Increased Expression of Meteorin-Like Hormone in Type 2 Diabetes and Obesity and Its Association with Irisin


 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Blood and Tissue Sampling
2.3. Anthropometric Measurements and Blood Biochemistry
2.4. Measurement of Plasma Levels of METRNL and Irisin Using ELISA
2.5. Statistics
3. Results
3.1. Characteristics of the Study Population
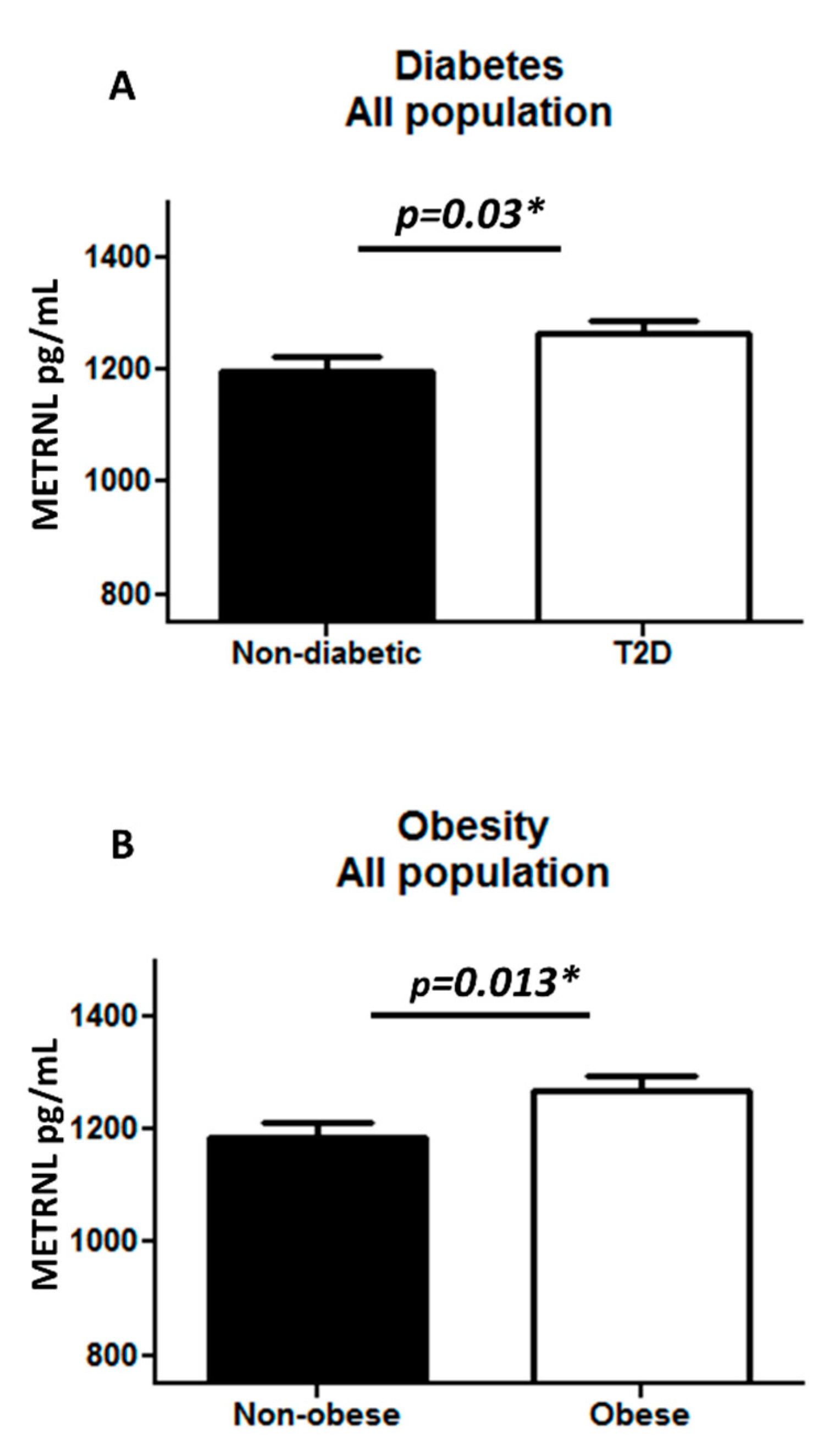
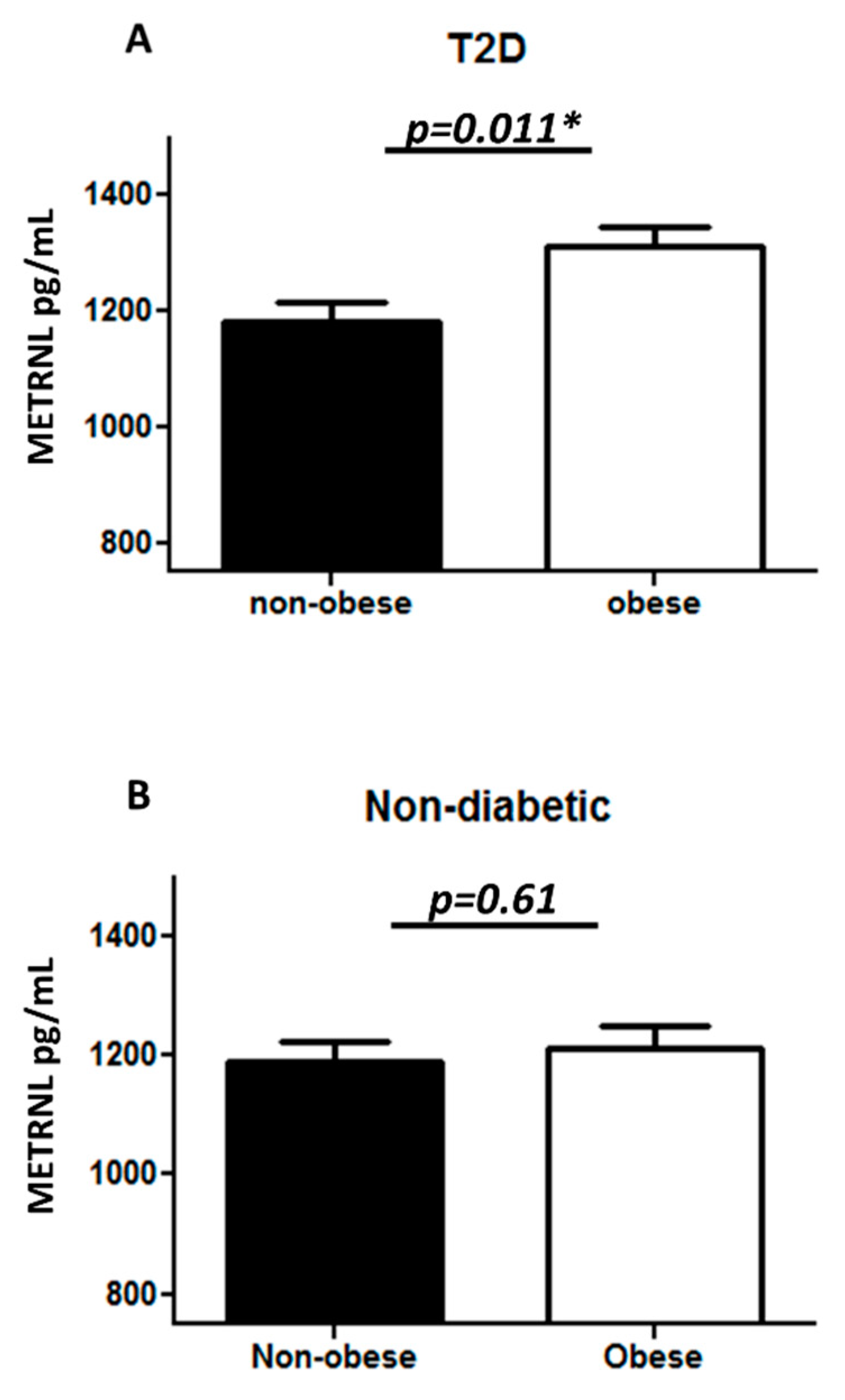
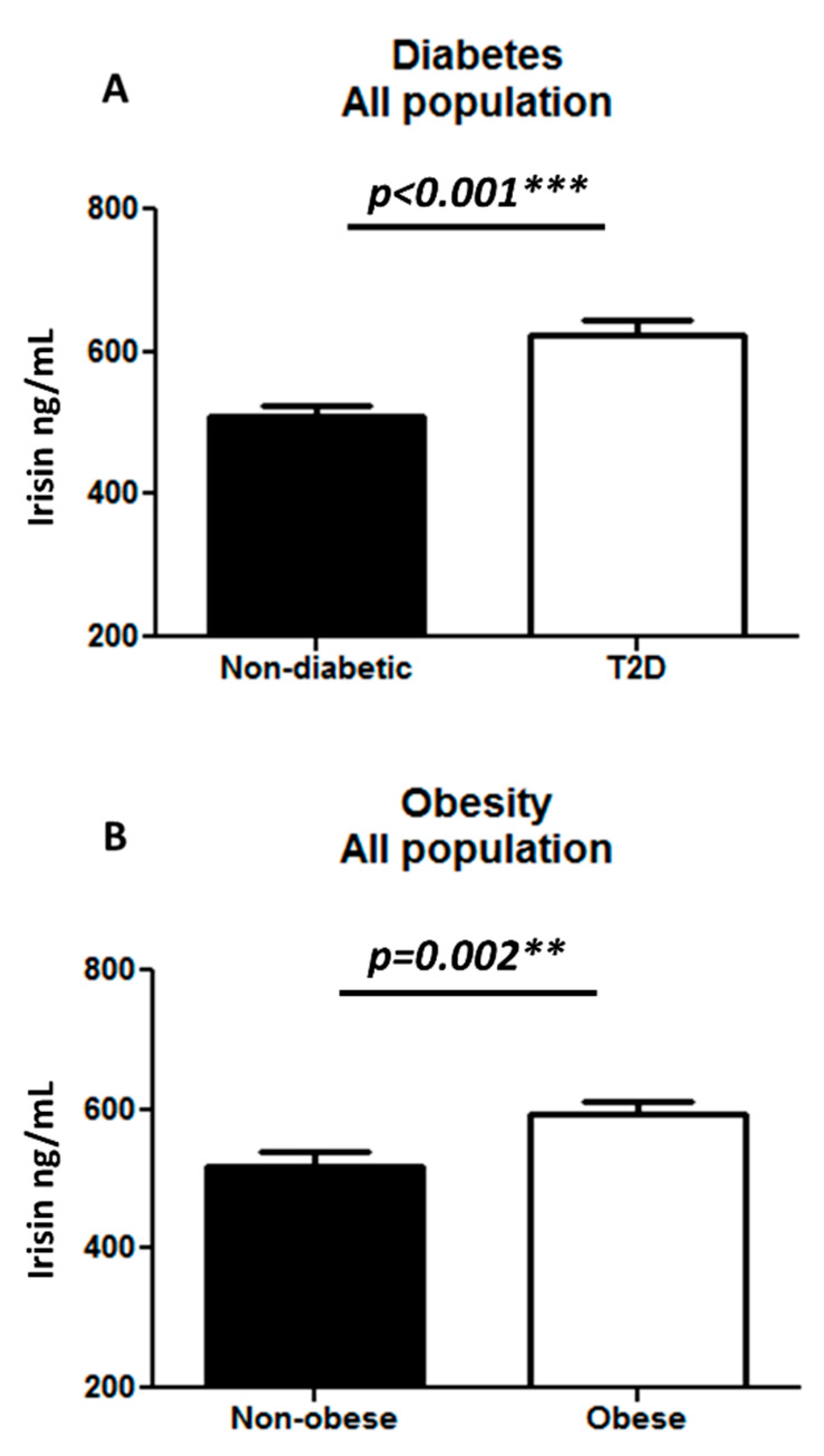
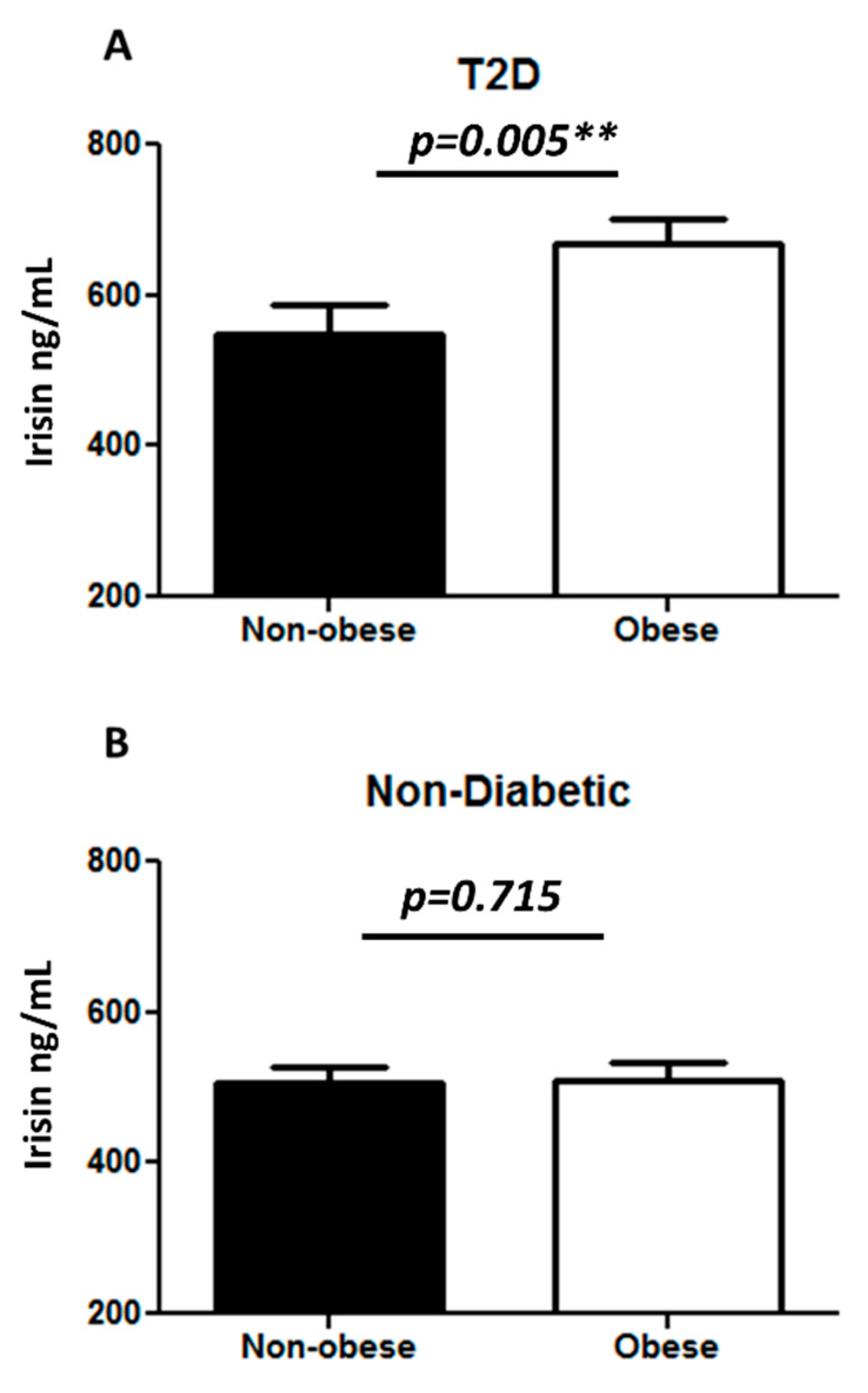
3.2. METRNL and Irisin Expression in the Circulation
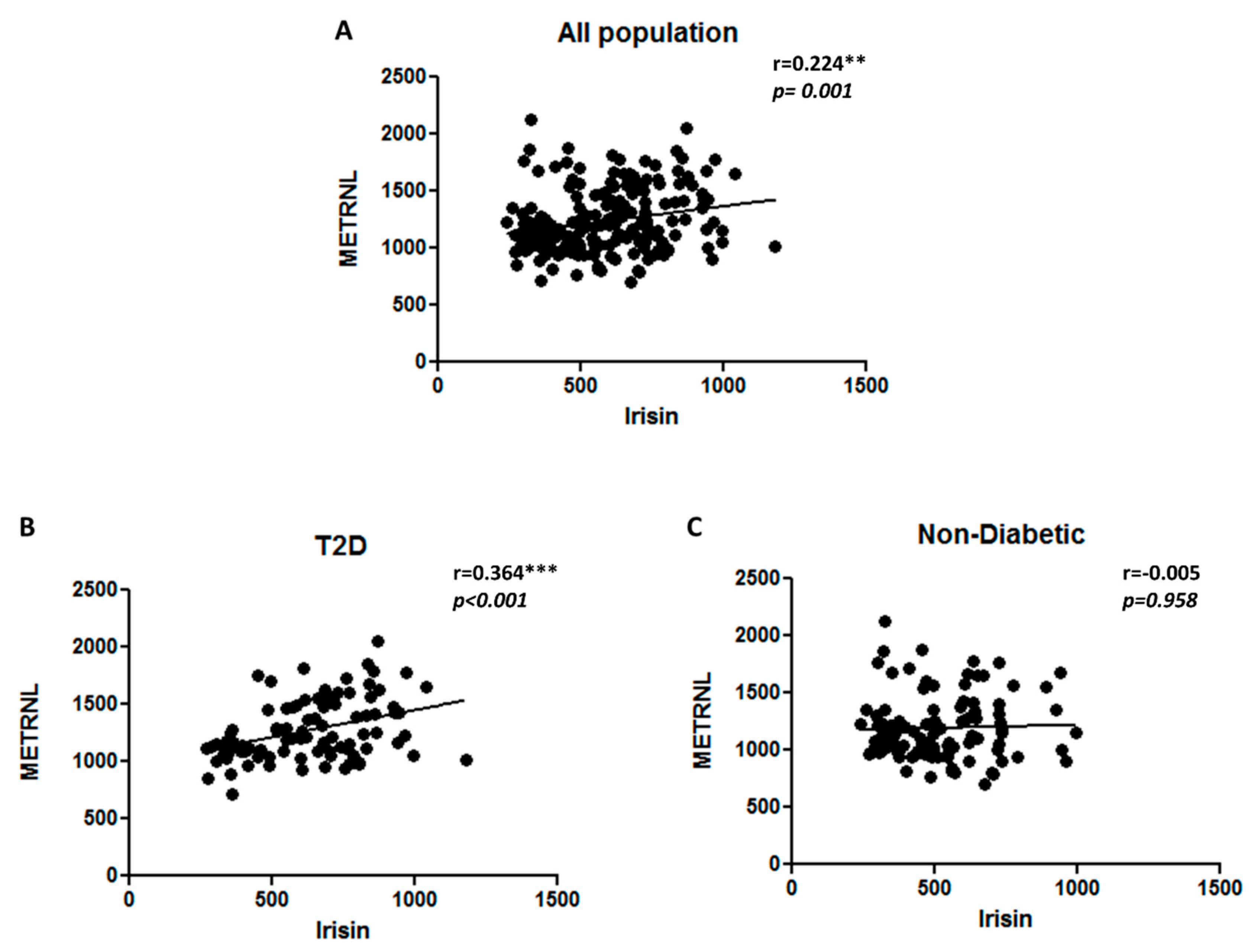
3.3. Correlation Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schlienger, J.L. Type 2 diabetes complications. Presse Med. 2013, 42, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- Lin, Y.; Sun, Z. Current views on type 2 diabetes. J. Endocrinol. 2010, 204, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.R.; Nachbar, R.T.; Gorjao, R.; Vinolo, M.A.; Festuccia, W.T.; Lambertucci, R.H.; Cury-Boaventura, M.F.; Silveira, L.R.; Curi, R.; Hirabara, S.M. Mechanisms underlying skeletal muscle insulin resistance induced by fatty acids: Importance of the mitochondrial function. Lipids Health Dis. 2012, 11, 30. [Google Scholar] [CrossRef]
- Turner, N.; Kowalski, G.M.; Leslie, S.J.; Risis, S.; Yang, C.; Lee-Young, R.S.; Babb, J.R.; Meikle, P.J.; Lancaster, G.I.; Henstridge, D.C.; et al. Distinct patterns of tissue-specific lipid accumulation during the induction of insulin resistance in mice by high-fat feeding. Diabetologia 2013, 56, 1638–1648. [Google Scholar] [CrossRef]
- Eckardt, K.; Gorgens, S.W.; Raschke, S.; Eckel, J. Myokines in insulin resistance and type 2 diabetes. Diabetologia 2014, 57, 1087–1099. [Google Scholar] [CrossRef]
- Pedersen, L.; Hojman, P. Muscle-to-organ cross talk mediated by myokines. Adipocyte 2012, 1, 164–167. [Google Scholar] [CrossRef] [Green Version]
- Schnyder, S.; Handschin, C. Skeletal muscle as an endocrine organ: PGC-1alpha, myokines and exercise. Bone 2015, 80, 115–125. [Google Scholar] [CrossRef]
- Oh, K.J.; Lee, D.S.; Kim, W.K.; Han, B.S.; Lee, S.C.; Bae, K.H. Metabolic Adaptation in Obesity and Type II Diabetes: Myokines, Adipokines and Hepatokines. Int. J. Mol. Sci. 2016, 18, 8. [Google Scholar] [CrossRef]
- Lee, J.H.; Jun, H.-S. Role of Myokines in Regulating Skeletal Muscle Mass and Function. Front. Physiol. 2019, 10, 42. [Google Scholar] [CrossRef]
- Esterbauer, H.; Oberkofler, H.; Krempler, F.; Patsch, W. Human peroxisome proliferator activated receptor gamma coactivator 1 (PPARGC1) gene: cDNA sequence, genomic organization, chromosomal localization, and tissue expression. Genomics 1999, 62, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Attie, A.D.; Kendziorski, C.M. PGC-1alpha at the crossroads of type 2 diabetes. Nat. Genet. 2003, 34, 244–245. [Google Scholar] [CrossRef] [PubMed]
- Lukaszuk, B.; Kurek, K.; Miklosz, A.; Zendzian-Piotrowska, M.; Chabowski, A. The Role of PGC-1alpha in the Development of Insulin Resistance in Skeletal Muscle—Revisited. Cell. Physiol. Biochem. 2015, 37, 2288–2296. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Kim, K. Exercise-induced PGC-1alpha transcriptional factors in skeletal muscle. Integr. Med. Res. 2014, 3, 155–160. [Google Scholar] [CrossRef]
- Lira, V.A.; Benton, C.R.; Yan, Z.; Bonen, A. PGC-1alpha regulation by exercise training and its influences on muscle function and insulin sensitivity. Am. J. Physiol. Endocrinol. Metab. 2010, 299, E145–E161. [Google Scholar] [CrossRef]
- Bostrom, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Bostrom, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1-alpha-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature 2012, 481, 463–468. [Google Scholar] [CrossRef]
- Roberts, L.D.; Bostrom, P.; O’Sullivan, J.F.; Schinzel, R.T.; Lewis, G.D.; Dejam, A.; Lee, Y.K.; Palma, M.J.; Calhoun, S.; Georgiadi, A.; et al. beta-Aminoisobutyric acid induces browning of white fat and hepatic beta-oxidation and is inversely correlated with cardiometabolic risk factors. Cell Metab. 2014, 19, 96–108. [Google Scholar] [CrossRef]
- Rao, R.R.; Long, J.Z.; White, J.P.; Svensson, K.J.; Lou, J.; Lokurkar, I.; Jedrychowski, M.P.; Ruas, J.L.; Wrann, C.D.; Lo, J.C.; et al. Meteorin-like is a hormone that regulates immune-adipose interactions to increase beige fat thermogenesis. Cell 2014, 157, 1279–1291. [Google Scholar] [CrossRef]
- Carobbio, S.; Guenantin, A.C.; Samuelson, I.; Bahri, M.; Vidal-Puig, A. Brown and beige fat: From molecules to physiology and pathophysiology. Biochim. Biophys. Acta Mol. Cell. Biol. Lipids 2019, 1864, 37–50. [Google Scholar] [CrossRef]
- Novelle, M.G.; Contreras, C.; Romero-Pico, A.; Lopez, M.; Dieguez, C. Irisin, two years later. Int. J. Endocrinol. 2013, 2013, 746281. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Ortega, F.; Serrano, M.; Guerra, E.; Pardo, G.; Tinahones, F.; Ricart, W.; Fernandez-Real, J.M. Irisin is expressed and produced by human muscle and adipose tissue in association with obesity and insulin resistance. J. Clin. Endocrinol. Metab. 2013, 98, E769–E778. [Google Scholar] [CrossRef] [PubMed]
- Varela-Rodriguez, B.M.; Pena-Bello, L.; Juiz-Valina, P.; Vidal-Bretal, B.; Cordido, F.; Sangiao-Alvarellos, S. FNDC5 expression and circulating irisin levels are modified by diet and hormonal conditions in hypothalamus, adipose tissue and muscle. Sci. Rep. 2016, 6, 29898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, X.Q.; Chen, D.; Sun, H.J.; Ding, L.; Wang, J.J.; Chen, Q.; Li, Y.H.; Zhou, Y.B.; Han, Y.; Zhang, F.; et al. FNDC5 overexpression and irisin ameliorate glucose/lipid metabolic derangements and enhance lipolysis in obesity. Biochim. Biophys. Acta 2015, 1852, 1867–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2008, 31, S55–S60. [Google Scholar] [CrossRef]
- Abu-Farha, M.; Abubaker, J.; Al-Khairi, I.; Cherian, P.; Noronha, F.; Hu, F.B.; Behbehani, K.; Elkum, N. Higher plasma betatrophin/ANGPTL8 level in Type 2 Diabetes subjects does not correlate with blood glucose or insulin resistance. Sci. Rep. 2015, 5, 10949. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Gizaw, M.; Anandakumar, P.; Debela, T. A Review on the Role of Irisin in Insulin Resistance and Type 2 Diabetes Mellitus. J. Pharmacopuncture 2017, 20, 235–242. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, R.; Meng, Y.; Li, S.; Donelan, W.; Zhao, Y.; Qi, L.; Zhang, M.; Wang, X.; Cui, T.; et al. Irisin stimulates browning of white adipocytes through mitogen-activated protein kinase p38 MAP kinase and ERK MAP kinase signaling. Diabetes 2014, 63, 514–525. [Google Scholar] [CrossRef]
- Zheng, S.L.; Li, Z.Y.; Song, J.; Liu, J.M.; Miao, C.Y. Metrnl: A secreted protein with new emerging functions. Acta Pharmacol. Sin. 2016, 37, 571–579. [Google Scholar] [CrossRef]
- Pardo, M.; Crujeiras, A.B.; Amil, M.; Aguera, Z.; Jimenez-Murcia, S.; Banos, R.; Botella, C.; de la Torre, R.; Estivill, X.; Fagundo, A.B.; et al. Association of irisin with fat mass, resting energy expenditure, and daily activity in conditions of extreme body mass index. Int. J. Endocrinol. 2014, 2014, 857270. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Mohammed, A.K.; Al-Attas, O.S.; Amer, O.E.; Clerici, M.; Alenad, A.; Alokail, M.S. SNPs in FNDC5 (irisin) are associated with obesity and modulation of glucose and lipid metabolism in Saudi subjects. Lipids Health Dis. 2016, 15, 54. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Hwang, S.Y.; Choi, J.H.; Lee, H.J.; Kim, N.H.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Baik, S.H.; et al. Implications of circulating Meteorin-like (Metrnl) level in human subjects with type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 136, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Ahn, S.V.; Choi, J.H.; Koh, S.B.; Chung, C.H. High Serum Irisin Level as an Independent Predictor of Diabetes Mellitus: A Longitudinal Population-Based Study. Medicine (Baltimore) 2016, 95, e3742. [Google Scholar] [CrossRef]
- Rana, K.S.; Pararasa, C.; Afzal, I.; Nagel, D.A.; Hill, E.J.; Bailey, C.J.; Griffiths, H.R.; Kyrou, I.; Randeva, H.S.; Bellary, S.; et al. Plasma irisin is elevated in type 2 diabetes and is associated with increased E-selectin levels. Cardiovasc. Diabetol. 2017, 16, 147. [Google Scholar] [CrossRef]
- Stengel, A.; Hofmann, T.; Goebel-Stengel, M.; Elbelt, U.; Kobelt, P.; Klapp, B.F. Circulating levels of irisin in patients with anorexia nervosa and different stages of obesity--correlation with body mass index. Peptides 2013, 39, 125–130. [Google Scholar] [CrossRef]
- Sanchis-Gomar, F.; Perez-Quilis, C. The p38-PGC-1alpha-irisin-betatrophin axis: Exploring new pathways in insulin resistance. Adipocyte 2014, 3, 67–68. [Google Scholar] [CrossRef]
- Shoukry, A.; Shalaby, S.M.; El-Arabi Bdeer, S.; Mahmoud, A.A.; Mousa, M.M.; Khalifa, A. Circulating serum irisin levels in obesity and type 2 diabetes mellitus. IUBMB Life 2016, 68, 544–556. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Nelson, A.J. HDL and cardiovascular disease. Pathology 2019, 51, 142–147. [Google Scholar] [CrossRef]
- Choi, Y.K.; Kim, M.K.; Bae, K.H.; Seo, H.A.; Jeong, J.Y.; Lee, W.K.; Kim, J.G.; Lee, I.K.; Park, K.G. Serum irisin levels in new-onset type 2 diabetes. Diabetes Res. Clin. Pract. 2013, 100, 96–101. [Google Scholar] [CrossRef]
- Kurdiova, T.; Balaz, M.; Vician, M.; Maderova, D.; Vlcek, M.; Valkovic, L.; Srbecky, M.; Imrich, R.; Kyselovicova, O.; Belan, V.; et al. Effects of obesity, diabetes and exercise on Fndc5 gene expression and irisin release in human skeletal muscle and adipose tissue: In vivo and in vitro studies. J. Physiol. 2014, 592, 1091–1107. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Ding, Z.; Lv, G.; Li, J.; Zhou, P.; Zhang, J. Lower irisin level in patients with type 2 diabetes mellitus: A case-control study and meta-analysis. J. Diabetes 2016, 8, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kang, Y.E.; Kim, J.M.; Choung, S.; Joung, K.H.; Kim, H.J.; Ku, B.J. Serum Meteorin-like protein levels decreased in patients newly diagnosed with type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 135, 7–10. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phenotype | Non-Diabetic (n = 123) | T2D (n = 104) | p-Value |
|---|---|---|---|
| Gender (M/F) | M (45); F (78) | M (55); F (49) | |
| Age (years) | 41.80 ± 1.10 | 52.30 ± 0.91 | <0.001 |
| † BMI (kg/m2) | 28.86 ± 0.48 | 31.62 ± 0.42 | <0.001 |
| Waist/Hip ratio | 0.86 ± 0.01 | 0.96 ± 0.02 | <0.001 |
| ‡ TC (mmol/L) | 5.09 ± 0.09 | 4.89 ± 0.13 | 0.207 |
| § HDL (mmol/L) | 1.37 ± 0.04 | 1.18 ± 0.05 | <0.001 |
| ‖ LDL (mmol/L) | 3.20 ± 0.08 | 3.00 ± 0.11 | 0.155 |
| ¶ TG (mmol/L) | 1.16 ± 0.08 | 1.63 ± 0.11 | <0.001 |
| †† FBG (mg/L) | 95.76 ± 1.8 | 146.88 ± 5.4 | <0.001 |
| ‡‡ HbA1c (DCCT%) | 5.56 ± 0.06 | 7.68 ± 0.18 | <0.001 |
| Insulin (mU/L) | 9.15 ± 0.61 | 15.17 ± 1.19 | <0.001 |
| C-peptide (μg/L) | 3.89 ± 0.35 | 2.76 ± 0.24 | 0.008 |
| §§ HOMA-IR (AU) | 0.53 ± 0.04 | 0.86 ± 0.06 | <0.001 |
| ¶¶ HOMA-β (AU) | 28.49 ± 1.89 | 14.82 ± 1.19 | <0.001 |
| Phenotype | Non-Obese (n = 111) | Obese (n = 117) | p-Value |
|---|---|---|---|
| Gender (M/F) | M (47); F (64) | M (53); F (63) | |
| Age (years) | 44.20 ± 1.17 | 48.91 ± 1.07 | <0.001 |
| † BMI (kg/m2) | 25.86 ± 0.27 | 34.21 ± 0.26 | <0.001 |
| Waist/Hip ratio | 0.86 ± 0.01 | 0.94 ± 0.02 | <0.001 |
| ‡ TC (mmol/L) | 5.01 ± 0.12 | 5.00 ± 0.10 | 0.927 |
| § HDL (mmol/L) | 1.34 ± 0.05 | 1.23 ± 0.04 | 0.077 |
| ‖ LDL (mmol/L) | 3.13 ± 0.10 | 3.10 ± 0.09 | 0.754 |
| ¶ TG (mmol/L) | 1.25 ± 0.10 | 1.49 ± 0.10 | 0.081 |
| †† FBG (mg/L) | 106.38 ± 3.42 | 131.40 ± 5.04 | <0.001 |
| ‡‡ HbA1c (DCCT%) | 5.95 ± 0.11 | 7.09 ± 0.18 | <0.001 |
| Insulin (mU/L) | 11.78 ± 1.01 | 12.57 ± 1.00 | 0.577 |
| C-peptide (μg/L) | 3.22 ± 0.32 | 3.45 ± 0.30 | 0.594 |
| §§ HOMA-IR (AU) | 0.58 ± 0.27 | 0.79 ± 0.05 | 0.002 |
| ¶¶ HOMA-β (AU) | 22.83 ± 1.53 | 20.74 ± 1.86 | 0.386 |
| Phenotype | Non-Diabetic (n = 124) | Diabetic (n = 104) | ||||
|---|---|---|---|---|---|---|
| Non-Obese (n = 73) | Obese (n = 51) | p-Value | Non-Obese (n = 38) | Obese (n = 66) | p-Value | |
| Gender (M/F) | M (26); F (47) | M (19); F (31) | M (21); F (17) | M (34); F (32) | ||
| Age (years) | 40.5 ± 1.40 | 43.64 ± 1.77 | 0.171 | 51.24 ± 1.60 | 52.91 ± 1.11 | 0.392 |
| † BMI (kg/m2) | 25.31 ± 0.35 | 34.04 ± 0.45 | <0.001 | 26.89 ± 0.37 | 34.34 ± 0.30 | <0.001 |
| Waist/Hip ratio | 0.83 ± 0.02 | 0.89 ± 0.01 | 0.005 | 0.92 ± 0.02 | 0.98 ± 0.03 | 0.072 |
| ‡ TC (mmol/L) | 5.10 ± 0.11 | 5.09 ± 0.14 | 0.939 | 4.84 ± 0.27 | 4.93 ± 0.14 | 0.769 |
| § HDL (mmol/L) | 1.39 ± 0.05 | 1.34 ± 0.05 | 0.478 | 1.23 ± 0.10 | 1.15 ± 0.05 | 0.435 |
| ‖ LDL (mmol/L) | 3.19 ± 0.1 | 3.21 ± 0.13 | 0.897 | 3.02 ± 0.21 | 3.0 ± 0.13 | 0.918 |
| ¶ TG (mmol/L) | 1.12 ± 0.12 | 1.214 ± 0.10 | 0.532 | 1.50 ± 0.18 | 1.71 ± 0.15 | 0.373 |
| †† FBG (mg/L) | 94.14 ± 2.7 | 98.1 ± 2.34 | 0.267 | 129.78 ± 6.84 | 156.6 ± 7.38 | 0.009 |
| ‡‡ HbA1c (DCCT %) | 5.56 ± 0.09 | 5.57 ± 0.08 | 0.892 | 6.66 ± 0.21 | 8.23 ± 0.22 | <0.001 |
| Insulin (mU/L) | 8.96 ± 0.79 | 9.58 ± 0.91 | 0.609 | 16.80 ± 2.16 | 14.13 ± 1.37 | 0.3 |
| C-peptide (μg/L) | 3.65 ± 0.43 | 4.22 ± 0.59 | 0.438 | 2.48 ± 0.40 | 2.91 ± 0.29 | 0.38 |
| §§ HOMA-IR (AU) | 5.10 ± 1.53 | 3.91 ± 0.92 | 0.51 | 0.79 ± 0.11 | 0.89 ± 0.06 | 0.448 |
| ¶¶ HOMA-β (AU) | 0.44 ± 0.03 | 0.65 ± 0.07 | 0.008 | 15.90 ± 1.88 | 14.24 ± 1.53 | 0.495 |
| Phenotype (All Populations) | METRNL | Irisin | ||
|---|---|---|---|---|
| r2 | p-Value | r2 | p-Value | |
| † BMI (kg/m2) | 0.206 ** | 0.002 | 0.245 *** | <0.001 |
| Waist/Hip ratio | 0.113 | 0.168 | 0.052 | 0.546 |
| ‡ TC (mmol/L) | 0.040 | 0.556 | 0.260 *** | <0.001 |
| § HDL (mmol/L) | −0.110 | 0.103 | −0.196 ** | 0.004 |
| ‖ LDL (mmol/L) | 0.087 | 0.197 | 0.240 *** | <0.001 |
| ¶ TG (mmol/L) | 0.083 | 0.221 | 0.377 *** | <0.001 |
| †† FBG (mg/L) | 0.128 | 0.058 | 0.224 ** | 0.001 |
| ‡‡ HbA1c (DCCT %) | 0.137 * | 0.044 | 0.256 *** | <0.001 |
| Insulin (mU/L) | 0.118 | 0.142 | 0.145 | 0.058 |
| C-peptide (μg/L) | 0.056 | 0.503 | −0.064 | 0.476 |
| §§ HOMA-IR (AU) | −0.024 | 0.750 | 0.127 | 0.086 |
| ¶¶ HOMA-β (AU) | −0.096 | 0.199 | −0.117 | 0.113 |
| Phenotype (T2D) | METRNL | Irisin | ||
|---|---|---|---|---|
| r2 | p-Value | r2 | p-Value | |
| † BMI (kg/m2) | 0.239 * | 0.015 | 0.292 ** | 0.005 |
| Waist/Hip ratio | 0.119 | 0.317 | 0.057 | 0.642 |
| ‡ TC (mmol/L) | 0.207 * | 0.039 | 0.321 ** | 0.002 |
| § HDL (mmol/L) | −0.013 | 0.896 | −0.114 | 0.289 |
| ‖ LDL (mmol/L) | 0.189 | 0.062 | 0.238 * | 0.025 |
| ¶ TG (mmol/L) | 0.133 | 0.188 | 0.416 *** | <0.001 |
| †† FBG (mg/L) | 0.083 | 0.407 | 0.213 * | 0.043 |
| ‡‡ HbA1c (DCCT%) | 0.126 | 0.210 | 0.202 | 0.056 |
| Insulin (mU/L) | 0.067 | 0.565 | 0.150 | 0.189 |
| C-peptide (μg/L) | 0.173 | 0.180 | 0.048 | 0.738 |
| §§ HOMA-IR (AU) | −0.073 | 0.494 | −0.025 | 0.815 |
| ¶¶ HOMA-β (AU) | −0.120 | 0.262 | −0.231 * | 0.029 |
| Phenotype (Non-Diabetic) | METRNL | Irisin | ||
|---|---|---|---|---|
| r2 | p-Value | r2 | p-Value | |
| † BMI (kg/m2) | 0.120 | 0.188 | 0.132 | 0.146 |
| Waist/Hip ratio | −0.001 | 0.992 | −0.120 | 0.327 |
| ‡ TC (mmol/L) | −0.078 | 0.400 | 0.243 ** | 0.007 |
| § HDL (mmol/L) | −0.115 | 0.212 | −0.211 * | 0.020 |
| ‖ LDL (mmol/L) | 0.017 | 0.852 | 0.262 ** | 0.004 |
| ¶ TG (mmol/L) | −0.041 | 0.659 | 0.289 ** | 0.001 |
| †† FBG (mg/L) | −0.059 | 0.522 | 0.039 | 0.674 |
| ‡‡ HbA1c (DCCT%) | 0.019 | 0.842 | 0.226 * | 0.015 |
| Insulin (mU/L) | 0.072 | 0.534 | 0.044 | 0.676 |
| C-peptide (μg/L) | −0.051 | 0.652 | −0.222 | 0.059 |
| §§ HOMA-IR (AU) | −0.102 | 0.340 | 0.155 | 0.138 |
| ¶¶ HOMA-β (AU) | −0.030 | 0.778 | 0.177 | 0.089 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlKhairi, I.; Cherian, P.; Abu-Farha, M.; Madhoun, A.A.; Nizam, R.; Melhem, M.; Jamal, M.; Al-Sabah, S.; Ali, H.; Tuomilehto, J.; et al. Increased Expression of Meteorin-Like Hormone in Type 2 Diabetes and Obesity and Its Association with Irisin. Cells 2019, 8, 1283. https://doi.org/10.3390/cells8101283
AlKhairi I, Cherian P, Abu-Farha M, Madhoun AA, Nizam R, Melhem M, Jamal M, Al-Sabah S, Ali H, Tuomilehto J, et al. Increased Expression of Meteorin-Like Hormone in Type 2 Diabetes and Obesity and Its Association with Irisin. Cells. 2019; 8(10):1283. https://doi.org/10.3390/cells8101283
Chicago/Turabian StyleAlKhairi, Irina, Preethi Cherian, Mohamed Abu-Farha, Ashraf Al Madhoun, Rasheeba Nizam, Motasem Melhem, Mohamed Jamal, Suleiman Al-Sabah, Hamad Ali, Jaakko Tuomilehto, and et al. 2019. "Increased Expression of Meteorin-Like Hormone in Type 2 Diabetes and Obesity and Its Association with Irisin" Cells 8, no. 10: 1283. https://doi.org/10.3390/cells8101283