Using Photo Stories to Support Doctor-Patient Communication: Evaluating a Communicative Health Literacy Intervention for Older Adults

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
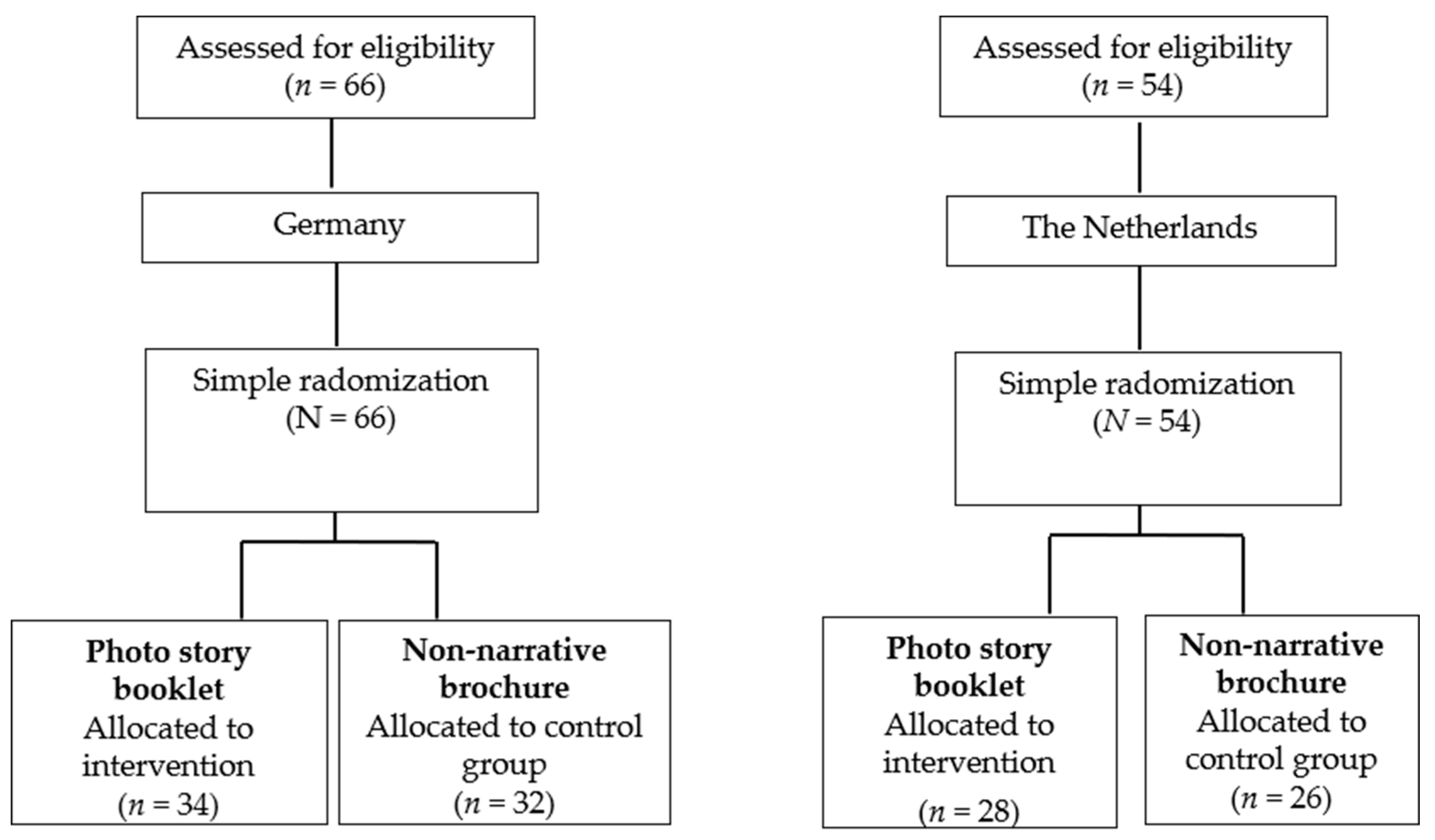
2.3. RCTs: Randomization
2.4. Intervention: Photo Story Booklet
2.5. Control Condition: Non-Narrative Brochure
2.6. Procedure
2.7. Measures
2.7.1. Primary Outcomes in the RCTs
2.7.2. Preferences as Additional Outcomes in the In-depth Interview Study in the Netherlands
2.8. Analyses
2.8.1. RCTs
2.8.2. In-depth Interview Study in the Netherlands
3. Results
3.1. RCTs: Participants
3.2. RCT in Germany: Outcomes
3.3. RCT in the Netherlands: Outcomes
3.4. In-depth Interview Study in the Netherlands: Participants
3.5. In-depth Interview Study in the Netherlands: Outcomes
Explanations for Preference
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Al Saya, F.; Majumdar, S.R.; Williams, B.; Robertson, S.; Johnson, J.A. Health literacy and health outcomes in diabetes: A systematic review. J. Gen. Int. Med. 2013, 28, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Mõttus, R.; Johnson, W.; Murray, C.; Wolf, M.S.; Starr, J.M.; Deary, I.J. Towards understanding the links between health literacy and physical health. Health Psychol. 2014, 33, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.K.; Dixon, A.; Trevena, L.; Nutbeam, D.; McCaffery, K.J. Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Soc. Sci. Med. 2009, 69, 1805–1812. [Google Scholar] [CrossRef]
- Katz, M.; Jacobson, T.; Veledar, E.; Kripalani, S. Patient literacy and question-asking behavior during the medical encounter: A mixed-methods analysis. J. Gen. Int. Med. 2007, 22, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Driever, E.M.; Stiggelbout, A.M.; Brand, P.L.P. Shared Decision Making: Physicians’ preferred role, usual role and their perception of its key components. Patient Edu. Couns. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Williams, M.V.; Davis, T.; Parker, R.M.; Weiss, B.D. The role of health literacy in patient-physician communication. Family Med. 2002, 34, 383–389. [Google Scholar]
- Joosten, E.A.G.; DeFuentes-Merillas, L.; De Weert, G.H.; Sensky, T.; Van der Staak, C.P.F.; Jong, C.A.J. Systematic Review of the Effects of Shared Decision-Making on Patient Satisfaction, Treatment Adherence and Health Status. Psychother. Psychosom. 2008, 77, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.A. Effective physician-patient communication and health outcomes: A review. Can. Med. Assoc. J. 1995, 152, 1423–1433. [Google Scholar]
- Zamora, H.; Clingerman, E.M. Health literacy among older adults: A systematic literature review. J. Gerontol. Nurs. 2011, 37, 41–51. [Google Scholar]
- National Cancer Institute. Health Information National Trends Survey 2006. Available online: http://hits.cancer.gov/ (accessed on 8 December 2016).
- Chaudhuri, S.; Le, T.; White, C.; Thompson, H.; Demiris, G. Examining health information-seeking behaviors of older adults. Cin. Comput. Inform. Nu. 2013, 31, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Paech, J.; Lippke, S. Health literacy as a key to healthy ageing in Europe. Eur. Health Psychol. 2015, 17, 67–71. [Google Scholar]
- Koops van ’t Jagt, R.; Hoeks, J.C.J.; Jansen, C.J.M.; De Winter, A.F.; Reijneveld, S.A. Comprehensibility of health related documents for older adults: A systematic review. J. Health Commun. 2016, 21, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Henselmans, I.; Heijmans, M.; Rademakers, J.; Van Dulmen, S. Participation of chronic patients in medical consultations: Patients’ perceived efficacy, barriers and interest in support. Health Expect. 2014, 18, 2375–2388. [Google Scholar] [CrossRef] [PubMed]
- Muscat, D.M.; Morony, S.; Shepherd, H.L.; Smith, S.K.; Dhillon, H.M.; Trevena, L.; McCaffery, K. Development and field testing of a consumer shared decision-making training program for adults with low literacy. Patient Edu. Couns. 2015, 98, 1180–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koops van ’t Jagt, R.; Hoeks, J.C.J.; Duizer, E.; Baron, M.; Molina, G.B.; Unger, J.B.; Jansen, C.J.M. Sweet Temptations: How does reading a fotonovela about diabetes affect Dutch adults with different levels of literacy? Health Commun. 2018, 33, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Boyte, R.M.; Pilisuk, T.; Matiella, A.C.; Macario, E. Developing a bilingual fotonovela to encourage human papillomavirus preteen immunization in California: A case study. Calif. J. Health Promot. 2014, 12, 1–13. [Google Scholar] [CrossRef]
- Davis, B.; Jansen, C. Using a fotonovela to battle chrystal meth in South Africa. J. Ethn. Subst. Abuse 2019, 1–19. [Google Scholar] [CrossRef] [PubMed]
- James, S.; Reddy, P.S.; Ruiter, R.A.C.; Taylor, M.; Jinabhai, C.C.; Van Empelen, P.; Van Den Borne, B. The effects of a systematically developed photo-novella on knowledge, attitudes, communication and behavioral intentions with respect to sexually transmitted infections among secondary school learners in South Africa. Health Promot. Int. 2005, 20, 157–165. [Google Scholar] [CrossRef]
- Kaur, N. Impact of photonovel interventions among people with low levels of health literacy: A rapid review. Edu. Inf. 2018, 35, 1–14. [Google Scholar] [CrossRef]
- Unger, J.B.; Cabassa, L.J.; Molina, G.B.; Contreras, S.; Baron, M. Evaluation of a fotonovela to increase depression knowledge and reduce stigma among Hispanic adults. J. Immigr. Minor. Health 2013, 15, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.B.; Molina, G.B.; Baron, M. Evaluation of Sweet Temptations, a fotonovela for diabetes education. Hisp. Health Care Int. 2009, 7, 145–152. [Google Scholar] [CrossRef]
- Mayer, R.E. The Cambridge handbook of multimedia learning; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Mayer, R.E.; Sims, V.K. For whom is a picture worth a thousand words? Extensions of a dual-coding theory of multimedia learning. J. Edu. Psychol. 1994, 86, 389. [Google Scholar] [CrossRef]
- Sweller, J.; Ayres, P.; Kalyuga, S. Cognitive Load Theory; Springer: New York, NY, USA, 2011. [Google Scholar]
- Moyer-Gusé, E.; Dale, K. Narrative persuasion theories. In The International Encyclopedia of Media Effects; Rössler, P., Hoffner, C.A., van Zoonen, L., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 1345–1355. [Google Scholar] [CrossRef]
- Moyer-Gusé, E. Toward a theory of entertainment persuasion: Explaining the persuasive effects of entertainment-education messages. Commun. Theor. 2008, 18, 407–425. [Google Scholar] [CrossRef]
- Slater, M.D.; Rouner, D. Entertainment-education and elaboration likelihood: Understanding the processing of narrative persuasion. Commun. Theor. 2002, 12, 173–191. [Google Scholar]
- Ryan, M.-L. Toward a definition of narrative. In The Cambridge companion to narrative; Herman, D., Ed.; Cambridge University Press: Cambridge, UK, 2007; pp. 22–35. [Google Scholar]
- Hinyard, L.J.; Kreuter, M.W. Using narrative communication as a tool for health behavior change: A conceptual, theoretical, and empirical overview. Health Edu.cation Behav. 2007, 34, 777–792. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Learning Theory; General Learning Press: New York, NY, USA, 1971. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social foundations of thought and action: A social cognitive theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Bandura, A. Self-efficacy in health functioning. In Cambridge handbook of psychology, health and medicine, 2nd ed.; Ayers, S., Baum, A., McManus, C., Newman, S., Wallston, K., Weinman, J., West, R., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 191–193. [Google Scholar]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Boeijinga, A. Storybridging: A narrative approach to health promotion for Dutch truck drivers. Ph.D. Thesis, Radboud University Nijmegen, Nijmegen, The Netherlands, 2018. [Google Scholar]
- Yzer, M. Reasoned action theory: Persuasion as belief-based behavior change. In The Sage handbook of persuasion: Developments in theory and practice, 2nd ed.; Dillard, J.P., Shen, L., Eds.; Sage: Los Angeles, CA, USA, 2013; pp. 120–136. [Google Scholar]
- Fransen, M.L.; Smit, E.G.; Verlegh, P.W.J. Strategies and motives for resistance to persuasion: An integrative framework. Front. Psychol. 2015, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Koops van ’t Jagt, R.; De Winter, A.F.; Reijneveld, S.A.; Hoeks, J.C.J.; Jansen, C.J.M. Development of a Communication Intervention for Older Adults with Limited Health Literacy: Photo Stories to Support Doctor–Patient Communication. J. Health Commun. 2016, 21, 69–82. [Google Scholar] [CrossRef]
- Mar, R.A.; Oatley, K. The function of fiction is the abstraction and simulation of social experience. Perspect. Psychol. Sci. 2008, 3, 173–192. [Google Scholar] [CrossRef] [PubMed]
- Braddock, K.; Dillard, J.P. Meta-analytic evidence for the persuasive effect of narratives on beliefs, attitudes, intentions, and behaviors. Commun. Monogr. 2016, 83, 446–467. [Google Scholar] [CrossRef]
- De Graaf, A.; Sanders, J.; Hoeken, J.A.L. Characteristics of narrative interventions and health effects: A review of the content, form, and context of narratives in health-related narrative persuasion research. Rev. Commun. Res. 2016, 4, 88–131. [Google Scholar]
- Shen, F.Y.; Sheer, V.C.; Li, R.B. Impact of narratives on persuasion in health communication: A meta-analysis. J. Advert. 2015, 44, 105–113. [Google Scholar] [CrossRef]
- McGuire, W.J. Attitude change: The information-processing paradigm. In Experimental Social Psychology; McClintock, C.G., Ed.; Holt, Rinehart & Winston: New York, NY, USA, 1972; pp. 108–141. [Google Scholar]
- Tan, S.L.; Whittal, A.; Lippke, S. Testing a photo story intervention in paper versus electronic tablet format compared to a traditional non-narrative brochure among older adults in Germany: Randomized controlled trial. JMIR Aging 2018, 1, e12145. [Google Scholar] [CrossRef] [PubMed]
- Spoorenberg, S.L.W.; Uittenbroek, R.J.; Middel, B.; Kremer, B.P.H.; Reijneveld, S.A.; Wynia, K. Embrace, a model for integrated elderly care: Study protocol of a randomized controlled trial on the effectiveness regarding patient outcomes, service use, costs, and quality of care. BMC Geriatrics 2013, 13, 62. [Google Scholar] [CrossRef]
- Clayman, M.L.; Pandit, A.U.; Bergeron, A.R.; Cameron, K.A.; Ross, E.; Wolf, M.S. Ask, understand, remember: A brief measure of patient communication self-efficacy within clinical encounters. J. Health Commun. 2010, 15, 72–79. [Google Scholar] [CrossRef]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Family Med. 2004, 26, 588–594. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A.G. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Ritchie, J.; Spencer, L.; O’Connor, W. Carrying out qualitative analysis. In Qualitative research practice: A guide for social science students and researchers; Ritchie, J., Lewis, J., Eds.; Sage: London, UK, 2003; pp. 219–262. [Google Scholar]
- McGuire, W.J. An information-processing model of advertising effectiveness. In Behavioral and Management Sciences in Marketing; Davis, H.L., Silk, A.J., Eds.; Ronald: New York, NY, USA, 1978; pp. 156–180. [Google Scholar]
- Petty, R.E.; Cacioppo, J.T. The effects of involvement on responses to argument quantity and quality: Central and peripheral routes to persuasion. J. Pers. Soc. Psychol. 1984, 46, 69–81. [Google Scholar] [CrossRef]
- Petty, R.E.; Cacioppo, J.T. Attitudes and Persuasion: Classic and Contemporary Approaches; Westview: Boulder, CO, USA, 1996. [Google Scholar]
- Geboers, B.; Reijneveld, S.A.; Jansen, C.J.M.; De Winter, A.F. Health literacy is associated with health behaviors and social factors among older adults: Results from the LifeLines Cohort Study. J. Health Commun. 2016, 21, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Ooms, J.; Jansen, C.; Hoeks, J. The story against smoking: An exploratory study into the processing and perceived effectiveness of narrative visual smoking warnings. Health Edu. J. 2019. [Google Scholar] [CrossRef]
- Lippke, S.; Ziegelmann, J.P.; Schwarzer, R. Behavioral intentions and action plans promote physical exercise: A longitudinal study with orthopedic rehabilitation patients. J. Sport Exerc. Psychol. 2004, 26, 470–483. [Google Scholar] [CrossRef]
- Boeijinga, A.; Hoeken, H.; Sanders, J.M. From intention to behavior: Dutch truck drivers’ road to healthy lifestyle changes. Work 2016, 55, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Gollwitzer, P.M.; Sheeran, P. Implementation intentions and goal achievement: A meta-analysis of effects and processes. Adv. Exp. Soc. Psycho. 2006, 38, 69–119. [Google Scholar]
- Geboers, B.; Reijneveld, S.A.; Koot, J.A.R.; De Winter, A.F. Moving towards a comprehensive approach for health literacy interventions: The development of a health literacy intervention model. Int. J. Environ. Res. Public Health 2018, 15, 1268. [Google Scholar] [CrossRef] [PubMed]
- Fennis, B.M.; Adriaanse, M.A.; Stroebe, W.; Pol, B. Bridging the intention-behavior gap: Inducing implementation intentions through persuasive appeals. J. Consum. Psychol. 2011, 21, 302–311. [Google Scholar] [CrossRef]
- Knauper, B.; Roseman, M.; Johnson, P.J.; Krantz, L.H. Using mental imagery to enhance the effectiveness of implementation intentions. Curr. Psychol. 2009, 28, 181–186. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage Publications Ltd.: London, UK, 2009. [Google Scholar]
- Hoeken, H. Wat leert onderzoek naar overtuigende teksten over het ontwerpen van overtuigender teksten? Een overzicht van meta-analytische studies [What does research into persuasive texts tell us about designing texts that are more persuasive? An overview of meta-analytic studies]. Tijdschrift voor Taalbeheersing 2019, 41, 105–128. [Google Scholar]
- Schwarz, N. Self-Reports. How the questions shape the answers. Am. Psychol. 1999, 54, 93–105. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Germany | The Netherlands | |||||
|---|---|---|---|---|---|---|
| Photo Story Booklet (n = 34) | Non-Narrative Brochure (n = 32) | Total (N = 66) | Photo Story Booklet (n = 28) | Non-Narrative Brochure (n = 26) | Total (N = 54) | |
| Gender (female) | 24 | 22 | 46 | 19 | 16 | 35 |
| Age | 73.2 (5.4) | 76.8 (8.5) | 75.0 (7.2) | 82.1 (2.7) | 83.6 (4.1) | 82.8 (3.5) |
| Age (range) | 62−80 | 54−94 | 54−94 | 77−88 | 79−95 | 77−95 |
| Education (estimated in years) | 10.74 (2.03) | 10.72 (2.26) | 10.73 (2.13) | 8.96 (2.81) | 8.69 (2.99) | 8.83 (2.88) |
| Health (1 poor−5 excellent) | 3.33 (0.85) | 3.28 (0.96) | 3.31 (0.90) | 2.32 (0.86) | 2.31 (0.62) | 2.31 (0.75) |
| Visiting frequency general practitioner (GP) (1 less than once a year–6 at least once a week) | 2.62 (0.99) | 2.66 (0.97) | 2.64 (0.97) | 2.50 (1.07) | 2.04 (1.04) | 2.28 (1.07) |
| Health communication self-efficacy (AURA) (4 minimum−20 maximum) | 15.76 (3.64) | 16.22 (2.90) | 15.98 (3.29) | 15.79 (3.79) | 17.35 (2.65) | 16.54 (3.35) |
| Health Literacy (SBSQ) (0 minimum−12 maximum) | 7.61 (2.28) | 7.81 (2.24) | 7.71 (2.24) | 8.74 (2.98) | 8.58 (3.08) | 8.66 (3.00) |
| Photo Story Booklet | Non-Narrative Brochure | |||||
|---|---|---|---|---|---|---|
| Low HL | Medium HL | High HL | Low HL | Medium HL | High HL | |
| Self-Efficacy | 3.98 (0.68) | 3.63 (1.01) | 4.09 (0.69) | 3.71 (0.88) | 4.03 (0.71) | 4.04 (0.63) |
| Intention | 4.02 (0.78) | 3.96 (0.87) | 4.55 (0.62) | 4.36 (0.37) | 4.20 (0.72) | 4.37 (0.53) |
| Photo Story Booklet | Non-Narrative Brochure | |||
|---|---|---|---|---|
| Low HL | High HL | Low HL | High HL | |
| Self-Efficacy | 3.65 (0.78) | 4.22 (0.82) | 3.82 (0.74) | 4.71 (0.31) |
| Intention | 3.63 (0.69) | 4.23 (0.90) | 3.88 (0.60) | 4.59 (0.40) |
| Photo Story Booklet (n = 24) | Non-Narrative Brochure (n = 20) | Total (N = 44) | |
|---|---|---|---|
| Gender (female) | 16 | 13 | 29 |
| Age | 82.3 (2.7) | 84.2 (4.5) | 83.2 (3.7) |
| Age (range) | 79−88 | 79−95 | 79−95 |
| Education (estimated in years) | 8.86 (2.90) | 9.00 (3.23) | 8.93 (3.02) |
| Health (1 poor−5 excellent) | 2.38 (0.88) | 2.25 (0.64) | 2.32 (0.77) |
| Visiting frequency GP (1 less than once a year−6 at least once a week) | 2.50 (1.10) | 2.15 (1.09) | 2.34 (1.10) |
| Health communication self-efficacy (AURA) (4 minimum−20 maximum) | 15.92 (3.80) | 16.95 (2.82) | 16.39 (3.39) |
| Health Literacy (SBSQ) (0 minimum−12 maximum) | 8.71 (2.90) | 8.50 (3.46) | 8.61 (3.13) |
| Photo Story Booklet | Non-Narrative Brochure | |||
|---|---|---|---|---|
| Number of Mentions | Illustrative Quotes | Number of Mentions | Illustrative Quotes | |
| (Q1) Why does the respondent consider the photo story booklet or the non-narrative brochure to be the best? | ||||
| Topic: Attention and motivation | ||||
| Attractiveness | 6 | ‘That one speaks to me more, it’s more pleasant.’ ‘I already know I like that one better, it’s more playful, I like it a lot more.’ | 1 | ‘This one is nicer of course… I think.’ |
| Topic: Comprehension | ||||
| Elaborateness | 10 | ‘That one has more information.’ ‘In that one it’s explained a bit more.’ | 0 | |
| Clearness | 15 | ‘It’s very clear and the situations are explained very well.’ ‘The way it’s written makes everything very clear.’ ‘This is very clear and easy to understand, because of the stories.’ | 1 | ‘It’s clear.’ |
| Comprehensibility | 2 | ‘It’s written in a simple style.’ ‘This one reads quicker.’ | 4 | ‘Well that one’s a bit shorter.’ ‘If there’s one thing I hate it’s having to read a lot.’ ‘That one’s more to the point.’ |
| Recognizability/relevance | 4 | ‘In that one you see pictures. Like it is in daily life.’ ‘No, it’s all really familiar and recognizable for me.’ | 0 | |
| Topic: Action | ||||
| Mental processing | 1 | ‘This one has more pictures, it’s much more visual.’ | 0 | |
| Emotional appeal | 3 | ‘Uhm, it gets to you more. It speaks to you.’ | 0 | |
| Behavioral appeal | 1 | ‘You respond to this one quicker.’ | 0 | |
| (Q2) Why does the respondent want to take the photo story booklet or the non-narrative brochure home? | ||||
| Topic: Attention and motivation | ||||
| Attractiveness | 4 | ‘Well that’s a pretty little book.’ ‘That one’s fun to read.’ | 0 | |
| Topic: Comprehension | ||||
| Elaborateness | 11 | ‘Because there’s more to read in that one.’ ‘That one is just a little more elaborate.’ | 0 | |
| Clearness | 5 | ‘Clear example situations.’ ‘Clear information.’ ‘Easy to understand.’ | 0 | |
| Comprehensibility | 3 | ‘That one’s easier to read, I think.’ | 2 | ‘Because this one is simpler. They put it in a way I can really understand it.’ |
| Recognizability/relevance | 2 | ’And, well, those questions, they are very identifiable. When you’re at the doctors.’ ‘Because there are so many things in there that are recognizable to me.’ | 0 | |
| Topic: Action | ||||
| Mental processing | 2 | ‘And if you look at those examples, it’s easier to remember.’ ‘That one makes you think more, I guess.’ | 0 | |
| Emotional appeal | 2 | ‘Because you, how do I explain this, can sympathize with that one more easily.’ ‘You really feel this one.’ | 0 | |
| Behavioral appeal | 1 | ‘You get more out of that one.’ | 0 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koops van ‘t Jagt, R.; Tan, S.L.; Hoeks, J.; Spoorenberg, S.; Reijneveld, S.A.; de Winter, A.F.; Lippke, S.; Jansen, C. Using Photo Stories to Support Doctor-Patient Communication: Evaluating a Communicative Health Literacy Intervention for Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 3726. https://doi.org/10.3390/ijerph16193726
Koops van ‘t Jagt R, Tan SL, Hoeks J, Spoorenberg S, Reijneveld SA, de Winter AF, Lippke S, Jansen C. Using Photo Stories to Support Doctor-Patient Communication: Evaluating a Communicative Health Literacy Intervention for Older Adults. International Journal of Environmental Research and Public Health. 2019; 16(19):3726. https://doi.org/10.3390/ijerph16193726
Chicago/Turabian StyleKoops van ‘t Jagt, Ruth, Shu Ling Tan, John Hoeks, Sophie Spoorenberg, Sijmen A. Reijneveld, Andrea F. de Winter, Sonia Lippke, and Carel Jansen. 2019. "Using Photo Stories to Support Doctor-Patient Communication: Evaluating a Communicative Health Literacy Intervention for Older Adults" International Journal of Environmental Research and Public Health 16, no. 19: 3726. https://doi.org/10.3390/ijerph16193726