Interactions of Genes and Sodium Intake on the Development of Hypertension: A Cohort-Based Case-Control Study


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Data Collection
2.3. Definition of Hypertension
2.4. GNB3 C825T Genotyping
2.5. Assessment of Sodium Intake
2.6. Covariates
2.7. Statistical Methods
3. Results
3.1. Study Population
3.2. Independent Effects of GNB3 and Sodium Intake
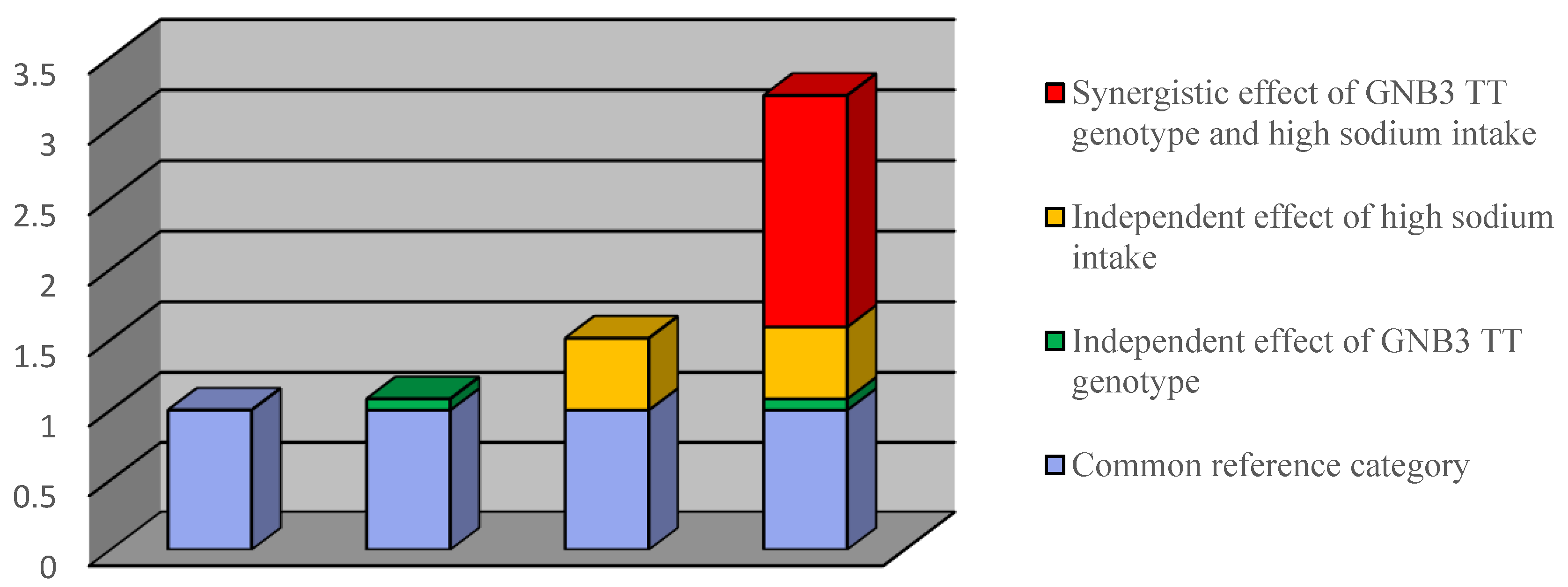
3.3. Joint Effects of GNB3 and Sodium Intake on the Risk of Hypertension
4. Discussion
4.1. Results Validity
4.2. Synthesis with the Previous Knowledge
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| GNB3 | protein beta3 subunit; |
| JNC7 | Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; |
| BP | blood pressure. |
References
- Kelly, T.N.; He, J. Genomic epidemiology of blood pressure salt sensitivity. J. Hypertens. 2012, 30, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, N.; Chasman, D.I.; Cooper-DeHoff, R.M.; Arnett, D.K. Genetic, ancestry and hypertension: Implications for targeted antihypertensive therapies. Curr. Hypertens. Rep. 2014, 16, 461. [Google Scholar] [CrossRef] [PubMed]
- Hamm, H.E. The many faces of G protein signaling. J. Biol. Chem. 1988, 273, 669–672. [Google Scholar] [CrossRef]
- Neves, S.R.; Ram, P.T.; Lyengar, R. G protein pathways. Science 2002, 296, 1636–1639. [Google Scholar] [CrossRef] [PubMed]
- Rosskopf, D.; Busch, S.; Manthey, I.; Siffert, W. G Protein beta3 Gene: Structure, Promoter and Additional Polymorphisms. Hypertension 2000, 36, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Siffert, W.; Rosskopf, D.; Siffert, G.; Busch, S.; Moritz, A.; Erbel, R.; Sharma, A.M.; Ritz, E.; Wichmann, H.E.; Jakobs, K.H.; et al. Association of a human G-protein β3 subunit variant with hypertension. Nat. Genet. 1998, 18, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Bagos, P.G.; Elefsinioti, A.L.; Nikolopoulos, G.K.; Hamodrakas, S.J. The GNB3 C825T polymorphism and essential hypertension: A meta-analysis of 34 studies including 14094 cases and 17760 controls. J. Hypertens 2007, 25, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Niu, W.; Qi, Y. Association of α-adducin and G-protein β3 genetic polymorphisms with hypertension: A meta-analysis of Chinese populations. PLoS ONE 2011, 2, e17052. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.A.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. National High Blood Pressure Education Program Coordinating Committee. Primary prevention of hypertension: Clinical and public health advisory from the National High Blood Pressure Education Program. JAMA 2002, 288, 1882–1888. [Google Scholar] [PubMed]
- Chobanian, A.V.; Hill, M. National Heart, Lung and Blood Institute workshop on sodium and blood pressure: Acritical review of current scientific evidence. Hypertension 1991, 17, 152–158. [Google Scholar] [CrossRef]
- Elijovich, F.; Weinberge, M.H.; Anderson, C.A.; Appel, L.J.; Bursztyn, M.; Cook, N.R.; Dart, R.A.; Newton-Cheh, C.H.; Sacks, F.M.; Laffer, C.L. Salt Sensitivity of Blood Pressure. Hypertension 2016, 68, e7–e46. [Google Scholar] [CrossRef] [PubMed]
- Beeks, E.; Kessels, A.G.H.; Kroon, A.A.; van der Klauw, M.M.; de Leauw, P.W. Genetic predisposition to salt-sensitivity: A systematic review. J. Hypertens. 2004, 22, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Pamies-Andreu, E.; Ramirez-Lorca, R.; García-Junco, P.S.; Muñiz-Grijalbo, O.; Vallejo-Maroto, I.; Morillo, S.G.; Miranda-Guisado, M.L.; Ortíz, J.V.; de la Fuente, J.C. Renin-angiotensin-aldosterone system and G-protein beta-3 subunit gene polymorphisms in salt-sensitive essential hypertension. J. Hum. Hypertens. 2003, 17, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Nunez, D.; Giner, V.; Bragulat, E.; Coca, A.; de la Sierra, A.; Poch, E. Absence of an association between the C825T polymorphism of the G-protein beta3 subunit and salt-sensitivity in essential arterial hypertension. Nefrologia 2001, 21, 355–361. [Google Scholar] [PubMed]
- Grimes, C.A.; Wright, J.D.; Liu, K.; Nowson, C.A.; Loria, C.M. Dietary sodium intake is associated with total fluid and sugar-sweetened beverage consumption in US children and adolescents age 2–18 y: NHANES 2005–2008. Am. J. Clin. Nutr. 2013, 98, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Andersson, P.; Alfredsson, L.; Kallberg, H.; Zdravkovic, S.; Ahlbom, A. Calculating measures of biological interaction. Eur. J. Epidemiol. 2005, 20, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J. The estimation of synergy or antagonism. Am. J. Epidemiol. 1976, 103, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemeshow, S. Confidence interval estimation of interaction. Epidemiology 1992, 3, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Demideniko, E. Sample size and optimal design for logistic regression with binary interaction. Stat. Med. 2008, 27, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, K.; Imai, Y.; Katsuya, T.; Ohkubo, T.; Tsuji, I.; Nagai, K.; Takami, S.; Nakata, Y.; Satoh, H.; Hisamichi, S.; et al. Human G-protein beta3 subunit variant is associated with serum potassium and total cholesterol levels but not with blood pressure. Am. J. Hypertens. 2000, 13, 140–145. [Google Scholar] [CrossRef]
- Takeuchi, F.; Yamamoto, K.; Katsuya, T.; Sugiyama, T.; Nabika, T.; Ohnaka, K.; Yamaguchi, S.; Takayanagi, R.; Ogihara, T.; Kato, N. Reevaluation of the association of seven candidate genes with blood pressure and hypertension: A replication study and meta-analysis with a larger sample size. Hypertens. Res. 2012, 35, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Marques, F.Z.; Campain, A.E.; Yang, Y.H.; Morris, B.J. Meta-analysis of genome-wide gene expression differences in onset and maintenance phases of genetic hypertension. Hypertension 2010, 56, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; Egger, M.; Scott, P.; Greerlings, M.I.; Vandenbroucke, J.P. When one depends on the other: Reporting of interaction in case-control and cohort studies. Epidemiology 2009, 20, 161–166. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J.; Robins, J.M. The identification of synergism in the sufficient-component-cause framework. Epidemiology 2007, 18, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.S. Interaction reaction. Epidemiology 2009, 20, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, E.; Gaddam, K.K.; Oparil, S.; Aban, I.; Husain, S.; Dell’Italia, L.J.; Calhoun, D.A. Effects of dietary sodium reduction on blood pressure in subjects with resistant hypertension: Results from a randomized trial. Hypertension 2009, 54, 475–481. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Cases n (%) | Controls n (%) | OR (95%C.I) | p Value |
|---|---|---|---|---|
| Total | 233 | 699 | ||
| Age (years) | <0.0001 | |||
| ≤40 | 11 (4.7%) | 61 (8.7%) | 1.00 | |
| 41–45 | 44 (18.9%) | 187 (26.8%) | 1.31 (0.63–2.68) | 0.20 |
| 46–50 | 106 (45.5%) | 282 (40.3%) | 2.08 (1.06–4.11) | 0.04 |
| ≥51 | 72 (30.9%) | 169 (24.2%) | 2.36 (1.18–4.75) | 0.0057 |
| Smoking | ||||
| No | 193 (82.8%) | 626 (89.6%) | 1.00 | |
| Yes | 40 (17.2%) | 73 (10.4%) | 1.78 (1.17–2.70) | 0.0070 |
| Alcohol Consumption | ||||
| No | 192 (82.4%) | 624 (89.3%) | 1.00 | |
| Yes | 41 (17.6%) | 75 (10.7%) | 1.78 (1.18–2.69) | 0.0065 |
| BMI (m/kg2) | ||||
| Normal | 88 (37.8%) | 422 (60.4%) | 1.00 | |
| Abnormal | 145 (62.2%) | 277 (39.6%) | 2.51 (1.85–3.41) | <0.0001 |
| TG (mg/dl) | 1.00 | |||
| Normal | 74 (31.8%) | 528 (75.5%) | ||
| High (>1000) | 159 (68.2%) | 171 (24.5%) | 6.63 (4.79–9.18) | <0.0001 |
| HDL (mg/dl) | ||||
| Normal | 132 (56.7%) | 540 (77.3%) | 1.00 | |
| Low (M: <40; F: <50) | 101 (43.3%) | 159 (22.7%) | 2.60 (1.90–3.56) | <0.0001 |
| LDL (mg/dl) | ||||
| Normal | 194 (83.3%) | 622 (89.0%) | 1.00 | |
| High (>150) | 39 (16.7%) | 77 (11.0%) | 1.62 (1.07–2.47) | 0.0228 |
| Vegetable intakes | ||||
| 71–100% | 67 (28.8%) | 279 (40.7%) | 1.00 | |
| 51–70% | 125 (53.6%) | 263 (38.3%) | 1.98 (1.41–2.78) | 0.0001 |
| <50% | 41 (17.6%) | 144 (21.0%) | 1.19 (0.77–1.84) | 0.3858 |
| Creatinine (mg/dl) | ||||
| Normal (0.6–1.4) | 221 (94.9%) | 536 (96.9%) | 1.00 | |
| Abnormal (<0.6 or >1.4) | 12 (5.2%) | 17 (3.1%) | 1.71 (0.80–3.65) | 0.1629 |
| Uric acid (mg/dl) | ||||
| Normal (2.5–7.5) | 196 (84.1%) | 434 (88.3%) | 1.00 | |
| Abnormal(<2.5 or >7.5) | 37 (15.9%) | 65 (11.7%) | 1.42 (0.92–2.20) | 0.12 |
| Urine protein (g/L) | ||||
| Normal (<0.1) | 208 (96.3%) | 513 (97.5%) | 1.00 | |
| Abnormal (≥0.1) | 8 (3.7%) | 13 (2.5%) | 1.52 (0.62–3.72) | 0.3609 |
| Diabetes mellitus | ||||
| No | 221 (94.8%) | 686 (98.1%) | 1.00 | |
| Yes | 12 (5.2%) | 13 (1.9%) | 2.86 (1.29–6.37) | 0.0099 |
| Thyroid disease | ||||
| No | 230 (98.7%) | 693 (99.1%) | 1.00 | |
| Yes | 3 (1.3%) | 6 (0.9%) | 1.51 (0.37–6.07) | 0.5642 |
| GNB3 | Cases n (%) | Controls n (%) | OR (95%C.I) | aOR (95%C.I) * | p Value |
|---|---|---|---|---|---|
| Total | 233 | 699 | |||
| CC + TC | 160 (68.7%) | 501 (71.7%) | 1.00 | 1.00 | |
| TT | 73 (31.3%) | 198 (28.3%) | 1.15 (0.84–1.59) | 1.21 (0.85–1.74) | 0.2929 |
| Sodium Intake | Cases n (%) | Controls n (%) | OR (95%C.I) | aOR (95%C.I) * | p Value |
|---|---|---|---|---|---|
| Total | 233 | 699 | |||
| Healthy salt intake ≤ 2500 mg (roughly 1 teaspoon of salt) | 182 (78.1%) | 621 (88.8%) | 1.00 | 1.00 | |
| High salt intake > 5000 mg (roughly 2 teaspoons of salt) | 51 (21.9%) | 78 (11.2%) | 2.23 (1.51–3.29) | 1.88 (1.20–2.94) | <0.0001 |
| Combination of GNB3 Gene and Sodium Intake | Cases n (%) | Controls n (%) | OR (95%C.I) | aOR (95%C.I) * | p Value |
|---|---|---|---|---|---|
| Total | 233 | 699 | |||
| CC or TC + Healthy sodium intake | 128 (54.9%) | 446 (63.8%) | 1.00 | 1.00 | |
| CC or TC + High sodium intake | 32 (13.7%) | 55 (7.9%) | 2.03 (1.26–3.27) | 1.51 (0.88–2.60) | 0.1916 |
| TT + Healthy sodium intake | 54 (23.2%) | 175 (25.0%) | 1.08 (0.75–1.55) | 1.08 (0.72–1.61) | 0.0114 |
| TT + High sodium intake | 19 (8.2%) | 23 (3.3%) | 2.88 (1.52–5.45) | 3.23 (1.52–6.83) | 0.0140 |
| Attributable proportion due to interaction (AP) | 0.51 (0.07–0.95) | ||||
| Rothman synergy index | 3.79 (0.58–24.66) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.-L.; Huang, T.-P.; Chen, T.-W.; Chan, H.-H.; Hwang, B.-F. Interactions of Genes and Sodium Intake on the Development of Hypertension: A Cohort-Based Case-Control Study. Int. J. Environ. Res. Public Health 2018, 15, 1110. https://doi.org/10.3390/ijerph15061110
Chen M-L, Huang T-P, Chen T-W, Chan H-H, Hwang B-F. Interactions of Genes and Sodium Intake on the Development of Hypertension: A Cohort-Based Case-Control Study. International Journal of Environmental Research and Public Health. 2018; 15(6):1110. https://doi.org/10.3390/ijerph15061110
Chicago/Turabian StyleChen, Mei-Ling, Tzu-Pi Huang, Tai-Wei Chen, Hsin-Hua Chan, and Bing-Fang Hwang. 2018. "Interactions of Genes and Sodium Intake on the Development of Hypertension: A Cohort-Based Case-Control Study" International Journal of Environmental Research and Public Health 15, no. 6: 1110. https://doi.org/10.3390/ijerph15061110