Effects of Polybrominated Diphenyl Ethers on Child Cognitive, Behavioral, and Motor Development

Abstract
:1. Introduction
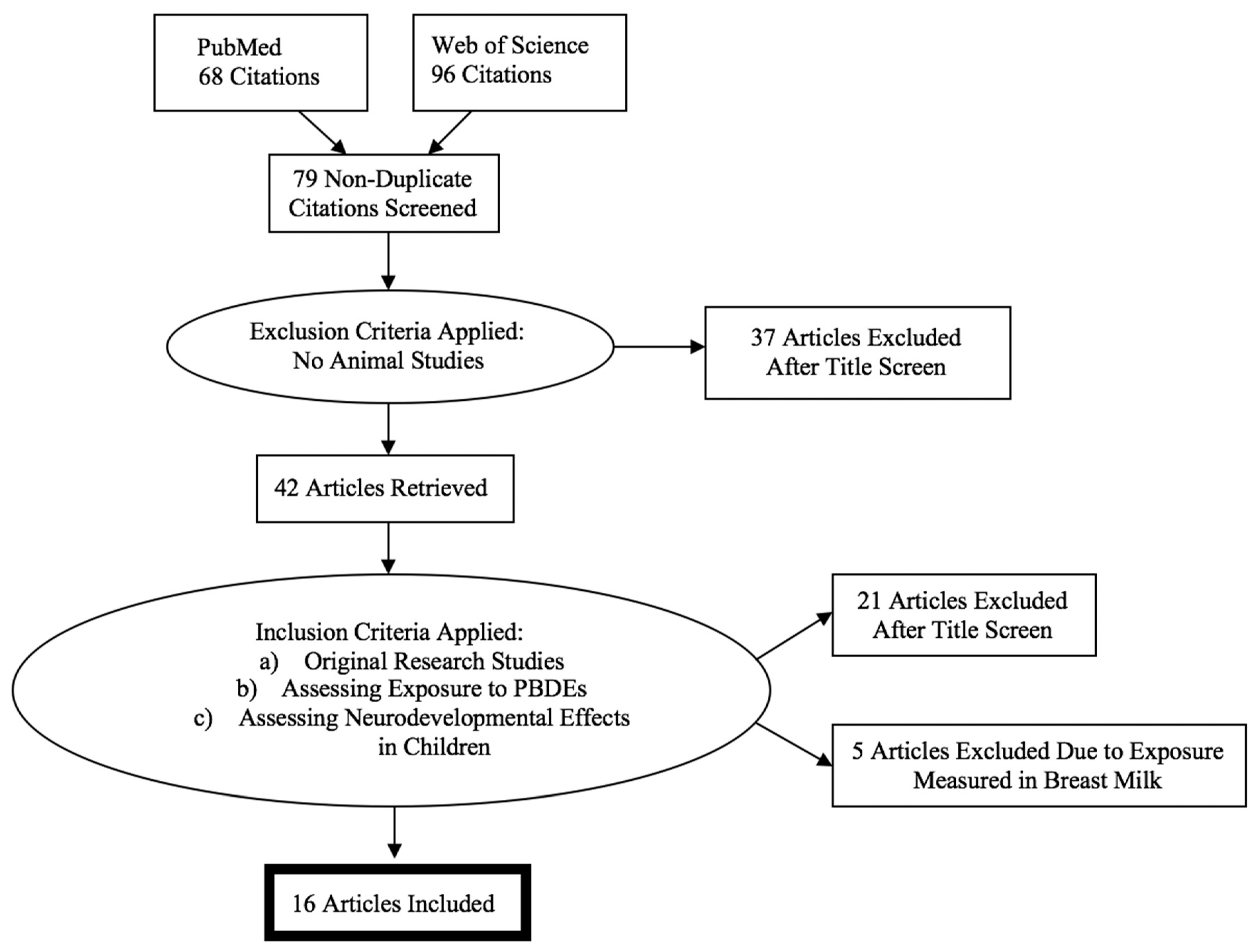
2. Methods
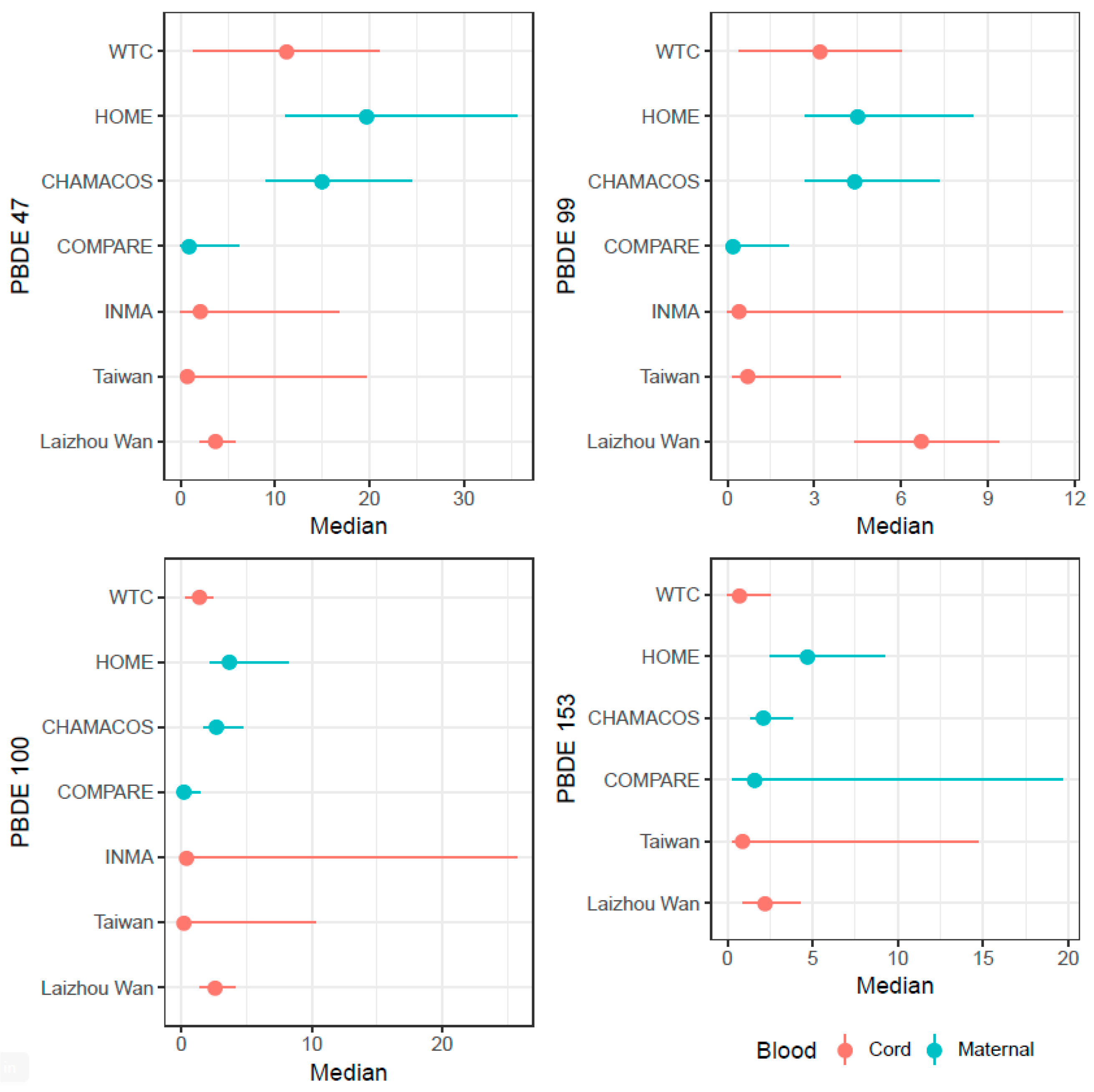
3. Summary of Studies
4. Results
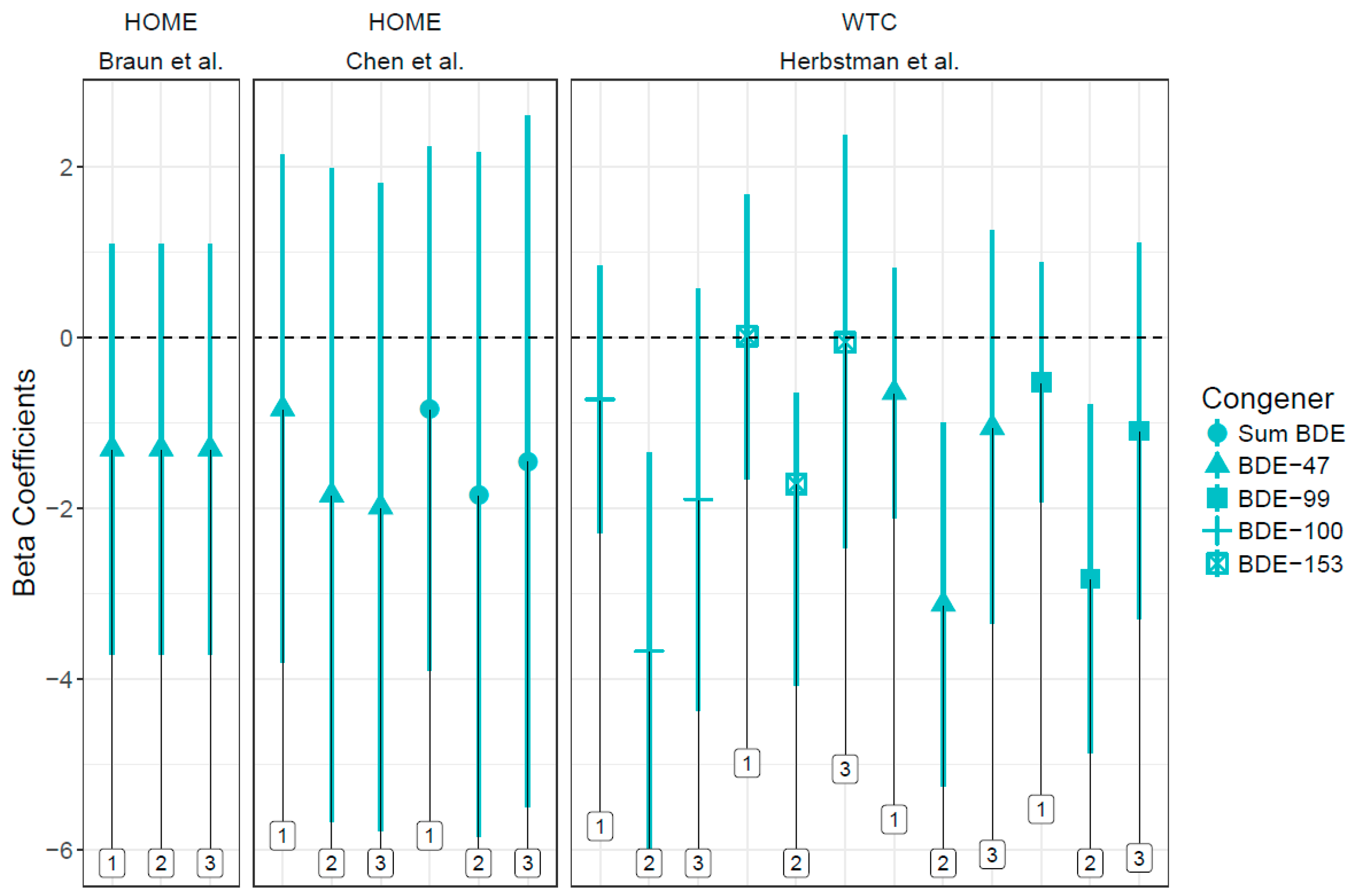
4.1. Motor
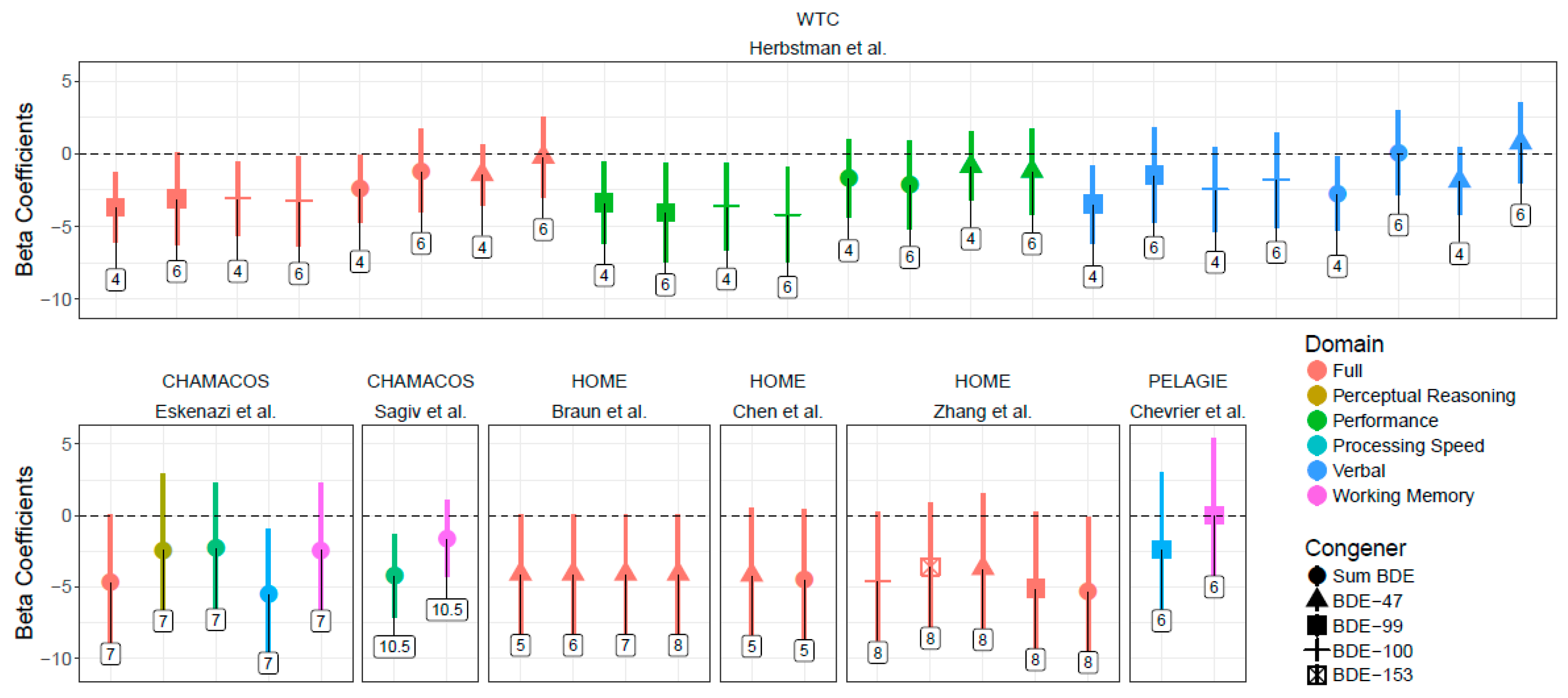
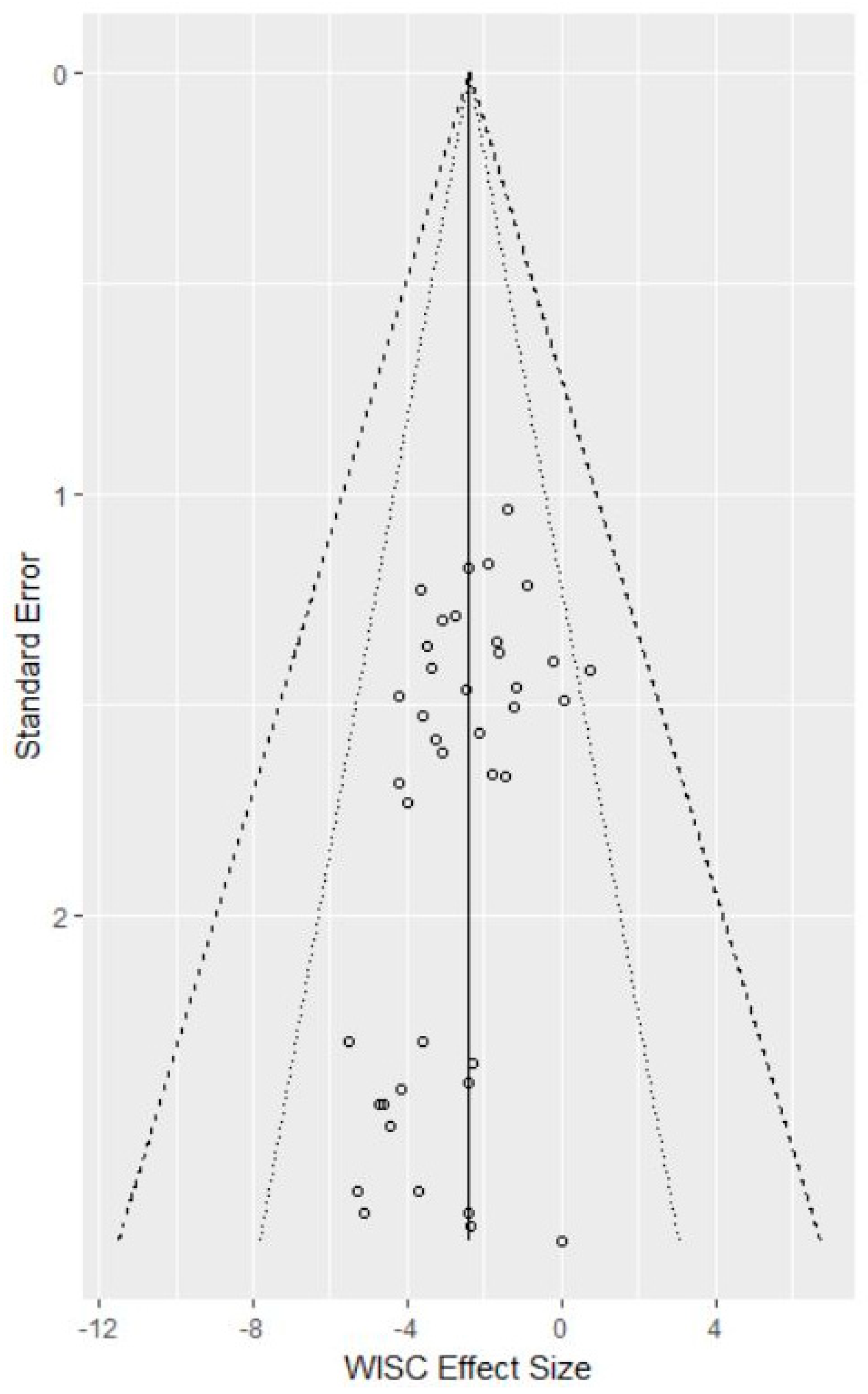
4.2. Cognitive
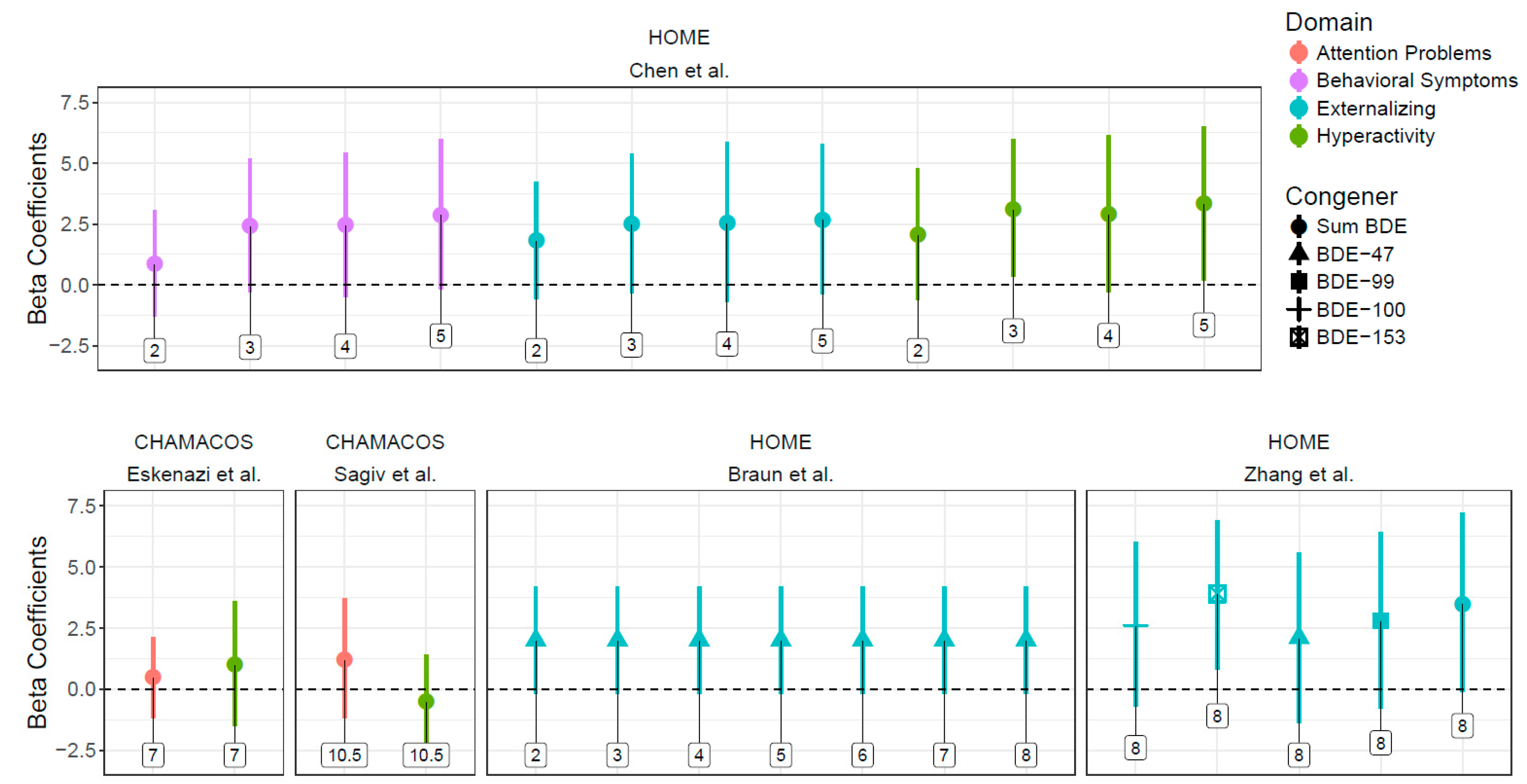
4.3. Behavior
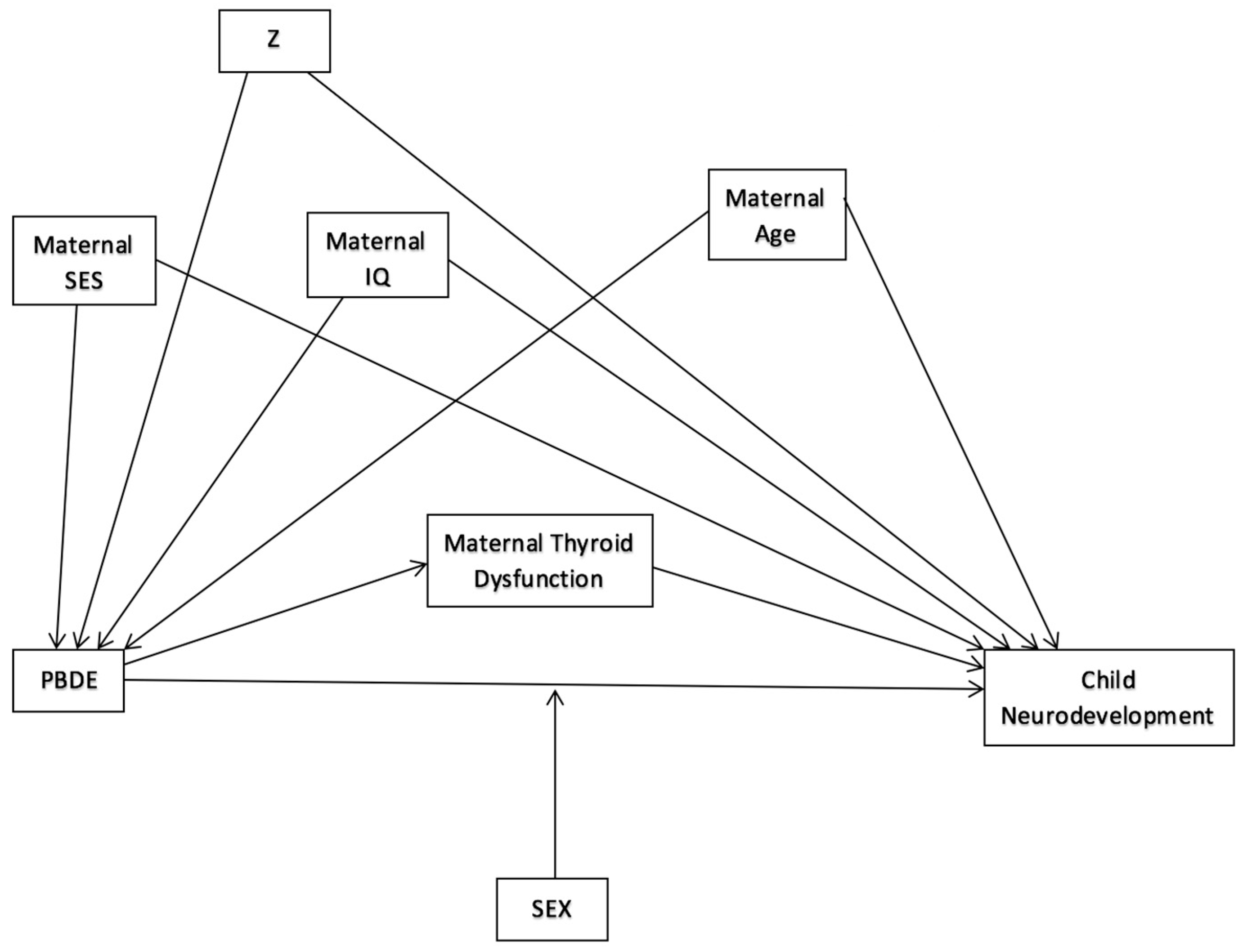
4.4. Interaction and Mediation
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Were subjects with varying levels of exposure drawn from the same underlying population? | Was exposure assessed using validated methods? | Are we confident that the outcome of interest was not present at start of study? | Did the study adjust for confounding? | Was an independently validated measure used for outcome assessment? | Did the statistical analysis include at least 60% of the cohort over the course of the study? | Was adjustment made for multiple statistical comparisons between congeners and outcomes? | |
| United States | |||||||
| CHAMACOS | |||||||
| Eskenazi et al., 2013 | X | X | X | X | X | X (266/526 = 51%) | X |
| Sagiv et al., 2015 | X | X | X | X | X | X (337/536 = 63%) | X |
| HOME | |||||||
| Chen et al., 2014 | X | X | X | X | X | X (309/389 = 79%) | X |
| Vuong et al., 2016 | X | X | X | X | X | X (256/390 = 66%) | X |
| Zhang et al., 2016 | X | X | X | X | X | X (239/389 = 61%) | X |
| Braun et al., 2017 | X | X | X | X | X | X (229/346 = 59%) | X |
| Vuong et al., 2017a | X | X | X | X | X | X (214/390 = 55%) | X |
| Vuong et al., 2017b | X | X | X | X | X | X (199/390 = 51%) | X |
| WTC | |||||||
| Herbstman et al., 2010 | X | X | X | X | X | X (152/329 = 46%) | X |
| Cowell et al., 2015 | X | X | X | X | X | X (109/329 = 33%) | X |
| Asia | |||||||
| Shy et al., 2011 | X | X | X | X | X | X (36/95 = 38%) | X |
| Ding et al., 2015 | X | X | X | X | X | X (192/347 = 55%) | X |
| Kim et al., 2018 | X | X | X | X | X | X (59/140 = 42%) | X |
| Europe | |||||||
| Gascon et al., 2011 | X | X | X | X | X | X (422/482 = 88%) | X |
| Roze et al., 2009 | X | X | X | X | X | X (62/69 = 90%) | X |
| Chevrier et al., 2016 | X | X | X | X | X | X (246/287 = 86%) | X |

References
- Hood, E. Endocrine disruption and flame-retardant chemicals: PBDE-99 effects on rat sexual development. Environ. Health Perspect. 2006, 114, A112–A113. [Google Scholar] [CrossRef]
- Lilienthal, H.; Hack, A.; Roth-Härer, A.; Grande, S.W.; Talsness, C.E. Effects of developmental exposure to 2,2′,4,4′,5-pentabromodiphenyl ether (PBDE-99) on sex steroids, sexual development, and sexually dimorphic behavior in rats. Environ. Health Perspect. 2006, 114, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, P.; Jakobsson, E.; Fredriksson, A. Brominated flame retardants: A novel class of developmental neurotoxicants in our environment? Environ. Health Perspect. 2001, 109, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, T.; Gassmann, K.; Götz, C.; Hübenthal, U.; Moors, M.; Krause, G.; Merk, H.F.; Nguyen, N.-H.; Scanlan, T.S.; Abel, J. Polybrominated diphenyl ethers induce developmental neurotoxicity in a human in vitro model: Evidence for endocrine disruption. Environ. Health Perspect. 2010, 118, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Lanphear, B.P.; Bellinger, D.; Axelrad, D.A.; McPartland, J.; Sutton, P.; Davidson, L.; Daniels, N.; Sen, S.; Woodruff, T.J. Developmental PBDE exposure and IQ/ADHD in childhood: A systematic review and meta-analysis. Environ. Health Perspect. 2017, 125, 086001. [Google Scholar] [CrossRef] [PubMed]
- Vuong, A.M.; Yolton, K.; Dietrich, K.N.; Braun, J.M.; Lanphear, B.P.; Chen, A. Exposure to polybrominated diphenyl ethers (PBDEs) and child behavior: Current findings and future directions. Horm. Behav. 2018, 101, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, H.M.; Sharma, S.; Getzinger, G.; Ferguson, P.L.; Gabriel, M.; Webster, T.F.; Blum, A. Novel and high volume use flame retardants in US couches reflective of the 2005 pentabde phase out. Environ. Sci. Technol. 2012, 46, 13432–13439. [Google Scholar] [CrossRef] [PubMed]
- Cowell, W.J.; Sjödin, A.; Jones, R.; Wang, Y.; Wang, S.; Herbstman, J.B. Temporal trends and developmental patterns of plasma polybrominated diphenyl ether concentrations over a 15-year period between 1998 and 2013. J. Expo. Sci. Environ. Epidemiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Polybrominated Diphenyl Ethers (PBDEs). Available online: https://www.atsdr.cdc.gov/toxprofiles/tp207.pdf (accessed on 1 May 2018).
- Geyer, H.J.; Schramm, K.-W.; Darnerud, P.O.; Aune, M.; Feicht, E.A.; Fried, K.W.; Henkelmann, B.; Lenoir, D.; Schmid, P.; McDonald, T.A. Terminal elimination half-lives of the brominated flame retardants TBBPA, HBCD, and lower brominated PBDEs in humans. Organohalogen Compd. 2004, 66, 3867–3872. [Google Scholar]
- Sjodin, A.; Jones, R.S.; Caudill, S.P.; Wong, L.Y.; Turner, W.E.; Calafat, A.M. Polybrominated diphenyl ethers, polychlorinated biphenyls, and persistent pesticides in serum from the national health and nutrition examination survey: 2003–2008. Environ. Sci. Technol. 2014, 48, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.R.; Meimaridou, A.; Haasnoot, W.; Meulenberg, E.; Albertus, F.; Mizuguchi, M.; Takeuchi, M.; Irth, H.; Murk, A.J. Biosensor discovery of thyroxine transport disrupting chemicals. Toxicol. Appl. Pharmacol. 2008, 232, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Hallgren, S.; Sinjari, T.; Håkansson, H.; Darnerud, P. Effects of polybrominated diphenyl ethers (PBDEs) and polychlorinated biphenyls (PCBs) on thyroid hormone and vitamin a levels in rats and mice. Arch. Toxicol. 2001, 75, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Ross, D.G.; DeVito, M.J.; Crofton, K.M. Effects of short-term in vivo exposure to polybrominated diphenyl ethers on thyroid hormones and hepatic enzyme activities in weanling rats. Toxicol. Sci. 2001, 61, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Haddow, J.E.; Palomaki, G.E.; Allan, W.C.; Williams, J.R.; Knight, G.J.; Gagnon, J.; O’heir, C.E.; Mitchell, M.L.; Hermos, R.J.; Waisbren, S.E. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N. Engl. J. Med. 1999, 341, 549–555. [Google Scholar] [CrossRef] [PubMed]
- de Escobar, G.M.; Obregón, M.A.J.; del Rey, F.E. Maternal thyroid hormones early in pregnancy and fetal brain development. Best Pract. Res. Clin. Endocrinol. Metab. 2004, 18, 225–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hites, R.A. Polybrominated diphenyl ethers in the environment and in people: A meta-analysis of concentrations. Environ. Sci. Technol. 2004, 38, 945–956. [Google Scholar] [CrossRef] [PubMed]
- Herbstman, J.B.; Mall, J.K. Developmental exposure to polybrominated diphenyl ethers and neurodevelopment. Curr. Environ. Health Rep. 2014, 1, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1. 0; [updated March 2011]; The Cochrane Collaboration: Hoboken, NJ, USA, 2011. [Google Scholar]
- Frederiksen, M.; Thomsen, C.; Froshaug, M.; Vorkamp, K.; Thomsen, M.; Becher, G.; Knudsen, L.E. Polybrominated diphenyl ethers in paired samples of maternal and umbilical cord blood plasma and associations with house dust in a Danish cohort. Int. J. Hyg. Environ. Health 2010, 213, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Terry, P.; Towers, C.V.; Liu, L.Y.; Peverly, A.A.; Chen, J.; Salamova, A. Polybrominated diphenyl ethers (flame retardants) in mother-infant pairs in the Southeastern US. Int. J. Environ. Health Res. 2017, 27, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (nos) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research institute: Oxford, UK, 2014. [Google Scholar]
- Roze, E.; Meijer, L.; Bakker, A.; Van Braeckel, K.N.; Sauer, P.J.; Bos, A.F. Prenatal exposure to organohalogens, including brominated flame retardants, influences motor, cognitive, and behavioral performance at school age. Environ. Health Perspect. 2009, 117, 1953–1958. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Vrijheid, M.; Martinez, D.; Forns, J.; Grimalt, J.O.; Torrent, M.; Sunyer, J. Effects of pre and postnatal exposure to low levels of polybromodiphenyl ethers on neurodevelopment and thyroid hormone levels at 4 years of age. Environ. Int. 2011, 37, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, C.; Warembourg, C.; Le Maner-Idrissi, G.; Lacroix, A.; Dardier, V.; Le Sourn-Bissaoui, S.; Rouget, F.; Monfort, C.; Gaudreau, E.; Mercier, F.; et al. Childhood exposure to polybrominated diphenyl ethers and neurodevelopment at six years of age. Neurotoxicology 2016, 54, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, G.D.; Yu, J.; Cui, C.; Chen, L.M.; Gao, Y.; Wang, C.F.; Zhou, Y.J.; Tian, Y. Association between prenatal exposure to polybrominated diphenyl ethers and young children’s neurodevelopment in China. Environ. Res. 2015, 142, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Shy, C.G.; Huang, H.L.; Chang-Chien, G.P.; Chao, H.R.; Tsou, T.C. Neurodevelopment of infants with prenatal exposure to polybrominated diphenyl ethers. Bull. Environ. Contam. Toxicol. 2011, 87, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Eom, S.; Kim, H.-J.; Lee, J.J.; Choi, G.; Choi, S.; Kim, S.; Kim, S.Y.; Cho, G.; Kim, Y.D. Association between maternal exposure to major phthalates, heavy metals, and persistent organic pollutants, and the neurodevelopmental performances of their children at 1 to 2years of age-check cohort study. Sci. Total Environ. 2018, 624, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, B.; Chevrier, J.; Rauch, S.A.; Kogut, K.; Harley, K.G.; Johnson, C.; Trujillo, C.; Sjodin, A.; Bradman, A. In utero and childhood polybrominated diphenyl ether (PBDE) exposures and neurodevelopment in the chamacos study. Environ. Health Perspect. 2013, 121, 257–262. [Google Scholar] [PubMed]
- Sagiv, S.K.; Kogut, K.; Gaspar, F.W.; Gunier, R.B.; Harley, K.G.; Parra, K.; Villasenor, D.; Bradman, A.; Holland, N.; Eskenazi, B. Prenatal and childhood polybrominated diphenyl ether (PBDE) exposure and attention and executive function at 9–12 years of age. Neurotoxicol. Teratol. 2015, 52, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Yolton, K.; Rauch, S.A.; Webster, G.M.; Hornung, R.; Sjodin, A.; Dietrich, K.N.; Lanphear, B.P. Prenatal polybrominated diphenyl ether exposures and neurodevelopment in US Children through 5 years of age: The home study. Environ. Health Perspect. 2014, 122, 856–862. [Google Scholar] [PubMed]
- Vuong, A.M.; Yolton, K.; Webster, G.M.; Sjodin, A.; Calafat, A.M.; Braun, J.M.; Dietrich, K.N.; Lanphear, B.P.; Chen, A.M. Prenatal polybrominated diphenyl ether and perfluoroalkyl substance exposures and executive function in school-age children. Environ. Res. 2016, 147, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Yolton, K.; Webster, G.M.; Sjodin, A.; Calafat, A.M.; Dietrich, K.N.; Xu, Y.; Xie, C.; Braun, J.M.; Lanphear, B.P.; et al. Prenatal PBDE and PCB exposures and reading, cognition, and externalizing behavior in children. Environ. Health Perspect. 2017, 125, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Yolton, K.; Stacy, S.L.; Erar, B.; Papandonatos, G.D.; Bellinger, D.C.; Lanphear, B.P.; Chen, A. Prenatal environmental chemical exposures and longitudinal patterns of child neurobehavior. Neurotoxicology 2017, 62, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Vuong, A.M.; Braun, J.M.; Yolton, K.; Xie, C.; Webster, G.M.; Sjödin, A.; Dietrich, K.N.; Lanphear, B.P.; Chen, A. Prenatal and postnatal polybrominated diphenyl ether exposure and visual spatial abilities in children. Environ. Res. 2017, 153, 83–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuong, A.M.; Yolton, K.; Poston, K.L.; Xie, C.; Webster, G.M.; Sjödin, A.; Braun, J.M.; Dietrich, K.N.; Lanphear, B.P.; Chen, A. Prenatal and postnatal polybrominated diphenyl ether (PBDE) exposure and measures of inattention and impulsivity in children. Neurotoxicol. Teratol. 2017, 64, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Cowell, W.J.; Lederman, S.A.; Sjodin, A.; Jones, R.; Wang, S.; Perera, F.P.; Wang, R.; Rauh, V.A.; Herbstman, J.B. Prenatal exposure to polybrominated diphenyl ethers and child attention problems at 3–7 years. Neurotoxicol. Teratol. 2015, 52, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Herbstman, J.B.; Sjodin, A.; Kurzon, M.; Lederman, S.A.; Jones, R.S.; Rauh, V.; Needham, L.L.; Tang, D.; Niedzwiecki, M.; Wang, R.Y.; et al. Prenatal exposure to PBDES and neurodevelopment. Environ. Health Perspect. 2010, 118, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Ni, K.; Lu, Y.; Wang, T.; Shi, Y.; Kannan, K.; Xu, L.; Li, Q.; Liu, S. Polybrominated diphenyl ethers (PBDEs) in China: Policies and recommendations for sound management of plastics from electronic wastes. J. Environ. Manag. 2013, 115, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Weisskopf, M.G.; Seals, R.M.; Webster, T.F. Bias amplification in epidemiologic analysis of exposure to mixtures. Environ. Health Perspect. 2018, 126, 047003. [Google Scholar] [CrossRef] [PubMed]
- Chao, H.R.; Tsou, T.C.; Huang, H.L.; Chang-Chien, G.P. Levels of breast milk PBDEs from southern Taiwan and their potential impact on neurodevelopment. Pediatr. Res. 2011, 70, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, K.; Adgent, M.; Goldman, B.D.; Sjodin, A.; Daniels, J.L. Lactational exposure to polybrominated diphenyl ethers and its relation to social and emotional development among toddlers. Environ. Health Perspect. 2012, 120, 1438–1442. [Google Scholar] [CrossRef] [PubMed]
- Adgent, M.A.; Hoffman, K.; Goldman, B.D.; Sjodin, A.; Daniels, J.L. Brominated flame retardants in breast milk and behavioural and cognitive development at 36 months. Paediatr. Perinat. Epidemiol. 2014, 28, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Fort, M.; Martinez, D.; Carsin, A.E.; Forns, J.; Grimalt, J.O.; Marina, L.S.; Lertxundi, N.; Sunyer, J.; Vrijheid, M. Polybrominated diphenyl ethers (PBDEs) in breast milk and neuropsychological development in infants. Environ. Health Perspect. 2012, 120, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, L.; Gibson, A.; Hieb, A. Chronic postnatal de-71 exposure: Effects on learning, attention and thyroxine levels. Neurotoxicol. Teratol. 2009, 31, 76–84. [Google Scholar] [CrossRef] [PubMed]






| Study | Exposure Matrix (Sample Size) | Years of Exposure Collection | Measured Congeners | Motor | Behavior | Cognitive | |
|---|---|---|---|---|---|---|---|
| United States | |||||||
| CHAMACOS cohort | |||||||
| Eskenazi et al., 2013 | Salinas Valley, California | Maternal blood during pregnancy or at delivery (n = 279) | 1999–2000 | Primary exposure: ΣPBDEs (BDE-47, -99, -100, and -153) | X | X | X |
| Sagiv et al., 2015 | Salinas Valley, California | Maternal blood during pregnancy or back-extrapolated (n = 622) | 1999–2002; additional 9-year-olds included in 2009–2011 | BDE-17, -28, -47, -66, -85, -99, -100, -153, -154, and -183 | X | X | X |
| HOME cohort | |||||||
| Chen et al., 2014 | Cincinnati, Ohio | Maternal serum at 16 weeks gestation (n = 309) | March 2003–February 2006 | BDE-17, -28, -47, -66, -85, -99, -100, -153, -154, and -183 (with focus on BDE-47) | X | X | X |
| Vuong et al., 2016 | Cincinnati, Ohio | Maternal serum at 4 months’ pregnancy (age 5, n = 201) | 2003–2006 | BDE-17, -28, -47, -66, -85, -99, -100, -153, -154, and -183 | X | X | |
| Zhang et al., 2016 | Cincinnati, Ohio | Maternal serum at 4 months’ pregnancy (n = 239) | 2003–2006 | BDE-17, -28, -47, -66, -85, -99, -100, -153, -154, and -183 | X | X | |
| Braun et al., 2017 | Cincinnati, Ohio | Maternal serum (n = 346) | March 2003–January 2006 | BDE -28, -47, -85, -99, -100, -153, -154 | X | X | X |
| Vuong et al., 2017a | Cincinnati, Ohio | Maternal serum at enrollment (n = 214) | 2003–2006 | BDE-17, -28, -47, -66, -85, -99, -100, -153, -154, and -183 | X | ||
| Vuong et al., 2017b | Cincinnati, Ohio | Maternal serum at 16 weeks’ gestation (n = 199) | 2003–2006 | BDE-17, -28, -47, -66, -85, -99, -100, -153, -154, and -183 | X | ||
| World Trade Center cohort | |||||||
| Herbstman et al., 2010 | New York, NY | Cord blood plasma (n = 152) | 2001–2002; Pregnant as of 9/11 | BDE-47, -99, and -100 | X | X | |
| Cowell et al., 2015 | New York, NY | Cord blood plasma (age 4, n = 109; age 6, n = 107) | December 2001–June 2002 | BDE-47, -85, -99, -100, -153, -154, and -183 | X | ||
| Asia | |||||||
| Shy et al., 2011 | Southern Taiwan | Cord blood (n = 36) | 2007–2008 | BDE-15, -28, -47, -49, -99, -100, -153, -154, -183, -196, and -197 | X | X | X |
| Ding et al., 2015 | Shandong Province, Northern China | Cord blood serum (12 months, n = 192; 24 months, n = 149) | September 2010–February 2012 | BDE-28, -47, -85, -99, -100, -153, -154, and -183 | X | X | X |
| Kim et al., 2018 | Seoul, Anyang, Ansan, and Jeju, Korea | Maternal serum (n = 59) | 2011–2012 | 19 unspecified PBDE congeners | X | X | X |
| Europe | |||||||
| Chevrier et al., 2016 | Brittany Region, France | Cord blood (n = 159); Household dust | 2002–2006 | BDE-47, -85, -99, -100, -119, -153, -154, -183, and -209 | X | ||
| Roze et al., 2009 | Northern Provinces of the Netherlands | Maternal serum at 35th week of pregnancy (n = 62) | October 2001–November 2002 | BDE-47, -99, -100, -153, and -154 | X | X | X |
| Gascon et al., 2011 | Catalonia, Spain | Cord blood (n = 88) | Mid 1997 | BDE-12–13, -32, -17, -28–33, -47, -100, -119, -99, -116, -85, -126, -155, -153, -183, -66, -71, -154, -138, and -190 | X | X | X |
| Study | Roze et al., 2009 | Herbstman et al., 2010 | Gascon et al., 2011 | Shy et al., 2011 | Eskenazi et al., 2013 | Braun et al., 2014 | Chen at al., 2014 | Cowell et al., 2015 | Ding et al., 2015 | Sagiv et al., 2015 | Chevrier et al., 2016 | Vuong et al., 2016 | Braun et al., 2017 | Vuong et al., 2017a | Vuong et al., 2017b | Zhang et al., 2017 | Kim et al., 2018 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cognitive development tests | Bayley 4 | Age | 1, 2, 3 | 1 | 1–3 | 1–3 | |||||||||||||
| Sign 1 | −/+, −, − | − | − | − | |||||||||||||||
| WISC 5 | Age | 5–6 | 4, 7 | 7 | 5 | 10.5 | 6 | 5–8 | 5, 8 | ||||||||||
| Sign 1 | 0 3 | −,− | −/+ | − | − | − | 0 3 | − | − | ||||||||||
| Other 10 | Age | 5–6 | 4 | 5 | 1, 2 | 9, 12 | 5, 8 | 8 | 5, 8 | ||||||||||
| Sign 1 | − | − | 0 3 | 0 3, − | − | −, − | −/+ | −, − | |||||||||||
| Behavioral development tests | BASC 6 | Age | 7 | 2–5 | 10.5 | 2–8 | 5, 8 | ||||||||||||
| Sign 1,2 | − | − | −/+ | − | −,− | ||||||||||||||
| Conners’ 7 | Age | 5, 7 | 9, 12 | 8 | |||||||||||||||
| Sign 1,2 | − | − | 0 3 | ||||||||||||||||
| CBCL 8 | Age | 5–6 | 5 | 3, 4, 5, 6, 7 | 1–2 | ||||||||||||||
| Sign 1,2 | − | − | −, −, 0 3, 0 3, − | − | |||||||||||||||
| Other 11 | Age | 4 | 1 | 4–5 | 1, 2 | 9, 12 | 5, 8 | ||||||||||||
| Sign 1,2 | − | − | −/+ | 0 3, − | − | − | |||||||||||||
| Motor development tests | Bayley 4 | Age | 1, 2, 3 | 1 | 1, 2, 3 | ||||||||||||||
| Sign 1 | −, −/+, −/+ | 0 3 | 0 3 | ||||||||||||||||
| MSCA 9 | Age | 5–6 | 4 | 5, 7 | |||||||||||||||
| Sign 1 | − | − | − | ||||||||||||||||
| Other 12 | Age | 5–6 | 5, 7 | 1–2 | 10.5 | ||||||||||||||
| Sign 1 | − | − | 0 3 | 0 3 | |||||||||||||||
| Author, Year | Braun et al., 2014 | Sagiv et al., 2015 | Zhang et al., 2016 | Vuong et al., 2016 | Chen et al., 2014 | Vuong et al., 2017a | Vuong et al., 2017b | Braun et al., 2017 | Gascon et al., 2011 | Herbstman et al., 2010 | Chevrier et al., 2016 | Cowell et al., 2015 | Kim et al., 2018 | Ding et al., 2015 | Eskenazi et al., 2013 | Roze et al., 2009 | Shy et al., 2011 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted Covariates (Confounders) | Mat. Age | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||
| Gest. Age 1 | √ | √ | √ | |||||||||||||||
| Edu. 1 | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||
| Race | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| Infant sex | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||
| Infant age at testing | √ | √ | √ | √ | √ | |||||||||||||
| BFD 1 | √ | √ | √ | √ | ||||||||||||||
| SES 1 | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||
| Smoking Status 1 | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||
| Maternal IQ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||
| Marital Status | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||
| Parity | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| HOME score 1 | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||
| Other chemicals 1 | √ | √ | √ | √ | ||||||||||||||
| Total | 12 | 11 | 10 | 9 | 9 | 9 | 9 | 8 | 8 | 8 | 7 | 6 | 6 | 5 | 5 | 3 | 2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibson, E.A.; Siegel, E.L.; Eniola, F.; Herbstman, J.B.; Factor-Litvak, P. Effects of Polybrominated Diphenyl Ethers on Child Cognitive, Behavioral, and Motor Development. Int. J. Environ. Res. Public Health 2018, 15, 1636. https://doi.org/10.3390/ijerph15081636
Gibson EA, Siegel EL, Eniola F, Herbstman JB, Factor-Litvak P. Effects of Polybrominated Diphenyl Ethers on Child Cognitive, Behavioral, and Motor Development. International Journal of Environmental Research and Public Health. 2018; 15(8):1636. https://doi.org/10.3390/ijerph15081636
Chicago/Turabian StyleGibson, Elizabeth A., Eva Laura Siegel, Folake Eniola, Julie Beth Herbstman, and Pam Factor-Litvak. 2018. "Effects of Polybrominated Diphenyl Ethers on Child Cognitive, Behavioral, and Motor Development" International Journal of Environmental Research and Public Health 15, no. 8: 1636. https://doi.org/10.3390/ijerph15081636