
Comparison of RNA Marker Panels for Circulating Tumor Cells and Evaluation of Their Prognostic Relevance in Breast Cancer

 , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Blood Samples
2.2. Processing of Blood Samples from Metastatic Breast Cancer
2.3. Processing of Blood Samples from Early Breast Cancer
2.4. Spiking Experiment Histopaque
2.5. mRNA Isolation
2.6. Preamplification and TaqMan®-Based qPCR
2.7. CK19 RT-qPCR Using FRET Probes
2.8. Calculation of Cut-Off Threshold Values
2.9. Statistics
3. Results
3.1. Spiking Experiment Histopaque Density Gradient Centrifugation
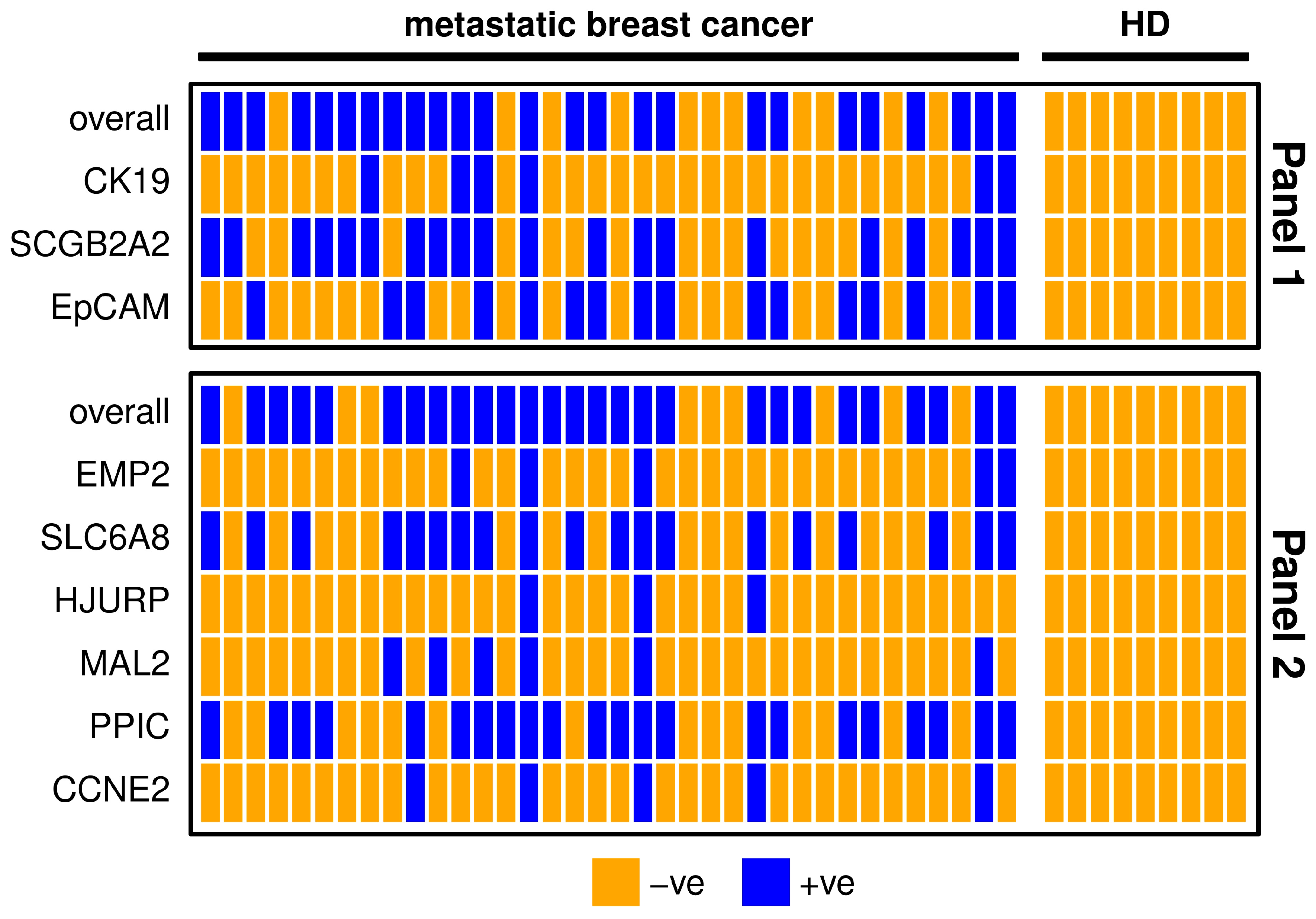
3.2. Evaluation of Gene Panels in Metastatic Breast Cancer Patients
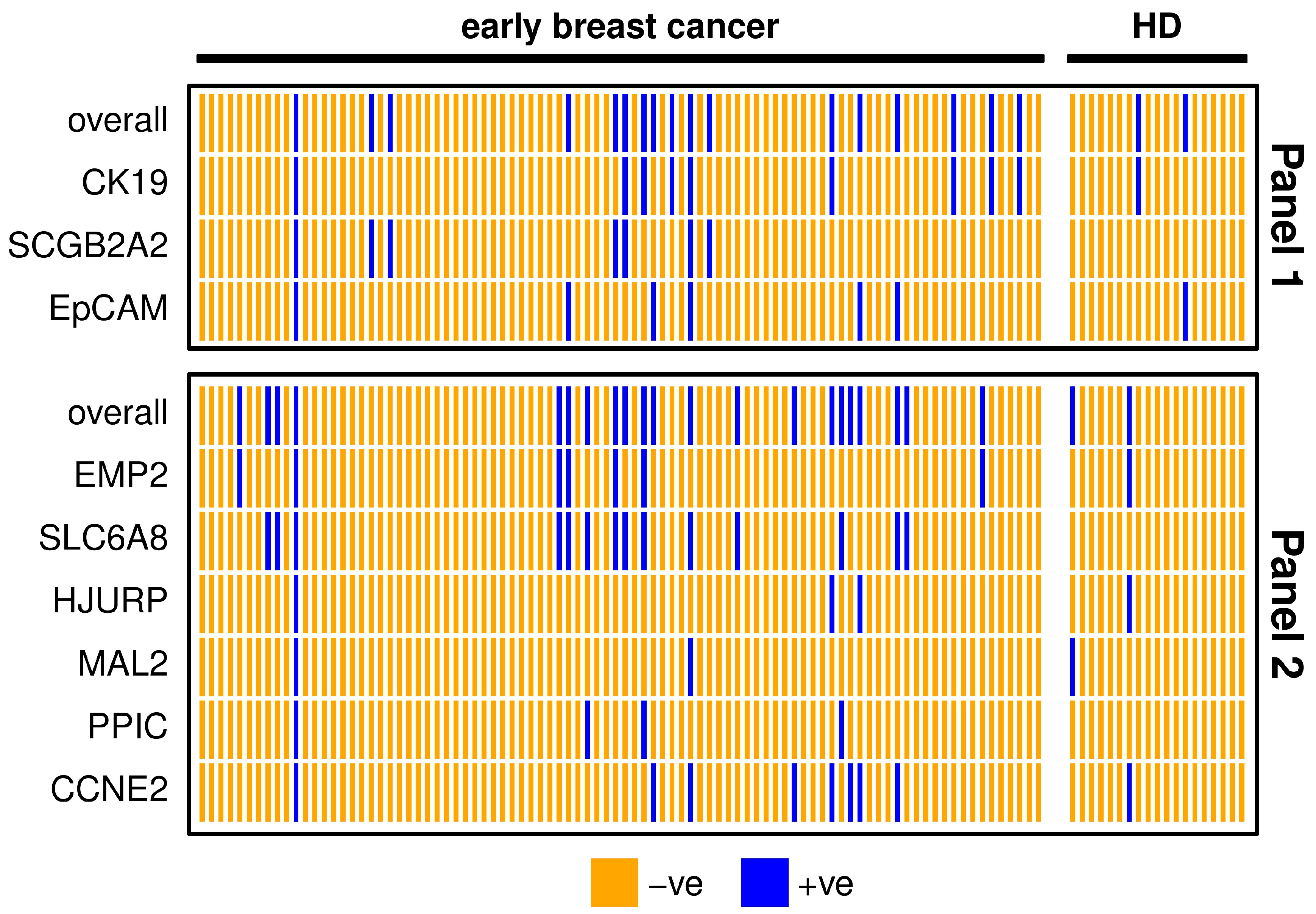
3.3. Evaluation of Gene Panels in Early Breast Cancer Patients
3.4. Association of CTC-Related Markers with Clinical Characteristics of the Patients
3.5. Marker Expression and Overall Survival of Metastatic Breast Cancer Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer Statistics for the Year 2020: An Overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Harbeck, N.; Gnant, M. Breast Cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, R.N.; Esen, B.Ö.; Mellemkjær, L.; Christiansen, P.; Ejlertsen, B.; Lash, T.L.; Nørgaard, M.; Cronin-Fenton, D. The Incidence of Breast Cancer Recurrence 10-32 Years After Primary Diagnosis. JNCI J. Natl. Cancer Inst. 2022, 114, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Ring, A.; Spataro, M.; Wicki, A.; Aceto, N. Clinical and Biological Aspects of Disseminated Tumor Cells and Dormancy in Breast Cancer. Front. Cell Dev. Biol. 2022, 10, 929893. [Google Scholar] [CrossRef] [PubMed]
- Matikas, A.; Kotsakis, A.; Apostolaki, S.; Politaki, H.; Perraki, M.; Kalbakis, K.; Nikolaou, M.; Economopoulou, P.; Hatzidaki, D.; Georgoulias, V. Detection of Circulating Tumour Cells before and Following Adjuvant Chemotherapy and Long-Term Prognosis of Early Breast Cancer. Br. J. Cancer 2022, 126, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Rack, B.; Schindlbeck, C.; Jückstock, J.; Andergassen, U.; Hepp, P.; Zwingers, T.; Friedl, T.W.P.; Lorenz, R.; Tesch, H.; Fasching, P.A.; et al. Circulating Tumor Cells Predict Survival in Early Average-to-High Risk Breast Cancer Patients. J. Natl. Cancer Inst. 2014, 106, dju066. [Google Scholar] [CrossRef]
- Peeters, D.J.E.; van Dam, P.-J.; Van den Eynden, G.G.M.; Rutten, A.; Wuyts, H.; Pouillon, L.; Peeters, M.; Pauwels, P.; Van Laere, S.J.; van Dam, P.A.; et al. Detection and Prognostic Significance of Circulating Tumour Cells in Patients with Metastatic Breast Cancer According to Immunohistochemical Subtypes. Br. J. Cancer 2014, 110, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Bidard, F.-C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-Analysis. J. Natl. Cancer Inst. 2018, 110, 560–567. [Google Scholar] [CrossRef]
- Janni, W.J.; Rack, B.; Terstappen, L.W.M.M.; Pierga, J.-Y.; Taran, F.-A.; Fehm, T.; Hall, C.; de Groot, M.R.; Bidard, F.-C.; Friedl, T.W.P.; et al. Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin. Cancer Res. 2016, 22, 2583–2593. [Google Scholar] [CrossRef] [Green Version]
- Sparano, J.; O’Neill, A.; Alpaugh, K.; Wolff, A.C.; Northfelt, D.W.; Dang, C.T.; Sledge, G.W.; Miller, K.D. Association of Circulating Tumor Cells With Late Recurrence of Estrogen Receptor–Positive Breast Cancer. JAMA Oncol. 2018, 4, 1700–1706. [Google Scholar] [CrossRef]
- Riethdorf, S.; Fritsche, H.; Müller, V.; Rau, T.; Schindlbeck, C.; Rack, B.; Janni, W.; Coith, C.; Beck, K.; Jänicke, F.; et al. Detection of Circulating Tumor Cells in Peripheral Blood of Patients with Metastatic Breast Cancer: A Validation Study of the CellSearch System. Clin. Cancer Res. 2007, 13, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.C.; Robinson, P.S.; Wagner, C.; O’Shannessy, D.J. The ParsortixTM Cell Separation System—A Versatile Liquid Biopsy Platform. Cytometry 2018, 93, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Ju, S.; Chen, C.; Zhang, J.; Xu, L.; Zhang, X.; Li, Z.; Chen, Y.; Zhou, J.; Ji, F.; Wang, L. Detection of Circulating Tumor Cells: Opportunities and Challenges. Biomark. Res. 2022, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Königsberg, R.; Obermayr, E.; Bises, G.; Pfeiler, G.; Gneist, M.; Wrba, F.; de Santis, M.; Zeillinger, R.; Hudec, M.; Dittrich, C. Detection of EpCAM Positive and Negative Circulating Tumor Cells in Metastatic Breast Cancer Patients. Acta Oncol. 2011, 50, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Obermayr, E.; Sanchez-Cabo, F.; Tea, M.-K.M.; Singer, C.F.; Krainer, M.; Fischer, M.B.; Sehouli, J.; Reinthaller, A.; Horvat, R.; Heinze, G.; et al. Assessment of a Six Gene Panel for the Molecular Detection of Circulating Tumor Cells in the Blood of Female Cancer Patients. BMC Cancer 2010, 10, 666. [Google Scholar] [CrossRef] [Green Version]
- Stathopoulou, A.; Ntoulia, M.; Perraki, M.; Apostolaki, S.; Mavroudis, D.; Malamos, N.; Georgoulias, V.; Lianidou, E.S. A Highly Specific Real-Time RT-PCR Method for the Quantitative Determination of CK-19 MRNA Positive Cells in Peripheral Blood of Patients with Operable Breast Cancer. Int. J. Cancer 2006, 119, 1654–1659. [Google Scholar] [CrossRef]
- Sajdik, C.; Schuster, E.; Holzer, B.; Krainer, M.; Deutschmann, C.; Peter, S.; Marhold, M.; Zeillinger, R.; Obermayr, E. Comparison of Microfluidic Platforms for the Enrichment of Circulating Tumor Cells in Breast Cancer Patients. Breast Cancer Res. Treat. 2022, 196, 75–85. [Google Scholar] [CrossRef]
- Müller, V.; Riethdorf, S.; Rack, B.; Janni, W.; Fasching, P.A.; Solomayer, E.; Aktas, B.; Kasimir-Bauer, S.; Pantel, K.; Fehm, T. Prognostic Impact of Circulating Tumor Cells Assessed with the CellSearch SystemTM and AdnaTest BreastTM in Metastatic Breast Cancer Patients: The DETECT Study. Breast Cancer Res. 2012, 14, R118. [Google Scholar] [CrossRef]
- Cohen, E.N.; Jayachandran, G.; Moore, R.G.; Cristofanilli, M.; Lang, J.E.; Khoury, J.D.; Press, M.F.; Kim, K.K.; Khazan, N.; Zhang, Q.; et al. A Multi-Center Clinical Study to Harvest and Characterize Circulating Tumor Cells from Patients with Metastatic Breast Cancer Using the Parsortix® PC1 System. Cancers 2022, 14, 5238. [Google Scholar] [CrossRef]
- Hartkopf, A.D.; Banys, M.; Krawczyk, N.; Wallwiener, M.; Schneck, H.; Neubauer, H.; Fehm, T. Circulating Tumor Cells in Early-Stage Breast Cancer. Geburtshilfe Frauenheilkd. 2011, 71, 1067–1072. [Google Scholar] [CrossRef] [Green Version]
- Obermayr, E.; Castillo-Tong, D.C.; Pils, D.; Speiser, P.; Braicu, I.; Van Gorp, T.; Mahner, S.; Sehouli, J.; Vergote, I.; Zeillinger, R. Molecular Characterization of Circulating Tumor Cells in Patients with Ovarian Cancer Improves Their Prognostic Significance—A Study of the OVCAD Consortium. Gynecol. Oncol. 2013, 128, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Xenidis, N.; Perraki, M.; Kafousi, M.; Apostolaki, S.; Bolonaki, I.; Stathopoulou, A.; Kalbakis, K.; Androulakis, N.; Kouroussis, C.; Pallis, T.; et al. Predictive and Prognostic Value of Peripheral Blood Cytokeratin-19 MRNA-Positive Cells Detected by Real-Time Polymerase Chain Reaction in Node-Negative Breast Cancer Patients. J. Clin. Oncol. 2006, 24, 3756–3762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidard, F.-C.; Mathiot, C.; Delaloge, S.; Brain, E.; Giachetti, S.; de Cremoux, P.; Marty, M.; Pierga, J.-Y. Single Circulating Tumor Cell Detection and Overall Survival in Nonmetastatic Breast Cancer. Ann. Oncol. 2010, 21, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Daskalaki, A.; Agelaki, S.; Perraki, M.; Apostolaki, S.; Xenidis, N.; Stathopoulos, E.; Kontopodis, E.; Hatzidaki, D.; Mavroudis, D.; Georgoulias, V. Detection of Cytokeratin-19 MRNA-Positive Cells in the Peripheral Blood and Bone Marrow of Patients with Operable Breast Cancer. Br. J. Cancer 2009, 101, 589–597. [Google Scholar] [CrossRef]
- Pierga, J.-Y.; Bidard, F.-C.; Mathiot, C.; Brain, E.; Delaloge, S.; Giachetti, S.; de Cremoux, P.; Salmon, R.; Vincent-Salomon, A.; Marty, M. Circulating Tumor Cell Detection Predicts Early Metastatic Relapse After Neoadjuvant Chemotherapy in Large Operable and Locally Advanced Breast Cancer in a Phase II Randomized Trial. Clin. Cancer Res. 2008, 14, 7004–7010. [Google Scholar] [CrossRef] [Green Version]
- Nieto, Y.; Franklin, W.A.; Jones, R.B.; Berman, S.I.; Pellom, J.; Barón, A.E.; Shpall, E.J. Prognostic Significance of Occult Tumor Cells in the Apheresis Products of Patients with Advanced Breast Cancer Receiving High-Dose Chemotherapy and Autologous Hematopoietic Progenitor Cell Support. Biol. Blood Marrow Transplant. 2004, 10, 415–425. [Google Scholar] [CrossRef]
- Stathopoulou, A.; Vlachonikolis, I.; Mavroudis, D.; Perraki, M.; Kouroussis, C.; Apostolaki, S.; Malamos, N.; Kakolyris, S.; Kotsakis, A.; Xenidis, N.; et al. Molecular Detection of Cytokeratin-19-Positive Cells in the Peripheral Blood of Patients with Operable Breast Cancer: Evaluation of Their Prognostic Significance. J. Clin. Oncol. 2002, 20, 3404–3412. [Google Scholar] [CrossRef]
- Colleoni, M.; Sun, Z.; Price, K.N.; Karlsson, P.; Forbes, J.F.; Thürlimann, B.; Gianni, L.; Castiglione, M.; Gelber, R.D.; Coates, A.S.; et al. Annual Hazard Rates of Recurrence for Breast Cancer During 24 Years of Follow-Up: Results From the International Breast Cancer Study Group Trials I to V. J. Clin. Oncol. 2016, 34, 927–935. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Panel 1 | Metastatic Breast Cancer | HD | Panel 2 | Metastatic Breast Cancer | HD |
|---|---|---|---|---|---|
| overall | 25 (69.4%) | 0 (0.0%) | overall | 27 (75.0%) | 0 (0.0%) |
| CK19 | 6 (16.7%) | 0 (0.0%) | EMP2 | 5 (13.9%) | 0 (0.0%) |
| SCGB2A2 | 20 (55.6%) | 0 (0.0%) | SLC6A8 | 19 (52.8%) | 0 (0.0%) |
| EPCAM | 16 (44.4%) | 0 (0.0%) | HJURP | 3 (8.3%) | 0 (0.0%) |
| MAL2 | 6 (16.7%) | 0 (0.0%) | |||
| PPIC | 22 (61.1%) | 0 (0.0%) | |||
| CCNE2 | 5 (13.9%) | 0 (0.0%) |
| Panel 1 | Early Breast Cancer | HD | Panel 2 | Early Breast Cancer | HD |
|---|---|---|---|---|---|
| overall | 17 (18.9%) | 2 (10.5%) | overall | 21 (23.3%) | 2 (10.5%) |
| CK19 | 9 (10.0%) | 1 (5.3%) | EMP2 | 7 (7.8%) | 1 (5.3%) |
| SCGB2A2 | 7 (7.8%) | 0 (0.0%) | SLC6A8 | 14 (15.6%) | 0 (0.0%) |
| EPCAM | 6 (6.7%) | 1 (5.3%) | HJURP | 3 (3.3%) | 1 (5.3%) |
| MAL2 | 2 (2.2%) | 1 (5.3%) | |||
| PPIC | 4 (4.4%) | 0 (0.0%) | |||
| CCNE2 | 8 (8.9%) | 1 (5.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Welsch, E.; Schuster, E.; Krainer, M.; Marhold, M.; Bartsch, R.; Fischer, M.B.; Hermann, M.; Hastermann, G.; Uher, H.; Sliutz, G.; et al. Comparison of RNA Marker Panels for Circulating Tumor Cells and Evaluation of Their Prognostic Relevance in Breast Cancer. Cancers 2023, 15, 1271. https://doi.org/10.3390/cancers15041271
Welsch E, Schuster E, Krainer M, Marhold M, Bartsch R, Fischer MB, Hermann M, Hastermann G, Uher H, Sliutz G, et al. Comparison of RNA Marker Panels for Circulating Tumor Cells and Evaluation of Their Prognostic Relevance in Breast Cancer. Cancers. 2023; 15(4):1271. https://doi.org/10.3390/cancers15041271
Chicago/Turabian StyleWelsch, Eva, Eva Schuster, Michael Krainer, Maximilian Marhold, Rupert Bartsch, Michael B. Fischer, Michael Hermann, Gabriele Hastermann, Heidemarie Uher, Gerhard Sliutz, and et al. 2023. "Comparison of RNA Marker Panels for Circulating Tumor Cells and Evaluation of Their Prognostic Relevance in Breast Cancer" Cancers 15, no. 4: 1271. https://doi.org/10.3390/cancers15041271