Neuroendocrine and Inflammatory Effects of Childhood Trauma Following Psychosocial and Inflammatory Stress in Women with Remitted Major Depressive Disorder


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
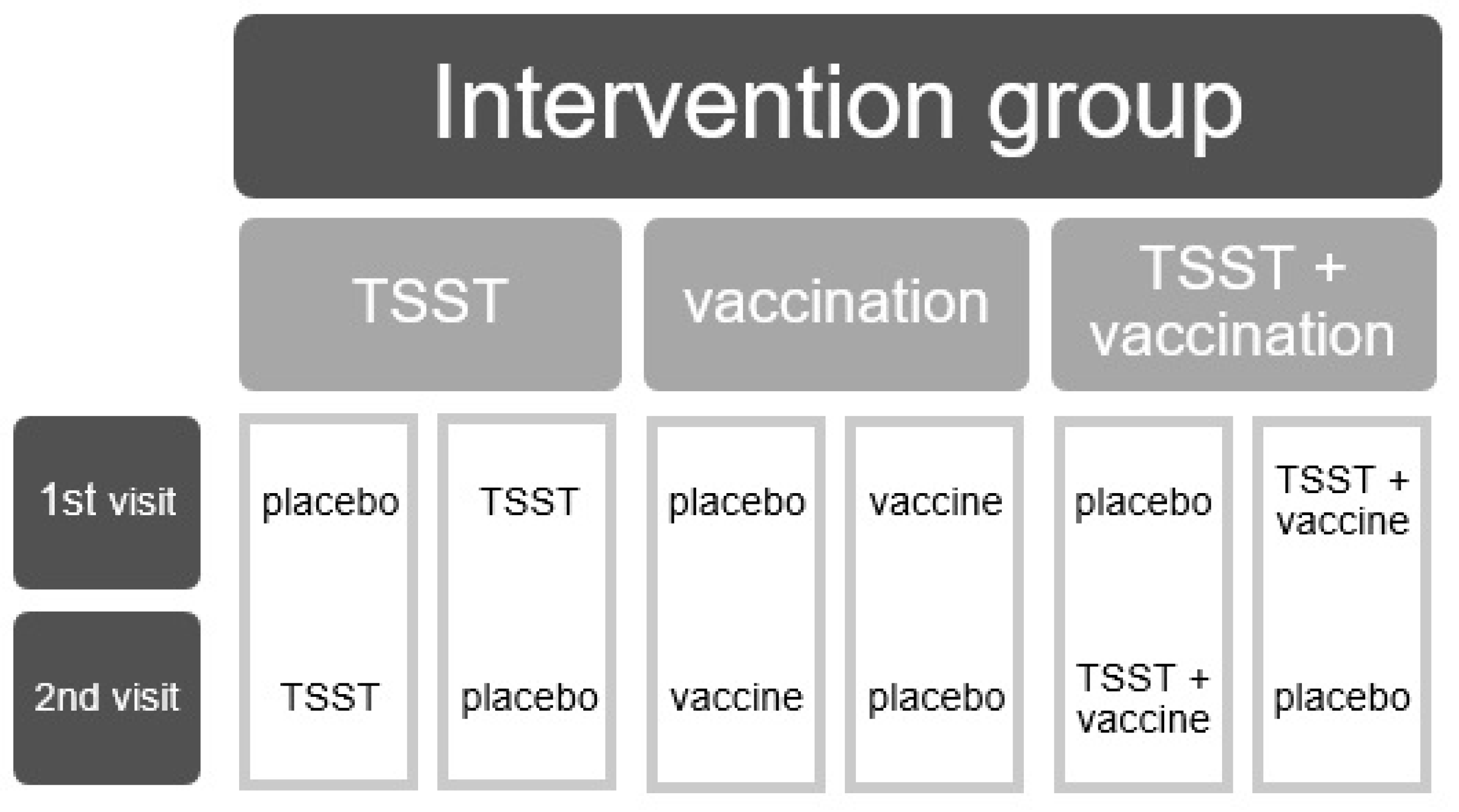
2.2. Study Design
2.3. Assessments
2.3.1. Baseline Mood
2.3.2. Childhood Trauma
2.3.3. Biological Measures
2.3.4. Statistical Analyses
3. Results
3.1. Demographics
3.2. Biological Outcomes
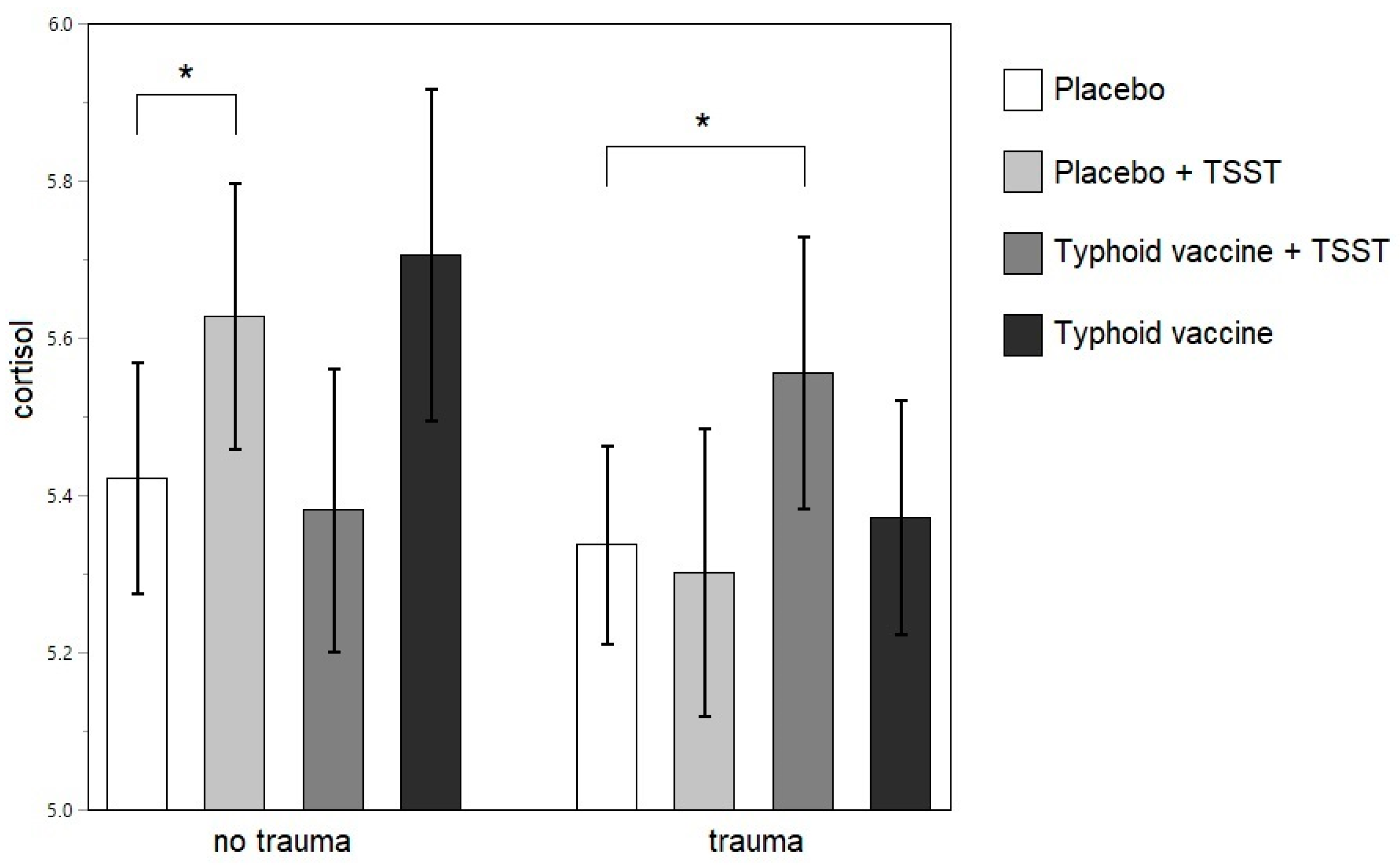
3.2.1. Neuroendocrine Outcomes
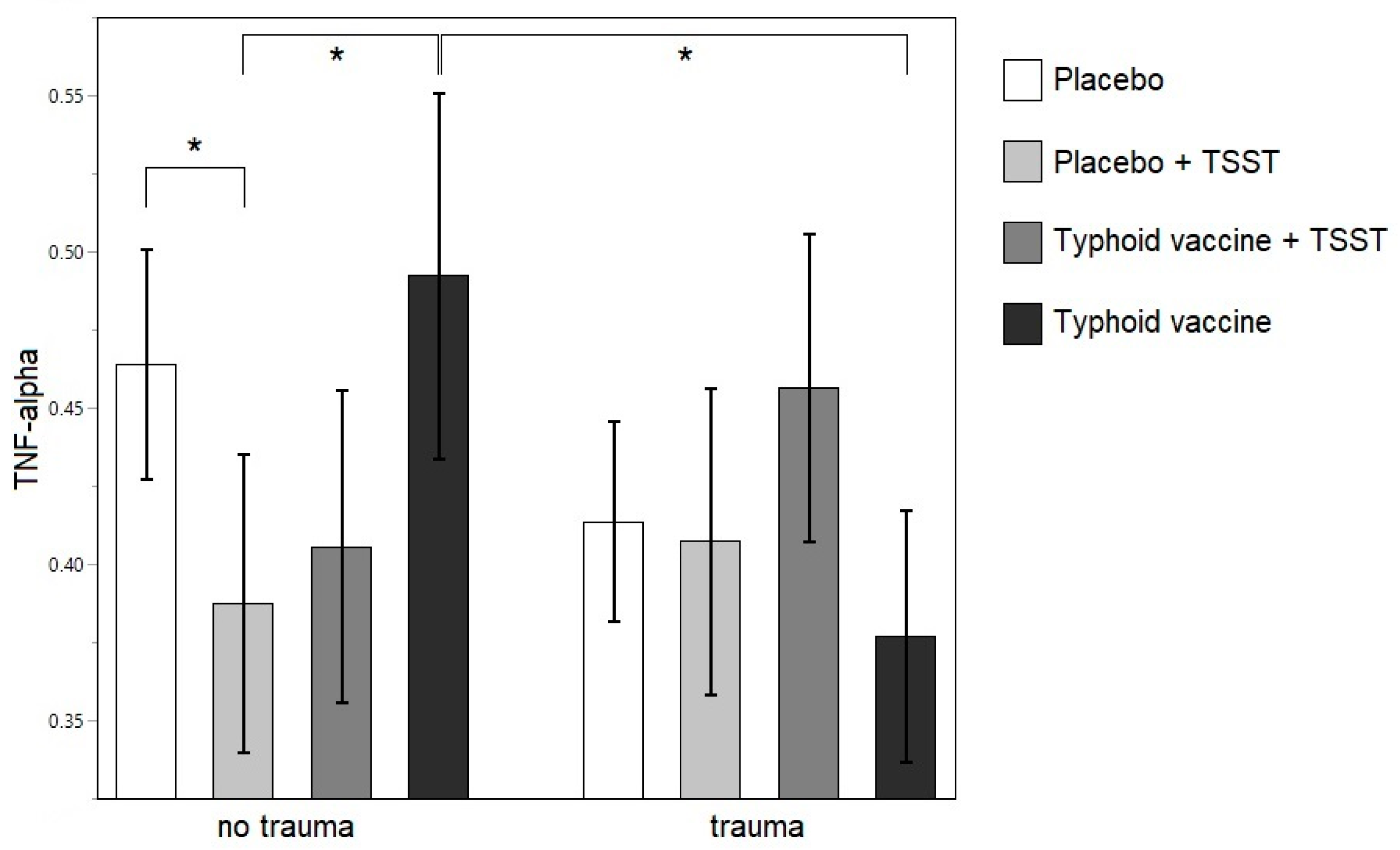
3.2.2. Inflammatory Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.L.L.; Vos, T.; Whiteford, H.A. Burden of Depressive Disorders by Country, Sex, Age, and Year: Findings from the Global Burden of Disease Study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duman, R.S. Molecular and Cellular Pathogenesis of Depression and Mechanisms for Treatments Response. In Neurobiology of Mental Illness; Charney, D.S., Buxbaum, J.D., Sklar, P., Nestler, E.J., Eds.; Oxford University Press: New York, NY, USA, 2013; pp. 425–437. [Google Scholar]
- Slavich, G.M.; Irwin, M.R. From stress to inflammation and major depressive disorder: A social signal transduction theory of depression. Psychol. Bull. 2014, 140, 774–815. [Google Scholar] [CrossRef] [PubMed]
- Plotsky, P.M.; Owens, M.J.; Nemeroff, C.B. Psychoneuroendocrinology of depression. Hypothalamic-pituitary-adrenal axis. Psychiatr. Clin. North Am. 1998, 21, 293–307. [Google Scholar] [CrossRef]
- Claes, S.J. CRH, stress, and major depression: A psychobiological interplay. Vitam. Horm. 2004, 69, 117–150. [Google Scholar] [PubMed]
- Holsboer, F. The Corticosteroid Receptor Hypothesis of Depression. Neuropsychopharmacology 2000, 23, 477–501. [Google Scholar] [CrossRef] [Green Version]
- Heuser, I.; Yassouridis, A.; Holsboer, F. The combined dexamethasone/CRH test: A refined laboratory test for psychiatric disorders. J. Psychiatr. Res. 1994, 28, 341–356. [Google Scholar] [CrossRef]
- Sher, L. Combined Dexamethasone Suppression-Corticotropin-Releasing Hormone Stimulation Test in Studies of Depression, Alcoholism, and Suicidal Behavior. Sci. World J. 2006, 6, 1398–1404. [Google Scholar] [CrossRef]
- Burke, H.M.; Davis, M.C.; Otte, C.; Mohr, D.C. Depression and cortisol responses to psychological stress: A meta-analysis. Psychoneuroendocrinology 2005, 30, 846–856. [Google Scholar] [CrossRef]
- Lok, A.; Mocking, R.J.T.; Ruhé, H.G.; Visser, I.; Koeter, M.W.J.; Assies, J.; Bockting, C.L.H.; Olff, M.; Schene, A.H. Longitudinal hypothalamic–pituitary–adrenal axis trait and state effects in recurrent depression. Psychoneuroendocrinology 2012, 37, 892–902. [Google Scholar] [CrossRef]
- Holsen, L.M.; Lancaster, K.; Klibanski, A.; Whitfield-Gabrieli, S.; Cherkerzian, S.; Buka, S.; Goldstein, J.M. HPA-axis hormone modulation of stress response circuitry activity in women with remitted major depression. Neuroscience 2013, 250, 733–742. [Google Scholar] [CrossRef] [Green Version]
- Höhne, N.; Poidinger, M.; Merz, F.; Pfister, H.; Brückl, T.; Zimmermann, P.; Uhr, M.; Holsboer, F.; Ising, M. Increased HPA axis response to psychosocial stress in remitted depression: The influence of coping style. Biol. Psychol. 2014, 103, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Behnken, A.; Bellingrath, S.; Symanczik, J.-P.; Rieck, M.J.; Zavorotnyy, M.; Domschke, K.; Arolt, V.; Zwanzger, P. Associations between cognitive performance and cortisol reaction to the DEX/CRH test in patients recovered from depression. Psychoneuroendocrinology 2013, 38, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Lange, C.; Zschucke, E.; Ising, M.; Uhr, M.; Bermpohl, F.; Adli, M. Evidence for a normal HPA axis response to psychosocial stress in patients remitted from depression. Psychoneuroendocrinology 2013, 38, 2729–2736. [Google Scholar] [CrossRef] [PubMed]
- Salvat-Pujol, N.; Labad, J.; Urretavizcaya, M.; de Arriba-Arnau, A.; Segalàs, C.; Real, E.; Ferrer, A.; Crespo, J.M.; Jiménez-Murcia, S.; Soriano-Mas, C.; et al. Hypothalamic-pituitary-adrenal axis activity and cognition in major depression: The role of remission status. Psychoneuroendocrinology 2017, 76, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Trestman, R.L.; Coccaro, E.F.; Mitropoulou, V.; Gabriel, S.M.; Horvath, T.; Siever, L.J. The cortisol response to clonidine in acute and remitted depressed men. Biol. Psychiatry 1993, 34, 373–379. [Google Scholar] [CrossRef]
- Zorn, J.V.; Schür, R.R.; Boks, M.P.; Kahn, R.S.; Joëls, M.; Vinkers, C.H. Cortisol stress reactivity across psychiatric disorders: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 77, 25–36. [Google Scholar] [CrossRef]
- Gold, P.W.; Pavlatou, M.G.; Carlson, P.J.; Luckenbaugh, D.A.; Costello, R.; Bonne, O.; Csako, G.; Drevets, W.C.; Remaley, A.T.; Charney, D.S.; et al. Unmedicated, remitted patients with major depression have decreased serum immunoglobulin A. Neurosci. Lett. 2012, 520, 1–5. [Google Scholar] [CrossRef]
- Vogelzangs, N.; de Jonge, P.; Smit, J.H.; Bahn, S.; Penninx, B.W. Cytokine production capacity in depression and anxiety. Transl. Psychiatry 2016, 6, e825. [Google Scholar] [CrossRef]
- Van Den Eede, F.; Van den Bossche, B.; Hulstijn, W.; Sabbe, B.G.C.; Cosyns, P.; Claes, S.J. Combined dexamethasone/CRF test in remitted outpatients with recurrent major depressive disorder. J. Affect. Disord. 2006, 93, 259–263. [Google Scholar] [CrossRef]
- Hardeveld, F.; Spijker, J.; Vreeburg, S.A.; De Graaf, R.; Hendriks, S.M.; Licht, C.M.M.; Nolen, W.A.; Penninx, B.W.J.H.; Beekman, A.T.F. Increased cortisol awakening response was associated with time to recurrence of major depressive disorder. Psychoneuroendocrinology 2014, 50, 62–71. [Google Scholar] [CrossRef]
- Bockting, C.L.H.; Lok, A.; Visser, I.; Assies, J.; Koeter, M.W.; Schene, A.H. DELTA study group Lower cortisol levels predict recurrence in remitted patients with recurrent depression: A 5.5 year prospective study. Psychiatry Res. 2012, 200, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Appelhof, B.C.; Huyser, J.; Verweij, M.; Brouwer, J.P.; van Dyck, R.; Fliers, E.; Hoogendijk, W.J.G.; Tijssen, J.G.P.; Wiersinga, W.M.; Schene, A.H. Glucocorticoids and Relapse of Major Depression (Dexamethasone/Corticotropin-Releasing Hormone Test in Relation to Relapse of Major Depression). Biol. Psychiatry 2006, 59, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Zobel, A.W.; Nickel, T.; Sonntag, A.; Uhr, M.; Holsboer, F.; Ising, M. Cortisol response in the combined dexamethasone/CRH test as predictor of relapse in patients with remitted depression. A prospective study. J. Psychiatr. Res. 2001, 35, 83–94. [Google Scholar] [CrossRef]
- Brietzke, E.; Sant’anna, M.K.; Jackowski, A.; Grassi-Oliveira, R.; Bucker, J.; Zugman, A.; Mansur, R.B.; Bressan, R.A. Impact of Childhood Stress on Psychopathology. Rev. Bras. Psiquiatr. 2012, 34, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Heim, C.; Shugart, M.; Craighead, W.E.; Nemeroff, C.B. Neurobiological and psychiatric consequences of child abuse and neglect. Dev. Psychobiol. 2010, 52, 671–690. [Google Scholar] [CrossRef]
- De Bellis, M.D.; Zisk, A. The biological effects of childhood trauma. Child Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 185–222. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.E.; Chen, E.; Zhou, E.S. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychol. Bull. 2007, 133, 25–45. [Google Scholar] [CrossRef] [Green Version]
- Kumsta, R.; Schlotz, W.; Golm, D.; Moser, D.; Kennedy, M.; Knights, N.; Kreppner, J.; Maughan, B.; Rutter, M.; Sonuga-Barke, E. HPA axis dysregulation in adult adoptees twenty years after severe institutional deprivation in childhood. Psychoneuroendocrinology 2017, 86, 196–202. [Google Scholar] [CrossRef]
- Schalinski, I.; Elbert, T.; Steudte-Schmiedgen, S.; Kirschbaum, C. The Cortisol Paradox of Trauma-Related Disorders: Lower Phasic Responses but Higher Tonic Levels of Cortisol Are Associated with Sexual Abuse in Childhood. PLoS ONE 2015, 10, e0136921. [Google Scholar] [CrossRef] [Green Version]
- Heim, C.; Mletzko, T.; Purselle, D.; Musselman, D.L.; Nemeroff, C.B. The Dexamethasone/Corticotropin-Releasing Factor Test in Men with Major Depression: Role of Childhood Trauma. Biol. Psychiatry 2008, 63, 398–405. [Google Scholar] [CrossRef]
- Danese, A.; Moffitt, T.E.; Pariante, C.M.; Ambler, A.; Poulton, R.; Caspi, A. Elevated Inflammation Levels in Depressed Adults With a History of Childhood Maltreatment. Arch. Gen. Psychiatry 2008, 65, 409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlman, K.R.; Chiang, J.J.; Horn, S.; Bower, J.E. Developmental psychoneuroendocrine and psychoneuroimmune pathways from childhood adversity to disease. Neurosci. Biobehav. Rev. 2017, 80, 166–184. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Slavich, G.M. Psychoneuroimmunology. In Handbook of Psychophysiology; Cacioppo, J.T., Tassinary, L.G., Berntson, G.G., Eds.; Cambridge University Press: Cambridge, UK, 2017; pp. 377–397. [Google Scholar]
- Bertone-Johnson, E.R.; Whitcomb, B.W.; Missmer, S.A.; Karlson, E.W.; Rich-Edwards, J.W. Inflammation and Early-Life Abuse in Women. Am. J. Prev. Med. 2012, 43, 611–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiecolt-Glaser, J.K.; Gouin, J.-P.; Weng, N.; Malarkey, W.B.; Beversdorf, D.Q.; Glaser, R. Childhood Adversity Heightens the Impact of Later-Life Caregiving Stress on Telomere Length and Inflammation. Psychosom. Med. 2011, 73, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemegeers, P.; De Boer, P.; Dumont, G.J.H.; Van Den Eede, F.; Fransen, E.; Claes, S.J.; Morrens, M.; Sabbe, B.G.C. Differential Effects of Inflammatory and Psychosocial Stress on Mood, Hypothalamic-Pituitary-Adrenal Axis, and Inflammation in Remitted Depression. Neuropsychobiology 2016, 74, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Rohleder, N.; Schommer, N.C.; Hellhammer, D.H.; Engel, R.; Kirschbaum, C. Sex differences in glucocorticoid sensitivity of proinflammatory cytokine production after psychosocial stress. Psychosom. Med. 2001, 63, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Paris, J.J.; Franco, C.; Sodano, R.; Freidenberg, B.; Gordis, E.; Anderson, D.A.; Forsyth, J.P.; Wulfert, E.; Frye, C.A. Sex differences in salivary cortisol in response to acute stressors among healthy participants, in recreational or pathological gamblers, and in those with posttraumatic stress disorder. Horm. Behav. 2010, 57, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Veldhuis, J.D.; Sharma, A.; Roelfsema, F. Age-Dependent and Gender-Dependent Regulation of Hypothalamic-Adrenocorticotropic-Adrenal Axis. Endocrinol. Metab. Clin. North Am. 2013, 42, 201–225. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV; Revised 4t; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The ’Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Walker, E.A.; Gelfand, A.; Katon, W.J.; Koss, M.P.; Von Korff, M.; Bernstein, D.; Russo, J. Adult health status of women with histories of childhood abuse and neglect. Am. J. Med. 1999, 107, 332–339. [Google Scholar] [CrossRef]
- Heim, C.; Newport, D.J.; Heit, S.; Graham, Y.P.; Wilcox, M.; Bonsall, R.; Miller, A.H.; Nemeroff, C.B. Pituitary-Adrenal and Autonomic Responses to Stress in Women After Sexual. J Am Med Assoc 2000, 284, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, L.L.; Shattuck, T.T.; Tyrka, A.R.; Geracioti, T.D.; Price, L.H. Effect of childhood physical abuse on cortisol stress response. Psychopharmacology (Berl). 2011, 214, 367–375. [Google Scholar] [CrossRef] [Green Version]
- Ouellet-Morin, I.; Odgers, C.L.; Danese, A.; Bowes, L.; Shakoor, S.; Papadopoulos, A.S.; Caspi, A.; Moffitt, T.E.; Arseneault, L. Blunted Cortisol Responses to Stress Signal Social and Behavioral Problems Among Maltreated/Bullied 12-Year-Old Children. Biol. Psychiatry 2011, 70, 1016–1023. [Google Scholar] [CrossRef] [Green Version]
- Booij, S.H.; Bouma, E.M.C.; de Jonge, P.; Ormel, J.; Oldehinkel, A.J. Chronicity of depressive problems and the cortisol response to psychosocial stress in adolescents: The TRAILS study. Psychoneuroendocrinology 2013, 38, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Silverman, M.N.; Pearce, B.D.; Biron, C.A.; Miller, A.H. Immune modulation of the hypothalamic-pituitary-adrenal (HPA) axis during viral infection. Viral. Immunol. 2005, 18, 41–78. [Google Scholar] [CrossRef]
- Morris, M.C.; Rao, U.; Wang, L.; Garber, J. Cortisol reactivity to experimentally manipulated psychosocial stress in young adults at varied risk for depression. Depress. Anxiety 2014, 31, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Bagley, S.L.; Weaver, T.L.; Buchanan, T.W. Sex differences in physiological and affective responses to stress in remitted depression. Physiol. Behav. 2011, 104, 180–186. [Google Scholar] [CrossRef]
- Sorrells, S.F.; Caso, J.R.; Munhoz, C.D.; Sapolsky, R.M. The Stressed CNS: When Glucocorticoids Aggravate Inflammation. Neuron 2009, 64, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.; Salamonsen, L.A. Inflammation, leukocytes and menstruation. Rev. Endocr. Metab. Disord. 2012, 13, 277–288. [Google Scholar] [CrossRef]
- Salamonsen, L.A.; Lathbury, L.J. Endometrial leukocytes and menstruation. Hum. Reprod. Update 2000, 6, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Maki, P.M.; Mordecai, K.L.; Rubin, L.H.; Sundermann, E.; Savarese, A.; Eatough, E.; Drogos, L. Menstrual cycle effects on cortisol responsivity and emotional retrieval following a psychosocial stressor. Horm. Behav. 2015, 74, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero-López, E.; Santos-Ruiz, A.; García-Ríos, M.C.; Rodríguez-Blázquez, M.; Rogers, H.L.; Peralta-Ramírez, M.I. The relationship between the menstrual cycle and cortisol secretion: Daily and stress-invoked cortisol patterns. Int. J. Psychophysiol. 2018, 131, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovallo, W.R.; Buchanan, T.W. Stress Hormones in Psychophysiological Research: Emotional, Behavioral, and Cognitive Implications. In Handbook of Psychophysiology; Cacioppo, J.T., Tassinary, L.G., Berntson, G.G., Eds.; Cambridge University Press: Cambridge, UK, 2017; pp. 465–494. [Google Scholar]
- Cattaneo, A.; Macchi, F.; Plazzotta, G.; Veronica, B.; Bocchio-Chiavetto, L.; Riva, M.A.; Pariante, C.M. Inflammation and neuronal plasticity: A link between childhood trauma and depression pathogenesis. Front. Cell. Neurosci. 2015, 9, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houtepen, L.C.; Vinkers, C.H.; Carrillo-Roa, T.; Hiemstra, M.; van Lier, P.A.; Meeus, W.; Branje, S.; Heim, C.M.; Nemeroff, C.B.; Mill, J.; et al. Genome-wide DNA methylation levels and altered cortisol stress reactivity following childhood trauma in humans. Nat. Commun. 2016, 7, 10967. [Google Scholar] [CrossRef] [Green Version]
- Ehlert, U. Enduring psychobiological effects of childhood adversity. Psychoneuroendocrinology 2013, 38, 1850–1857. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Remitted MDD Group | Healthy Control Group | |||||
|---|---|---|---|---|---|---|
| No Trauma (n = 9) | Trauma (n = 12) | No Trauma (n = 15) | Trauma (n = 3) | |||
| Median (IQR) | Median (IQR) | p Value | Median (IQR) | Median (IQR) | p Value | |
| Age | 38.0 (11.5) | 29.5 (8.5) | 0.0639 | 30.0 (13.0) | 32.0 (18.0) | 0.9524 |
| MADRS | 3 (12.0) | 5 (9.5) | 0.7207 | 0.0 (1.0) | 0.0 (2.0) | 1.0000 |
| Baseline ACTH | 2.162 (1.995) | 1.953 (1.595) | 0.8940 | 1.847 (1.847) | 2.057 (1.097) | 0.8930 |
| Baseline cortisol | 248.218 (113.717) | 269.462 (254.402) | 0.8590 | 277.923 (333.931) | 135.835 (151.745) | 0.1551 |
| Baseline IL-6 | 0.485 (0.185) | 0.510 (0.465) | 1.0000 | 0.474 (0.157) | 0.647 (1.403) | 0.1116 |
| Baseline IFN-γ | 4.363 (13.665) | 3.780 (4.388) | 0.8036 | 3.590 (4.230) | 4.320 (82.897) | 0.9057 |
| Baseline TNF-α | 1.470 (0.706) | 1.490 (0.707) | 0.6959 | 1.341 (0.453) | 1.780 (1.172) | 0.2863 |
| Mean (SD) | Mean (SD) | p Value | Mean (SD) | Mean (SD) | p Value | |
| BMI | 23.9 (3.0) | 24.1 (2.8) | 0.8694 | 22.0 (2.9) | 24.5 (4.3) | 0.4210 |
| CTQ | 30.6 (3.6) | 51.8 (16.8) | 0.0011 | 29.4 (3.1) | 41.7 (10.7) | 0.1834 |
| Column Percentage | Column Percentage | p Value | Column Percentage | Column Percentage | p Value | |
| Oral contraceptives | 66.67 | 25.00 | 0.0562 | 66.67 | 66.67 | 1.000 |
| Ethnicity | 0.2367 | 0.1797 | ||||
| African | 11.11 | 0.00 | 0.00 | 0.00 | ||
| Maghrebi | 0.00 | 0.00 | 6.67 | 33.33 | ||
| European | 88.89 | 100.00 | 93.33 | 66.67 | ||
| Antidepressants | 55.56 | 75.00 | 0.3496 | 00.00 | 00.00 | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassiers, L.L.M.; Niemegeers, P.; Fransen, E.; Morrens, M.; De Boer, P.; Van Nueten, L.; Claes, S.; Sabbe, B.G.C.; Van Den Eede, F. Neuroendocrine and Inflammatory Effects of Childhood Trauma Following Psychosocial and Inflammatory Stress in Women with Remitted Major Depressive Disorder. Brain Sci. 2019, 9, 375. https://doi.org/10.3390/brainsci9120375
Cassiers LLM, Niemegeers P, Fransen E, Morrens M, De Boer P, Van Nueten L, Claes S, Sabbe BGC, Van Den Eede F. Neuroendocrine and Inflammatory Effects of Childhood Trauma Following Psychosocial and Inflammatory Stress in Women with Remitted Major Depressive Disorder. Brain Sciences. 2019; 9(12):375. https://doi.org/10.3390/brainsci9120375
Chicago/Turabian StyleCassiers, Laura L.M., Peter Niemegeers, Erik Fransen, Manuel Morrens, Peter De Boer, Luc Van Nueten, Stephan Claes, Bernard G.C. Sabbe, and Filip Van Den Eede. 2019. "Neuroendocrine and Inflammatory Effects of Childhood Trauma Following Psychosocial and Inflammatory Stress in Women with Remitted Major Depressive Disorder" Brain Sciences 9, no. 12: 375. https://doi.org/10.3390/brainsci9120375