Management of Glucose Control in Noncritically Ill, Hospitalized Patients Receiving Parenteral and/or Enteral Nutrition: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
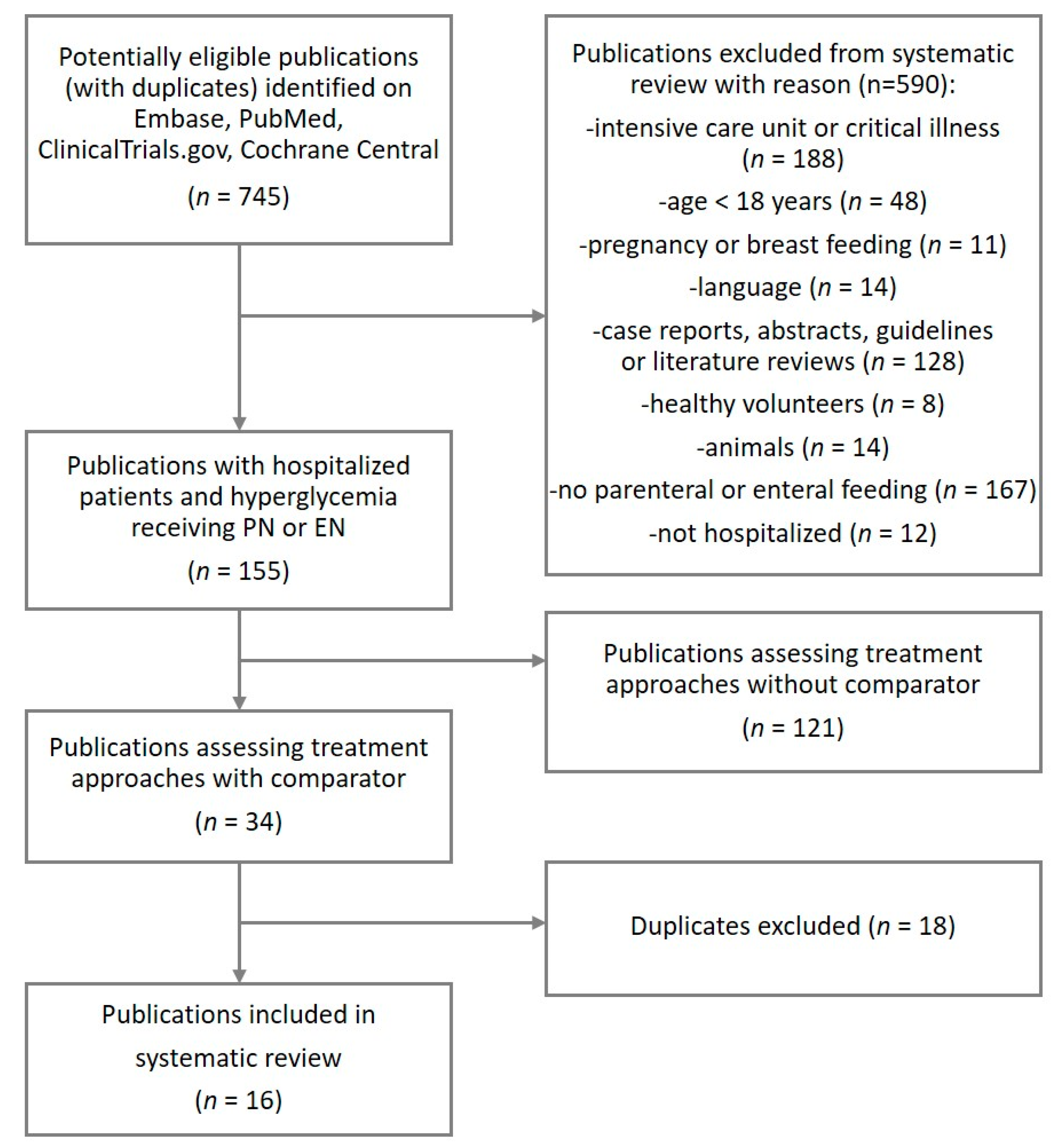
3.1. Study Identification and Selection
3.2. Characteristics of the Included Studies
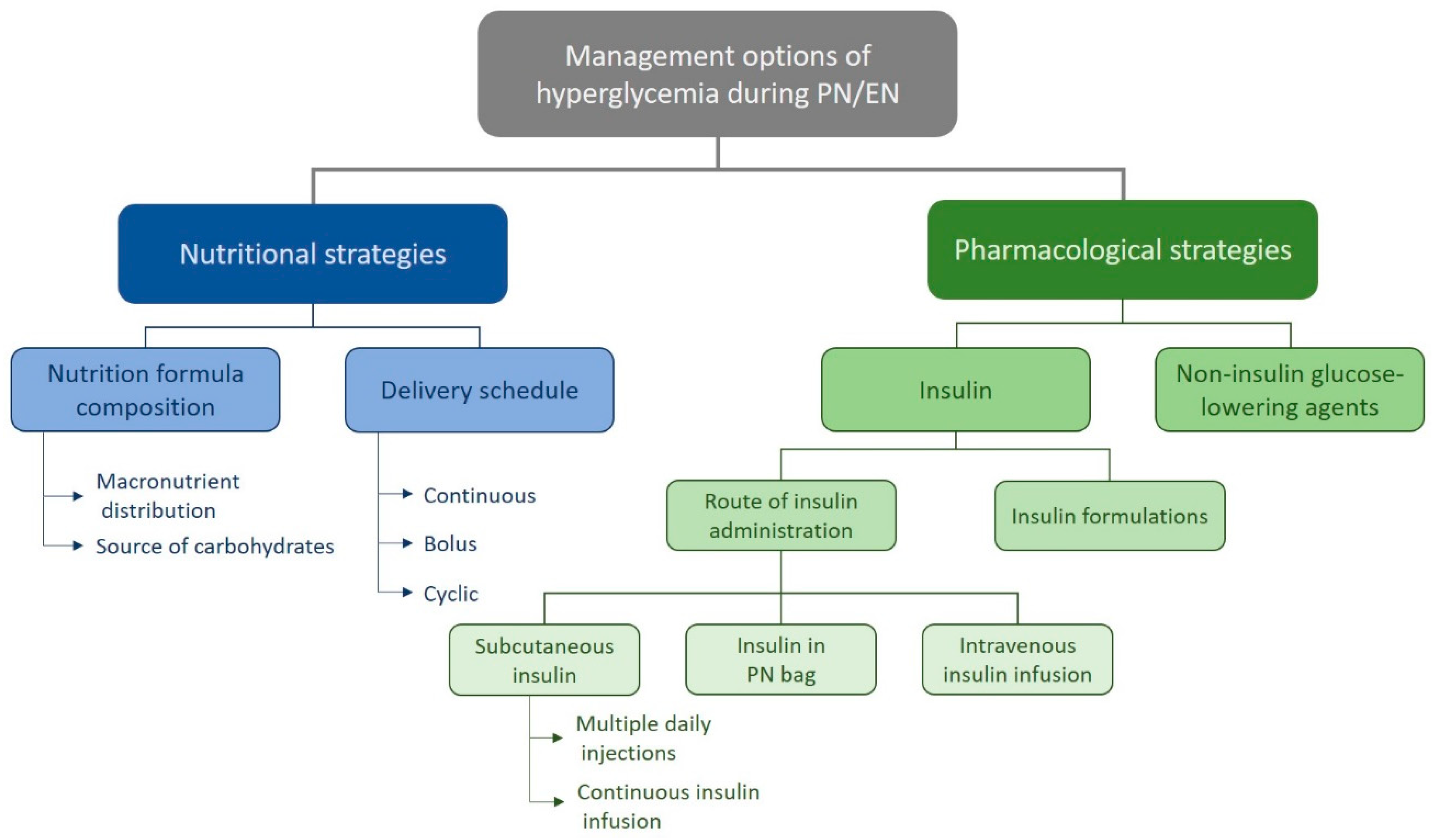
3.3. Studies Examining Nutritional Strategies
3.4. Studies Examining Insulin Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Pasquel, F.J.; Spiegelman, R.; McCauley, M.; Smiley, D.; Umpierrez, D.; Johnson, R.; Rhee, M.; Gatcliffe, C.; Lin, E.; Umpierrez, E.; et al. Hyperglycemia during total parenteral nutrition: An important marker of poor outcome and mortality in hospitalized patients. Diabetes Care 2010, 33, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Davidson, P.; Kwiatkowski, C.A.; Wien, M. Management of Hyperglycemia and Enteral Nutrition in the Hospitalized Patient. Nutr. Clin. Pract. 2015, 30, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Pleva, M.; Mirtallo, J.M.; Steinberg, S.M. Hyperglycemic events in non-intensive care unit patients receiving parenteral nutrition. Nutr. Clin. Pract. 2009, 24, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Pancorbo-Hidalgo, P.L.; Garcia-Fernandez, F.P.; Ramirez-Perez, C. Complications associated with enteral nutrition by nasogastric tube in an internal medicine unit. J. Clin. Nurs. 2001, 10, 482–490. [Google Scholar] [CrossRef] [PubMed]
- McCowen, K.C.; Malhotra, A.; Bistrian, B.R. Stress-Induced Hyperglycemia. J. Clin. Nurs. 2001, 17, 107–124. [Google Scholar] [CrossRef]
- Herrmann, C.; Göke, R.; Richter, G.; Fehmann, H.C.; Arnold, R.; Göke, B. Glucagon-Like Peptide-1 and Glucose-Dependent Insulin-Releasing Polypeptide Plasma Levels in Response to Nutrients. Digestion 1995, 56, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Andrews, R.C.; Walker, B.R. Glucocorticoids and insulin resistance: Old hormones, new targets. Clin. Sci. 1999, 96, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Marathe, C.S.; Rayner, C.K.; Bound, M.; Checklin, H.; Standfield, S.; Wishart, J.; Lange, K.; Jones, K.L.; Horowitz, M. Small intestinal glucose exposure determines the magnitude of the incretin effect in health and type 2 diabetes. Diabetes 2014, 63, 2668–2675. [Google Scholar] [CrossRef] [PubMed]
- Olveira, G.; Tapia, M.J.; Ocón, J.; Cabrejas-Gómez, C.; Ballesteros-Pomar, M.D.; Vidal-Casariego, A.; Arraiza-Irigoyen, C.; Olivares, J.; Conde-García, M.e.C.; García-Manzanares, A.; et al. Parenteral nutrition-associated hyperglycemia in non-critically ill inpatients increases the risk of in-hospital mortality (multicenter study). Diabetes Care 2013, 36, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.Y.; Lin, H.C.; Lee, P.C.; Ma, W.Y.; Lin, H.D. Hyperglycemia correlates with outcomes in patients receiving total parenteral nutrition. Am. J. Med Sci. 2007, 333, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.W.; Napier, B.; Zaccaria, C.; Fletcher, J.P. Hyperglycemia is associated with adverse outcomes in patients receiving total parenteral nutrition. Diabetes Care 2005, 28, 2367–2371. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Liu, T.; Zhang, X.; Si, Y.; Ye, Y.; Zhao, C.; Wang, Q.; Shen, X. Intensive Versus Conventional Glycemic Control in Patients with Diabetes During Enteral Nutrition After Gastrectomy. J. Gastrointest. Surg. 2015, 19, 1553–1558. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Coburn, J.A.; Coto-Yglesias, F.; Dzyubak, S.; Hazem, A.; Lane, M.A.; Prokop, L.J.; Montori, V.M. Glycemic Control in Non-Critically Ill Hospitalized Patients: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2012, 97, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, Z.-Q.; Huo, J.-L.; Zhai, X.-J. Effects of perioperative tight glycemic control on postoperative outcomes: A meta-analysis. Endocr. Connect. 2018, 7, R316–R327. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Smiley, D.; Zisman, A.; Prieto, L.M.; Palacio, A.; Ceron, M.; Puig, A.; Mejia, R. Randomized Study of Basal-Bolus Insulin Therapy in the Inpatient Management of Patients with Type 2 Diabetes (RABBIT 2 Trial). Diabetes Care 2007, 30, 2181. [Google Scholar] [CrossRef] [PubMed]
- Turchin, A.; Matheny, M.E.; Shubina, M.; Scanlon, J.V.; Greenwood, B.; Pendergrass, M.L. Hypoglycemia and clinical outcomes in patients with diabetes hospitalized in the general ward. Diabetes Care 2009, 32, 1153–1157. [Google Scholar] [CrossRef]
- Finfer, S.; Chittock, D.R.; Su, S.Y.; Blair, D.; Foster, D.; Dhingra, V.; Bellomo, R.; Cook, D.; Dodek, P.; Henderson, W.R.; et al. Intensive versus Conventional Glucose Control in Critically Ill Patients. N. Engl. J. Med. 2009, 360, 1283–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association, A.D. 15. Diabetes Care in the Hospital. Diabetes Care 2019, 42, S173–S181. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Hellman, R.; Korytkowski, M.T.; Kosiborod, M.; Maynard, G.A.; Montori, V.M.; Seley, J.J.; Van den Berghe, G.; Society, E. Management of hyperglycemia in hospitalized patients in non-critical care setting: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 16–38. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, A.; Bansiya, V.; Woodward, J.M. Addition of Insulin to Parenteral Nutrition for Control of Hyperglycemia. JPEN 2018, 42, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Aragon, D. Evaluation of nursing work effort and perceptions about blood glucose testing in tight glycemic control. Am. J. Crit. Care 2006, 15, 370–377. [Google Scholar] [PubMed]
- Elia, M.; Ceriello, A.; Laube, H.; Sinclair, A.J.; Engfer, M.; Stratton, R.J. Enteral nutritional support and use of diabetes-specific formulas for patients with diabetes: A systematic review and meta-analysis. Diabetes Care 2005, 28, 2267–2279. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.; Brooke, J. Evaluation of the role of enteral nutrition in managing patients with diabetes: A systematic review. Nutrients 2014, 6, 5142–5152. [Google Scholar] [CrossRef] [PubMed]
- Rodbard, D. Continuous Glucose Monitoring: A Review of Recent Studies Demonstrating Improved Glycemic Outcomes. Diabetes Technol. Ther. 2017, 19, S25–S37. [Google Scholar] [CrossRef] [PubMed]
- Pickup, J.C. Insulin-pump therapy for type 1 diabetes mellitus. N. Engl J. Med. 2012, 366, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Bally, L.; Thabit, H.; Hovorka, R. Closed-loop for type 1 diabetes—an introduction and appraisal for the generalist. BMC Med. 2017, 15, 14. [Google Scholar] [CrossRef] [PubMed]
- Bally, L.; Thabit, H.; Hovorka, R. Glucose-responsive insulin delivery for type 1 diabetes: The artificial pancreas story. Int. J. Pharm. 2017. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Boughton, C.K.; Bally, L.; Martignoni, F.; Hartnell, S.; Herzig, D.; Vogt, A.; Wertli, M.M.; Wilinska, M.E.; Evans, M.L.; Coll, A.P.; et al. Fully closed-loop insulin delivery in inpatients receiving nutritional support: A two-center, open-label, randomized controlled trial. Lancet Diabetes Endocri. 2019, 7, 368–377. [Google Scholar] [CrossRef]
- Olveira, G.; Abuin, J.; Lopez, R.; Herranz, S.; Garcia-Almeida, J.M.; Garcia-Malpartida, K.; Ferrer, M.; Cancer, E.; Luengo-Perez, L.M.; Alvarez, J.; et al. Regular insulin added to total parenteral nutrition vs. subcutaneous glargine in non-critically ill diabetic inpatients, a multicenter randomized clinical trial: INSUPAR trial. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hakeam, H.A.; Mulia, H.A.; Azzam, A.; Amin, T. Glargine Insulin Use Versus Continuous Regular Insulin in Diabetic Surgical Noncritically Ill Patients Receiving Parenteral Nutrition: Randomized Controlled Study. JPEN 2017, 41, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Lidder, P.; Flanagan, D.; Fleming, S.; Russell, M.; Morgan, N.; Wheatley, T.; Rahamin, J.; Shaw, S.; Lewis, S. Combining enteral with parenteral nutrition to improve postoperative glucose control. Br. J. Nutr. 2010, 103, 1635–1641. [Google Scholar] [CrossRef] [PubMed]
- Tiyapanjanit, T.; Boonyavarakul, A. Comparative study between the Phramongkutklao’s diabetic blenderized diets and commercial diabetic diets on glycemic variability in continuous tube fed patients with type 2 diabetes. J. Med. Assoc. Thai. 2014, 97, 1151–1156. [Google Scholar] [PubMed]
- Leon-Sanz, M.; Garcia-Luna, P.P.; Sanz-Paris, A.; Gomez-Candela, C.; Casimiro, C.; Chamorro, J.; Pereira-Cunill, J.L.; Martin-Palmero, A.; Trallero, R.; Martinez, J.; et al. Glycemic and lipid control in hospitalized type 2 diabetic patients: Evaluation of 2 enteral nutrition formulas (low carbohydrate-high monounsaturated fat vs. high carbohydrate). JPEN 2005, 29, 21–29. [Google Scholar] [CrossRef]
- Hyperglycemia in Patients with Stroke and Indication of Enteral Nutrition. Available online: https://ClinicalTrials.gov/show/NCT03422900 (accessed on 20 May 2019).
- Li, F.F.; Zhang, W.L.; Liu, B.L.; Zhang, D.F.; Chen, W.; Yuan, L.; Chen, M.Y.; Zhai, X.F.; Wu, J.D.; Su, X.F.; et al. Management of glycemic variation in diabetic patients receiving parenteral nutrition by continuous subcutaneous insulin infusion (CSII) therapy. Sci. Rep. 2018, 8, 5888. [Google Scholar] [CrossRef]
- Kruyt, N.D.; Biessels, G.J.; Vriesendorp, T.M.; Devries, J.H.; Hoekstra, J.B.; Elbers, P.W.; Kappelle, L.J.; Portegies, P.; Vermeulen, M.; Roos, Y.B. Subjecting acute ischemic stroke patients to continuous tube feeding and an intensive computerized protocol establishes tight glycemic control. Neurocrit. Care 2010, 12, 62–68. [Google Scholar] [CrossRef]
- Korytkowski, M.T.; Salata, R.J.; Koerbel, G.L.; Selzer, F.; Karslioglu, E.; Idriss, A.M.; Lee, K.K.; Moser, A.J.; Toledo, F.G. Insulin therapy and glycemic control in hospitalized patients with diabetes during enteral nutrition therapy: A randomized controlled clinical trial. Diabetes Care 2009, 32, 594–596. [Google Scholar] [CrossRef]
- Valero, M.A.; Leon-Sanz, M.; Escobar, I.; Gomis, P.; de la Camara, A.; Moreno, J.M. Evaluation of nonglucose carbohydrates in parenteral nutrition for diabetic patients. Eur. J. Clin. Nutr. 2001, 55, 1111–1116. [Google Scholar] [CrossRef]
- Truong, S.; Park, A.; Kamalay, S.; Hung, N.; Meyer, J.G.; Nguyen, N.; Momenzadeh, A. Glycemic Control in Adult Surgical Patients Receiving Regular Insulin Added to Parenteral Nutrition vs. Insulin Glargine: A Retrospective Chart Review. Nutr. Clin. Pract. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hijaze, D.; Szalat, A. Retrospective Evaluation of Glycemic Control with Basal-Bolus or Neutral Protamine Hagedorn Insulin Regimens in Patients Receiving Continuous Enteral Nutrition Therapy in Medicine Wards. Nutr. Clin. Pract. 2017, 32, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.; Donegan, D.; MacMahon, J.; O’Hanlon, C.; Keane, N.; Agha, A.; Thompson, C.; Smith, D. Management of parenteral nutrition associated hyperglycemia: A comparison of subcutaneous and intravenous insulin regimen. Ir. Med. J. 2014, 107, 141–143. [Google Scholar] [PubMed]
- Hsia, E.; Seggelke, S.A.; Gibbs, J.; Rasouli, N.; Draznin, B. Comparison of 70/30 biphasic insulin with glargine/lispro regimen in non-critically ill diabetic patients on continuous enteral nutrition therapy. Nutr. Clin. Pract. 2011, 26, 714–717. [Google Scholar] [CrossRef] [PubMed]
- Dardai, E. Basics in clinical nutrition: Nutritional support in the diabetic patient. e-SPEN 2009, 4, e304–e307. [Google Scholar] [CrossRef] [Green Version]
- Woods, H.F.; Alberti, K.G. Dangers of intravenous fructose. Lancet 1972, 2, 1354–1357. [Google Scholar] [CrossRef]
- Thomas, D.W.; Edwards, J.B.; Gilligan, J.E.; Lawrence, J.R.; Edwards, R.G. Complications following intravenous administration of solutions containing xylitol. Med. J. Aust. 1972, 1, 1238–1246. [Google Scholar]
- Thomas, D.W.; Gilligan, J.E.; Edwards, J.B.; Edwards, R.G. Lactic acidosis and osmotic diuresis produced by xylitol infusion. Med. J. Aust. 1972, 1, 1246–1248. [Google Scholar]
- Keller, U. The sugar substitutes fructose and sorbite: An unnecessary risk in parenteral nutrition. Schweiz Med. Wochenschr. 1989, 119, 101–106. [Google Scholar]
- Tappy, L.; Schwarz, J.M.; Schneiter, P.; Cayeux, C.; Revelly, J.P.; Fagerquist, C.K.; Jequier, E.; Chiolero, R. Effects of isoenergetic glucose-based or lipid-based parenteral nutrition on glucose metabolism, de novo lipogenesis, and respiratory gas exchanges in critically ill patients. Crit. Care Med. 1998, 26, 860–867. [Google Scholar] [CrossRef]
- Ahrens, C.L.; Barletta, J.F.; Kanji, S.; Tyburski, J.G.; Wilson, R.F.; Janisse, J.J.; Devlin, J.W. Effect of low-calorie parenteral nutrition on the incidence and severity of hyperglycemia in surgical patients: A randomized, controlled trial. Crit. Care Med. 2005, 33, 2507–2512. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Koh, S.O.; Park, M.S. Higher dextrose delivery via TPN related to the development of hyperglycemia in non-diabetic critically ill patients. Nutr. Res. Pract. 2011, 5, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Forchielli, M.L.; Bongiovanni, F.; Platé, L.; Piazza, G.; Puggioli, C.; D’Alise, A.; Bersani, G. Insulin Instability in Parenteral Nutrition Admixtures. JPEN 2018, 42, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Mühlebach, S.; Franken, C.; Stanga, Z.; Working group for developing the guidelines for parenteral nutrition of The German Association for Nutritional Medicine. Practical handling of AIO admixturesߞGuidelines on Parenteral Nutrition, Chapter 10. Ger. Med. Sci. 2009, 7, Doc18. [Google Scholar] [CrossRef]
- Pasquel, F.J.; Gianchandani, R.; Rubin, D.J.; Dungan, K.M.; Anzola, I.; Gomez, P.C.; Peng, L.; Hodish, I.; Bodnar, T.; Wesorick, D.; et al. Efficacy of sitagliptin for the hospital management of general medicine and surgery patients with type 2 diabetes (Sita-Hospital): A multicentre, prospective, open-label, non-inferiority randomized trial. Lancet Diabetes Endocrinol 2017, 5, 125–133. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design 1 | Sample Size | Population | Nutrition Therapy | Interventions | Primary Outcome {Study Period} | Main Results | Risk of Bias 3 |
|---|---|---|---|---|---|---|---|---|
| Insulin adaptation | ||||||||
| Boughton et al., 2019 [31] | RCT, parallel, two-center | 43 | Non-T1D surgical and medical | PN and/or EN | Fully automated s.c. closed-loop insulin delivery (closed loop, n = 21) | % time in target (5.6–10.0 mM) based on CGM values {Up to 15 d or discharge} | % time in target higher in closed-loop vs. control (68% vs. 36%, p < 0.0001); hypoglycemia (<3.9 mM) infrequent and similar between closed-loop and control (0.5% for both), p = ns) | Low |
| Conventional s.c. insulin therapy according to local practice (control, n = 22) | ||||||||
| Olveira et al., 2019 [32] | RCT, parallel, multi-center (26 sites) | 161 | T2D surgical and medical | TPN | 100% regular insulin in PN bag (100% in bag, n = 80) | Mean glucose based on capillary POC BG values {Up to 15 d or until PN stop} | Mean glucose during TPN 9.2 vs. 9.6 mM 100% in bag vs. 50% in bag (ns); mean glucose 48 h post-TPN higher in 100% in bag vs. 50% in bag (8.9 vs. 7.9 mM, p = 0.024); number of patients with hypoglycemia (≤3.9 mM) lower in 100% in bag vs. 50% in bag (9 vs. 22, p = 0.016) | Medium |
| 50% s.c. glargine + 50% regular insulin in PN bag (50% in bag, n = 81) | ||||||||
| Li et al., 2018 [38] | RCT, parallel, single-center | 102 | T2D surgical | PN (cyclic) | Continuous s.c. insulin infusion (CSII, n = 50) | mean amplitude of glycemic excursion (MAGE) based on CGM {4 d} | MAGE lower in CSII vs. basbol (3.7 vs. 6.2 mM, p < 0.05), no hypoglycemia events (<3.9 mM) occurred | High |
| S.c. basal–bolus glargine/aspart (basbol, n = 52) | ||||||||
| Hakeam et al., 2017 [33] | RCT, parallel, single-center | 67 | Non-T1D surgical (non-cardiac) | PN | S.c. glargine (scGlarg, n = 35) | Mean glucose based on capillary POC BG values from day 5 on PN and % of patients who achieved target glycaemia (7.8–10.0 mM) {9 d} | Comparable mean BG in scGlar vs. RIbag, % of values in target 52% in scGlar vs. 48% in RIbag (p = 0.06); no significant difference in hypoglycemic (<3.9 mM) events | Medium |
| Regular insulin added to PN bag (RIbag, n = 32) | ||||||||
| Yuan et al., 2015 [12] | RCT, parallel, single-center | 212 | T2D surgical (gastrectomy for gastric cancer) | EN (continuous) | VRII (short-acting insulin NOS) (VRII, n = 106) | PO not specified; mean glucose based on capillary POC BG values, infective and noninfective complications {8–10 d} | Mean BG lower in VRII vs. s.c.Ins. (5.4 vs. 9.5 mM, p < 0.001); higher rate of severe hypoglycemia (≤2.2 mM) in VRII vs. s.c.Ins. (8% vs. 1%, p = 0.035) | High |
| S.c. conventional insulin therapy (s.c.Ins., n = 106) | ||||||||
| Kruyt et al., 2010 [39] | Single-arm intervention with historical control | 23 | Hyperglycemic patients (excluded patients with previous insulin use)medical (stroke unit) | EN | Continuous feeding with computerized VRII group (continuous, n = 10) | % of capillary POC BG values in target range (4.4–6.1 mM){5 d} | Higher % values in target and mean glucose in continuous vs. inter group (55% vs. 19%, p < 0.005 and 5.8 vs. 7.6 mM, p < 0.005) | Medium |
| Bolus feeding with regular i.v. insulin adaptation intermediate group (inter, n = 13) | ||||||||
| Korytkowski et al., 2009 [40] | RCT, parallel, single-center | 50 | Diabetes NOS surgical and medical | EN | S.c. SSI (regular insulin) every 4–6 h (SSRI, n = 25); (NPH initialized if persistent BG > 10.0 mM) | PO not specified; mean glucose based on capillary POC BG values {8 d} | mean BG similar in SSRI and basalPLUS (8.9 vs. 9.2 mM, p = ns); NPH initialized in 55% of those on SSRI | High |
| S.c. SSRI plus s.c. glargine (basalPLUS, n = 25) | ||||||||
| Nutrition adaptation | ||||||||
| Tiyapanjanit et al., 2014 [35] | Non-randomized cross-over (no washout) | 10 | T2D (BG < 10 mM wo antidiabetic medication) medical | EN (continuous) | In-house prepared EN formula with 50% CHO thereof 67% fructose, (inhouse, n = 10) | PO not specified; mean glucose based on capillary POC BG values; glycemic variability based on CGM {3 d, each formula for 36 h) | Mean glucose lower in inhouse vs. standard group (6.8 vs. 8.0 mM, p = 0.022); glucose variability comparable | High |
| Standard diabetic EN formula with 53% CHO thereof 15% fructose and 57% maltodextrin (standard, n = 10) | ||||||||
| Lidder et al., 2009 [34] | RCT, parallel, single-center | 30 | Prediabetes (fasting BG < 7 mM) surgical (esophagectomy for esophageal cancer) | PN with or wo EN | 100% of energy covered by PN (PN, n = 14) | Mean glucose values based on CGM values {surgery until postoperative day 5} | Mean glucose comparable over entire study period, lower from day 3 post-surgery to day 5 post-surgery in PN + EN vs. PN (p = 0.002) | Medium |
| 70% covered by PN + 30% covered by EN (PN + EN, n = 16) | ||||||||
| Léon-Sanz et al., 2005 [36] | RCT, parallel, multi-center (4 sites) | 104 | T2D surgical and medical | EN (continuous) | Low-CHO high-MUFA nutrition formula (lowCHO, n = 51) | Mean glucose based on capillary POC BG values and mean daily insulin dose {2 weeks} | BG increase from baseline lower in lowCHO than highCHO after 7 d on EN (10% vs. 21%, p = 0.006); mean BG identical (12.7 vs. 12.7 mM2) | Medium |
| Energy-matched high-CHO nutrition formula (highCHO, n = 53) | ||||||||
| Valero et al., 2001 [41] | RCT, parallel, double-blind, single-center | 138 | T1D (21%) and T2D (79%) surgical and medical | TPN (continuous) | Standard TPN containing glucose (PN_G, n = 71) | PO not specified; number of patients with target glycaemia (capillary POC BG values 8.3–11.1 mM) at end of TPN {TPN duration 5–46 d) | BG < 11.1 mM at end of TPN reached in 75% vs. 85% in PN_G and PN_GFX respectively 2 | High |
| Energy-matched TPN containing glucose:fructose:xylitol 2:1:1 (PN_GFX, n = 67) |
| Author, Year | Study Design | Sample Size | Population | Nutrition Therapy | Interventions | Primary Outcome {Study Period} | Main Results |
|---|---|---|---|---|---|---|---|
| Insulin adaptation | |||||||
| Truong et al., 2019 [42] | Retrospective observational, single-center | 102 | Hyperglycemic patients (≥ 2 BG values > 10.0 mM, including T1D and T2D) surgical and medical | PN (continuous or cyclic) | Regular insulin added to PN bag (100% bag, n = 78) | % of patients with ≥5/6 capillary POC BG values per day <10.0 mM for ≥2 consecutive days {during PN or until target reached} | Higher % of patients with target achieved in 100%bag vs. scGlarg (72% vs. 49%, p = 0.017); ≥2 hypoglycemic events (<3.9 mM) in 9% of 100%bag and 17% of scGlarg group (p = ns); lower need for corrective insulin less in 100%bag vs. scGlarg (28 vs. 57% of patients, p = 0.003) |
| S.c. insulin glargine (scGlarg, n = 35) | |||||||
| Hijaze et al., 2017 [43] | Retrospective observational, single-center | 53 | Non-T1D medical | EN (continuous) | S.c. NPH insulin 3×/day (NPH, n = 26) (Rescue bolus with 6 units rapid insulin analoga if BG > 16.7 mM) | PO not specified; mean glucose based on capillary POC BG values and % of values in the target range (7.8–10 mM) {until discharge or stop EN} | mean BG comparable in NPH vs. basbol (10.6 vs. 11.1 mM, p = ns), 24% and 22% of values in range (p = ns) |
| S.c. basal–bolus insulin analoga therapy (basbol, n = 27) | |||||||
| Neff et al., 2014 [44] | Retrospective observational, single-center | 53 | Hyperglycemic patients (BG > 10 mM including T1D and T2D) surgical and medical | PN | Protocol-driven VRII (VRII, n = 32) | PO not specified; mean glucose based on POC BG values and % of values in target range (4.0–10.0 mM) {until stop PN} | Mean glucose lower and % values in target range higher in VRII vs. basbol (9.6 vs. 11.2 mM, p = 0.009 and 62% vs. 43%, p = 0.008) |
| S.c. basal–bolus insulin (basbol, n = 21) | |||||||
| Hsia et al., 2011 [45] | Retrospective observational, single-center | 22 | Diabetes NOS surgical and medical | EN (continuous) | S.c. basal–bolus with glargine/lispro (basbol, n = 8) | PO not specified; mean glucose based on POC BG values, % of values in target range (7.8–10.0 mM) {72 h} | mean glucose comparable, % of values in target range higher in mixed3 vs. mixed2 and basbol (69% vs. 22% vs. 24%, p < 0.01); patients with hypoglycemic events (<3.9 mM) in basbol vs. mixed2 and mixed3 (5 vs. 2 vs. 1) |
| S.c. 70/30 premixed insulin 2×/day (mixed2, n = 8) | |||||||
| S.c. 70/30 pre-mixed insulin 3×/day (mixed3, n = 6) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laesser, C.I.; Cumming, P.; Reber, E.; Stanga, Z.; Muka, T.; Bally, L. Management of Glucose Control in Noncritically Ill, Hospitalized Patients Receiving Parenteral and/or Enteral Nutrition: A Systematic Review. J. Clin. Med. 2019, 8, 935. https://doi.org/10.3390/jcm8070935
Laesser CI, Cumming P, Reber E, Stanga Z, Muka T, Bally L. Management of Glucose Control in Noncritically Ill, Hospitalized Patients Receiving Parenteral and/or Enteral Nutrition: A Systematic Review. Journal of Clinical Medicine. 2019; 8(7):935. https://doi.org/10.3390/jcm8070935
Chicago/Turabian StyleLaesser, Céline Isabelle, Paul Cumming, Emilie Reber, Zeno Stanga, Taulant Muka, and Lia Bally. 2019. "Management of Glucose Control in Noncritically Ill, Hospitalized Patients Receiving Parenteral and/or Enteral Nutrition: A Systematic Review" Journal of Clinical Medicine 8, no. 7: 935. https://doi.org/10.3390/jcm8070935