Differences in Prenatal Tobacco Exposure Patterns among 13 Race/Ethnic Groups in California

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Cotinine Analysis
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- US Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014.
- Mund, M.; Louwen, F.; Klingelhoefer, D.; Gerber, A. Smoking and Pregnancy—A Review on the First Major Environmental Risk Factor of the Unborn. Int. J. Environ. Res. Public Health 2013, 10, 6485–6499. [Google Scholar] [CrossRef] [PubMed]
- Tong, V.T.; Dietz, P.M.; Morrow, B.; D’Angelo, D.V.; Farr, S.L.; Rockhill, K.M.; England, L.J.; Centers for Disease Control and Prevention (CDC). Trends in smoking before, during, and after pregnancy—Pregnancy Risk Assessment Monitoring System, United States, 40 sites, 2000–2010. MMWR Surveill. Summ. 2013, 62, 1–19. [Google Scholar] [PubMed]
- Pineles, B.L.; Park, E.; Samet, J.M. Systematic Review and Meta-Analysis of Miscarriage and Maternal Exposure to Tobacco Smoke During Pregnancy. Am. J. Epidemiol. 2014, 179, 807–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, K.; Xu, X.; Liu, X.; Wang, X.; Hua, S.; Wang, C.; Liu, X. The Associations Between Maternal Factors During Pregnancy and the Risk of Childhood Acute Lymphoblastic Leukemia: A Meta-Analysis. Pediatr. Blood Cancer 2015, 62, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Spindel, E.R. Pulmonary Effects of Maternal Smoking on the Fetus and Child: Effects on Lung Development, Respiratory Morbidities, and Life Long Lung Health. Paediatr. Respir. Rev. 2017, 21, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibbs, K.; Collaco, J.M.; McGrath-Morrow, S.A. Impact of Tobacco Smoke and Nicotine Exposure on Lung Development. Chest 2016, 149, 552–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banderali, G.; Martelli, A.; Landi, M.; Moretti, F.; Betti, F.; Radaelli, G.; Lassandro, C.; Verduci, E. Short and long term health effects of parental tobacco smoking during pregnancy and lactation: A descriptive review. Transl. Med. 2015, 13, 327. [Google Scholar] [CrossRef]
- Zhang, D.; Cui, H.; Zhang, L.; Huang, Y.; Zhu, J.; Li, X. Is maternal smoking during pregnancy associated with an increased risk of congenital heart defects among offspring? A systematic review and meta-analysis of observational studies. J. Matern. Fetal Neonatal Med. 2017, 30, 645–657. [Google Scholar] [CrossRef]
- Dietz, P.M.; England, L.J.; Shapiro-Mendoza, C.K.; Tong, V.T.; Farr, S.L.; Callaghan, W.M. Infant Morbidity and Mortality Attributable to Prenatal Smoking in the U.S. Am. J. Prev. Med. 2010, 39, 45–52. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General Office on Smoking and Health (US); U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006.
- Leonardi-Bee, J.; Britton, J.; Venn, A. Secondhand Smoke and Adverse Fetal Outcomes in Nonsmoking Pregnant Women: A Meta-analysis. Pediatrics 2011, 127, 734–741. [Google Scholar] [CrossRef]
- Kharrazi, M.; DeLorenze, G.N.; Kaufman, F.L.; Eskenazi, B.; Bernert, J.T., Jr.; Graham, S.; Pearl, M.; Pirkle, J. Environmental Tobacco Smoke and Pregnancy Outcome. Epidemiology 2004, 15, 660–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuijsen, M.J.; Dadvand, P.; Grellier, J.; Martinez, D.; Vrijheid, M. Environmental risk factors of pregnancy outcomes: A summary of recent meta-analyses of epidemiological studies. Environ. Health 2013, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Burke, H.; Leonardi-Bee, J.; Hashim, A.; Pine-Abata, H.; Chen, Y.; Cook, D.G.; Britton, J.R.; McKeever, T.M. Prenatal and Passive Smoke Exposure and Incidence of Asthma and Wheeze: Systematic Review and Meta-analysis. Pediatrics 2012, 129, 735–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayfield, S.; Plugge, E. Systematic review and meta-analysis of the association between maternal smoking in pregnancy and childhood overweight and obesity. J. Epidemiol. Community Health 2017, 71, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Daniels, J.L.; Poole, C.; Olshan, A.F.; Hornung, R.; Bernert, J.T.; Khoury, J.; Needham, L.L.; Barr, D.B.; Lanphear, B.P. Prenatal environmental tobacco smoke exposure and early childhood body mass index. Paediatr. Perinat. Epidemiol. 2010, 24, 524–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durmus, B.; Kruithof, C.J.; Gillman, M.H.; Willemsen, S.P.; Hofman, A.; Raat, H.; Eilers, P.H.; Steegers, E.A.; Jaddoe, V.W. Parental smoking during pregnancy, early growth, and risk of obesity in preschool children: The Generation R Study. Am. J. Clin. Nutr. 2011, 94, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Clifford, A.; Lang, L.; Anstey, K.J. Is exposure to secondhand smoke associated with cognitive parameters of children and adolescents?—A systematic literature review. Ann. Epidemiol. 2013, 23, 652–661. [Google Scholar] [CrossRef]
- Dick, S.; Friend, A.; Dynes, K.; AlKandari, F.; Doust, E.; Cowie, H.; Ayres, J.G.; Turner, S.W. A systematic review of associations between environmental exposures and development of asthma in children aged up to 9 years. BMJ Open 2014, 4, e006554. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Wang, X. Maternal smoking and increased risk of sudden infant death syndrome: A meta-analysis. Leg. Med. 2013, 15, 115–121. [Google Scholar] [CrossRef]
- Treyster, Z.; Gitterman, B. Second hand smoke exposure in children: Environmental factors, physiological effects, and interventions within pediatrics. Rev. Environ. Health 2011, 26, 187–195. [Google Scholar] [CrossRef]
- Raghuveer, G.; White, D.A.; Hayman, L.L.; Woo, J.G.; Villafane, J.; Celermajer, D.; Ward, K.D.; de Ferranti, S.D.; Zachariah, J. Cardiovascular Consequences of Childhood Secondhand Tobacco Smoke Exposure: Prevailing Evidence, Burden, and Racial and Socioeconomic Disparities: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e336–e359. [Google Scholar] [CrossRef] [PubMed]
- Ladd-Acosta, C.; Shu, C.; Lee, B.K.; Gidaya, N.; Singer, A.; Schieve, L.A.; Schendel, D.E.; Jones, N.; Daniels, J.L.; Windham, G.C.; et al. Presence of an epigenetic signature of prenatal cigarette smoke exposure in childhood. Environ. Res. 2016, 144, 139–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ncube, C.N.; Mueller, B.A. Daughters of Mothers Who Smoke: A Population-based Cohort Study of Maternal Prenatal Tobacco use and Subsequent Prenatal Smoking in Offspring. Paediatr. Perinat. Epidemiol. 2017, 31, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Vandewater, E.A.; Park, S.E.; Carey, F.R.; Wilkinson, A.V. Intergenerational Transfer of Smoking Across Three Generations and Forty-five Years. Nicotine Tob. Res. 2014, 16, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Dietz, P.M.; Homa, D.; England, L.J.; Burley, K.; Tong, V.T.; Dube, S.R.; Bernert, J.T. Estimates of Nondisclosure of Cigarette Smoking Among Pregnant and Nonpregnant Women of Reproductive Age in the United States. Am. J. Epidemiol. 2011, 173, 355–359. [Google Scholar] [CrossRef] [PubMed]
- DeLorenze, G.N.; Kharrazi, M.; Kaufman, F.L.; Eskenazi, B.; Bernert, J.T. Exposure to environmental tobacco smoke in pregnant women: The association between self-report and serum cotinine. Environ. Res. 2002, 90, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, F.L.; Kharrazi, M.; Delorenze, G.N.; Eskenazi, B.; Bernert, J.T. Estimation of environmental tobacco smoke exposure during pregnancy using a single question on household smokers versus serum cotinine. J. Expo. Sci. Environ. Epidemiol. 2002, 12, 286–295. [Google Scholar] [CrossRef] [Green Version]
- Woodruff, T.J.; Zota, A.R.; Schwartz, J.M. Environmental Chemicals in Pregnant Women in the United States: NHANES 2003–2004. Environ. Health Perspect. 2011, 119, 878–885. [Google Scholar] [CrossRef] [Green Version]
- Child Trends Databank. Mothers Who Smoke While Pregnant. Available online: http://www.childtrends.org/?indicators=mothers-who-smoke-while-pregnant (accessed on 1 October 2018).
- Washio, Y.; Cassey, H. Systematic Review of Interventions for Racial/Ethnic-Minority Pregnant Smokers. J. Smok. Cessat. 2016, 11, 12–27. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Cohen, B.B.; Hawkins, S.S.; Cohen, B.B. Affordable Care Act standards for race and ethnicity mask disparities in maternal smoking during pregnancy. Prev. Med. 2014, 65, 92–95. [Google Scholar] [CrossRef] [Green Version]
- Hoeffel, E.M.; Rastogi, S.; Kim, M.O.; Shahid, H. 2010 Census Briefs, The Asian Population: 2010; U.S. Census Bureau, U.S. Department of Commerce: Washington, DC, USA, 2012.
- Centers for Disease Control and Prevention (CDC). Current cigarette smoking among adults—United States, 2011. Morb. Mortal. Wkly. Rep. 2012, 61, 889–894. [Google Scholar]
- Cunningham, G.C.; Tompkinison, D.G. Cost and effectiveness of the California triple marker prenatal screening program. Genet. Med. 1999, 1, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Steinmaus, C.; Pearl, M.; Kharrazi, M.; Blount, B.C.; Miller, M.D.; Pearce, E.N.; Valentin-Blasini, L.; DeLorenze, G.; Hoofnagle, A.N.; Liaw, J. Thyroid Hormones and Moderate Exposure to Perchlorate during Pregnancy in Women in Southern California. Environ. Health Perspect. 2016, 124, 861–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernert, J.T., Jr.; Turner, W.E.; Pirkle, J.L.; Sosnoff, C.S.; Akins, J.R.; Waldrep, M.K.; Ann, Q.; Covey, T.R.; Whitfield, W.E.; Gunter, E.W.; et al. Development and validation of sensitive method for determination of serum cotinine in smokers and nonsmokers by liquid chromatography/atmospheric pressure ionization tandem mass spectrometry. Clin. Chem. 1997, 43, 2281–2291. [Google Scholar]
- Benowitz, N.L.; Bernert, J.T.; Caraballo, R.S.; Holiday, D.B.; Wang, J. Optimal Serum Cotinine Levels for Distinguishing Cigarette Smokers and Nonsmokers Within Different Racial/Ethnic Groups in the United States Between 1999 and 2004. Am. J. Epidemiol. 2008, 169, 236–248. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Tsoh, J.Y.; Grigg-Saito, D.; Tucker, P.; Liao, Y. Decreased Smoking Disparities Among Vietnamese and Cambodian Communities—Racial and Ethnic Approaches to Community Health (REACH) Project, 2002–2006. MMWR Surveill. Summ. 2014, 63, 37–45. [Google Scholar]
- Webber, W.L.; Van Erp, B.; Stoddard, P.; Tsoh, J.Y. Determinants of Exposure to Secondhand Smoke Among Vietnamese Adults: California Vietnamese Adult Tobacco Use Survey, 2007–2008. Prev. Chronic Dis. 2014, 11, E81. [Google Scholar] [CrossRef]
- Petersen, A.B.; Tsoh, J.Y.; Nguyen, T.T.; McPhee, S.J.; Burke, N.J. Suffering in Silence: Impact of Tobacco Use on Communication Dynamics Within Vietnamese and Chinese Immigrant Families. J. Fam. Nurs. 2016, 22, 108–132. [Google Scholar] [CrossRef]
- Pokhrel, P.; Fagan, P.; Cassel, K.; Trinidad, D.R.; Kaholokula, J.K.; Herzog, T.A. Social Network Characteristics, Social Support, and Cigarette Smoking among Asian/Pacific Islander Young Adults. Am. J. Community Psychol. 2016, 57, 353–365. [Google Scholar] [CrossRef] [Green Version]
- Noah, A.J.; Landale, N.S.; Sparks, C.S. How Does the Context of Reception Matter? The Role of Residential Enclaves in Maternal Smoking During Pregnancy Among Mexican-Origin Mothers. Matern. Child Health J. 2015, 19, 1825–1833. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.C.; Shoff, C.; Noah, A.J.; Black, N.; Sparks, C.S. Racial segregation and maternal smoking during pregnancy: A multilevel analysis using the racial segregation interaction index. Soc. Sci. Med. 2014, 107, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Center for Public Health Systems Science at Washington University in St. Louis; Tobacco Control Legal Consortium. Point-of-Sale Strategies: A Tobacco Control Guide; Public Health Law Center at Mitchell Hamline School of Law: St Paul, MN, USA, 2014. [Google Scholar]
- U.S. Department of Health and Human Services. Tobacco Use Among U.S. Racial/Ethnic Minority Groups—African Americans, American Indians and Alaska Natives, Asian Americans and Pacific Islanders, and Hispanics: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 1998.
- Herzog, T.A.; Pokhrel, P. Ethnic differences in smoking rate, nicotine dependence, and cessation-related variables among adult smokers in Hawaii. J. Community Health 2012, 37, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Acevedo-Garcia, D.; Barbeau, E.; Bishop, J.A.; Pan, J.; Emmons, K.M. Undoing an Epidemiological Paradox: The Tobacco Industry’s Targeting of US Immigrants. Am. J. Public Health 2004, 94, 2188–2193. [Google Scholar] [CrossRef] [PubMed]
- Heo, H.H.; Braun, K.L. Culturally tailored interventions of chronic disease targeting Korean Americans: A systematic review. Ethn. Health 2014, 19, 64–85. [Google Scholar] [CrossRef] [PubMed]
- Tabb, K.M.; Huang, H.; Menezes, P.R.; Azevedo e Silva, G.; Chan, Y.F.; Faisal-Cury, A. Ethnic Differences in Tobacco Use During Pregnancy: Findings From a Primary Care Sample in São Paulo, Brazil. Ethn. Health 2015, 20, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Griner, D.; Smith, T.B. Culturally Adapted Mental Health Interventions: A Meta-Analytic Review. Psychotherapy 2006, 43, 531–548. [Google Scholar] [CrossRef]
- Levy, D.; Mohlman, M.K.; Zhang, Y. Estimating the Potential Impact of Tobacco Control Policies on Adverse Maternal and Child Health Outcomes in the United States Using the SimSmoke Tobacco Control Policy Simulation Model. Nicotine Tob. Res. 2016, 18, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Adams, E.K.; Markowitz, S.; Kannan, V.; Dietz, P.M.; Tong, V.T.; Malarcher, A.M. Reducing Prenatal Smoking: The Role of State Policies. Am. J. Prev. Med. 2012, 43, 34–40. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Baum, C.F. Impact of State Cigarette Taxes on Disparities in Maternal Smoking During Pregnancy. Am. J. Public Health 2014, 104, 1464–1470. [Google Scholar] [CrossRef] [Green Version]
- Been, J.V.; Nurmatov, U.B.; Cox, B.; Nawrot, T.S.; van Schayck, C.P.; Sheikh, A. Effect of smoke-free legislation on perinatal and child health: A systematic review and meta-analysis. Lancet 2014, 383, 1549–1560. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Baum, C.F.; Oken, E.; Gillman, M.W. Associations of Tobacco Control Policies With Birth Outcomes. JAMA Pediatr. 2014, 168, e142365. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.R.; Lotfipour, S.; Chakravarthy, B. Growing Trend of Alternative Tobacco Use Among the Nation’s Youth: A New Generation of Addicts. West. J. Emerg. Med. 2016, 17, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, D.; Jacob, P., III; Benowitz, N.L. Accelerated metabolism of nicotine and cotinine in pregnant smokers. J. Pharmacol. Exp. Ther. 2002, 301, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Pearl, M.; Wier, M.L.; Kharrazi, M. Assessing the quality of last menstrual period date on California birth records. Paediatr. Perinat. Epidemiol. 2007, 21, 50–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schick, S.F.; Blount, B.C.; Jacob, P., III; Saliba, N.A.; Bernert, J.T.; El Hellani, A.; Jatlow, P.; Pappas, R.S.; Wang, L.; Foulds, J.; et al. Biomarkers of exposure to new and emerging tobacco delivery products. Am. J. Physiol. Lung Cell. Mol. Physiol. 2017, 313, L425–L452. [Google Scholar] [CrossRef] [PubMed]
- King, B.A.; Pechacek, T.F.; Mariolis, P. Best Practices for Comprehensive Tobacco Control Programs; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014.
- Pierce, J.P.; Shi, Y.; Hendrickson, E.M.; White, M.M.; Noble, M.L.; Kealey, S.; Strong, D.R.; Trinidad, D.R.; Hartman, A.M.; Messer, K. Tobacco control in California compared with the rest of the USA: Trends in adult per capita cigarette consumption. Tob. Control 2018, 27, e112–e117. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Race/Ethnicity | N = 3014 | Column % | Mother’s Age ≤ 25 Years (%) | Mother’s Education < 16 Years (%) | Mother’s Insurance Public Funding (%) | Mother is Foreign-Born (%) |
|---|---|---|---|---|---|---|
| White | 95 | 3.2 | 20.0 | 49.5 | 14.7 | 13.7 |
| African American | 263 | 8.7 | 47.5 | 87.5 | 57.0 | 8.7 |
| Hispanic | 82 | 2.7 | 37.8 | 89.0 | 62.2 | 70.7 |
| Asian Indian | 274 | 9.1 | 11.3 | 29.2 | 11.3 | 91.6 |
| Cambodian | 274 | 9.1 | 43.1 | 82.8 | 41.2 | 90.9 |
| Chinese | 275 | 9.1 | 4.4 | 20.4 | 3.3 | 88.7 |
| Filipino | 274 | 9.1 | 17.9 | 51.8 | 14.2 | 76.6 |
| Japanese | 265 | 8.8 | 5.7 | 42.6 | 7.2 | 65.3 |
| Korean | 262 | 8.7 | 6.1 | 29.8 | 17.2 | 94.3 |
| Laotian | 280 | 9.3 | 32.9 | 81.1 | 32.9 | 90.4 |
| Native American | 213 | 7.1 | 40.4 | 85.9 | 33.8 | 8.0 |
| Samoan | 170 | 5.6 | 41.8 | 91.8 | 42.9 | 42.4 |
| Vietnamese | 287 | 9.5 | 13.2 | 74.9 | 31.4 | 98.6 |
| Chi Square p-value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
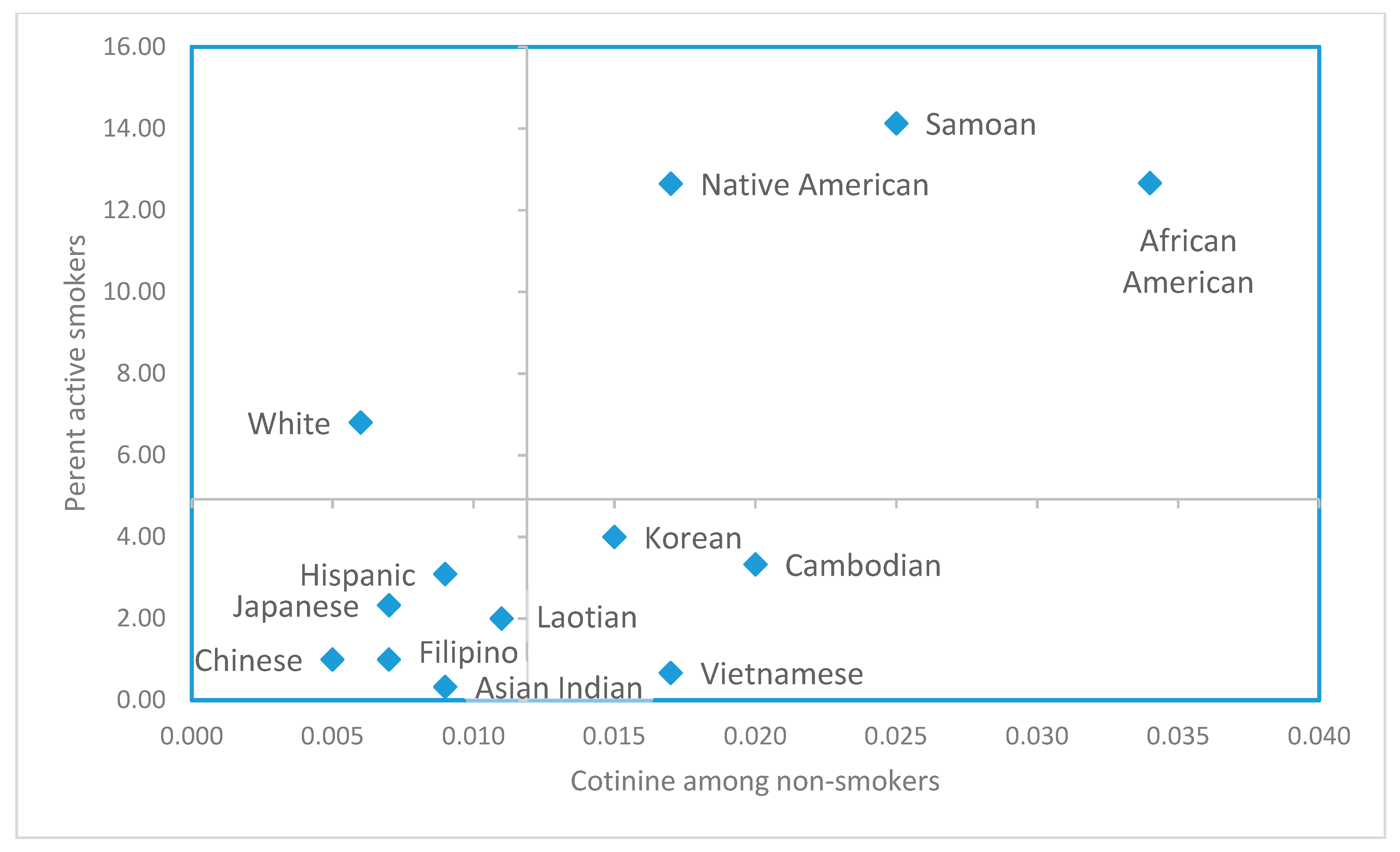
| Race-Ethnicity | No | No of Smokers * | % | 95% Confidence Interval |
|---|---|---|---|---|
| Samoan | 184 | 26 | 14.1 | 9.8–19.9 |
| African American | 300 | 38 | 12.7 | 9.4–16.9 |
| Native American | 245 | 31 | 12.7 | 9.1–17.4 |
| White | 103 | 7 | 6.8 | 3.3–13.4 |
| Korean | 300 | 12 | 4.0 | 2.3–6.9 |
| Cambodian | 300 | 10 | 3.3 | 1.8–6.0 |
| Hispanic | 97 | 3 | 3.1 | 1.1–8.7 |
| Japanese | 300 | 7 | 2.3 | 1.1–4.7 |
| Laotian | 300 | 6 | 2.0 | 0.9–4.3 |
| Filipino | 300 | 3 | 1.0 | 0.3–2.9 |
| Chinese | 300 | 3 | 1.0 | 0.3–2.9 |
| Vietnamese | 300 | 2 | 0.7 | 0.2–2.4 |
| Asian Indian | 300 | 1 | 0.3 | 0.1–1.9 |
| Race-Ethnicity † | N | % Detectable Cotinine | Geometric Mean Cotinine (ng/mL) ‡ | 95% Confidence Interval | IQR 25–75th Percentile |
|---|---|---|---|---|---|
| African American a | 262 | 90.5 | 0.034 | 0.026–0.044 | 0.009–0.151 |
| Samoan a,b | 158 | 88.0 | 0.025 | 0.018–0.034 | 0.010–0.077 |
| Cambodian b,c | 290 | 90.3 | 0.020 | 0.016–0.025 | 0.006–0.066 |
| Native American c | 214 | 84.6 | 0.017 | 0.013–0.022 | 0.004–0.058 |
| Vietnamese c | 298 | 90.3 | 0.017 | 0.014–0.020 | 0.006–0.046 |
| Korean c,d | 288 | 88.2 | 0.015 | 0.012–0.018 | 0.006–0.039 |
| Laotian d,e | 294 | 80.6 | 0.011 | 0.009–0.014 | 0.003–0.039 |
| Asian Indian e,f | 299 | 82.3 | 0.009 | 0.008–0.011 | 0.003–0.030 |
| Hispanic e,f,g | 94 | 79.8 | 0.009 | 0.006–0.012 | 0.003–0.028 |
| Filipino f,g | 297 | 75.1 | 0.007 | 0.006–0.009 | 0.001–0.030 |
| Japanese f,g,h | 293 | 75.4 | 0.007 | 0.005–0.008 | 0.001–0.020 |
| White g,h | 96 | 75.0 | 0.006 | 0.004–0.009 | 0.001–0.019 |
| Chinese h | 297 | 75.4 | 0.005 | 0.004–0.006 | 0.001–0.017 |
| Variable | Parameter Estimate (log10 Cotinine, ng/mL) ‡ | Pr > F |
|---|---|---|
| Model R2 = 0.18 | ||
| Intercept | −0.687 | 0.044 |
| Demographic covariates (as group) | <0.0001 | |
| Mother has less than 16 years of education | 0.233 | <0.0001 |
| Mother’s care is publicly funded | 0.346 | <0.0001 |
| Mother’s age (continuous) | −0.098 | <0.0001 |
| Mother’s age (squared term) | 0.001 | 0.001 |
| Race/ethnic covariates * (as group) | <0.0001 | |
| Korean | 0.429 | <0.0001 |
| African-American | 0.403 | <0.0001 |
| Samoan | 0.367 | <0.0002 |
| Vietnamese | 0.319 | 0.0004 |
| Cambodian | 0.269 | 0.0030 |
| Native American | 0.228 | 0.0165 |
| Asian Indian | 0.223 | 0.0125 |
| Japanese | 0.120 | 0.1825 |
| Laotian | 0.108 | 0.2298 |
| Chinese | 0.084 | 0.3472 |
| Filipino | 0.050 | 0.5727 |
| Hispanic | −0.207 | 0.0716 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoshiko, S.; Pearl, M.; Yang, J.; Aldous, K.M.; Roeseler, A.; Dominguez, M.E.; Smith, D.; DeLorenze, G.N.; Kharrazi, M. Differences in Prenatal Tobacco Exposure Patterns among 13 Race/Ethnic Groups in California. Int. J. Environ. Res. Public Health 2019, 16, 458. https://doi.org/10.3390/ijerph16030458
Hoshiko S, Pearl M, Yang J, Aldous KM, Roeseler A, Dominguez ME, Smith D, DeLorenze GN, Kharrazi M. Differences in Prenatal Tobacco Exposure Patterns among 13 Race/Ethnic Groups in California. International Journal of Environmental Research and Public Health. 2019; 16(3):458. https://doi.org/10.3390/ijerph16030458
Chicago/Turabian StyleHoshiko, Sumi, Michelle Pearl, Juan Yang, Kenneth M. Aldous, April Roeseler, Martha E. Dominguez, Daniel Smith, Gerald N. DeLorenze, and Martin Kharrazi. 2019. "Differences in Prenatal Tobacco Exposure Patterns among 13 Race/Ethnic Groups in California" International Journal of Environmental Research and Public Health 16, no. 3: 458. https://doi.org/10.3390/ijerph16030458