Increasing Incidence of Liposarcoma: A Population-Based Study of National Surveillance Databases, 2001–2016


Abstract
:1. Introduction
2. Methods
2.1. Variables Available from SEER and CNCPR Datasets
2.2. Variables Available from SEER Dataset
2.3. Time Trends
3. Results
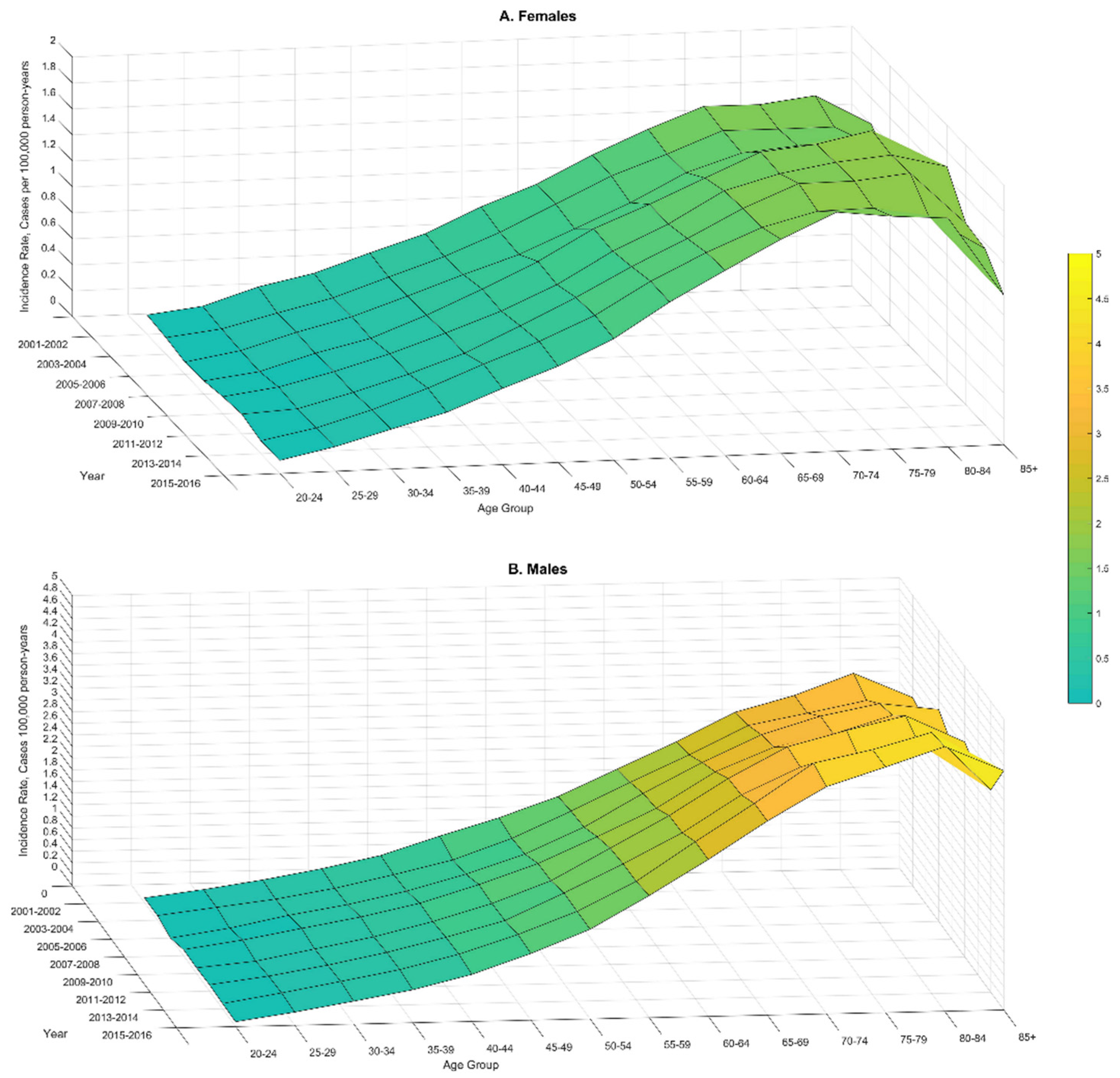
3.1. Age-Specific Rates from SEER and CNPCR
3.2. Time Trends from SEER and CNPCR
3.3. Distribution of Liposarcoma by Grade, Size, and Stage from SEER
3.4. Liposarcoma Survival from SEER
4. Discussion
5. Conclusions
- This analysis found that men and whites have higher risk of liposarcoma compared to other demographic subgroups.
- The liposarcoma tumors most frequently were found in the extremities and retroperitoneum.
- This population-based comprehensive analysis demonstrates increasing incident rates of liposarcoma between 2001–2016.
- The increase in incidence was mostly pronounced in high-risk demographic subgroups, suggesting an interaction between genetic and non-genetic modifiable risk factors that may play a role in liposarcoma etiology.
- Retroperitoneal tumors showed poor survival but greater increase in incidence.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| APC | Annual percent change |
| CNPCR | Combined SEER-National Program of Cancer Registries |
| CI | Confidence interval |
| NCIN | National Cancer Intelligence Network |
| NPCR | National Program of Cancer Registries |
| SEER | Surveillance, Epidemiology, and End Result |
| PC | Total percent change |
| U.K. | United Kingdom |
| U.S. | United States |
| WHO | World Health Organization |
References
- Gatta, G.; Van Der Zwan, J.M.; Casali, P.; Siesling, S.; Tos, A.P.D.; Kunkler, I.; Otter, R.; Licitra, L.; Mallone, S.; Tavilla, A.; et al. Rare cancers are not so rare: The rare cancer burden in Europe. Eur. J. Cancer 2011, 47, 2493–2511. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. NCI Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/791790 (accessed on 21 November 2019).
- DeSantis, C.; Kramer, J.L.; Jemal, A. The burden of rare cancers in the United States. CA A Cancer J. Clin. 2017, 67, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronicke, S.; Hirsch, M.C.; Türk, E.; Larionov, K.; Tientcheu, D.; Wagner, A.D. Can a decision support system accelerate rare disease diagnosis? Evaluating the potential impact of Ada DX in a retrospective study. Orphanet J. Rare Dis. 2019, 14, 69. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Capocaccia, R.; Botta, L.; Mallone, S.; De Angelis, R.; Ardanaz, E.; Comber, H.; Dimitrova, N.; Leinonen, M.K.; Siesling, S.; et al. Burden and centralised treatment in Europe of rare tumours: Results of RARECAREnet—A population-based study. Lancet Oncol. 2017, 18, 1022–1039. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. United States Cancer Statistics: Data Visualizations. Changes Over Time: Colon and Rectum. Available online: https://gis.cdc.gov/Cancer/USCS/DataViz.html (accessed on 21 November 2019).
- Francesco, M.; Frenos, F.; Bettini, L.; Matera, D.; Mondanelli, N.; Scorianz, M.; Cuomo, P.; Scoccianti, G.; Beltrami, G.; Greto, D.; et al. Liposarcoma: Clinico-pathological analysis, prognostic factors and survival in a series of 307 patients treated at a single institution. J. Orthop. Sci. 2018, 23, 1038–1044. [Google Scholar] [CrossRef] [Green Version]
- Barbetakis, N.; Samanidis, G.; Samanidou, E.; Kirodimos, E.; Kiziridou, A.; Bischiniotis, T.; Tsilikas, C. Primary mediastinal liposarcoma: A case report. J. Med Case Rep. 2007, 1, 161. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Qian, S.; Jin, L. Prognostic factors of patients with extremity myxoid liposarcomas after surgery. J. Orthop. Surg. Res. 2019, 14, 90. [Google Scholar] [CrossRef] [Green Version]
- Tseng, W.H.; Martinez, S.R.; Do, L.; Tamurian, R.M.; Borys, D.; Canter, R.J. Lack of Survival Benefit Following Adjuvant Radiation in Patients with Retroperitoneal Sarcoma: A SEER Analysis. J. Surg. Res. 2011, 168, e173–e180. [Google Scholar] [CrossRef]
- Smith, C.A.; Martinez, S.R.; Tseng, W.H.; Tamurian, R.M.; Bold, R.J.; Borys, D.; Canter, R.J. Predicting Survival for Well-Differentiated Liposarcoma: The Importance of Tumor Location. J. Surg. Res. 2012, 175, 12–17. [Google Scholar] [CrossRef]
- Gerry, D.; Fox, N.F.; Spruill, L.S.; Lentsch, E.J. Liposarcoma of the head and neck: Analysis of 318 cases with comparison to non-head and neck sites. Head Neck 2013, 36, 393–400. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. NPCR and SEER incidence- U.S. Cancer Statistics Public Use Database Data Standards and Data Dictionary. Available online: https://www.cdc.gov/cancer/uscs/public-use/pdf/npcr-seer-public-use-database-data-dictionary-2001-2015-508.pdf (accessed on 5 April 2019).
- SEER.Cancer.gov. List of SEER Registries. Available online: https://seer.cancer.gov/registries/list.html (accessed on 5 April 2019).
- Centers for Disease Control and Prevention. Costs of Intimate Partner Violence against Women in the United States; CDC, National Center for Injury Prevention and Control: Atlanta, GA, USA, 2003.
- Surveillance Research Program, National Cancer Institute, Version 8.3; SEER*Stat Software; National Cancer Institute: Bethesda, MD, USA, 2019.
- Fay, M.P. Approximate confidence intervals for rate ratios from directly standardized rates with sparse data. Commun. Stat.-Theory Methods 1999, 28, 2141–2160. [Google Scholar] [CrossRef]
- Fay, M.P.; Tiwari, R.C.; Feuer, E.J.; Zou, Z. Estimating Average Annual Percent Change for Disease Rates without Assuming Constant Change. Biometrics 2006, 62, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Jo, V.; Fletcher, C.D.M. WHO classification of soft tissue tumours: An update based on the 2013 (4th) edition. Pathology 2014, 46, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Blay, J. The theory. An introduction on dedifferentiated liposarcoma. Cancer Chemother. Rev. 2018, 13, 3–6. [Google Scholar]
- Ruhl, J.L.; Callaghan, C.; Hurlbut, A.; Ries, L.A.G.; Adamo, P.; Dickie, L.; Schussler, N. (Eds.) Summary Stage 2018: Codes and Coding Instructions; National Cancer Institute: Bethesda, MD, USA, 2018.
- Nattinger, A.; McAuliffe, T.L.; Schapira, M.M. Generalizability of the surveillance, epidemiology, and end results registry population: Factors relevant to epidemiologic and health care research. J. Clin. Epidemiol. 1997, 50, 939–945. [Google Scholar] [CrossRef]
- Kuo, T.; Mobley, L.R. How generalizable are the SEER registries to the cancer populations of the USA? Cancer Causes Control 2016, 27, 1117–1126. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, J.K.; Rosholm, J.-U.; Ewertz, M.; Engholm, G.; Lindahl-Jacobsen, R.; Christensen, K. Declining cancer incidence at the oldest ages: Hallmark of aging or lower diagnostic activity? J. Geriatr. Oncol. 2019, 10, 792–798. [Google Scholar] [CrossRef] [Green Version]
- Harding, C.; Pompei, F.; Lee, E.E.; Wilson, R. Cancer Suppression at Old Age. Cancer Res. 2008, 68, 4465–4478. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Intelligence Network (NCIN). Liposarcoma: Incidence and Survival Rates in England. NCIN Data Briefings. Available online: http://www.ncin.org.uk/publications/data_briefings/liposarcoma_incidence_and_survival_rates_in_england (accessed on 5 April 2019).
- Radkiewicz, C.; Johansson, A.L.V.; Dickman, P.; Lambe, M.; Edgren, G. Sex differences in cancer risk and survival: A Swedish cohort study. Eur. J. Cancer 2017, 84, 130–140. [Google Scholar] [CrossRef]
- Afshar, N.; English, D.R.; Thursfield, V.; Mitchell, P.L.; Marvelde, L.T.; Farrugia, H.; Giles, G.G.; Milne, R.L. Differences in cancer survival by sex: A population-based study using cancer registry data. Cancer Causes Control 2018, 29, 1059–1069. [Google Scholar] [CrossRef]
- Ellison, L.F. Differences in cancer survival in Canada by sex. Heal. Rep. 2016, 27, 19–27. [Google Scholar]
- Greto, D.; Saieva, C.; Loi, M.; Terziani, F.; Visani, L.; Garlatti, P.; Russo, M.L.; Muntoni, C.; Becherini, C.; Topulli, J.; et al. Influence of age and subtype in outcome of operable liposarcoma. Radiol. Med. 2018, 124, 290–300. [Google Scholar] [CrossRef] [PubMed]
- De Vita, A.; Mercatali, L.; Recine, F.; Pieri, F.; Riva, N.; Bongiovanni, A.; Liverani, C.; Spadazzi, C.; Miserocchi, G.; Amadori, D.; et al. Current classification, treatment options, and new perspectives in the management of adipocytic sarcomas. OncoTargets Ther. 2016, 9, 6233–6246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.Y.; Lucas, D.R. Dedifferentiated Liposarcoma with Myofibroblastic Differentiation. Arch. Pathol. Lab. Med. 2018, 142, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, P.B.; Walle, K.V.; Winslow, E.R.; Ethun, C.G.; Tran, T.B.; Poultsides, G.; Tseng, J.; Roggin, K.; Grignol, V.; Howard, J.H.; et al. Predictors of Disease-Free and Overall Survival in Retroperitoneal Sarcomas: A Modern 16-Year Multi-Institutional Study from the United States Sarcoma Collaboration (USSC). Sarcoma 2019. [Google Scholar] [CrossRef] [PubMed]
- Harazin-Lechowska, A.; Ambroziak-Lackowska, B.; Ryś, J.; Kruczak, A.; Gruchala, A.; Jaszcz-Gruchała, A.; Danda, D.; Przewoźnik, M.; Halaszka, K. The role of histology, grading, location of tumour and ploidy in evaluation of outcome in patients with liposarcoma. Pol. J. Pathol. 2017, 68, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Dalal, K.M.; Antonescu, C.R.; Singer, S. Diagnosis and management of lipomatous tumors. J. Surg. Oncol. 2008, 97, 298–313. [Google Scholar] [CrossRef]
- Wibmer, C.; Leithner, A.; Zielonke, N.; Sperl, M.; Windhager, R. Increasing incidence rates of soft tissue sarcomas? A population-based epidemiologic study and literature review. Ann. Oncol. 2010, 21, 1106–1111. [Google Scholar] [CrossRef]
- Kollár, A.; Rothermundt, C.; Klenke, F.; Bode, B.; Baumhoer, D.; Arndt, V.; Feller, A.; NICER Working Group. Incidence, mortality, and survival trends of soft tissue and bone sarcoma in Switzerland between 1996 and 2015. Cancer Epidemiol. 2019, 63, 101596. [Google Scholar] [CrossRef]
- Pasquali, S.; Colombo, C.; Pizzamiglio, S.; Verderio, P.; Callegaro, D.; Stacchiotti, S.; Broto, J.M.; López-Pousa, A.; Ferrari, S.; Poveda, A.; et al. High-risk soft tissue sarcomas treated with perioperative chemotherapy: Improving prognostic classification in a randomised clinical trial. Eur. J. Cancer 2018, 93, 28–36. [Google Scholar] [CrossRef]
- Pasquali, S.; Pizzamiglio, S.; Touati, N.; Litiere, S.; Marreaud, S.; Kasper, B.; Gelderblom, H.; Stacchiotti, S.; Judson, I.; Tos, A.P.D.; et al. The impact of chemotherapy on survival of patients with extremity and trunk wall soft tissue sarcoma: Revisiting the results of the EORTC-STBSG 62931 randomised trial. Eur. J. Cancer 2019, 109, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Callegaro, D.; Miceli, R.; Mariani, L.; Raut, C.P.; Gronchi, A. Soft tissue sarcoma nomograms and their incorporation into practice. Cancer 2017, 123, 2802–2820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA A Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Siegel, R.L.; Rosenberg, P.S.; Jemal, A. Emerging cancer trends among young adults in the USA: Analysis of a population-based cancer registry. Lancet Public Heal. 2019, 4, e137–e147. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| SEER | CNPCR | |||
|---|---|---|---|---|
| Count (%) | Incidence Rate, Cases per 100,000 person-years (95% CI) | Count (%) | Incidence Rate, Cases per 100,000 person-years (95% CI) | |
| All cases | 11,162 (100) | 1.08 (1.06–1.10) | 37,499 (100) | 1.01 (1.00–1.02) |
| Sex | ||||
| Male (ref) | 6803 (60.95) | 1.44 (1.41–1.48) | 22,681 (60.48) | 1.33 (1.31–1.35) |
| Female | 4359 (39.05) | 0.79 (0.77–0.82) * | 14,818 (39.52) | 0.75 (0.74–0.77)* |
| Race | ||||
| White (ref) | 9198 (82.40) | 1.13 (1.10–1.15) | 32,186 (85.83) | 1.04 (1.03–1.05) |
| Black | 922 (8.26) | 0.85 (0.7– 0.91) * | 3235 (8.63) | 0.81 (0.78–0.84)* |
| Other | 1042 (9.34) | 0.95 (0.89–1.01) * | 2078 (5.54) | 1.03 (0.99–1.08) |
| SEER | CNPCR | |||
|---|---|---|---|---|
| Count (%) | Incidence Rate, Cases per 100,000 p-years (95% CI) | Count (%) | Incidence Rate, Cases per 100,000 p-years (95% CI) | |
| Histological type | ||||
| Well-differentiated (ref) | 3688 (33.04) | 0.35 (0.34–0.37) | 11,629 (31.01) | 0.31 (0.30–0.32) |
| Myxoid | 2094 (18.76) | 0.21 (0.20–0.22) * | 6938 (18.50) | 0.19 (0.19–0.20) * |
| Pleomorphic | 818 (7.33) | 0.08 (0.07–0.09) * | 2922 (7.79) | 0.08 (0.08–0.08) * |
| Dedifferentiated | 2193 (19.65) | 0.21 (0.20–0.22) * | 7558 (20.16) | 0.20 (0.20–0.21) * |
| Other # | 2369 (21.22) | 0.23 (0.22–0.24) * | 8452 (22.54) | 0.23 (0.20– 0.23) * |
| Tumor site | ||||
| Extremities (ref) | 4531 (40.59) | 0.44 (0.43–0.45) | 14,768 (39.38) | 0.40 (0.40–0.41) |
| Retroperitoneal | 2323 (20.81) | 0.22 (0.21–0.23) * | 8203 (21.88) | 0.22 (0.21–0.22) * |
| Other sites | 4308 (38.60) | 0.42 (0.41–0.43) | 14,528 (38.74) | 0.39 (0.38–0.40) |
| SEER | CNPCR | |||
|---|---|---|---|---|
| Total % change | Annual % change (95% CI) | Total % change | Annual % change (95% CI) | |
| All cases | 27.16 | 1.77 (1.21–2.33) | 18.95 | 1.43 (1.12–1.74) |
| Sex | ||||
| Males | 31.53 | 1.87 (1.37–2.37) | 21.77 | 1.67 (1.34–2.00) |
| Females | 19.95 | 1.47 (0.68–2.27) | 12.57 | 0.89 (0.51–1.26) |
| Race/ethnicity | ||||
| Whites | 26.14 | 1.69 (1.01–2.37) | 19.33 | 1.40 (1.06–1.74) |
| Blacks | 14.01 | 1.62 (0.00–3.29) | 4.38 | 0.88 (0.02–1.76) |
| Other | 48.13 | 3.16 (1.74–4.60) | 30.35 | 2.68 (1.69–3.68) |
| Site | ||||
| Extremities | 2.80 | 1.07 (0.29–1.87) | 2.89 | 0.58 (0.18–0.98) |
| Retroperitoneal | 28.22 | 1.36 (0.34–2.40) | 26.03 | 1.94 (1.40–2.49) |
| Other | 64.23 | 2.69 (1.85–3.53) | 34.41 | 2.02 (1.57–2.48) |
| Relative Survival, % (95% CI) | |
|---|---|
| All cases | 79.8 (78.6–80.9) |
| Sex | |
| Male | 79.0 (77.5–80.4) |
| Female | 81.0 (79.2–82.6) |
| Race | |
| White | 79.5 (78.2–80.8) |
| Black | 80.9 (76.8–84.3) |
| Other | 80.9 (77.1–84.1) |
| Histological type | |
| Well-differentiated | 95.5 (93.6–96.9) |
| Myxoid | 85.7 (83.5–87.7) |
| Pleomorphic | 64.1 (59.1–68.7) |
| Dedifferentiated | 57.2 (54.0–60.3) |
| Other | 75.0 (72.4–77.4) |
| Site | |
| Retroperitoneal | 63.9 (61.0 – 66.7) |
| Extremities | 89.9 (88.4–91.3) |
| Other | 76.7 (74.7–78.6) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bock, S.; Hoffmann, D.G.; Jiang, Y.; Chen, H.; Il’yasova, D. Increasing Incidence of Liposarcoma: A Population-Based Study of National Surveillance Databases, 2001–2016. Int. J. Environ. Res. Public Health 2020, 17, 2710. https://doi.org/10.3390/ijerph17082710
Bock S, Hoffmann DG, Jiang Y, Chen H, Il’yasova D. Increasing Incidence of Liposarcoma: A Population-Based Study of National Surveillance Databases, 2001–2016. International Journal of Environmental Research and Public Health. 2020; 17(8):2710. https://doi.org/10.3390/ijerph17082710
Chicago/Turabian StyleBock, Suzanne, Douglas G. Hoffmann, Yi Jiang, Hao Chen, and Dora Il’yasova. 2020. "Increasing Incidence of Liposarcoma: A Population-Based Study of National Surveillance Databases, 2001–2016" International Journal of Environmental Research and Public Health 17, no. 8: 2710. https://doi.org/10.3390/ijerph17082710