Trends in Life Expectancy and Its Association with Economic Factors in the Belt and Road Countries—Evidence from 2000–2014

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
3.1. Change of LE in the B&R Countries from 2000 to 2014
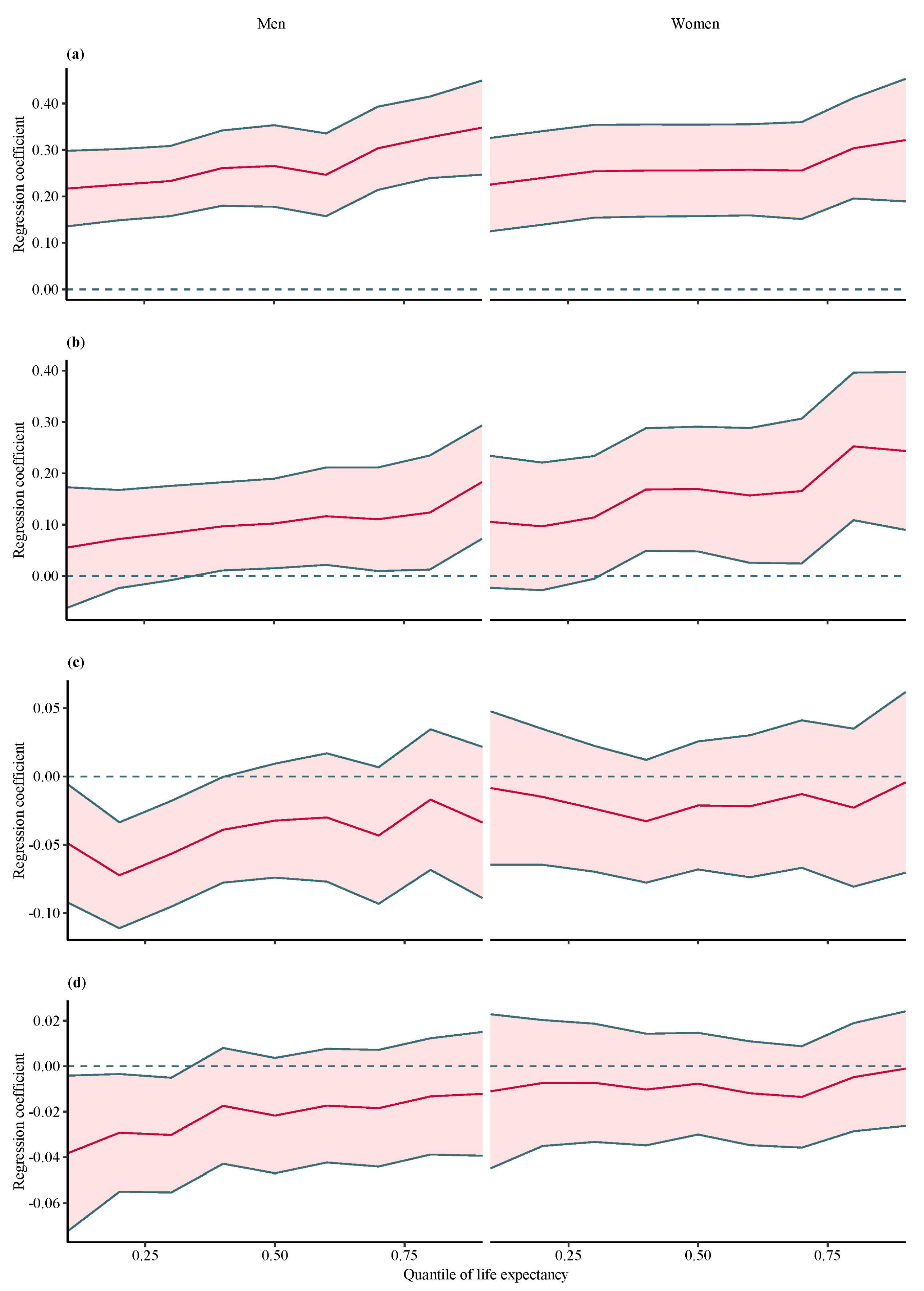
3.2. Associations between LE and Macroeconomic Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smits, J.; Monden, C. Length of life inequality around the globe. Soc. Sci Med. 2009, 68, 1114–1123. [Google Scholar] [CrossRef]
- Hosseinpoor, A.R.; Harper, S.; Lee, J.H.; Lynch, J.; Mathers, C.; Abou-Zahr, C. International shortfall inequality in life expectancy in women and in men, 1950-2010. Bull. World Health Organ. 2012, 90, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Sagar, A.D.; Najam, A. The human development index: A critical review. Ecol. Econ. 1998, 25, 249–264. [Google Scholar] [CrossRef]
- Oeppen, J.; Vaupel, J.W. Demography. Broken limits to life expectancy. Science 2002, 296, 1029–1031. [Google Scholar] [CrossRef]
- Olshansky, S.J.; Passaro, D.J.; Hershow, R.C.; Layden, J.; Carnes, B.A.; Brody, J.; Hayflick, L.; Butler, R.N.; Allison, D.B.; Ludwig, D.S. A potential decline in life expectancy in the United States in the 21st century. N Engl. J. Med. 2005, 352, 1138–1145. [Google Scholar] [CrossRef]
- Wilkinson, R.G. For Debate—Income-Distribution and Life Expectancy. Brit. Med. J. 1992, 304, 165–168. [Google Scholar] [CrossRef]
- Stephens, A.S.; Gupta, L.; Thackway, S.; Broome, R.A. Socioeconomic, remoteness and sex differences in life expectancy in New South Wales, Australia, 2001–2012: A population-based study. BMJ Open 2017, 7, e013227. [Google Scholar] [CrossRef] [PubMed]
- Mondal, M.N.; Shitan, M. Relative importance of demographic, socioeconomic and health factors on life expectancy in low- and lower-middle-income countries. J. Epidemiol. 2014, 24, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Neumayer, E.; Plümper, T. Inequalities of Income and Inequalities of Longevity: A Cross-Country Study. Am. J. Public Health 2016, 106, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araki, S.; Murata, K. Factors affecting the longevity of total Japanese population. Tohoku J. Exp. Med. 1987, 151, 15–24. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Looman, C.W. Life expectancy and national income in Europe, 1900-2008: An update of Preston’s analysis. Int. J. Epidemiol. 2013, 42, 1100–1110. [Google Scholar] [CrossRef]
- Leung, M.C.M.; Zhang, J.; Zhang, J.S. An economic analysis of life expectancy by gender with application to the United States. J. Health Econ. 2004, 23, 737–759. [Google Scholar] [CrossRef] [PubMed]
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association Between Income and Life Expectancy in the United States, 2001–2014. JAMA 2016, 315, 1750–1766. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E.; European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef]
- Hu, R.; Liu, R.; Hu, N. China’s Belt and Road Initiative from a global health perspective. Lancet Glob. Health 2017, 5, e752–e753. [Google Scholar] [CrossRef]
- Tang, K.; Li, Z.; Li, W.; Chen, L. China’s Silk Road and global health. Lancet 2017, 390, 2595–2601. [Google Scholar] [CrossRef]
- Geraci, M.; Bottai, M. Linear quantile mixed models. Stat. Comput. 2014, 24, 461–479. [Google Scholar] [CrossRef]
- World Bank. World Bank Open Data. Available online: http://databank.worldbank.org/data/home.aspx (accessed on 1 March 2017).
- World Health Organization. Global Health Observatory data repository. Available online: http://apps.who.int/gho/data/?theme=main&vid=60340 (accessed on 1 March 2017).
- Fountoulakis, K.N.; Kawohl, W.; Theodorakis, P.N.; Kerkhof, A.J.; Navickas, A.; Hoschl, C.; Lecic-Tosevski, D.; Sorel, E.; Rancans, E.; Palova, E.; et al. Relationship of suicide rates to economic variables in Europe: 2000-2011. Br. J. Psychiatry 2014, 205, 486–496. [Google Scholar] [CrossRef]
- Geraci, M. Linear Quantile Mixed Models: The lqmm Package for Laplace Quantile Regression. J. Stat. Softw. 2014, 57, 1–29. [Google Scholar] [CrossRef]
- Bottai, M.; Cai, B.; McKeown, R.E. Logistic quantile regression for bounded outcomes. Stat. Med. 2010, 29, 309–317. [Google Scholar] [CrossRef]
- Singh, M. Health and Health Policy in Singapore. Asean Econ. Bull. 1999, 16, 330–343. [Google Scholar] [CrossRef]
- Chen, L.C.; Phua, K.H. Transferring lessons from Singapore: An art or a science? Lancet 2013, 382, 930–931. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Jaber, S.; Aziz, M.I.; AlBuhairan, F.; AlGhaithi, A.; AlHamad, N.M.; Al-Hooti, S.N.; Al-Jasari, A.; AlMazroa, M.A.; AlQasmi, A.M.; et al. The state of health in the Arab world, 1990-2010: An analysis of the burden of diseases, injuries, and risk factors. Lancet 2014, 383, 309–320. [Google Scholar] [CrossRef]
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- Waldron, H. Mortality differentials by lifetime earnings decile: Implications for evaluations of proposed Social Security law changes. Soc. Secur. Bull. 2013, 73, 1–37. [Google Scholar] [PubMed]
- Messias, E. Income inequality, illiteracy rate, and life expectancy in Brazil. Am. J. Public Health 2003, 93, 1294–1296. [Google Scholar] [CrossRef]
- Cockerham, W.C.; Hattori, H.; Yamori, Y. The social gradient in life expectancy: The contrary case of Okinawa in Japan. Soc. Sci Med. 2000, 51, 115–122. [Google Scholar] [CrossRef]
- Rosero-Bixby, L. The exceptionally high life expectancy of Costa Rican nonagenarians. Demography 2008, 45, 673–691. [Google Scholar] [CrossRef]
- Bartoll, X.; Marídell’Olmo, M. Patterns of life expectancy before and during economic recession, 2003-12: A European regions panel approach. Eur. J. Public Health 2016, 26, 783–788. [Google Scholar] [CrossRef]
- Brenner, M.H. Commentary: Economic growth is the basis of mortality rate decline in the 20th century--experience of the United States 1901–2000. Int J. Epidemiol 2005, 34, 1214–1221. [Google Scholar] [CrossRef]
- Barr, B.; Taylor-Robinson, D.; Whitehead, M. Impact on health inequalities of rising prosperity in England 1998–2007, and implications for performance incentives: Longitudinal ecological study. BMJ 2012, 345, e7831. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M. Inequalities in US Life Expectancy by Area Unemployment Level, 1990–2010. Scientifica 2016, 2016, 8290435. [Google Scholar] [CrossRef] [PubMed]
- McLeod, C.B.; Hall, P.A.; Siddiqi, A.; Hertzman, C. How society shapes the health gradient: Work-related health inequalities in a comparative perspective. Annu. Rev. Public Health 2012, 33, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Tapia Granados, J.A.; Ionides, E.L. The reversal of the relation between economic growth and health progress: Sweden in the 19th and 20th centuries. J. Health Econ. 2008, 27, 544–563. [Google Scholar] [CrossRef]
- Ruhm, C.J. Commentary: Mortality increases during economic upturns. Int. J. Epidemiol. 2005, 34, 1206–1211. [Google Scholar] [CrossRef] [Green Version]
- Williams, C.; Gilbert, B.J.; Zeltner, T.; Watkins, J.; Atun, R.; Maruthappu, M. Effects of economic crises on population health outcomes in Latin America, 1981-2010: An ecological study. BMJ Open 2016, 6, e007546. [Google Scholar] [CrossRef]
- Bind, M.A.; Coull, B.A.; Peters, A.; Baccarelli, A.A.; Tarantini, L.; Cantone, L.; Vokonas, P.S.; Koutrakis, P.; Schwartz, J.D. Beyond the Mean: Quantile Regression to Explore the Association of Air Pollution with Gene-Specific Methylation in the Normative Aging Study. Environ. Health Perspect. 2015, 123, 759–765. [Google Scholar] [CrossRef]


{kind=link}
| Year | Women | Men |
|---|---|---|
| 2000 | 69.6 | 65.7 |
| 2001 | 69.9 | 66.1 |
| 2002 | 70.2 | 66.4 |
| 2003 | 70.5 | 66.7 |
| 2004 | 70.8 | 67.0 |
| 2005 | 71.1 | 67.3 |
| 2006 | 71.4 | 67.6 |
| 2007 | 71.8 | 67.9 |
| 2008 | 72.0 | 68.2 |
| 2009 | 72.3 | 68.5 |
| 2010 | 72.6 | 68.7 |
| 2011 | 72.9 | 69.0 |
| 2012 | 73.2 | 69.2 |
| 2013 | 73.4 | 69.5 |
| 2014 | 73.7 | 69.7 |
| Country | 2000 | 2014 | 15 Years Increase in Life Expectancy | |||
|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | |
| Afghanistan | 56.1 | 53.7 | 61.3 | 58.6 | 5.2 | 4.9 |
| Albania | 76.4 | 69.4 | 80.6 | 74.7 | 4.2 | 5.3 |
| Armenia | 75.1 | 68.7 | 77.5 | 71.4 | 2.4 | 2.7 |
| Azerbaijan | 69.8 | 63.4 | 75.5 | 69.4 | 5.7 | 6.0 |
| Bahrain | 75.5 | 73.7 | 77.8 | 76.0 | 2.3 | 2.3 |
| Bangladesh | 65.6 | 64.9 | 72.7 | 70.2 | 7.1 | 5.3 |
| Belarus | 73.5 | 62.6 | 77.7 | 66.3 | 4.2 | 3.7 |
| Bhutan | 60.3 | 60.0 | 69.7 | 69.2 | 9.4 | 9.2 |
| Bosnia and Herzegovina | 77.2 | 71.8 | 79.6 | 74.8 | 2.4 | 3.0 |
| Brunei Darussalam | 76.0 | 73.1 | 79.1 | 76.2 | 3.1 | 3.1 |
| Bulgaria | 74.7 | 67.8 | 77.8 | 70.9 | 3.1 | 3.1 |
| Cambodia | 59.9 | 55.3 | 70.2 | 66.1 | 10.3 | 10.8 |
| China | 73.5 | 70.1 | 77.4 | 74.4 | 3.9 | 4.3 |
| Croatia | 78.2 | 71.1 | 81.0 | 74.4 | 2.8 | 3.3 |
| Cyprus | 80.2 | 76.0 | 82.5 | 78.2 | 2.3 | 2.2 |
| Czech Republic | 78.1 | 71.2 | 81.5 | 75.6 | 3.4 | 4.4 |
| Egypt | 71.4 | 66.4 | 73.0 | 68.6 | 1.6 | 2.2 |
| Estonia | 76.1 | 65.4 | 81.8 | 72.3 | 5.7 | 6.9 |
| Georgia | 75.5 | 68.0 | 78.4 | 70.5 | 2.9 | 2.5 |
| Greece | 81.1 | 75.4 | 83.5 | 78.1 | 2.4 | 2.7 |
| Hungary | 76.0 | 67.5 | 79.0 | 72.1 | 3.0 | 4.6 |
| India | 63.4 | 61.7 | 69.5 | 66.6 | 6.1 | 4.9 |
| Indonesia | 68.0 | 64.6 | 71.0 | 66.9 | 3.0 | 2.3 |
| Iran | 71.2 | 69.4 | 76.5 | 74.4 | 5.3 | 5.0 |
| Iraq | 72.3 | 67.8 | 71.1 | 64.9 | −1.2 | −2.9 |
| Israel | 80.8 | 76.8 | 84.0 | 80.2 | 3.2 | 3.4 |
| Jordan | 73.3 | 70.4 | 75.7 | 72.4 | 2.4 | 2.0 |
| Kazakhstan | 69.9 | 58.3 | 74.5 | 65.3 | 4.6 | 7.0 |
| Kuwait | 74.4 | 72.4 | 75.8 | 73.6 | 1.4 | 1.2 |
| Kyrgyzstan | 70.7 | 62.6 | 74.8 | 66.9 | 4.1 | 4.3 |
| Laos | 59.7 | 56.5 | 66.8 | 63.7 | 7.1 | 7.2 |
| Latvia | 75.7 | 64.4 | 79.0 | 69.4 | 3.3 | 5.0 |
| Lebanon | 74.3 | 71.2 | 76.4 | 73.4 | 2.1 | 2.2 |
| Lithuania | 77.2 | 65.9 | 79.0 | 67.9 | 1.8 | 2.0 |
| Macedonia | 74.9 | 70.5 | 77.7 | 73.4 | 2.8 | 2.9 |
| Malaysia | 74.9 | 70.2 | 77.1 | 72.5 | 2.2 | 2.3 |
| Maldives | 70.4 | 68.9 | 79.8 | 76.6 | 9.4 | 7.7 |
| Mongolia | 65.7 | 60.0 | 72.8 | 64.3 | 7.1 | 4.3 |
| Montenegro | 75.6 | 70.4 | 77.9 | 74.0 | 2.3 | 3.6 |
| Myanmar | 64.1 | 60.2 | 68.3 | 64.4 | 4.2 | 4.2 |
| Nepal | 63.5 | 61.5 | 71.0 | 68.2 | 7.5 | 6.7 |
| Oman | 74.9 | 70.7 | 79.0 | 74.7 | 4.1 | 4.0 |
| Pakistan | 63.6 | 62.0 | 67.2 | 65.2 | 3.6 | 3.2 |
| Philippines | 69.9 | 63.9 | 71.8 | 65.2 | 1.9 | 1.3 |
| Poland | 77.9 | 69.5 | 81.2 | 73.4 | 3.3 | 3.9 |
| Qatar | 77.8 | 75.3 | 79.9 | 77.3 | 2.1 | 2.0 |
| Republic of Moldova | 71.0 | 63.2 | 75.9 | 67.6 | 4.9 | 4.4 |
| Romania | 74.3 | 67.2 | 78.6 | 71.2 | 4.3 | 4.0 |
| Russian Federation | 72.0 | 58.7 | 76.1 | 64.5 | 4.1 | 5.8 |
| Saudi Arabia | 74.4 | 71.0 | 75.9 | 73.1 | 1.5 | 2.1 |
| Serbia | 75.6 | 69.7 | 78.2 | 72.7 | 2.6 | 3.0 |
| Singapore | 80.9 | 75.9 | 85.9 | 79.8 | 5.0 | 3.9 |
| Slovakia | 77.1 | 68.9 | 80.1 | 72.7 | 3.0 | 3.8 |
| Slovenia | 79.7 | 72.2 | 83.6 | 77.7 | 3.9 | 5.5 |
| Sri Lanka | 75.1 | 68.2 | 78.1 | 71.3 | 3.0 | 3.1 |
| Syrian Arab Republic | 74.9 | 70.5 | 69.7 | 59.9 | -5.2 | -10.6 |
| Tajikistan | 67.6 | 60.3 | 73.4 | 66.4 | 5.8 | 6.1 |
| Thailand | 74.6 | 67.8 | 77.8 | 71.7 | 3.2 | 3.9 |
| Turkey | 73.8 | 67.1 | 78.6 | 72.3 | 4.8 | 5.2 |
| Turkmenistan | 67.9 | 59.9 | 70.3 | 62.0 | 2.4 | 2.1 |
| Ukraine | 73.2 | 62.0 | 75.8 | 65.7 | 2.6 | 3.7 |
| United Arab Emirates | 75.7 | 73.4 | 78.5 | 76.2 | 2.8 | 2.8 |
| Uzbekistan | 70.4 | 63.8 | 72.6 | 65.9 | 2.2 | 2.1 |
| Viet Nam | 78.2 | 68.5 | 80.5 | 71.1 | 2.3 | 2.6 |
| Yemen | 62.2 | 59.5 | 66.9 | 63.9 | 4.7 | 4.4 |
| Range | 56.1–81.1 | 53.7–76.8 | 61.3–85.9 | 58.6–80.2 | −5.2–10.3 | −10.6–10.8 |
| Total | 69.6 | 65.7 | 73.7 | 69.7 | 4.1 | 4.0 |
| 10th Percentile 1 | 20th Percentile 1 | 30th Percentile 1 | 40th Percentile 1 | 50th Percentile 1 | 60th Percentile 1 | 70th Percentile 1 | 80th Percentile 1 | 90th Percentile 1 | Random Effect Model 2 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Women | |||||||||||
| GDP growth rate (%) | Coefficient 3 | −0.01 | −0.02 | −0.02 | −0.03 | −0.02 | −0.02 | −0.01 | −0.02 | 0.00 | −0.04 |
| 95% CI 4 | (−0.07, 0.05) | (−0.07, 0.04) | (−0.07, 0.02) | (−0.08, 0.01) | (−0.07, 0.03) | (−0.07, 0.03) | (−0.07, 0.04) | (−0.08, 0.04) | (−0.07, 0.06) | (−0.06, −0.02) | |
| p-value | 0.768 | 0.557 | 0.314 | 0.153 | 0.376 | 0.411 | 0.641 | 0.439 | 0.899 | <0.001 | |
| Unemployment rate (%) | Coefficient 3 | 0.11 | 0.10 | 0.11 | 0.17 | 0.17 | 0.16 | 0.17 | 0.25 | 0.24 | 0.00 |
| 95% CI 4 | (−0.02, 0.23) | (−0.03, 0.22) | (−0.01, 0.23) | (0.05, 0.29) | (0.05, 0.29) | (0.03, 0.29) | (0.02, 0.31) | (0.11, 0.40) | (0.09, 0.40) | (−0.04, 0.04) | |
| p-value | 0.108 | 0.128 | 0.062 | 0.006 | 0.006 | 0.019 | 0.022 | 0.001 | 0.002 | 0.965 | |
| GDP per capita/1000 | Coefficient 3 | 0.23 | 0.24 | 0.25 | 0.26 | 0.26 | 0.26 | 0.26 | 0.30 | 0.32 | 0.17 |
| 95% CI 4 | (0.13, 0.33 | (0.14, 0.34) | (0.15, 0.35) | (0.16, 0.36) | (0.16, 0.35) | (0.16, 0.36) | (0.15, 0.36) | (0.20, 0.41) | (0.19,0.45) | (0.15, 0.19) | |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Inflation (%) | Coefficient 3 | −0.01 | −0.01 | -0.01 | −0.01 | −0.01 | −0.01 | −0.01 | −0.01 | 0.00 | −0.02 |
| 95% CI 4 | (−0.05, 0.02) | (−0.04, 0.02) | (−0.03, 0.02) | (−0.04, 0.01) | (−0.03, 0.02) | (−0.04, 0.01) | (−0.04, 0.01) | (−0.03, 0.02) | (−0.03,0.02) | (−0.03, −0.01) | |
| p-value | 0.522 | 0.600 | 0.581 | 0.412 | 0.500 | 0.306 | 0.234 | 0.690 | 0.933 | <0.001 | |
| 2. Men | |||||||||||
| GDP growth rate (%) | Coefficient 3 | −0.05 | −0.07 | −0.06 | −0.04 | −0.03 | −0.03 | −0.04 | −0.02 | −0.03 | −0.06 |
| 95% CI 4 | (−0.09, −0.01) | (−0.11, −0.03) | (−0.10, −0.02) | (−0.08, 0.00) | (−0.07, 0.01) | (−0.08, 0.02) | (−0.09, 0.01) | (−0.07, 0.04) | (−0.09,0.02) | (−0.08, −0.04) | |
| p-value | 0.027 | 0.000 | 0.004 | 0.048 | 0.129 | 0.211 | 0.090 | 0.519 | 0.234 | <0.001 | |
| Unemployment rate (%) | Coefficient 3 | 0.06 | 0.07 | 0.08 | 0.10 | 0.10 | 0.12 | 0.11 | 0.12 | 0.18 | 0.01 |
| 95% CI 4 | (−0.06, 0.17) | (−0.02, 0.17) | (−0.01, 0.18) | (0.01, 0.18) | (0.02, 0.19) | (0.02, 0.21) | (0.01, 0.21) | (0.01, 0.24) | (0.07,0.29) | (−0.03, 0.04) | |
| p-value | 0.360 | 0.142 | 0.076 | 0.028 | 0.022 | 0.016 | 0.032 | 0.030 | 0.001 | 0.811 | |
| GDP per capita/1000 | Coefficient 3 | 0.22 | 0.23 | 0.23 | 0.26 | 0.27 | 0.25 | 0.30 | 0.33 | 0.35 | 0.19 |
| 95% CI 4 | (0.14, 0.30) | (0.15, 0.30) | (0.16, 0.31) | (0.18, 0.34) | (0.18, 0.35) | (0.16, 0.34) | (0.21, 0.39) | (0.24, 0.42) | (0.25,0.45) | (0.17, 0.21) | |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Inflation (%) | Coefficient 3 | −0.04 | −0.03 | −0.03 | −0.02 | −0.02 | −0.02 | −0.02 | −0.01 | −0.01 | −0.02 |
| 95% CI 4 | (−0.07, 0.00) | (−0.06, 0.00) | (−0.06, −0.01) | (−0.04, 0.01) | (−0.05, 0.00) | (−0.04, 0.01) | (−0.04, 0.01) | (−0.04, 0.01) | (−0.04,0.02) | (−0.03, −0.01) | |
| p-value | 0.028 | 0.026 | 0.019 | 0.179 | 0.093 | 0.173 | 0.158 | 0.308 | 0.381 | <0.001 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, R.; Wei, J.; An, R.; Li, Y.; Collett, L.; Dang, S.; Dong, W.; Wang, D.; Fang, Z.; Zhao, Y.; et al. Trends in Life Expectancy and Its Association with Economic Factors in the Belt and Road Countries—Evidence from 2000–2014. Int. J. Environ. Res. Public Health 2018, 15, 2890. https://doi.org/10.3390/ijerph15122890
Bai R, Wei J, An R, Li Y, Collett L, Dang S, Dong W, Wang D, Fang Z, Zhao Y, et al. Trends in Life Expectancy and Its Association with Economic Factors in the Belt and Road Countries—Evidence from 2000–2014. International Journal of Environmental Research and Public Health. 2018; 15(12):2890. https://doi.org/10.3390/ijerph15122890
Chicago/Turabian StyleBai, Ruhai, Junxiang Wei, Ruopeng An, Yan Li, Laura Collett, Shaonong Dang, Wanyue Dong, Duolao Wang, Zeping Fang, Yaling Zhao, and et al. 2018. "Trends in Life Expectancy and Its Association with Economic Factors in the Belt and Road Countries—Evidence from 2000–2014" International Journal of Environmental Research and Public Health 15, no. 12: 2890. https://doi.org/10.3390/ijerph15122890