
The Classification of Substance Use Disorders: Historical, Contextual, and Conceptual Considerations

Abstract
:1. Introduction
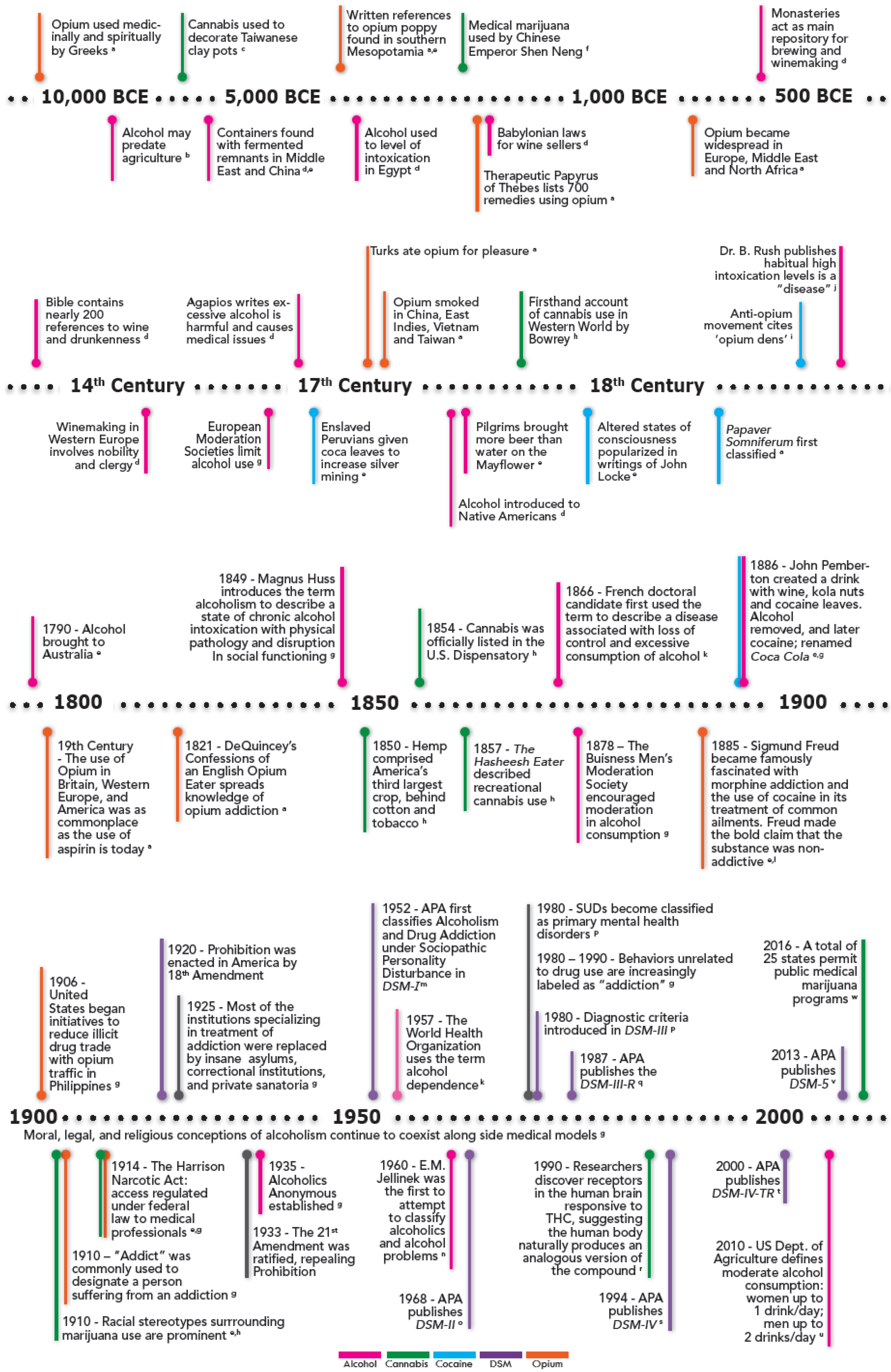
2. Historical Considerations: A Long History of Psychoactive Substances
2.1. Opioids
2.2. Cannabis
2.3. Cocaine
2.4. Alcohol
3. Cultural and Contextual Considerations
3.1. Societal Influences on Attitudes and Perceptions of Substance Use
3.1.1. Religious Influences
Paul the apostle considered wine to be a creation of God and therefore inherently good and recommended its use for medicinal purposes but condemned intoxication and recommended abstinence for those who could not control their drinking.[4] (p. 3)
3.1.2. Cultural Influences
3.1.3. Industrialization
4. Legality and Morality
5. Modern Developments
5.1. Opioids
5.2. Cannabis
5.3. Cocaine
5.4. Alcohol
6. Modern Classification of Substance Use Disorders: The DSM
6.1. DSM-I: 1952
6.2. DSM-II: 1968
6.3. DSM-III: 1980
Such criticisms would form the basis for recommendations to alter these categories in the next iteration.distinction between “abuse” and “dependence” is made entirely on the basis of evidence for the presence of physiological tolerance or withdrawal…[which leaves the current system] vulnerable to powerful, swiftly changing social forces such as the tightening of laws restricting alcohol use while driving. Thus, for example, actions of a legislature in a particular state can determine the number of residents who met DSM-III criteria for a mental disorder (i.e., alcohol abuse).[52]
6.4. DSM-III-R (1987)
6.5. DSM-IV (1994), DSM-IV-TR (2000)
6.6. DSM-5: 2013 (See Also Section 7)
7. Discussion
7.1. Potential Practical Implications of Atheoretical Nosology
7.2. Removal of Legal Problems Criterion
7.3. Removal of the Abuse/Dependence Paradigm
7.4. Addition of Craving Criterion
7.5. Inclusion of “Behavioral Addictions”
8. Conclusions
While mental health disorders have characteristically lacked clearly demarcated boundaries and have so far largely defied attempts to elucidate and categorize their exclusive etiologies, an increasing number of individuals have, over time, connected such concerns to the descriptive vs. etiological nature of psychiatric nosology and the limitations inherent in maintaining such a model [107,108].The evolution of the DSM illustrates that what is considered to be “medical” and “scientific” is often not an immutable standard, but rather, may be variable across time and culture, and in this way contingent upon changes in dominant schools of thought.[108] (p. 7)
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- Davenport-Hines, R. The Pursuit of Oblivion: A Global History of Narcotics; WW Norton & Company: New York, NY, USA, 2003. [Google Scholar]
- Booth, M. Opium : A History; St. Martin’s Griffin: New York, NY, USA, 1999. [Google Scholar]
- Hanson, D. Historical Evolution of Alcohol Consumption in Society; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Earleywine, M. Understanding Marijuana: A New Look at the Scientific Evidence; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Sournia, J.C. A History of Alcoholism; Blackwell: London, UK, 1990. [Google Scholar]
- Grinspoon, L.; Bakalar, J.B. Marihuana, the Forbidden Medicine; Yale University Press: New Haven, CT, USA, 1997. [Google Scholar]
- White, W.L. Slaying the Dragon: The History of Addiction Treatment and Recovery in America; Chestnut Health Systems/Lighthouse Institute: Bloomington, IL, USA, 1998. [Google Scholar]
- Lee, M.A. Smoke Signals: A Social History of Marijuana—Medical, Recreational and Scientific; Scribner: New York, NY, USA, 2013. [Google Scholar]
- Berridge, V. Victorian Opium Eating: Responses to Opiate Use in Nineteenth-Century England. Vic. Stud. 1978, 21, 437–461. [Google Scholar] [PubMed]
- Shorter, E. The History of Nosology and the Rise of the Diagnostic and Statistical Manual of Mental Disorders. Dialogues Clin. Neurosci. 2015, 17, 59–67. [Google Scholar] [PubMed]
- Keller, M.; Doria, J. On Defining Alcoholism. Alcohol Health Res. World 1991, 15, 253–259. [Google Scholar]
- Markel, H. Über Coca: Sigmund Freud, Carl Koller, and Cocaine. JAMA 2011, 305, 1360–1361. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual: Mental Disorders, 1st ed.; American Psychiatric Association: Washington, DC, USA, 1952. [Google Scholar]
- Jellinek, E.M. The Disease Concept of Alcoholism; Hillhouse Press: New Haven, CT, USA, 1960. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 2nd ed.; American Psychiatric Association: Washington, DC, USA, 1968. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd rev. ed.; American Psychiatric Association: Washington, DC, USA, 1987. [Google Scholar]
- Howlett, A.C.; Bidaut-Russell, M.; Devane, W.A.; Melvin, L.S.; Johnson, M.R.; Herkenham, M. The Cannabinoid Receptor: Biochemical, Anatomical and Behavioral Characterization. Trends Neurosci. 1990, 13, 420–423. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services (USDA/HHS). Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans; USDA, Agricultural Research Service: Washington, DC, USA, 2010.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM--5®), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- National Conference of State Legislatures. State Medical Marijuana Laws. Avalable online: http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx (accessed on 7 December 2015).
- Abel, E.L. Marihuana, the First Twelve Thousand Years; Plenum Press: New York, NY, USA, 1980. [Google Scholar]
- Carter, T.F. The Invention of Printing in China and Its Spread Westward; Ronald Press: New York, NY, USA, 1955. [Google Scholar]
- Kunisaki, J. A Handy Guide to Papermaking; University of California Press: Berkeley, CA, USA, 1948. [Google Scholar]
- Karch, S.B. A Brief History of Cocaine; CRC Press: Boca Raton, FL, USA, 2005. [Google Scholar]
- Levy, J.V.; Freye, E. Pharmacology and Abuse of Cocaine, Amphetamines, Ecstasy and Related Designer Drugs: A Comprehensive Review on Their Mode of Action, Treatment of Abuse and Intoxication; Springer: Dordrecht, The Netherlands, 2009. [Google Scholar]
- Long, H.; Greller, H.; Mercurio-Zappala, M.; Nelson, L.S.; Hoffman, R.S. Medicinal Use of Cocaine: A Shifting Paradigm over 25 Years. Laryngoscope 2004, 114, 1625–1629. [Google Scholar] [CrossRef] [PubMed]
- Merrill, J.L. The Bible and the American Temperance Movement: Text, Context, and Pretext. Harv. Theol. Rev. 1988, 81, 145–170. [Google Scholar] [CrossRef]
- Alcoholics Anonymous. Alcoholics Anonymous: The Story of How Many Thousands of Men and Women Have Recovered from Alcoholism, 4th ed.; Alcoholics Anonymous World Services: New York, NY, USA, 2001. [Google Scholar]
- Silkworth, W.D. The Doctor’s Opinion. Available online: http://www.step12.com/silkworthdoctors-opinion.html(accessed on 25 November 2015).
- Alcoholics Anonymous General Service Office. Estimates of A.A. Groups and Members as of January 1, 2015. Available online: http://www.aa.org/assets/en_US/smf-53_en.pdf (accessed on 4 April 2016).
- Maines, R. The Technology of Orgasm: “Hysteria,” the Vibrator, and Women’s Sexual Satisfaction; American Council of Learned Societies: Baltimore, MD, USA, 2001. [Google Scholar]
- Yorke, C. A Critical Review of Some Psychoanalytic Literature on Drug Addiction. Br. J. Med. Psychol. 1970, 43, 141–159. [Google Scholar] [CrossRef] [PubMed]
- Independence Hall Association. Economic Growth and the Early Industrial Revolution. Available online: http://www.ushistory.org (accessed on 21 March 2016).
- Provine, D.M. Unequal under Law: Race in the War on Drugs; University of Chicago Press: Chicago, IL, USA, 2008. [Google Scholar]
- Fields, H.L. The Doctor’s Dilemma: Opiate Analgesics and Chronic Pain. Neuron 2011, 69, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, A.; Marsch, L.A.; Joseph, H.; Portenoy, R.K. Opioids and the Treatment of Chronic Pain: Controversies, Current Status, and Future Directions. Exp. Clin. Psychopharmacol. 2008, 16, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Prescription Painkiller Overdoses in the U.S.; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2011. [Google Scholar]
- National Institute on Drug Abuse. Trends & Statistics; National Institute on Drug Abuse: North Bethesda, MD, USA, 2014. [Google Scholar]
- Thompson, A.E. Medical Marijuana. JAMA 2015, 313, 2508. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2015. [Google Scholar]
- Grabowski, J. NIDA Research Monographs 50, Cocaine: Pharmacology, Effects, and Treatment of Abuse; Diane Publishing Co: Darby, PA, USA, 1994. [Google Scholar]
- U.S. Department of Justice. List of Controlled Substances. Drug Enforcement Administration. Available online: http://www.deadiversion.usdoj.gov/schedules (accessed on 15 December 2015).
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Wilson, M. DSM-III and the Transformation of American Psychiatry: A History. Am. J. Psychiatry 1993, 150, 399–410. [Google Scholar] [PubMed]
- Paris, J.; Phillips, J. Making the DSM-5: Concepts and Controversies; Springer: New York, NY, USA, 2013. [Google Scholar]
- American Medical Association. AMA History Timeline. Available online: http://www.ama-assn.org/ama/pub/about-ama/our-history/ama-history-timeline.pagefiles/38/AMAHistoryTimeline.html (accessed on 31 March 2015).
- Feighner, J.P.; Robins, E.; Guze, S.B.; Woodruff, R.A., Jr.; Winokur, G.; Munoz, R. Diagnostic Criteria for Use in Psychiatric Research. Arch. Gen. Psychiatry 1972, 26, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Williams, J.B.; Skodol, A.E. DSM-III: The Major Achievements and an Overview. Am. J. Psychiatry. 1980, 137, 151–164. [Google Scholar] [PubMed]
- Rounsaville, B.J.; Spitzer, R.L.; Williams, J.B. Proposed Changes in DSM-III Substance Use Disorders: Description and Rationale. Am. J. Psychiatry 1986, 143, 463–468. [Google Scholar] [PubMed]
- Widiger, T.A.; Smith, G.T. Addiction and Nosology. In Apa Addiction Syndrome Handbook, Vol. 1: Foundations, Influences, and Expressions of Addiction; Shaffer, H.J., LaPlante, D.A., Nelson, S.E., Shaffer, H.J., LaPlante, D.A., Nelson, S.E., Eds.; American Psychological Association: Washington, DC, USA, 2012; pp. 49–66. [Google Scholar]
- Edwards, G. The Alcohol Dependence Syndrome: A Concept as Stimulus to Enquiry. Br. J. Addict. 1986, 81, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, J.C. DSM-5 Substance Use Disorder: How Conceptual Missteps Weakened the Foundations of the Addictive Disorders Field. Acta Psychiatr. Scand. 2015, 132, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Beckson, M.; Tucker, D. Commentary: Craving Diagnostic Validity in DSM-5 Substance Use Disorders. J. Am. Acad. Psychiatry Law 2014, 42, 453–458. [Google Scholar] [PubMed]
- Hasin, D.S.; Fenton, M.C.; Beseler, C.; Park, J.Y.; Wall, M.M. Analyses Related to the Development of DSM-5 Criteria for Substance Use Related Disorders: 2. Proposed DSM-5 Criteria for Alcohol, Cannabis, Cocaine and Heroin Disorders in 663 Substance Abuse Patients. Drug Alcohol Depend. 2012, 122, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A.; Barlow, D.H. Dimensional Versus Categorical Classification of Mental Disorders in the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders and Beyond: Comment on the Special Section. J. Abnorm. Psychol. 2005, 114, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Krueger, R.F. The Structure of Common Mental Disorders. Arch. Gen. Psychiatry 1999, 56, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Widiger, T.A.; Simonsen, E. Alternative Dimensional Models of Personality Disorder: Finding a Common Ground. J. Personal. Disord. 2005, 19, 110–130. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Bhat, V.; Adler, D.; Dixon, L.; Goldman, B.; Koh, S.; Levine, B.; Oslin, D.; Siris, S. How Do Clinicians Actually Use the Diagnostic and Statistical Manual of Mental Disorders in Clinical Practice and Why We Need to Know More. J. Nerv. Ment. Dis. 2014, 202, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.S.; Ahn, W.-K. Clinical Psychologists’ Theory-Based Representations of Mental Disorders Predict Their Diagnostic Reasoning and Memory. J. Exp. Psychol. Gen. 2002, 131, 451–476. [Google Scholar] [CrossRef] [PubMed]
- Sobell, L.C.; Ellingstad, T.P.; Sobell, M.B. Natural Recovery from Alcohol and Drug Problems: Methodological Review of the Research with Suggestions for Future Directions. Addiction 2000, 95, 749–764. [Google Scholar] [CrossRef] [PubMed]
- Sobell, M.B.; Sobell, L.C. Controlled Drinking after 25 Years: How Important Was the Great Debate? Addiction 1995, 90, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Sobell, M.B.; Sobell, L.C. Moderation, Public Health and Paternalism. Addiction 1995, 90, 1175–1177. [Google Scholar] [CrossRef]
- Volkow, N.D.; Koob, G. Brain Disease Model of Addiction: Why Is It So Controversial? Lancet Psychiatry 2015, 2, 677–679. [Google Scholar] [CrossRef]
- Hall, W.; Carter, A.; Forlini, C. The Brain Disease Model of Addiction: Is It Supported by the Evidence and Has It Delivered on Its Promises? Lancet Psychiatry 2015, 2, 105–110. [Google Scholar] [CrossRef]
- Heyman, G.M. Addiction: A Disorder of Choice; Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Beutler, L.E.; Williams, R.E.; Wakefield, P.J.; Entwistle, S.R. Bridging Scientist and Practitioner Perspectives in Clinical Psychology. Am. Psychol. 1995, 50, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.E. Charlatanism, Scientism, and Psychology’s Social Contract. 103rd Annual Convention of the American Psychological Association: Presidential Address (1995, New York, New York). Am. Psychol. 1996, 51, 777–784. [Google Scholar] [CrossRef]
- Lilienfeld, S.O. Can Psychology Become a Science? Personal. Individ. Differ. 2010, 49, 281–288. [Google Scholar] [CrossRef]
- Stewart, R.E.; Chambless, D.L.; Baron, J. Theoretical and Practical Barriers to Practitioners’ Willingness to Seek Training in Empirically Supported Treatments. J. Clin. Psychol. 2012, 68, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Barlow, D.H.; Levitt, J.T.; Bufka, L.F. The Dissemination of Empirically Supported Treatments: A View to the Future. Behav. Res. Ther. 1999, 37, S147–S162. [Google Scholar] [CrossRef]
- Forman, R.F.; Bovasso, G.; Woody, G. Staff Beliefs About Addiction Treatment. J. Subst. Abus. Treat. 2001, 21, 1–9. [Google Scholar] [CrossRef]
- Herbeck, D.M.; Hser, Y.-I.; Teruya, C. Empirically Supported Substance Abuse Treatment Approaches: A Survey of Treatment Providers’ Perspectives and Practices. Addict. Behav. 2008, 33, 699–712. [Google Scholar] [CrossRef] [PubMed]
- Willenbring, M.L.; Kivlahan, D.; Kenny, M.; Grillo, M.; Hagedorn, H.; Postier, A. Beliefs About Evidence-Based Practices in Addiction Treatment: A Survey of Veterans Administration Program Leaders. J. Subst. Abus. Treat. 2004, 26, 79–85. [Google Scholar] [CrossRef]
- Mark, T.L.; Kassed, C.A.; Vandivort-Warren, R.; Levit, K.R.; Kranzler, H.R. Alcohol and Opioid Dependence Medications: Prescription Trends, Overall and by Physician Specialty. Drug Alcohol Depend. 2009, 99, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, H.K.; Ducharme, L.J.; Roman, P.M. The Adoption of Medications in Substance Abuse Treatment: Associations with Organizational Characteristics and Technology Clusters. Drug Alcohol Depend. 2007, 87, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.A.; Lukens, J.M.; Kole, J.W.; Sisti, D.A. Views About Responsibility for Alcohol Addiction and Negative Evaluations of Naltrexone. Subst. Abus. Treat. Prev. Policy 2015, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Rubinsky, A.D.; Chen, C.; Batki, S.L.; Williams, E.C.; Harris, A.H. Comparative Utilization of Pharmacotherapy for Alcohol Use Disorder and Other Psychiatric Disorders among US Veterans Health Administration Patients with Dual Diagnoses. J. Psychiatr. Res. 2015, 69, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Compton, W.M.; Saha, T.D.; Conway, K.P.; Grant, B.F. The Role of Cannabis Use within a Dimensional Approach to Cannabis Use Disorders. Drug Alcohol Depend. 2009, 100, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Saha, T.D.; Chou, S.P.; Grant, B.F. Toward an Alcohol Use Disorder Continuum Using Item Response Theory: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychol. Med. 2006, 36, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Shmulewitz, D.; Keyes, K.; Beseler, C.; Aharonovich, E.; Aivadyan, C.; Spivak, B.; Hasin, D. The Dimensionality of Alcohol Use Disorders: Results from Israel. Drug Alcohol Depend. 2010, 111, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Gelhorn, H.; Hartman, C.; Sakai, J.; Stallings, M.; Young, S.; Rhee, S.H.; Corley, R.; Hewitt, J.; Hopfer, C.; Crowley, T. Toward Dsm-V: An Item Response Theory Analysis of the Diagnostic Process for DSM-IV Alcohol Abuse and Dependence in Adolescents. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 1329–1339. [Google Scholar] [CrossRef] [PubMed]
- Fischer, B.A. A Review of American Psychiatry through Its Diagnoses: The History and Development of the Diagnostic and Statistical Manual of Mental Disorders. J. Nerv. Ment. Dis. 2012, 200, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L. The Diagnostic Status of Homosexuality in DSM-III: A Reformulation of the Issues. Am. J. Psychiatry 1981, 138, 210–215. [Google Scholar] [PubMed]
- American Psychiatric Association. Homosexuality and Sexuality Orientation Disturbance: Proposed Change in DSM-II, 6th Printing, Page 44; No. 730008; American Psychiatric Association: Arlington, VA, USA, 1973. [Google Scholar]
- Babor, T. Drug Policy and the Public Good; Oxford University Press: Oxford, NY, USA, 2010. [Google Scholar]
- Kurtzleben, D. Data Show Racial Disparity in Crack Sentencing. US News & World Report. 2010. Available online: http://www.usnews.com/news/articles/2010/08/03/data-show-racial-disparity-in-crack-sentencing (accessed on 8 March 2016).
- Nutt, D.J.; King, L.A.; Phillips, L.D. Drug Harms in the UK: A Multicriteria Decision Analysis. Lancet 2010, 376, 1558–1565. [Google Scholar] [CrossRef]
- Van Amsterdam, J.; Opperhuizen, A.; Koeter, M.; Van Den Brink, W. Ranking the Harm of Alcohol, Tobacco and Illicit Drugs for the Individual and the Population. Eur. Addict. Res. 2010, 16, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Weissenborn, R.; Nutt, D.J. Popular Intoxicants: What Lessons Can Be Learned from the Last 40 Years of Alcohol and Cannabis Regulation? J. Psychopharmacol. 2012, 26, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Borges, G.; Ye, Y.; Bond, J.; Cherpitel, C.J.; Cremonte, M.; Moskalewicz, J.; Swiatkiewicz, G.; Rubio-Stipec, M. The Dimensionality of Alcohol Use Disorders and Alcohol Consumption in a Cross-National Perspective. Addiction 2010, 105, 240–254. [Google Scholar] [CrossRef] [PubMed]
- Harford, T.C.; Yi, H.Y.; Faden, V.B.; Chen, C.M. The Dimensionality of DSM-IV Alcohol Use Disorders among Adolescent and Adult Drinkers and Symptom Patterns by Age, Gender, and Race/Ethnicity. Alcohol. Clin. Exp. Res. 2009, 33, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Hasin, D.S.; Beseler, C.L. Dimensionality of Lifetime Alcohol Abuse, Dependence and Binge Drinking. Drug Alcohol Depend. 2009, 101, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Hasin, D.S. Socio-Economic Status and Problem Alcohol Use: The Positive Relationship between Income and the DSM-IV Alcohol Abuse Diagnosis. Addiction 2008, 103, 1120–1130. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F.; Caetano, R. The Trouble with Alcohol Abuse: What Are We Trying to Measure, Diagnose, Count and Prevent? Addiction 2008, 103, 1057–1059. [Google Scholar] [CrossRef] [PubMed]
- Hasin, D.; Paykin, A.; Endicott, J.; Grant, B. The Validity of DSM-IV Alcohol Abuse: Drunk Drivers Versus All Others. J. Stud. Alcohol. 1999, 60, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Szasz, T.S. The Myth of Mental Illness. Am. Psychol. 1960, 15, 113–118. [Google Scholar] [CrossRef]
- Kendler, K.S.; Gardner, C.O., Jr. Boundaries of Major Depression: An Evaluation of DSM-IV Criteria. Am. J. Psychiatry 1998, 155, 172–177. [Google Scholar] [PubMed]
- Najman, J.M. Commentary on Wakefield & Schmitz (2015): Diagnosing an Alcohol Use Disorder—What Criteria Should Be Used? Addiction 2015, 110, 943–944. [Google Scholar] [PubMed]
- Norko, M.A.; Fitch, W.L. ‘DSM-5 and Substance Use Disorders’: Reply. J. Am. Acad. Psychiatry Law 2015, 43, 263–264. [Google Scholar] [PubMed]
- Haass-Koffler, C.L.; Leggio, L.; Kenna, G.A. Pharmacological Approaches to Reducing Craving in Patients with Alcohol Use Disorders. CNS Drugs 2014, 28, 343–360. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.E.; Berridge, K.C. The Neural Basis of Drug Craving: An Incentive-Sensitization Theory of Addiction. Brain Res. Rev. 1993, 18, 247–291. [Google Scholar] [CrossRef]
- Blaszczynski, A. Commentary On: Are We Overpathologizing Everyday Life? A Tenable Blueprint for Behavioral Addiction Research. J. Behav. Addict. 2015, 4, 142–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frances, A.J. DSM-5 Suggests Opening the Door to Behavioral Addictions. Available online: https://www.psychologytoday.com/blog/dsm5-in-distress/201003/dsm5-suggests-opening-the-door-behavioral-addictions (accessed on 3 March 2016).
- Frances, A.J.; Widiger, T.A. Psychiatric Diagnosis: Lessons from the DSM-IV Past and Cautions for the DSM-5 Future. Annu. Rev. Clin. Psychol. 2012, 8, 109–130. [Google Scholar] [CrossRef] [PubMed]
- Kawa, S.; Giordano, J. A Brief Historicity of the Diagnostic and Statistical Manual of Mental Disorders: Issues and Implications for the Future of Psychiatric Canon and Practice. Philos. Ethics Humanit. Med. 2012, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K.; Sanislow, C.; Wang, P. Research Domain Criteria (Rdoc): Toward a New Classification Framework for Research on Mental Disorders. Am. J. Psychiatry 2010, 167, 748–751. [Google Scholar] [CrossRef] [PubMed]
- Goldfried, M.R. On Possible Consequences of National Institute of Mental Health Funding for Psychotherapy Research and Training. Prof. Psychol. Res. Pract. 2016, 47, 77–83. [Google Scholar] [CrossRef]
- Schutz, C.G. DSM-V, RDoC and Diagnostic Approaches in Addiction Research and Therapy. J. Addict. Res. Ther. 2012. [Google Scholar] [CrossRef]
- Moreno-López, L.; Catena, A.; Fernández-Serrano, M.J.; Delgado-Rico, E.; Stamatakis, E.A.; Pérez-García, M.; Verdejo-García, A. Trait Impulsivity and Prefrontal Gray Matter Reductions in Cocaine Dependent Individuals. Drug Alcohol Depend. 2012, 125, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.; Verdejo-García, A.; Goudriaan, A.E.; Roeyers, H.; Dom, G.; Vanderplasschen, W. Impulsivity as a Vulnerability Factor for Poor Addiction Treatment Outcomes: A Review of Neurocognitive Findings among Individuals with Substance Use Disorders. J. Subst. Abus. Treat. 2014, 47, 58–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilcox, C.E.; Pommy, J.M.; Adinoff, B. Neural Circuitry of Impaired Emotion Regulation in Substance Use Disorders. Am. J. Psychiatry 2016, 173, 344–361. [Google Scholar] [CrossRef] [PubMed]
- Toyokawa, S.; Uddin, M.; Koenen, K.C.; Galea, S. How Does the Social Environment ‘Get into the Mind’? Epigenetics at the Intersection of Social and Psychiatric Epidemiology. Soc. Sci. Med. 2012, 74, 67–74. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Category | DSM-I | DSM-II | DSM-III | DSM-III-R | DSM-IV | DSM-5 |
|---|---|---|---|---|---|---|
| Terminology | Alcoholism; Drug Addiction | Alcoholism; Drug Dependence | Substance Use Disorders; Substance Abuse, Substance Dependence | Psychoactive Substance Use Disorders; Substance Dependence, Substance Abuse | Substance-Related Disorders; Substance Use Disorders, Substance Dependence and Substance Abuse | Substance-Related and Addictive Disorders a |
| Categorization | Sociopathic Personality Disturbance | Personality Disorder and Certain other Non-psychotic Mental Disorders | Classified Independently | Classified Independently | Classified Independently | Classified Independently |
| Role of Personality Disorders (PD) in relation to SUD | Primary. Alcoholism and drug addiction considered a “reaction” (secondary diagnosis) | Primary. Although Alcoholism is secondary, additional/separate diagnosis encouraged | Personality disturbance is listed as “Associated features” which are often present, and may be intensified by the SUD b | Personality disturbance is listed as “Associated features” which are often present, and may be intensified by the SUD c | Antisocial and Borderline PD are listed as “associated mental disorders” which are often co-morbid with and can complicate SUDs | SUDs are commonly seen in individuals with antisocial PDs which are associated with poorer prognosis |
| Main Sub-categories | Not applicable d | Excessive drinking (Episodic, Habitual) Alcohol addiction | Substance Abuse, Dependence | Psychoactive Substance Abuse, Dependence | Substance Abuse, Dependence | Substance Use Disorders with Severity/Specifiers |
| Course Specifiers | Not specified | Not specified | Continuous e, Episodic f, In remission g, Unspecified | Partial h and Full Remission i | Early Full Remission j; Early Partial Remission k; Sustained Full Remission l; Sustained Partial Remission m; On Agonist Therapy; In a Controlled Environment | Early remission n; Sustained remission o; On maintenance therapy; In a controlled environment |
| Severity Specifiers | Not specified | Not specified | Not specified | Mild, Moderate, Severe p | With, Without Physiological Dependence q | Mild, Moderate, Severe r |
| Duration | Not specified | Not specified | At least one month s | At least one month t | Within a 12-month period t | Within a 12-month period |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, S.M.; Adinoff, B. The Classification of Substance Use Disorders: Historical, Contextual, and Conceptual Considerations. Behav. Sci. 2016, 6, 18. https://doi.org/10.3390/bs6030018
Robinson SM, Adinoff B. The Classification of Substance Use Disorders: Historical, Contextual, and Conceptual Considerations. Behavioral Sciences. 2016; 6(3):18. https://doi.org/10.3390/bs6030018
Chicago/Turabian StyleRobinson, Sean M., and Bryon Adinoff. 2016. "The Classification of Substance Use Disorders: Historical, Contextual, and Conceptual Considerations" Behavioral Sciences 6, no. 3: 18. https://doi.org/10.3390/bs6030018