] [CrossRef]
- Siepmann, J.; Siepman, F. Microparticles used as drug delivery systems. Progr. Colloid Polym. Sci. 2006, 133, 15–21. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Voltage (kV) | Flow rate (mL/hr) | Travel distance (cm) |
|---|---|---|---|
| A | 9 | 1 | 5 |
| B | 9 | 1 | 10 |
| C | 9 | 1 | 20 |
| D | 6 | 1 | 10 |
| E | 15 | 1 | 10 |
| F | 9 | 2 | 10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-M.; Liu, K.-C.; Yeh, W.-L.; Chen, J.-C.; Liu, S.-J. Sustained Release of Levobupivacaine, Lidocaine, and Acemetacin from Electrosprayed Microparticles: In Vitro and In Vivo Studies. Int. J. Mol. Sci. 2020, 21, 1093. https://doi.org/10.3390/ijms21031093
Chen J-M, Liu K-C, Yeh W-L, Chen J-C, Liu S-J. Sustained Release of Levobupivacaine, Lidocaine, and Acemetacin from Electrosprayed Microparticles: In Vitro and In Vivo Studies. International Journal of Molecular Sciences. 2020; 21(3):1093. https://doi.org/10.3390/ijms21031093
Chicago/Turabian StyleChen, Jian-Ming, Kuan-Chieh Liu, Wen-Ling Yeh, Jin-Chung Chen, and Shih-Jung Liu. 2020. "Sustained Release of Levobupivacaine, Lidocaine, and Acemetacin from Electrosprayed Microparticles: In Vitro and In Vivo Studies" International Journal of Molecular Sciences 21, no. 3: 1093. https://doi.org/10.3390/ijms21031093