
Clinical Profile and Aspects of Differential Diagnosis in Patients with ME/CFS from Latvia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Eligibility Criteria
- 18 years or older;
- Patient or legally authorised representative capable to give informed consent;
- Fatigue lasting for at least six consecutive months;
- Subjective symptoms of fatigue for more than six months or previously diagnosed with ME/CFS using the Fukuda et.al diagnostic criteria;
- Meets the neurologic criteria;
- Fatigue includes PEM as a compulsory symptom.
- Younger than 18 years;
- Pregnancy or breast feeding;
- Inability to obtain or declined informed consent;
- Cancer, radiation, chemotherapy at the time of enrolment;
- Acute infectious or inflammatory diseases;
- Previously diagnosed depression and/or any other psychiatric disorder;
- Substance abuse and/or eating disorder within two years of the onset of ME/CFS symptoms;
- Obesity with body mass index greater than 45;
- Primary brain disorder.
2.2. Symptom Registration
2.3. Statystical Analysis
2.4. Ethical Consideration
3. Results
3.1. Subject Characteristics in ME/CFS and Non/ME/CFS Patients
3.2. Characteristic Differences in the Three, Previously Defined Groups
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [Green Version]
- Valdez, A.R.; Hancock, E.E.; Adebayo, S.; Kiernicki, D.J.; Proskauer, D.; Attewell, J.R.; Bateman, L.; DeMaria, A.; Lapp, C.W.; Rowe, P.C.; et al. Estimating Prevalence, Demographics, and Costs of ME/CFS Using Large Scale Medical Claims Data and Machine Learning. Front. Pediatrics 2018, 6, 412. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.A.; Sunnquist, M.; Brown, A.; McManimen, S.; Furst, J. Reflections on the Institute of Medicine’s systemic exertion intolerance disease. Pol. Arch. Med. Wewn. 2015, 125, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Nacul, L.; Authier, F.J.; Scheibenbogen, C.; Lorusso, L.; Helland, I.B.; Martin, J.A.; Sirbu, C.A.; Mengshoel, A.M.; Polo, O.; Behrends, U.; et al. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina 2021, 57, 510. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Kot, B.; Sunnquist, M.; Brown, A.; Evans, M.; Jantke, R.; Williams, Y.; Furst, J.; Vernon, S.D. Chronic fatigue syndrome and myalgic encephalomyelitis: Towards an empirical case definition. Health Psychol. Behav. Med. 2015, 3, 82–93. [Google Scholar] [CrossRef]
- Cortes, R.M.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Comprehensive Review. Diagnostics 2019, 9, 91. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Strand, E.B.; Nacul, L.; Mengshoel, A.M.; Helland, I.B.; Grabowski, P.; Krumina, A.; Alegre-Martin, J.; Efrim-Budisteanu, M.; Sekulic, S.; Pheby, D. Myalgic encephalomyelitis/chronic fatigue Syndrome (ME/CFS): Investigating care practices pointed out to disparities in diagnosis and treatment across European Union. PLoS ONE 2019, 14, e0225995. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, M. A report–chronic fatigue syndrome: Guidelines for research. J. R. Soc. Med. 1991, 84, 118–121. [Google Scholar] [CrossRef] [Green Version]
- Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; National Academies Press (US): Washington, DC, USA, 2015. [Google Scholar]
- Lacerda, E.M.; Bowman, E.W.; Cliff, J.M.; Kingdon, C.C.; King, E.C.; Lee, J.-S.; Clark, T.G.; Dockrell, H.M.; Riley, E.M.; Curran, H. The UK ME/CFS biobank for biomedical research on myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and multiple sclerosis. Open J. Bioresour. 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.A.; McManimen, S.; Sunnquist, M.; Newton, J.L.; Strand, E.B. Clinical criteria versus a possible research case definition in chronic fatigue syndrome/myalgic encephalomyelitis. Fatigue: Biomed. Health Behav. 2017, 5, 89–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hays, R.D.; Sherbourne, C.D.; Mazel, R.M. The rand 36-item health survey 1.0. Health Econ. 1993, 2, 217–227. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL™ 4.0: Reliability and validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Mundt, J.C.; Marks, I.M.; Shear, M.K.; Greist, J.H. The Work and Social Adjustment Scale: A simple measure of impairment in functioning. Br. J. Psychiatry 2002, 180, 461–464. [Google Scholar] [CrossRef]
- Cella, M.; Sharpe, M.; Chalder, T. Measuring disability in patients with chronic fatigue syndrome: Reliability and validity of the Work and Social Adjustment Scale. J. Psychosom. Res. 2011, 71, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.M.; Beqaj, S.H.; Fitzgerald, J.T. Validation of the energy index point score to serially measure the degree of disability in patients with chronic fatigue syndrome. In Vivo 2008, 22, 799–801. [Google Scholar] [PubMed]
- Graf, C. The Lawton instrumental activities of daily living scale. AJN Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Vink, M.; Vink-Niese, A. The draft updated NICE guidance for ME/CFS highlights the unreliability of subjective outcome measures in non-blinded trials. J. Health Psychol. 2021. [Google Scholar] [CrossRef]
- Jason, L.A.; Evans, M.; Brown, M.; Porter, N.; Brown, A.; Hunnell, J.; Anderson, V.; Lerch, A. Fatigue scales and chronic fatigue syndrome: Issues of sensitivity and specificity. Disabil. Stud. Q. DSQ 2011, 31, 9–10. [Google Scholar] [CrossRef]
- Maruish, M. User’s Manual for the SF-12v2 Health Survey, 3rd ed.; QualityMetric Incorporated: Lincoln, RI, USA, 2012. [Google Scholar]
- Ware Jr, J.E.; Scherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar]
- Schrag, A.; Selai, C.; Jahanshahi, M.; Quinn, N.P. The EQ-5D—A generic quality of life measure—Is a useful instrument to measure quality of life in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2000, 69, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devlin, N.J.; Brooks, R. EQ-5D and the EuroQol group: Past, present and future. Appl. Health Econ. Health Policy 2017, 15, 127–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, T.; Zammit, G.; Kushida, C.; Doghramji, K.; Mathias, S.D.; Wong, J.M.; Buysse, D.J. A new questionnaire to detect sleep disorders. Sleep Med. 2002, 3, 99–108. [Google Scholar] [CrossRef]
- Josev, E.K.; Jackson, M.L.; Bei, B.; Trinder, J.; Harvey, A.; Clarke, C.; Snodgrass, K.; Scheinberg, A.; Knight, S.J. Sleep quality in adolescents with chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J. Clin. Sleep Med. 2017, 13, 1057–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Buysse, D.J.; Germain, A.; Moul, D.E.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Pilkonis, P.A. Development of short forms from the PROMIS™ sleep disturbance and sleep-related impairment item banks. Behav. Sleep Med. 2012, 10, 6–24. [Google Scholar] [CrossRef]
- Lapp, C.W. Initiating Care of a Patient With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Front. Pediatrics 2019, 6, 415. [Google Scholar] [CrossRef]
- Minnock, P.; Ringnér, A.; Bresnihan, B.; Veale, D.; FitzGerald, O.; McKee, G. Perceptions of the Cause, Impact and Management of Persistent Fatigue in Patients with Rheumatoid Arthritis Following Tumour Necrosing Factor Inhibition Therapy. Musculoskelet. Care 2017, 15, 23–35. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Reyes, M.; Nisenbaum, R.; Hoaglin, D.C.; Unger, E.R.; Emmons, C.; Randall, B.; Stewart, J.A.; Abbey, S.; Jones, J.F.; Gantz, N. Prevalence and incidence of chronic fatigue syndrome in Wichita, Kansas. Arch. Intern. Med. 2003, 163, 1530–1536. [Google Scholar] [CrossRef]
- Torres-Harding, S.R.; Jason, L.A.; Taylor, R.R. Fatigue severity, attributions, medical utilization, and symptoms in persons with chronic fatigue. J. Behav. Med. 2002, 25, 99–113. [Google Scholar] [CrossRef]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S. Prospective cohort study precipitated by viral and non-viral pathogens: Post-infective and chronic fatigue syndromes. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [Green Version]
- Rasa, S.; Nora-Krukle, Z.; Henning, N.; Eliassen, E.; Shikova, E.; Harrer, T.; Scheibenbogen, C.; Murovska, M.; Prusty, B.K. Chronic viral infections in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2018, 16, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Cameron, B.; Flamand, L.; Juwana, H.; Middeldorp, J.; Naing, Z.; Rawlinson, W.; Ablashi, D.; Lloyd, A. Serological and virological investigation of the role of the herpesviruses EBV, CMV and HHV-6 in post-infective fatigue syndrome. J. Med. Virol. 2010, 82, 1684–1688. [Google Scholar] [CrossRef]
- Bested, A.; Saunders, P.; Logan, A. Chronic fatigue syndrome: Neurological findings may be related to blood–brain barrier permeability. Med. Hypotheses 2001, 57, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Heim, C.; Nater, U.M.; Maloney, E.; Boneva, R.; Jones, J.F.; Reeves, W.C. Childhood trauma and risk for chronic fatigue syndrome: Association with neuroendocrine dysfunction. Arch. Gen. Psychiatry 2009, 66, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Nater, U.M.; Maloney, E.; Heim, C.; Reeves, W.C. Cumulative life stress in chronic fatigue syndrome. Psychiatry Res. 2011, 189, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Onset Patterns and Course of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Pediatrics 2019, 7, 12. [Google Scholar] [CrossRef]
- Nisenbaum, R.; Jones, J.F.; Unger, E.R.; Reyes, M.; Reeves, W.C. A population-based study of the clinical course of chronic fatigue syndrome. Health Qual. Life Outcomes 2003, 1, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milrad, S.F.; Hall, D.L.; Jutagir, D.R.; Lattie, E.G.; Ironson, G.H.; Wohlgemuth, W.; Nunez, M.V.; Garcia, L.; Czaja, S.J.; Perdomo, D.M. Poor sleep quality is associated with greater circulating pro-inflammatory cytokines and severity and frequency of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) symptoms in women. J. Neuroimmunol. 2017, 303, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Comhaire, F.; Deslypere, J.P. News and views in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): The role of co-morbidity and novel treatments. Med. Hypotheses 2020, 134, 109444. [Google Scholar] [CrossRef] [PubMed]
- Burgess, H.J.; Park, M.; Ong, J.C.; Shakoor, N.; Williams, D.A.; Burns, J. Morning versus evening bright light treatment at home to improve function and pain sensitivity for women with fibromyalgia: A pilot study. Pain Med. 2017, 18, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Williams, G.; Waterhouse, J.; Mugarza, J.; Minors, D.; Hayden, K. Therapy of circadian rhythm disorders in chronic fatigue syndrome: No symptomatic improvement with melatonin or phototherapy. Eur. J. Clin. Investig. 2002, 32, 831–837. [Google Scholar] [CrossRef]
- Jones, D.; Gray, J.; Frith, J.; Newton, J. Fatigue severity remains stable over time and independently associated with orthostatic symptoms in chronic fatigue syndrome: A longitudinal study. J. Intern. Med. 2011, 269, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Whistler, T.; Jones, J.F.; Unger, E.R.; Vernon, S.D. Exercise responsive genes measured in peripheral blood of women with chronic fatigue syndrome and matched control subjects. BMC Physiol 2005, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, C.; Zainal, N.; Middleton, S.; Paykel, E. A family history study of chronic fatigue syndrome. Psychiatr. Genet. 2001, 11, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Albright, F.; Light, K.; Light, A.; Bateman, L.; Cannon-Albright, L.A. Evidence for a heritable predisposition to Chronic Fatigue Syndrome. BMC Neurol. 2011, 11, 62. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.; Benton, M.; Torres-Harding, S.; Muldowney, K. The impact of energy modulation on physical functioning and fatigue severity among patients with ME/CFS. Patient Educ. Couns. 2009, 77, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Friedberg, F.; Dechene, L.; McKenzie, M.J., II; Fontanetta, R. Symptom patterns in long-duration chronic fatigue syndrome. J. Psychosom Res. 2000, 48, 59–68. [Google Scholar] [CrossRef]
- Brown, M.M.; Brown, A.A.; Jason, L.A. Illness duration and coping style in chronic fatigue syndrome. Psychol. Rep. 2010, 106, 383–393. [Google Scholar] [CrossRef] [Green Version]
- Twisk, F.N. Accurate diagnosis of myalgic encephalomyelitis and chronic fatigue syndrome based upon objective test methods for characteristic symptoms. World J. Methodol. 2015, 5, 68–87. [Google Scholar] [CrossRef] [Green Version]
- Kidd, E.; Brown, A.; McManimen, S.; Jason, L.A.; Newton, J.L.; Strand, E.B. The Relationship between Age and Illness Duration in Chronic Fatigue Syndrome. Diagnostics 2016, 6, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, S.D.; Levine, C.; Ganz, N.; Frame, D.; Estok, R.; Stone, L.; Ludensky, V. Systematic review of the current literature related to disability and chronic fatigue syndrome. Evid. Rep./Technol. Assess. (Summ.) 2002, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Tiersky, L.; Deluca, J.; Hill, N.; Dhar, S.; Johnson, S.; Lange, G.; Rappolt-Schlichtmann, G.; Natelson, B. Longitudinal Assessment of Neuropsychological Functioning, Psychiatric Status, Functional Disability and Employment Status in Chronic Fatigue Syndrome. Appl. Neuropsychol. 2001, 8, 41–50. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
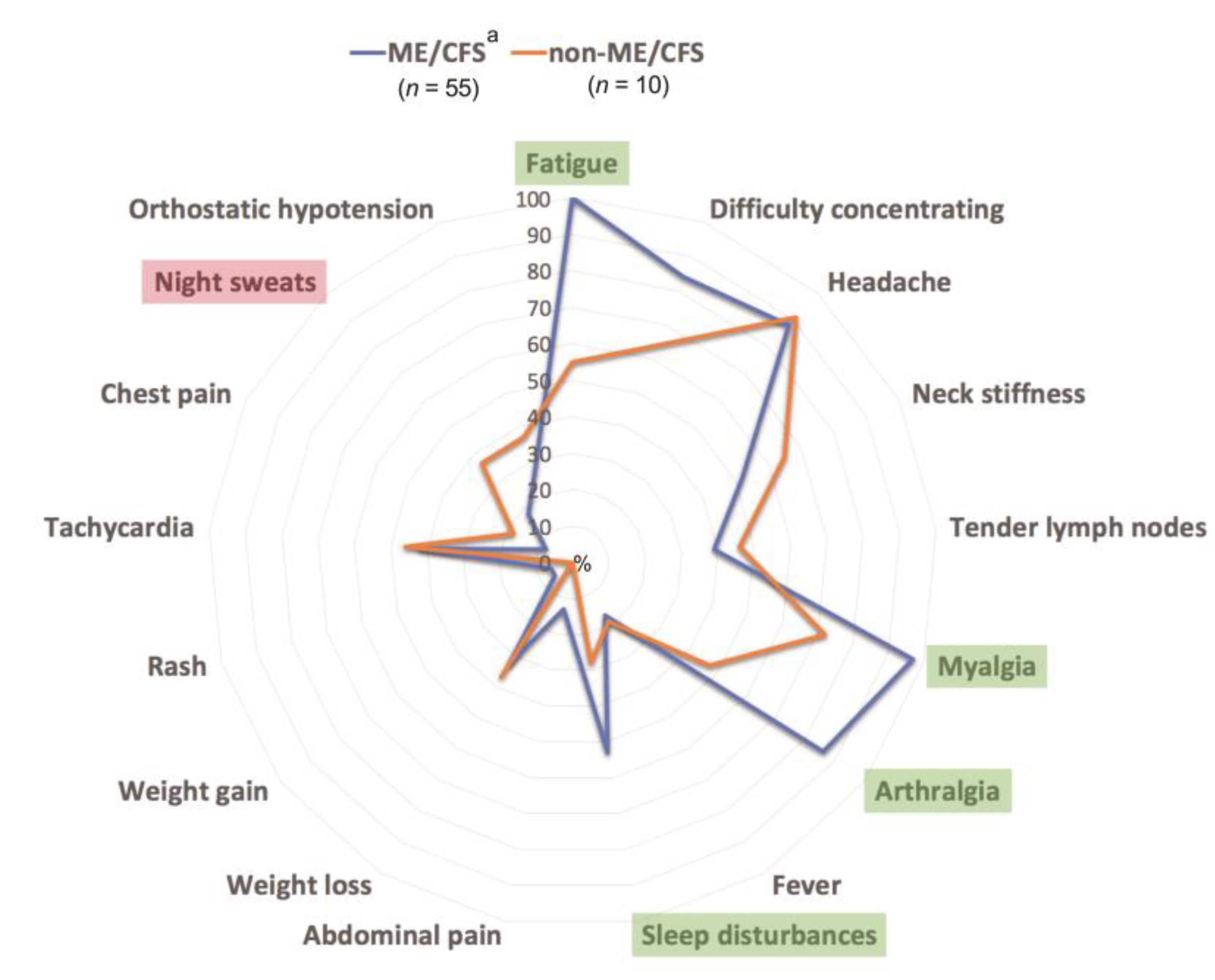
| Clinical Features | ME/CFS, ME/CFS + Comorbidities Patients (n = 55) | 95% CI |
|---|---|---|
| Fatigue | 55 (100.0) | 90.5–100.0 |
| Myalgia | 53 (96.4) | 87.0–100.0 |
| Headache | 48 (87.3) | 78.4–96.1 |
| Arthralgia | 47 (85.5) | 76.7–94.2 |
| Difficulty concentrating | 46 (83.6) | 74.9–92.3 |
| Neck stiffness | 29 (52.7) | 45.8–59.7 |
| Sleep disturbances | 29 (52.7) | 45.8–59.7 |
| Tachycardia | 23 (41.8) | 35.7–48.0 |
| Tender lymph nodes | 21 (38.2) | 32.3–44.1 |
| Night sweats | 19 (32.7) | 27.3–38.2 |
| Weight loss | 18 (27.3) | 22.3–32.2 |
| Orthostatic hypotension | 15 (18.2) | 14.1–22.2 |
| Fever | 9 (16.4) | 12.5–20.2 |
| Abdominal pain | 7 (12.7) | 9.3–16.1 |
| Chest pain | 4 (7.3) | 4.7–9.8 |
| Weight gain | 3 (5.5) | 3.2–7.7 |
| Rash | 3 (5.5) | 3.2–7.7 |
| Clinical Features | Non-ME/CFS Patients (n = 10) | 95% CI |
| Headache | 10 (90.9) | 81.9–100.0 |
| Myalgia | 8 (72.7) | 64.6–80.8 |
| Difficulty concentrating | 7 (63.6) | 56.1–71.2 |
| Neck stiffness | 7 (63.6) | 56.1–71.3 |
| Fatigue | 6 (54.5) | 47.5–61.5 |
| Tender lymph nodes | 5 (45.5) | 39.0–51.9 |
| Arthralgia | 5 (45.5) | 39.0–51.9 |
| Tachycardia | 5 (45.5) | 39.0–51.9 |
| Weight loss | 4 (36.4) | 30.6–42.1 |
| Night sweats | 4 (36.4) | 30.6–42.1 |
| Orthostatic hypotension | 4 (36.4) | 30.6–42.1 |
| Sleep disturbances | 3 (27.3) | 22.3–32.2 |
| Fever | 2 (18.2) | 14.1–22.2 |
| Chest pain | 2 (18.2) | 14.1–22.2 |
| Abdominal pain | 0 (0.0) | 0.0–0.0 |
| Weight gain | 0 (0.0) | 0.0–0.0 |
| Rash | 0 (0.0) | 0.0–0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krumina, A.; Vecvagare, K.; Svirskis, S.; Gravelsina, S.; Nora-Krukle, Z.; Gintere, S.; Murovska, M. Clinical Profile and Aspects of Differential Diagnosis in Patients with ME/CFS from Latvia. Medicina 2021, 57, 958. https://doi.org/10.3390/medicina57090958
Krumina A, Vecvagare K, Svirskis S, Gravelsina S, Nora-Krukle Z, Gintere S, Murovska M. Clinical Profile and Aspects of Differential Diagnosis in Patients with ME/CFS from Latvia. Medicina. 2021; 57(9):958. https://doi.org/10.3390/medicina57090958
Chicago/Turabian StyleKrumina, Angelika, Katrine Vecvagare, Simons Svirskis, Sabine Gravelsina, Zaiga Nora-Krukle, Sandra Gintere, and Modra Murovska. 2021. "Clinical Profile and Aspects of Differential Diagnosis in Patients with ME/CFS from Latvia" Medicina 57, no. 9: 958. https://doi.org/10.3390/medicina57090958