 Han Wu
Han Wu Zilong Lu2†
Zilong Lu2† Jing Wei
Jing Wei Xue Liu
Xue Liu- 1Department of Epidemiology, School of Public Health, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, China
- 2Shandong Center for Disease Control and Prevention, and Academy of Preventive Medicine, Shandong University, Jinan, China
- 3Department of Atmospheric and Oceanic Science, Earth System Science Interdisciplinary Center, University of Maryland, College Park, MD, United States
- 4Department of Nutrition and Food Hygiene, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, China
- 5Information and Data Analysis Lab, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, China
Background: Local governments in China took restrictive measures after the outbreak of COVID-19 to control its spread, which unintentionally resulted in reduced anthropogenic emission sources of air pollutants. In this study, we intended to examine the effects of the COVID-19 lockdown policy on the concentration levels of particulate matter with aerodynamic diameters of ≤1 μm (PM1), ≤2.5 μm (PM2.5), and ≤10 μm (PM10), nitrogen dioxide (NO2), sulfur dioxide (SO2), ozone (O3), and carbon monoxide (CO) and the potential subsequent reductions in the incidence of ischemic and hemorrhagic stroke in Shandong Province, China.
Methods: A difference-in-difference model combining the daily incidence data for ischemic and hemorrhagic stroke and air pollutant data in 126 counties was used to estimate the effect of the COVID-19 lockdown on the air pollutant levels and ischemic and hemorrhagic stroke incident counts. The avoided ischemic stroke cases related to the changes in air pollutant exposure levels were further estimated using concentration-response functions from previous studies.
Results: The PM1, PM2.5, PM10, NO2, and CO levels significantly decreased by −30.2, −20.9, −13.5, −46.3, and −13.1%, respectively. The O3 level increased by 11.5% during the lockdown compared with that in the counterfactual lockdown phase of the past 2 years. There was a significant reduction in population-weighted ischemic stroke cases (−15,315, 95% confidence interval [CI]: −27,689, −2,942), representing a reduction of 27.6% (95% CI: −49.9%, −5.3%). The change in the number of hemorrhagic stroke cases was not statistically significant. The total avoided PM1-, PM2.5-, PM10-, NO2-, and CO–related ischemic stroke cases were 739 (95% CI: 641, 833), 509 (95% CI: 440, 575), 355 (95% CI: 304, 405), 1,132 (95% CI: 1,024, 1,240), and 289 (95% CI: 236, 340), respectively.
Conclusion: The COVID-19 lockdown indirectly reduced the concentration levels of PM1, PM2.5, PM10, NO2, and CO and subsequently reduced the associated ischemic stroke incidence. The health benefits due to the lockdown are temporary, and long-term measures should be implemented to increase air quality and related health benefits in the post-COVID-19 period.
Introduction
COVID-19 broke out in China in December 2019. Within a few months, this disease spread around the world, becoming a global pandemic (1). The governments of most countries adopted lockdowns to retard the spread of COVID-19 (2). Chinese provincial governments took the Level I major public health emergency response action on 24 January 2020, and all cities implemented lockdowns. Thus, many industrial and human activities were restricted only to the essentials or a bare minimum (3–6).
Although the cost of implementing nationwide restrictions is undoubtedly enormous, the lockdowns contributed markedly to successfully controlling the spread of the pandemic. Moreover, they generated a range of unintended environmental and health benefits (7). Extensive studies have been conducted to evaluate the impacts of the COVID-19 lockdowns on air quality, as there were substantial reductions in the industrial and vehicle emissions of air pollutants due to the reduced anthropogenic sources (8–10). Most studies suggest that the lockdowns had positive effects on the improvement of regional air quality, especially in areas with severe air pollution (e.g., the Middle East, India, and China) (4, 9–12). Furthermore, some studies focused on the health benefits attributable to the COVID-19 lockdowns (13–18). For example, significant reductions in mortality and hospitalizations for cardiovascular diseases, such as atrial fibrillation, acute coronary syndrome, myocardial infarction, and ischemic stroke, were observed in both developed and developing countries (13–18).
In China, there were approximately 29 million prevalent stroke cases in 2019, and stroke has become the leading cause of death and disability-adjusted life-years (19). Accumulating evidence suggests that short-term exposure to air pollutants is associated with increased risks of stroke incidence and mortality (20). Therefore, the lowered air pollution levels due to the lockdowns may have reduced stroke-associated events. Several studies confirmed the causal effects of the COVID-19 lockdown on improved air quality and its subsequent health benefits. However, most of them focused on stroke mortality, and using mortality as the outcome of interest may underestimate the number of people affected by the lockdowns (3, 5, 17). In contrast, using stroke incidence as an outcome may greatly outnumber mortality events, and the estimated number of stroke incidence cases avoided because of the reduced air pollution levels due to the lockdowns may be greater than that of mortality, thus providing greater statistical power for examining the health benefits generated by the COVID-19 lockdowns.
To the best of our knowledge, no study has yet examined the reduction effect of the COVID-19 lockdowns on ischemic and hemorrhagic stroke incidence in China to date. In addition, most previous studies focused on the changes in commonly monitored air pollutants (i.e., PM2.5, PM10, SO2, NO2, O3, and CO), and only limited studies (from Croatia, France, India, Italy, and the western Mediterranean) examined the effect of the COVID-19 lockdowns on the PM1 level and relevant literature is scarce in China (21–25). In this study, we investigated the impacts of a COVID-19 lockdown on the concentrations of PM1 and other air pollutants (PM2.5, PM10, SO2, NO2, O3, and CO) and the potential subsequent reductions in ischemic and hemorrhagic stroke incidence in 126 counties in Shandong Province, China. We collected stroke incidence data from a stroke registry system, which covered all stroke case records from every medical institution (e.g., private clinics, community health service centers, and public hospitals) in the included counties.
Materials and Methods
Stroke Registry Data
Data on the county-specific daily incidence of stroke were obtained from the stroke registry system operated by the Shandong Center for Disease Control and Prevention (CDC). Patient admissions to all medical institutions with a stroke diagnosis in each county must be reported to this registry system. From 2017 to 2020, the system covered 126 of the 136 counties in Shandong, and the total population of these counties was 91 million, equivalent to 6.4% of the whole population of China.
In this stroke registry system, registry certificates were filled in by the attending physician who diagnoses patients according to their symptoms, inquiries, complaints, and medical inspection results. The diagnosis was then categorized according to the International Classification of Diseases version 10 (ICD-10). In addition, each patient was asked to report when clinical symptoms occurred, which was then recorded as the incidence date. Then, the registry certificates were reported to the registry system in real-time. The information on each certificate was validated by professionals in the CDC of each county within 7 days, who also checked for completeness and coding. In this study, we focused on ischemic stroke (ICD-10 code: I63) and hemorrhagic stroke (ICD-10 codes: I60-I61). Ethical approval was obtained from the Ethics Review Committee of Public Health, Shandong University (No. LL20211203).
Air Pollution Data
Daily ambient PM1, PM2.5, PM10, NO2, SO2, O3, and CO data were collected from ChinaHighAirPollutants (CHAP, available at https://weijing-rs.github.io/product.html) datasets for Shandong province from 2017 to 2020 at a spatial resolution of 0.1° (≈10 km). These data were estimated using a developed space-time extremely randomized trees model, which integrates satellite remote sensing products, atmospheric reanalysis, and ground-based measurements to accomplish model simulations (26–32). The data on the predicted air pollutants levels were compared validly with ground-level measurements. The cross-validation coefficients of determination (CV-R2) were 0.82, 0.91, 0.86, 0.84, 0.84, 0.87, and 0.80, and the root-mean-square errors (RMSEs) were 10.86, 12.67, 24.34, 7.99, 10.07, 17.10, and 0.29 mg/m3 for daily concentrations of PM1, PM2.5, PM10, NO2, SO2, O3, and CO, respectively. The CHAP datasets have been widely applied in recent epidemiological studies evaluating the impact of exposure to ambient air pollutants on population health in China (33–35). For our analysis, the daily mean concentrations of PM1, PM2.5, PM10, NO2, SO2, O3, and CO for each county were estimated by calculating the average of the pixel values weighted by the proportion of the area of the county covered by the pixel, which enhanced the spatial representativeness of air pollution for each county.
Statistical Analysis
In this study, we first calculated the changes in the levels of each air pollutant and the ischemic and hemorrhagic stroke counts. Then, we calculated the estimated avoided stroke incident cases attributable to these air pollution changes by county. We employed a quasi-experiment design and used a difference-in-difference (DID) approach to estimate the effect of the COVID-19 lockdown on air pollutant levels (PM1, PM2.5, PM10, SO2, NO2, O3, and CO) and ischemic and hemorrhagic stroke incident counts. Using this approach, we compared the same period in the past 2 years before the COVID-19 lockdown with a certain period in the year of the lockdown. Then, the net treatment effect of the lockdown on the air pollutant levels and stroke incident counts can be estimated. The detailed procedure is illustrated in Figure 1.
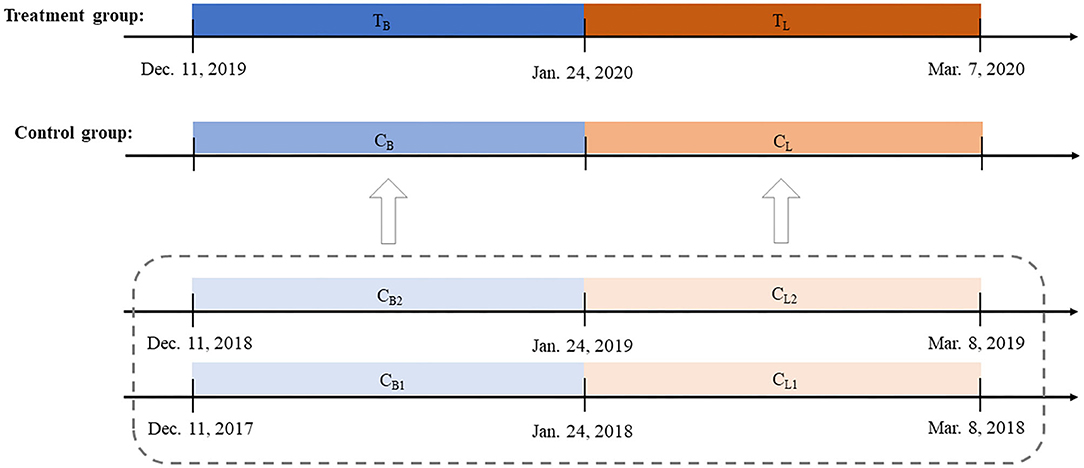
Figure 1. Settings of the difference-in-difference (DID) model.
The government of Shandong province announced the Level I major public health emergency response on 24 January and lifted the Level I response on 7 March. In this context, the lockdown phase was defined as the period between 24 January and 7 March, which lasted for a sum of 44 days. We set the period between 11 December 2019, and 23 January 2020, as the baseline phase to make the time length of the baseline phase equal to that of the lockdown phase. Then, we created a DID model to quantify the change level of each air pollutant for each county. Taking PM1 as an example, we first selected four corresponding phases (CB1, CL1, CB2, and CL2) from 2017 to 2019, with CB1 denoting the mean daily PM1 concentration level from 11 December 2017 to 23 January 2018, CL1 the mean daily PM1 concentration level from 24 January 2018 to 8 March 2018, CB2 the mean daily PM1 concentration level from 11 December 2018 to 23 January 2019, and CL2 the mean daily PM1 concentration level from 24 January 2019 to 8 March 2019. Next, the means of CB1 and CB2 (i.e., CB) and CL1 and CL2 (i.e., CL) were calculated to form a PM1 concentration at the baseline and lockdown phases, respectively, as the counterfactual control groups. Then, we calculated the difference in the PM1 concentration levels of the treatment group and the control group during the lockdown phase (TL – CL) and the difference between the two groups during the baseline phase (TB – CB). The changes in the PM1 concentration level for each county related to the lockdown policy beyond background trends can be estimated using the above two differences: (TL – CL) – (TB – CB).
Three key assumptions of DID should be satisfied (36). First, the event shock should be completely exogenous. In this study, the COVID-19 lockdown in Shandong province is used as a quasi-experiment, and no one could have predicted the COVID-19 outbreak or the unprecedented nationwide lockdown in late 2019, which can be regarded as a “black swan.” Thus, the DID model used in this study meets the exogeneity assumption. Second, the exogenous shock should affect only the treatment units and not the potential control units. In this study, the 44 days before and after the day of the announcement of the lockdown policy (24 January 2020) were selected as the treatment group, and the same period in the past 2 years was selected as the control group. The COVID-19 outbreak in 2020 cannot affect the air quality levels in 2018 or 2019. Third, the outcome of interest between the treatment and control groups must have similar fits before the exogenous event occurs, otherwise known as the parallel trend assumption. If this assumption is satisfied, we can reasonably assume that the parallel trends of air pollutant concentrations over time would be the same for both groups. This assumption was examined using a regression model, which included the interaction term between time and the baseline period (18). We found that the coefficient for the interaction term is not statistically significant for each of the outcomes, indicating the parallel trend assumption for the DID model is plausible (Supplementary Table 1) (18).
Our preliminary analyses showed a statistically significant change in ischemic stroke cases. Thus, the following formula was used to estimate the counts of the avoided ischemic stroke cases related to changes in the air pollutant exposure levels, which was adopted from recent studies evaluating the impact of ambient air pollutants exposure on population health (3, 37, 38):
ΔCm indicates the avoided ischemic stroke incident cases for county m, Bm is the baseline counts (i.e., the average of the counts from 24 January to 7 March in 2018 and 2019) for ischemic stroke for county m, β represents the exposure-response effect estimates extracted from two previous studies (Supplementary Table 2) (39, 40), and Δapm is the change in one specific air pollutant for county m.
All the above analyses were weighted by the population in each county. We conducted a sensitivity analysis by estimating the change of the sex- and age-adjusted incidence rates of ischemic stroke and hemorrhagic stroke during the lockdown phase in the DID model to further check the robustness of using the incident count of stroke as the outcome. The sex- and age-adjusted incidence rates were calculated using the population data for each county, which were collected from China's 2010 census survey.
The statistical analysis was carried out using R 4.0.3 (The R Project for Statistical Computing, Vienna, Austria), and two-sided values of p < 0.05 were considered statistically significant.
Result
During the lockdown phase in 2020, the mean [standard deviation (SD)] population-weighted PM1, PM2.5, PM10, NO2, SO2, O3, and CO concentration levels were 45.1 (7.6) μg/m3, 58.5 (8.9) μg/m3, 79.5 (10.0) μg/m3, 23.9 (3.0) μg/m3, 13.9 (2.5) μg/m3, 83.6 (3.5) μg/m3, and 0.95 (0.07) mg/m3, respectively, and the total ischemic and hemorrhagic stroke cases were 44,043 and 9,434, respectively (Table 1).
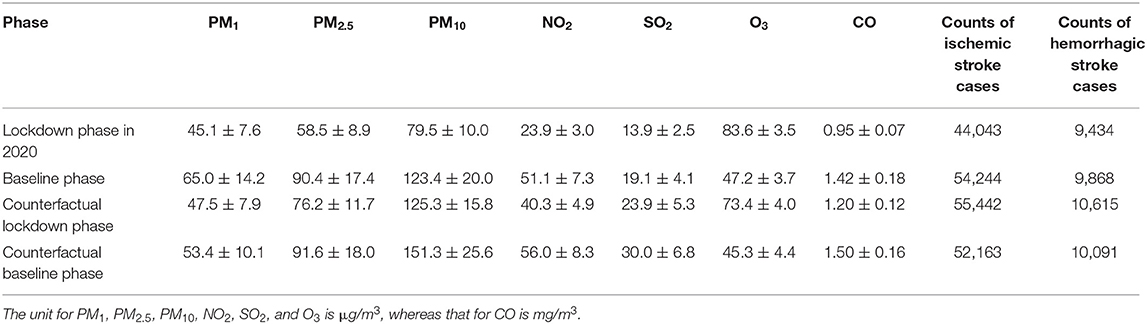
Table 1. Means and standard deviations (SD) for air pollutant concentration levels and counts of stroke cases for the four phases.
Figure 2 shows the changes in population-weighted average air pollutant levels and stroke cases between the lockdown phase in 2020 and the counterfactual lockdown phase of the past 2 years for each county using the DID model. All 126 counties (100.0%) showed reductions in PM1 and NO2 levels, 122 counties (96.8%) showed reductions in PM2.5 level, 120 counties (95.2%) showed reductions in PM10 level, 110 counties (87.3%) showed reductions in CO levels, while 94 counties (74.6%) showed increases in SO2 levels, and 123 counties (97.6%) showed increases in O3 levels. The average changes in the population-weighted PM1, PM2.5, PM10, NO2, O3, and CO levels across the 126 counties were statistically significant (Table 2), and the respective estimates were −14.3 (95% confidence interval [CI]: −17.9, −10.8) μg/m3, −15.9 (95% CI: −20.5, −11.4) μg/m3, −16.9 (95% CI: −22.8, −11.0) μg/m3, −11.1 (95% CI: −13.1, −9.0) μg/m3, 8.4 (95% CI: 7.0, 9.9) mg/m3, and −0.16 (95% CI: −0.20, −0.11) μg/m3, representing a change of −30.2% (95% CI: −37.6%, −22.8%), −20.9% (95% CI: −26.9%, −15.0%), −13.5% (95% CI: −18.2%, −8.8%), −46.3% (95% CI: −54.7%, −37.8%), 11.5% (95% CI: 9.5%, 13.4%), and −13.1% (95% CI: −17.0%, −9.3%) relative to the counterfactual lockdown phase of the past 2 years, respectively. The average change in the SO2 level was 0.9 (95% CI: −1.0, 2.9) μg/m3, corresponding to a change of 2.3% (95% CI: −2.5%, 7.1%), which was not statistically significant.
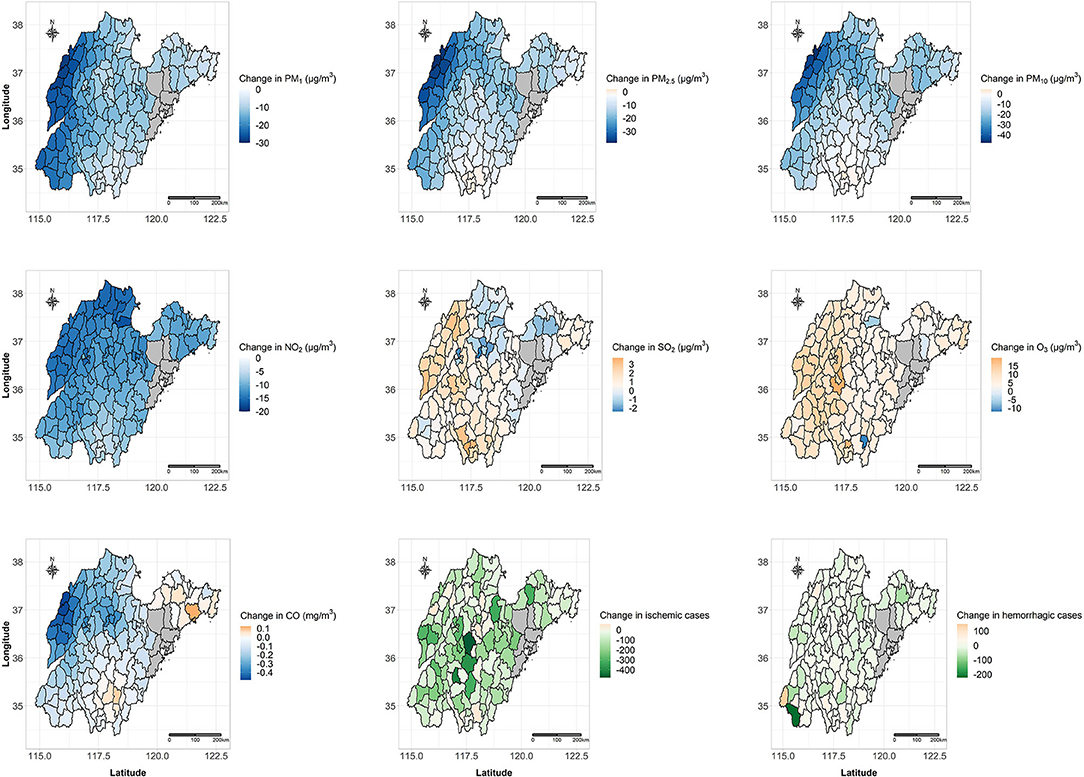
Figure 2. Changes in population-weighted average air pollutant levels and stroke cases between the lockdown phase in 2020 and the counterfactual lockdown phase of the past 2 years for each of the 126 included counties using the DID model.
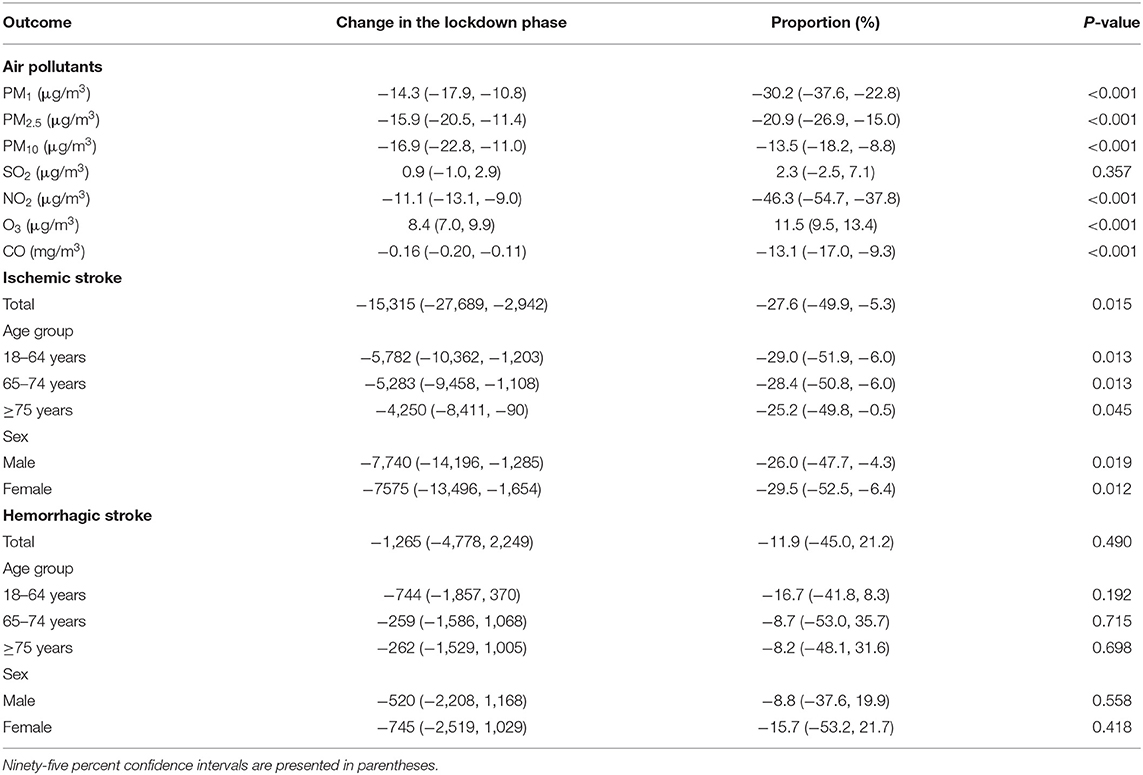
Table 2. Changes in average air pollutant concentration levels and total counts of stroke cases in the lockdown phase relative to the counterfactual lockdown phase of the past 2 years.
In total, 110 counties (87.3%) showed a reduction in ischemic stroke cases, whereas 80 counties (63.5%) showed a reduction in hemorrhagic stroke cases. The population-weighted ischemic stroke cases were significantly reduced across the 126 counties (−15,315, 95% CI: −27,689, −2,942), representing a 27.6% reduction (95% CI: −49.9%, −5.3%) compared with that of the counterfactual lockdown phase. Furthermore, the reductions in the population-weighted ischemic stroke cases in both male and female subgroups, and all three age subgroups (18–64, 65–74, and ≥75 years) were also statistically significant. The total change in the hemorrhagic stroke cases was −1,265 (95% CI: −4,778, 2,249), which was not statistically significant. In addition, the changes in the hemorrhagic stroke cases were also not statistically significant in the sex or age subgroups. The sensitivity analysis revealed similar results, showing that the sex- and age-adjusted incidence rate for ischemic stroke decreased by 144 per 100,000 (95% CI: −257, −30, p = 0.013), and the sex- and age-adjusted incidence rate for hemorrhagic stroke increased by 5 per 100,000 (95% CI: −22, 32, P=0.730) during the lockdown for each county.
Since there were no statistically significant changes in the SO2 level and hemorrhagic stroke cases, we estimated the changes in the ischemic stroke cases attributed to the changes in the PM1, PM2.5, PM10, NO2, CO, and O3 levels across the 126 counties using the concentration–response function from previous studies (Table 3). The total avoided PM1-, PM2.5-, PM10-, NO2-, and CO–related ischemic stroke cases were 739 (95% CI: 641, 833), 509 (95% CI: 440, 575), 355 (95% CI: 304, 405), 1,132 (95% CI: 1,024, 1,240), and 289 (95% CI: 236, 340), respectively. The corresponding percentages of the avoided ischemic stroke cases were 4.8% (95% CI: 4.2%, 5.4%), 3.3% (95% CI: 2.9%, 3.8%), 2.3% (95% CI: 2.0%, 2.6%), 7.4% (95% CI: 6.7%, 8.1%), and 1.9% (95% CI: 1.5%, 2.2%), respectively. The increased O3 concentration levels across the 126 counties during the lockdown phase led to the increased counts of O3-related ischemic stroke cases at 48 (95% CI: 41, 54), corresponding to an increase of 0.3% (95% CI: 0.3%, 0.4%).
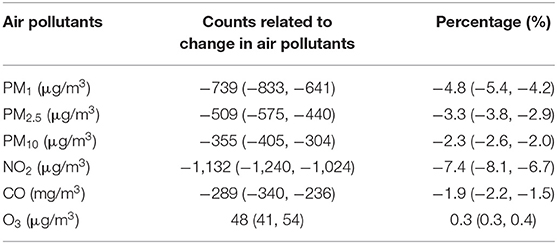
Table 3. Estimated counts of ischemic stroke cases related to the change in air pollutants in the lockdown phase relative to the counterfactual lockdown phase of the past 2 years.
Discussion
With the spread of COVID-19 worldwide, varying degrees of lockdown policies were implemented by the government to control this pandemic in most countries, and almost all aspects of life were affected during this period (2). The government of Shandong province imposed strict restrictions to lower the intensity of population outdoor activities (e.g., industry, traffic, construction, and entertainment), and the whole province was thrown into an unprecedented state of shutdown for about 6 weeks. This pandemic allowed us to estimate the changes in air pollutants and stroke cases relative to those during the same period in previous years using a quasi-experiment design.
The DID model indicated that if no lockdown occurred, the average concentrations of PM1, PM2.5, PM10, NO2, and CO across the 126 counties would increase by 30.2, 20.9, 13.5, 46.3, and 13.1%, respectively, whereas the average concentration of O3 would decrease by 11.5%. Most previous studies focused on the changes in commonly monitored air pollutants, and no study has quantified the change in PM1 levels during the lockdown in China (21–25). Our findings added to the growing literature evaluating the role of the COVID-19 lockdowns on ambient particulate matter, as we found substantial reductions in PM1, PM2.5, and PM10 levels during the COVID-19 lockdown phase. Moreover, the PM1 concentration level seemed to decrease more precipitously than those of PM2.5 and PM10. The detailed reason for the heterogeneity of the reduction effect of the lockdown on the particulate matter of different sizes is unclear and requires further exploration in future studies.
For other gaseous air pollutants, many studies from China and other countries (e.g., France, India, Italy, and Mexico) also found that the concentration of NO2 showed the most significant decrease and that of O3 showed an increase during the lockdowns (6, 12, 22, 23, 41, 42). A previous study based on 597 major cities worldwide reported similar findings (43). As nitrogen oxide is mainly related to emissions from motor vehicles, the remarkable reduction in the NO2 level may be due to the restriction of human traffic activities during the lockdowns (12, 42). Then, the reductions in the nitrogen oxide emissions because of the depressed anthropogenic activities may explain the observed increases in O3 during the lockdowns, as the drop in nitric oxide (NO) may slow down its interaction with O3 (NO + O3 = NO2 + O2). Thus, the O3 concentration may increase (7, 42).
Our results indicated that the COVID-19 lockdown did not result in significant changes in SO2 concentrations, which was consistent with several previous studies in northern and eastern China (44, 45). However, some studies also suggested that the levels of SO2 significantly decreased during the lockdowns in other regions of China (3, 6, 11). A possible interpretation for the limited influence of the lockdown on the SO2 levels in this area is that the additional emissions from coal-burning for residential heating because of the people staying at home during the relatively cold season may counterbalance the reduction in other emissions, such as those from factories (44, 45).
Several studies suggested significant drops in mortality or hospital admissions during the COVID-19 lockdowns, but only limited studies used stroke-related events as the outcome of interest (17, 46–48). For instance, in France, a significant drop in hospitalization related to stroke was observed only in the area most affected by COVID-19 compared with those in previous years. In contrast, no significant change in hospitalization for stroke was observed in the least affected area (17). Another study collected data from a hospital in Spain and reported that relative to March 2019, the number of stroke admissions declined by about 23% in March 2020 (46). Similarly, Zhao et al. reported that hospital admissions for stroke reduced by ~40% in February 2020 compared with that in the same period in 2019 in 227 hospitals across China (47). Kansagra et al. used the number of patients with stroke who underwent imaging as a surrogate for the number of cases of acute ischemic stroke in more than 800 hospitals in the United States, and they found that the number decreased by 39% during the early days of the pandemic (48). In this study, we estimated that the lockdown resulted in a drop of 27.6% in ischemic stroke cases compared with average values for the same periods of the previous 2 years. The reductions in PM1, PM2.5, PM10, NO2, and CO concentrations could have prevented as many as 4.8, 3.3, 2.3, 7.4, and 1.9% of the total ischemic stroke cases, respectively. The count of hemorrhagic stroke cases fell by a much smaller number (n = −1,265), which was not statistically significant. This finding is partly in line with previous studies indicating that exposure to air pollutants may exclusively increase ischemic stroke risks and not those of hemorrhagic stroke (20).
We noticed that not all avoided ischemic stroke cases could be attributed to the improved air quality during the COVID-19 lockdowns. Several other potential reasons may contribute to the observed decrease in the counts of ischemic stroke cases. First, the chance of family members and friends recognizing that a patient was having stroke symptoms may have been decreased because of the increased social isolation due to the lockdown (47). Second, most hospitals canceled their courses on stroke awareness education because of the imposition of social distancing (47). Third, patients with suspected acute stroke may have been worried about being infected with COVID-19 at hospitals (17). Fourth, some patients with severe stroke might have died at home (17). Fifth, evidence from other countries suggests that the reduced capacity of emergency services due to the burden of patients with COVID-19 may have limited the number of patients with stroke seeking essential medical services (49). However, only a total of no more than 800 COVID-19 cases were diagnosed across Shandong province during the lockdown, and this has limited influence on hospitals providing medical services for patients with stroke (50). Moreover, a recent study revealed that the onset-to-door time became even shorter during the lockdowns in Beijing, China, which might have benefited from the better traffic situation (51).
Our results imply that substantial health benefits could be achieved if stringent and effective control measures are implemented to tackle air pollution. Lockdowns are not appropriate for improving air quality in the long run, and persistent efforts are needed to reduce air pollution through a series of abatement measures for anthropogenic emissions (52). For example, policymakers could consider comprehensive strategies to upgrade local power and steel industries, provide more subsidies for public or electric transportation, and encourage households to transition from coal to cleaner energy sources (such as gas and electricity) (4).
Our study has several limitations. First, this is a quasi-experiment based on stroke count data at the population level. Thus, confounding factors at the individual level (e.g., tobacco smoking, hypertension, physical activity, and diet) (19, 53) could not be fully excluded, although the reductions in ischemic stroke cases were significant in all sex and age subgroups. However, we expect that the individual changes in the confounding factors did not cause substantial bias in the relation between the lockdown and stroke incidence at a population level (52). Second, the avoided ischemic stroke cases attributed to the changes in the air pollutant concentration levels were estimated using single-pollutant models. The strong correlation between the included air pollutants and the absence of epidemiological dose-response functions that account for the full suite of pollutants did not allow us to estimate the independent effect of each air pollutant. Therefore, some avoided stroke cases might have been counted more than once (52). Third, the method we used could not rule out the influence of meteorological conditions (e.g., air pressure, temperature, and wind field) on air pollutant concentration levels and the effect of extreme cold temperature on ischemic stroke incidence (54). However, a previous study suggested that the adjustment of meteorological variables had little effect on the estimated changes in air pollutant concentration levels during the lockdown in China (7). In addition, all people had to stay at home during the lockdown. Thus, we anticipate that the outdoor extreme cold temperature had a limited influence on the ischemic stroke incidence. Fourth, household air pollution (HAP) is also a risk factor for ischemic stroke (55), and the exposure level of HAP might be increased as most residents had to stay at home for longer durations during the lockdown (56). However, the additional counts of ischemic stroke resulting from HAP could not be estimated because of the lack of relevant data.
Conclusion
The life-changing restrictions during the COVID-19 lockdown indirectly reduced the concentration levels of air pollutants (PM1, PM2.5, PM10, NO2, and CO) and subsequently reduced the associated ischemic stroke incidence. However, the health benefits brought by the lockdown are temporary, and long-term measures should be implemented to decrease air pollution levels and related health loss in the post-COVID-19 period.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Review Committee of Public Health, Shandong University. The Ethics Committee waived the requirement of written informed consent for participation.
Author Contributions
HW: formal analysis, methodology, visualization, and writing the original draft. ZL and BZ: investigation, data curation, writing, reviewing, and editing. JW: methodology, resources, data curation, writing, reviewing, and editing. XL: validation, writing, reviewing, and editing. MZ: formal analysis, validation, and writing the original draft. WL: software, writing, reviewing, and editing. XG: supervision, resources, writing, reviewing, and editing. BX: conceptualization, supervision, funding acquisition, writing, reviewing, and editing. All authors contributed to the article and approved the submitted version.
Funding
Funding was received from the National Important Project of the Ministry of Science and Technology in China (2017YFC1501404) and the Innovation Team of Climbing Program of Shandong University and the Youth Team of Humanistic and Social Science of Shandong University (20820IFYT1902).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.876615/full#supplementary-material
References
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. (2020) 382:727–33. doi: 10.1056/NEJMoa2001017
2. Zhang H, Lin Y, Wei S, Loo BPY, Lai PC, Lam YF, et al. Global association between satellite-derived nitrogen dioxide (NO(2)) and lockdown policies under the COVID-19 pandemic. Sci Total Environ. (2021) 761:144148. doi: 10.1016/j.scitotenv.2020.144148
3. Yumin L, Shiyuan L, Ling H, Ziyi L, Yonghui Z, Li L, et al. The casual effects of COVID-19 lockdown on air quality and short-term health impacts in China. Environ Pollut. (2021) 290:117988. doi: 10.1016/j.envpol.2021.117988
4. Chen G, Tao J, Wang J, Dong M, Li X, Sun X, et al. Reduction of air pollutants and associated mortality during and after the COVID-19 lockdown in China: impacts and implications. Environ Res. (2021) 200:111457. doi: 10.1016/j.envres.2021.111457
5. Giani P, Castruccio S, Anav A, Howard D, Hu W, Crippa P. Short-term and long-term health impacts of air pollution reductions from COVID-19 lockdowns in China and Europe: a modelling study. Lancet Planet Health. (2020) 4:e474–82. doi: 10.1016/S2542-5196(20)30224-2
6. Li L, Li Q, Huang L, Wang Q, Zhu A, Xu J, et al. Air quality changes during the COVID-19 lockdown over the Yangtze River Delta Region: an insight into the impact of human activity pattern changes on air pollution variation. Sci Total Environ. (2020) 732:139282. doi: 10.1016/j.scitotenv.2020.139282
7. He GJ, Pan YH, Tanaka T. The short-term impacts of COVID-19 lockdown on urban air pollution in China. Nat Sustain. (2020) 3:1005–11. doi: 10.1038/s41893-020-0581-y
8. Potts DA, Marais EA, Boesch H, Pope RJ, Lee J, Drysdale W, et al. Diagnosing air quality changes in the UK during the COVID-19 lockdown using TROPOMI and GEOS-Chem. Environ Res Lett. (2021) 16:054031. doi: 10.1088/1748-9326/abde5d
9. El Kenawy AM, Lopez-Moreno JI, McCabe MF, Domínguez-Castro F, Peña-Angulo D, Gaber IM, et al. The impact of COVID-19 lockdowns on surface urban heat island changes and air-quality improvements across 21 major cities in the Middle East. Environ Pollut. (2021) 288:117802. doi: 10.1016/j.envpol.2021.117802
10. Shukla S, Khan R, Saxena A, Sekar S, Ali EF, Shaheen SM. Appraisal of COVID-19 lockdown and unlocking effects on the air quality of North India. Environ Res. (2022) 204:112107. doi: 10.1016/j.envres.2021.112107
11. Wang M, Liu F, Zheng M. Air quality improvement from COVID-19 lockdown: evidence from China. Air Qual Atmos Health. (2020) 14:591–604. doi: 10.1007/s11869-020-00963-y
12. Nie D, Shen F, Wang J, Ma X, Li Z, Ge P, et al. Changes of air quality and its associated health and economic burden in 31 provincial capital cities in China during COVID-19 pandemic. Atmos Res. (2021) 249:105328. doi: 10.1016/j.atmosres.2020.105328
13. Wu Y, Li H, Xu D, Li H, Chen Z, Cheng Y, et al. Associations of fine particulate matter and its constituents with airway inflammation, lung function, and buccal mucosa microbiota in children. Sci Total Environ. (2021) 773:145619. doi: 10.1016/j.scitotenv.2021.145619
14. Tsigkas G, Koufou EE, Katsanos K, Patrinos P, Moulias A, Miliordos I, et al. Potential relationship between lifestyle changes and incidence of hospital admissions for acute coronary syndrome during the COVID-19 lockdown. Front Cardiovasc Med. (2021) 8:604374. doi: 10.3389/fcvm.2021.604374
15. Holt A, Gislason GH, Schou M, Zareini B, Biering-Sørensen T, Phelps M, et al. New-onset atrial fibrillation: incidence, characteristics, and related events following a national COVID-19 lockdown of 5.6 million people. Eur Heart J. (2020) 41:3072–9. doi: 10.1093/eurheartj/ehaa494
16. Candelaresi P, Manzo V, Servillo G, Muto M, Barone P, Napoletano R, et al. The impact of Covid-19 lockdown on stroke admissions and treatments in campania. J Stroke Cerebrovasc Dis. (2021) 30:105448. doi: 10.1016/j.jstrokecerebrovasdis.2020.105448
17. Mariet AS, Giroud M, Benzenine E, Cottenet J, Roussot A, Aho-Glélé LS, et al. Hospitalizations for stroke in france during the COVID-19 pandemic before, during, and after the national lockdown. Stroke. (2021) 52:1362–9. doi: 10.1161/STROKEAHA.120.032312
18. Son JY, Fong KC, Heo S, Kim H, Lim CC, Bell ML. Reductions in mortality resulting from reduced air pollution levels due to COVID-19 mitigation measures. Sci Total Environ. (2020) 744:141012. doi: 10.1016/j.scitotenv.2020.141012
19. Ma Q, Li R, Wang L, Yin P, Wang Y, Yan C, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990-2019: an analysis for the global burden of disease study 2019. Lancet Public Health. (2021) 6:e897–906. doi: 10.1016/S2468-2667(21)00228-0
20. Verhoeven JI, Allach Y, Vaartjes ICH, Klijn CJM, de Leeuw FE. Ambient air pollution and the risk of ischaemic and haemorrhagic stroke. Lancet Planet Health. (2021) 5:e542–52. doi: 10.1016/S2542-5196(21)00145-5
21. Jakovljević I, Štrukil ZS, Godec R, Davila S, Pehnec G. Influence of lockdown caused by the COVID-19 pandemic on air pollution and carcinogenic content of particulate matter observed in Croatia. Air Qual Atmos Health. (2021) 14:467–72. doi: 10.1007/s11869-020-00950-3
22. Sannino A, D'Emilio M, Castellano P, Amoruso S, Boselli A. Analysis of air quality during the COVID-19 pandemic lockdown in Naples (Italy). Aerosol Air Quality Res. (2021) 21:200381. doi: 10.4209/aaqr.2020.07.0381
23. Petit JE, Dupont JC, Favez O, Gros V, Zhang YJ, Sciare J, et al. Response of atmospheric composition to COVID-19 lockdown measures during spring in the Paris region (France). Atmospheric Chem Phy. (2021) 21:17167–83. doi: 10.5194/acp-21-17167-2021
24. Clemente Á, Yubero E, Nicolás JF, Caballero S, Crespo J, Galindo N. Changes in the concentration and composition of urban aerosols during the COVID-19 lockdown. Environ Res. (2022) 203:111788. doi: 10.1016/j.envres.2021.111788
25. Jain CD, Madhavan BL, Singh V, Prasad P, Sai Krishnaveni A, Ravi Kiran V, et al. Phase-wise analysis of the COVID-19 lockdown impact on aerosol, radiation and trace gases and associated chemistry in a tropical rural environment. Environ Res. (2021) 194:110665. doi: 10.1016/j.envres.2020.110665
26. Wei J, Li Z, Guo J, Sun L, Huang W, Xue W, et al. Satellite-Derived 1-km-Resolution PM1 Concentrations from 2014 to 2018 across China. Environ Sci Technol. (2019) 53:13265–74. doi: 10.1021/acs.est.9b03258
27. Wei J, Li Z, Xue W, Sun L, Fan T, Liu L, et al. The ChinaHighPM(10) dataset: generation, validation, and spatiotemporal variations from 2015 to 2019 across China. Environ Int. (2021) 146:106290. doi: 10.1016/j.envint.2020.106290
28. Wei J, Li Z, Lyapustin A, Sun L, Peng Y, Xue W, et al. Reconstructing 1-km-resolution high-quality PM2.5 data records from 2000 to 2018 in China: spatiotemporal variations and policy implications. Remote Sens Environ. (2021) 252:112136. doi: 10.1016/j.rse.2020.112136
29. Wei J, Li Z, Li K, Dickerson RR, Pinker RT, Wang J, et al. Full-coverage mapping and spatiotemporal variations of ground-level ozone (O3) pollution from 2013 to. across China. Remote Sens Environ. (2020) 2022:112775. doi: 10.1016/j.rse.2021.112775
30. Wei J. ChinaHighSO2: Big Data Seamless 10 km Ground-Level SO2 Dataset for China (Version 1). Zenodo (2021). doi: 10.5281/zenodo.4641538
31. Wei J LZ. ChinaHighNO2: Big Data Seamless 10 km Ground-Level NO2 Dataset for China (Version 1). Zenodo (2021). doi: 10.5281/zenodo.4641542
32. Wei J. ChinaHighCO: Big Data Seamless 10 km Ground-Level CO dataset for China (Version 1). Zenodo (2021). doi: 10.5281/zenodo.4641530 (accessed January 1, 2022).
33. Liu M, Tang W, Zhang Y, Wang Y, Kangzhuo B, Li Y, et al. Urban-rural differences in the association between long-term exposure to ambient air pollution and obesity in China. Environ Res. (2021) 201:111597. doi: 10.1016/j.envres.2021.111597
34. Wang L, Chen G, Pan Y, Xia J, Chen L, Zhang X, et al. Association of long-term exposure to ambient air pollutants with blood lipids in Chinese adults: The China Multi-Ethnic Cohort study. Environ Res. 2021; 197. doi: 10.1016/j.envres.2021.111174
35. Xu J, Zhou J, Luo P, Mao D, Xu W, Nima Q, et al. Associations of long-term exposure to ambient air pollution and physical activity with insomnia in Chinese adults. Sci Total Environ. (2021) 792:148197. doi: 10.1016/j.scitotenv.2021.148197
36. Ming W, Zhou ZQ, Ai HS, Bi HM, Zhong Y. COVID-19 and air quality: evidence from China. Emerg Mark Finance Trade. (2020) 56:2422–42. doi: 10.1080/1540496X.2020.1790353
37. Wang Q, Wang J, Zhou J, Ban J, Li T. Estimation of PM(2·5)-associated disease burden in China in 2020 and 2030 using population and air quality scenarios: a modelling study. Lancet Planet Health. (2019) 3:e71–80. doi: 10.1016/S2542-5196(18)30277-8
38. Li Y, Liao Q, Zhao X, Tao Y, Bai Y, Peng L. Premature mortality attributable to PM(2.5) pollution in China during 2008-2016: underlying causes and responses to emission reductions. Chemosphere. (2021) 263:127925. doi: 10.1016/j.chemosphere.2020.127925
39. Chen L, Zhang Y, Zhang W, Chen G, Lu P, Guo Y, et al. Short-term effect of PM(1) on hospital admission for ischemic stroke: a multi-city case-crossover study in China. Environ Pollut. (2020) 260:113776. doi: 10.1016/j.envpol.2019.113776
40. Tian Y, Liu H, Zhao Z, Xiang X, Li M, Juan J, et al. Association between ambient air pollution and daily hospital admissions for ischemic stroke: a nationwide time-series analysis. PLoS Med. (2018) 15:e1002668. doi: 10.1371/journal.pmed.1002668
41. Markandeya, Verma PK, Mishra V, Singh NK, Shukla SP, Mohan D. Spatio-temporal assessment of ambient air quality, their health effects and improvement during COVID-19 lockdown in one of the most polluted cities of India. Environ Sci Pollut Res Int. (2021) 28:10536–51. doi: 10.1007/s11356-020-11248-3
42. Hernández-Paniagua IY, Valdez SI, Almanza V, Rivera-Cárdenas C, Grutter M, Stremme W, et al. Impact of the COVID-19 lockdown on air quality and resulting public health benefits in the Mexico City metropolitan area. Front Public Health. (2021) 9:642630. doi: 10.3389/fpubh.2021.642630
43. Liu F, Wang M, Zheng M. Effects of COVID-19 lockdown on global air quality and health. Sci Total Environ. (2021) 755:142533. doi: 10.1016/j.scitotenv.2020.142533
44. Shi X, Brasseur GP. The response in air quality to the reduction of chinese economic activities during the COVID-19 outbreak. Geophys Res Lett. (2020) 47:e2020GL088070. doi: 10.1029/2020GL088070
45. Filonchyk M, Hurynovich V, Yan HW, Gusev A, Shpilevskaya N. Impact assessment of COVID-19 on variations of SO2, NO2, CO and AOD over East China. Aerosol Air Quality Res. (2020) 20:1530–40. doi: 10.4209/aaqr.2020.05.0226
46. Rudilosso S, Laredo C, Vera V, Vargas M, Renú A, Llull L, et al. Acute stroke care is at risk in the era of COVID-19: experience at a comprehensive stroke center in Barcelona. Stroke. (2020) 51:1991–5. doi: 10.1161/STROKEAHA.120.030329
47. Zhao J, Li H, Kung D, Fisher M, Shen Y, Liu R. Impact of the COVID-19 Epidemic on stroke care and potential solutions. Stroke. (2020) 51:1996–2001. doi: 10.1161/STROKEAHA.120.030225
48. Kansagra AP, Goyal MS, Hamilton S, Albers GW. Collateral effect of Covid-19 on stroke evaluation in the United States. N Engl J Med. (2020) 383:400–1. doi: 10.1056/NEJMc2014816
49. Bersano A, Kraemer M, Touzé E, Weber R, Alamowitch S, Sibon I, et al. Stroke care during the COVID-19 pandemic: experience from three large European countries. Eur J Neurol. (2020) 27:1794–800. doi: 10.1111/ene.14375
50. The People's Government of Shandong Province. Epidemic Situation of COVID-19 in Shandong Province From 12:00 to 24:00 on March 7, 2020. Available online at: http://www.shandong.gov.cn/art/2020/3/8/art_94238_8887882.html (accessed March 31, 2022).
51. Wu Y, Chen F, Wang Z, Feng W, Liu Y, Wang Y, et al. Reductions in hospital admissions and delays in acute stroke care during the pandemic of COVID-19. Front Neurol. (2020) 11:584734. doi: 10.3389/fneur.2020.584734
52. Ye T, Guo S, Xie Y, Chen Z, Abramson MJ, Heyworth J, et al. Health and related economic benefits associated with reduction in air pollution during COVID-19 outbreak in 367 cities in China. Ecotoxicol Environ Saf. (2021) 222:112481. doi: 10.1016/j.ecoenv.2021.112481
53. Qi M, Li P, Moyle W, Weeks B, Jones C. Physical activity, health-related quality of life, and stress among the chinese adult population during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:6494. doi: 10.3390/ijerph17186494
54. Luo Y, Li H, Huang F, Van Halm-Lutterodt N, Qin X, Wang A, et al. The cold effect of ambient temperature on ischemic and hemorrhagic stroke hospital admissions: a large database study in Beijing, China between years 2013 and 2014-utilizing a distributed lag non-linear analysis. Environ Pollut. (2018) 232:90–6. doi: 10.1016/j.envpol.2017.09.021
55. Lu H, Tan Z, Liu Z, Wang L, Wang Y, Suo C, et al. Spatiotemporal trends in stroke burden and mortality attributable to household air pollution from solid fuels in 204 countries and territories from 1990 to 2019. Sci Total Environ. (2021) 775:145839. doi: 10.1016/j.scitotenv.2021.145839
Keywords: lockdown, air pollution, ischemic stroke, COVID-19, incidence
Citation: Wu H, Lu Z, Wei J, Zhang B, Liu X, Zhao M, Liu W, Guo X and Xi B (2022) Effects of the COVID-19 Lockdown on Air Pollutant Levels and Associated Reductions in Ischemic Stroke Incidence in Shandong Province, China. Front. Public Health 10:876615. doi: 10.3389/fpubh.2022.876615
Received: 15 February 2022; Accepted: 19 April 2022;
Published: 27 May 2022.
Edited by:
Yunquan Zhang, Wuhan University of Science and Technology, ChinaCopyright © 2022 Wu, Lu, Wei, Zhang, Liu, Zhao, Liu, Guo and Xi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bo Xi, xibo2010@sdu.edu.cn; Xiaolei Guo, guoxiaolei@126.com
†These authors have contributed equally to this work