 Jacqueline Cortinhas Monteiro1,2
Jacqueline Cortinhas Monteiro1,2 Ricardo Roberto de Souza Fonseca1,2Tuane Carolina de Sousa Ferreira1,2Luana Lorena Silva Rodrigues1,2Andreza Reis Brasil da Silva1
Ricardo Roberto de Souza Fonseca1,2Tuane Carolina de Sousa Ferreira1,2Luana Lorena Silva Rodrigues1,2Andreza Reis Brasil da Silva1 Samara Tatielle Gomes3Rodrigo Vellasco Duarte Silvestre3
Samara Tatielle Gomes3Rodrigo Vellasco Duarte Silvestre3 Andréa Nazaré Monteiro Rangel Silva2Ilze Pamplona4
Andréa Nazaré Monteiro Rangel Silva2Ilze Pamplona4 Antonio Carlos Rosário Vallinoto1,2
Antonio Carlos Rosário Vallinoto1,2 Ricardo Ishak1,2
Ricardo Ishak1,2 Luiz Fernando Almeida Machado1,2*
Luiz Fernando Almeida Machado1,2*- 1Biology of Infectious and Parasitic Agents Post-Graduate Program, Federal University of Pará, Belém, Brazil
- 2Virology Laboratory, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
- 3Papillomavirus Laboratory, Evandro Chagas Institute, Health Ministry of Brazil, Ananindeua, Brazil
- 4Reference Unit Specialized in Infectious and Parasitic Diseases, Belém, Brazil
Human papillomavirus (HPV) is the most common sexually transmitted infection in the world. Several studies have shown a higher prevalence of HPV infection in HIV-infected women. The aim of this study was to determine the prevalence and the genotype diversity of HPV infection in HIV-infected women. From April 2010 to December 2012 cervical specimens were collected from 169 HIV-infected women who screening for cervical cancer at Reference Unit in Belém. The detection of HPV infection was performed by nested PCR and HPV type was performed using a commercial system. The prevalence of HPV infection was 63.3%. Of the 47 genotyped samples, 40.4% was found positive for high risk-HPV 16 and 12.8% for high risk-HPV 52. HPV infection was predominant in the group of women with no incidence of cytological abnormalities and more prevalent in women of reproductive age, unmarried, low education level, and who reported use condoms during sexual intercourse. It was observed an association between HPV infection and independent variables, such as condom use, multiple sexual partners, and history of sexually transmitted diseases. High-risk types of HPV infection were prevalent in our study. Infection with multiple high-risk HPV genotypes may potentiate the development of cervical cancer in HIV-infected women.
Introduction
The human papillomavirus (HPV) belongs to the Pappillomaviridae family, which currently consists of two subfamilies that include more than 50 genera and more than 130 species that can infect various classes of vertebrates (1). Morphologically, papillomaviruses are non-enveloped viruses, ~55 nm in diameter. The capsid exhibits icosahedral symmetry and surrounds the viral genome, a double-stranded circular DNA molecule of ~8,000 nucleotide base pairs (bp). Thus far, 228 HPV genotypes have been identified (2).
HPV infects the epithelial surface and can lead to the development of proliferative benign lesions in the skin, mucosa and genital tract (3). Genital HPV infection is among the sexually transmitted infections (STIs) with the highest incidence and prevalence worldwide (4–7) and is associated with the development of low- to high-grade squamous intraepithelial lesions (LSIL and HSIL, respectively).
Currently, the World Health Organization pinpoints HPV as the causal agent of cervical cancer, and virus types are classified as high- and low-risk according to their oncogenic potential. The most common low-risk HPV types are HPV-6 and HPV-11, which are most frequently detected in benign genital warts (8, 9). Among the most prominent high-risk types, HPV-16, HPV-18, HPV-31, and HPV-45 are frequently found in squamous cell carcinomas of the cervix, accounting for almost 80% of cases (10) HPV-16 and HPV-18 are responsible for 50 and 20% of all cases worldwide, respectively (11–15).
The prevalence of HPV infection can vary significantly according to the studied population and HPV detection methods. High rates have been described among sexually active adolescent girls and human immunodeficiency virus (HIV)-positive women (16–21). In immunocompetent women, HPV infection resolves within up to 24 months. However, ~10% of affected women develop a persistent infection (22). The high rate of HPV prevalence among HIV-infected women is thought to be due to the compromised immune system caused by HIV infection, thus enabling viral persistence of HPV (23) and increasing the probability of contracting infections from multiple HPV genotypes, resulting in a higher risk of progression to cervical neoplasia (24, 25).
The HPV types related with the development of HSIL and cervical intraepithelial neoplasia (CIN) in HIV-positive women living in Pará state, in oriental Amazon Region are not well-characterized. In this sense, the present study aimed to describe the prevalence of infection by different HPV types among HIV-positive women in the city of Belém, Pará State, Brazil.
Materials and Methods
Type of Study and Ethical Aspects
The present work is an observational population-based cross-sectional prevalence study in which epidemiological information was obtained from a single data collection. Abiding by resolutions 196/96 and 347/05 of the National Health Council, the present project was submitted to review and was approved by the Research Ethics Committee of the Instituto de Ciências da Saúde of the Universidade Federal do Pará—UFPA, under the protocol number 1765/10.
Ethics
Written informed consent were obtained from all 169 women for the publication of any potentially identifiable images or data included in this article.
Study Population
A total of 169 women with a previously confirmed diagnosis of HIV-1 infection who underwent clinical and laboratorial care at Unidade de Referência Especializada em Doenças Infecciosas e Parasitárias Especiais (UREDIPE) under the Executive Secretariat of Public Health of the State of Pará (Secretaria Executiva de Saúde Pública do Estado do Pará—SESPA) participated in the study from March 2010 to December 2012 (Figure 1). The UREDIPE is a reference center that provides HIV services and care for HIV within the public health system in city of Belém, Pará, Brazil. Among the HIV services and cares provided there is the Cervical Cancer Prevention Sector (CCPS) and all individuals who participated this study sought spontaneously CCPS services.
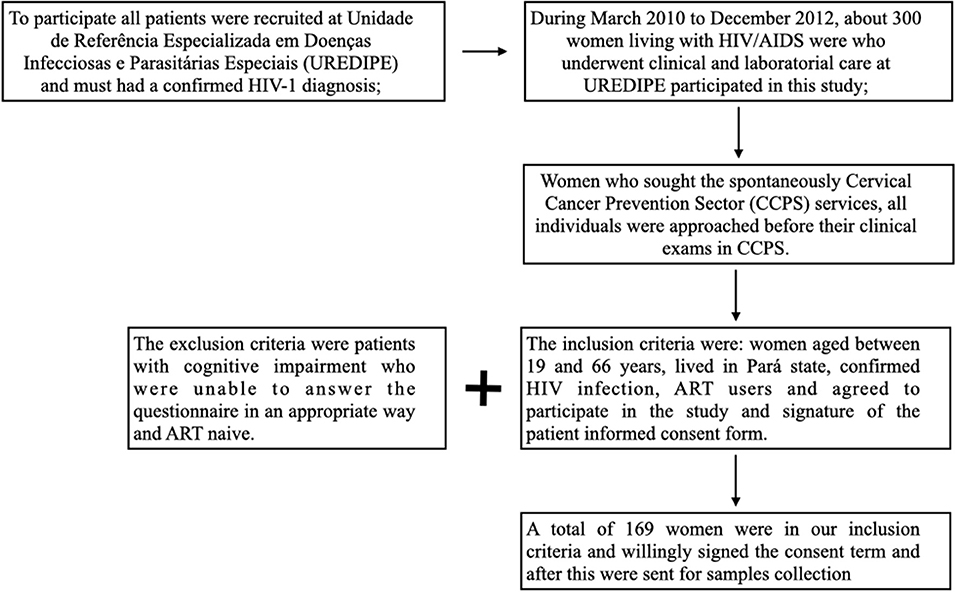
Figure 1. Flowchart for the selection of study participants.
The inclusion criteria were: women aged between 19 and 66 years, lived in Pará state, confirmed HIV infection, ART users and agreed to participate in the study and signature of the patient informed consent form. The exclusion criteria were patients with cognitive impairment who were unable to answer the questionnaire in an appropriate way and ART naive.
Cytological Samples and DNA Extraction
Two uterine cervix smears samples were collected from each participant: one was processed on slides for cytological analysis according to the guidelines for cervical cancer screening of the Ministry of Health of Brazil, and the other was submitted to molecular biological analysis for HPV testing.
Slides were stained by the Papanicolaou method and were analyzed by a professional specializing in cytopathology at the Laboratório Central do Estado do Pará (LACEN-PA). Cytology results were classified according to the Brazilian Nomenclature for Cervical Cytology Reports (26). Descriptive diagnosis involves normal cytological limits of the examined material, the occurrence of benign alterations (inflammation, repair, immature squamous metaplasia, inflammatory atrophy, radiation) and the occurrence of pre-malignant or malignant alterations (atypia of undetermined significance—squamous, glandular, and of undetermined origin; LSIL; HSIL; carcinoma in situ).
Uterine cervix samples intended for molecular biological analysis were collected with endocervical brushes and placed in flasks containing 2 mL of phosphate-buffered saline (PBS). After collection, samples were taken to the Virology Laboratory of the Institute of Biological Sciences of the UFPA, where they were registered and stored at −0°C until use.
All samples were submitted to total DNA extraction from exfoliated cervical cells (cervix sample) by means of phenol-chloroform extraction (27).
Nested PCR
The HPV L1 open reading frame (ORF) (450 bp) was amplified by means of nested-PCR with primers MY09/11 (first stage) and GP05+/06+ (second stage), which were previously described (28, 29). Each reaction contained a final volume of 50 μL with 200 ng of extracted DNA; 200 μM of each dNTP; 10 pmol of each primer; 50 nM KCL, 2.5 mM MgCl2; 10 mM Tris-HCl, pH 8.3, and 1 U of Taq polymerase (29).
All amplifications were performed in a Peltier Thermal Cycler (Biocycler, USA) using the following settings: 95°C for 5 min, 40 cycles of (95°C for 1 min; 56°C for 1 min; 72°C for 1 min), and a final extension at 72°C for 10 min. PCR products were submitted to electrophoresis (100 V/45 min) in 2 % (HPV) and 3 % (interleukin genes) agarose gel with 1x TAE buffer containing 6 μL of SYBR Safe (Invitrogen, Oregon, USA) and were then visualized in a UV transilluminator.
Genotyping
HPV genotyping was performed with the Linear Array HPV Genotyping Test (Roche Molecular Systems, Inc., New Jersey, USA) according to the manufacturer's instructions. This method allows the detection of 37 different types of HPV.
Information on CD4+/CD8+ T lymphocyte counts and plasma HIV-1 viral load was obtained by means of access to the Laboratory Test Control System of the Brazilian National CD4+/CD8+ T Lymphocyte Count and Viral Load Network.
Statistical Analysis
The results on HPV prevalence in HIV-1-infected patients were correlated with epidemiological information obtained from interviews using Chi-square test, G-test and Exact Fisher's Test.
Results
The global prevalence of HPV infection in the studied population was 63.3% (107/169). Epidemiological profile analysis of the group of HIV-positive women co-infected with HPV revealed that infection was most prevalent among women of reproductive age (64.5%; 69/107); between 19 and 38 years; single, separated or widowed (55.1%; 59/107); and with a low education level (52.3%; 56/107). Furthermore, prevalence decreased with increasing age, with a 1.6 odds ratio of infection in the group of women of reproductive age.
There were no statistically significant relationships between HPV infection and the variables age, marital status and education level. There were also no statistically significant relationships with the risk factors for infection by HPV (drinking, smoking, and illegal drug use), given that the highest prevalence of infection was found in the group that exhibited none of these habits (Table 1).
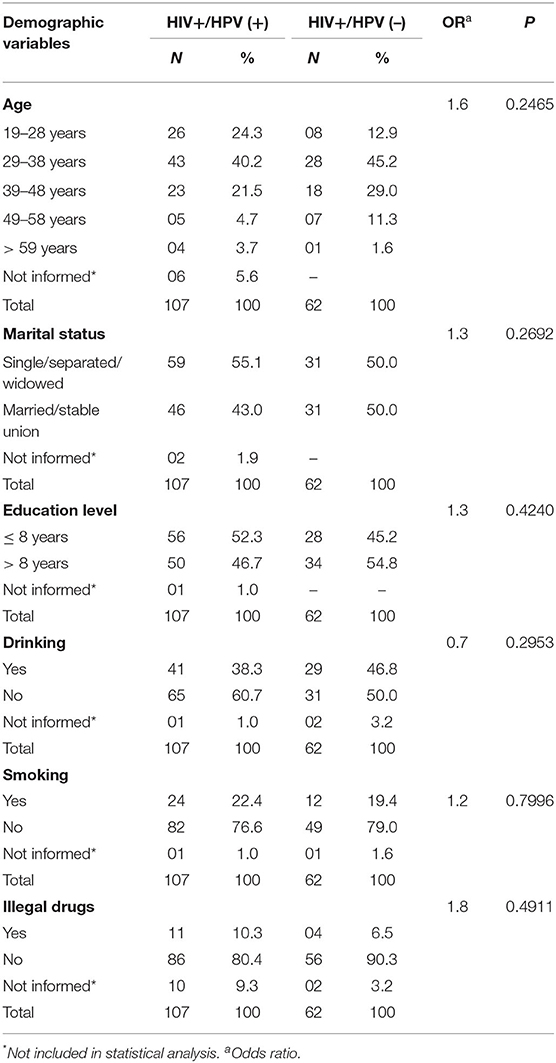
Table 1. Demographic characteristics of women co-infected with HPV/HIV who were seen at the UREDIPE in the period between April 2010 and December 2012.
With respect to sexual behavior, approximately half the HPV-infected women (50.4%) had their first sexual intercourse at the age of 15 years. Most self-reported to be heterosexual (96.2%; 103/107), with an active sex life (76.6%; 72/107), in a steady relationship (69.2%; 74/107) and to practice anal sex (46.7%; 50/107). There were statistically significant associations between infection and the use of condoms and with the number of different sex partners in the past year, with a 2.6-fold higher chance of infection in the group of women who regularly used condoms during sexual intercourse (Table 2).
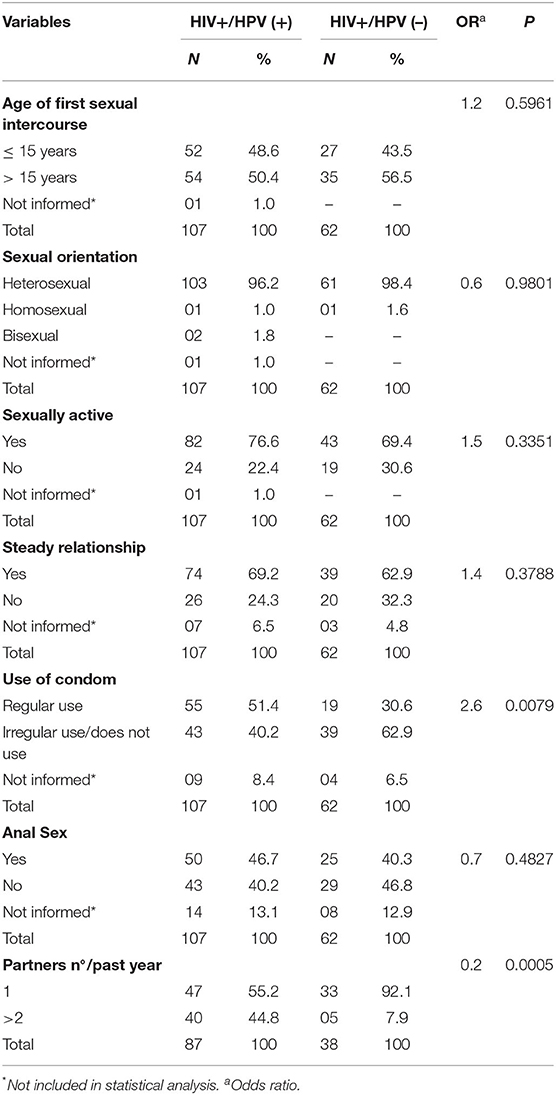
Table 2. Distribution of sexual behavior variables in a group of women co-infected with HPV/HIV who were seen at the UREDIPE and who had Pap smears in the period between April 2010 and December 2012.
The occurrence of HPV infection was highest in the group of women with a previous history of STIs (68.2%; 73/107), no history of genital warts (65.4%; 70/107), and on antiretroviral therapy (ART). The chance of acquiring an HPV infection was 17.6-fold higher in the group with a history of STIs and 2-fold higher in the group with a history of genital warts (Table 3).
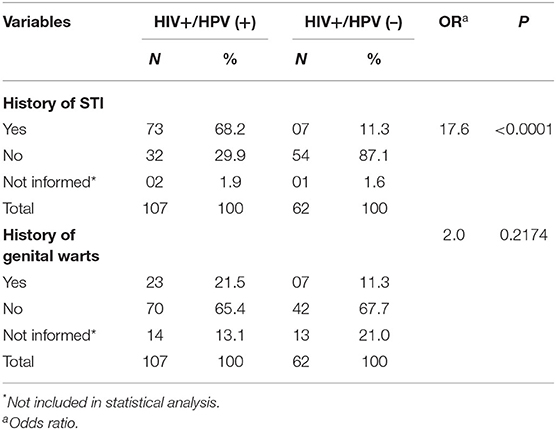
Table 3. Distribution of the variables history of STI and genital warts in a group of women co-infected with HPV/HIV who were seen at the UREDIPE and who had Pap smears in the period of April 2010 to December 2012.
With respect to cytology, two samples were unsuitable for analysis. Only 3.5% (6/169) of the examined cervical smears were free of cellular alterations. Furthermore, 75.8% (128/169) exhibited some type of benign alteration, and 19.5% (33/169) exhibited pre-malignant alterations. There was no statistically significant difference between cytology results and HPV infection (Table 4).
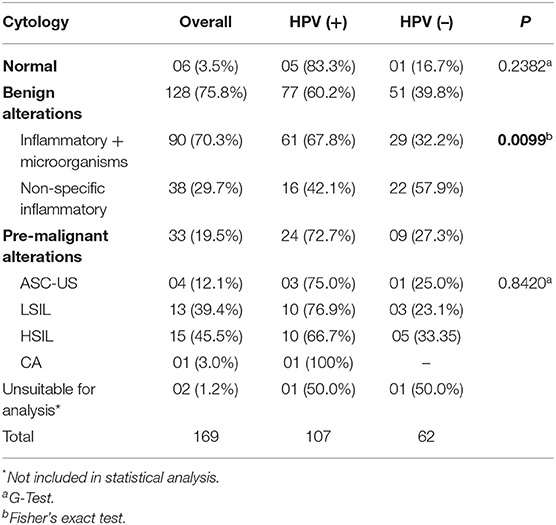
Table 4. Prevalence of HPV infection with respect to the cytology report in a group of HIV-infected women who were seen at the UREDIPE and who had Pap smears in the period of April 2010 to December 2012.
Among women with normal cytology, HPV was present in 83.3% (5/6) of the examined material. In the group of women with cytological alterations, HPV was detected in 60.2% (77/128) of the cases with benign alterations and in 72.7% (24/33) of those with pre-malignant alterations (Table 4).
In the group of women with benign alterations (128/169), inflammatory alterations associated with microorganisms corresponded to 70.3% (90/128) of the cases, among which HPV was detected in 61 samples (67.8%). With respect to samples with a non-specific inflammatory smear (29.7%; 38/128), HPV was detected in 16 specimens (42.1%).
The analysis of the type of benign alteration identified in the studied sample exhibited a statistically significant association with HPV infection, with a 2.9-fold higher odds ratio in the group that exhibited alterations associated with the presence of microorganisms (Table 4).
Among the inflammatory alterations associated with the presence of microorganisms (n = 90), 40% (36/90) corresponded to microbiological findings (Lactobacillus, cocci and other bacilli). Bacilli suggestive of infections by Gardnerella vaginalis were found in 32.2% (29/90) of the examined women. The presence of Trichomonas vaginalis and findings suggestive of HPV infection were observed in 6% of the cases.
With respect to pre-malignant alterations, 28 (84.8%) of the 33 samples exhibited intraepithelial lesions, among which 15 (45.4%) were HSIL and 13 (39.4%) were LSIL. The occurrence of atypical squamous cells of undetermined significance (ASC-US) was identified in 12.1% (6/33) of the samples. One case of invasive carcinoma (Ca) was also detected. However, there was no statistically significant relationship between the different grades of intraepithelial lesion and the presence of HPV (G = 0.3439; p = 0.8420; Table 4).
Genotyping identified the HPV types in as few as 43.9% (47/107) of the samples. Twenty-six different types were identified, among which the most prevalent were HPV-16 (40.4%; 19/47), HPV-52 (12.8%; 6/47), and HPV-84 (8.5%; 4/47).
Furthermore, among the genotyped samples, 51.0% (24/47) exhibited infection by a single genotype, among which HPV-16 was found in 37.5% (9/24), followed by HPV-61 in 12.5 % (3/24). Infections by multiple genotypes corresponded to 49% (23/47), among which HPV-16 and HPV-52 were detected in 43.5% (10/23) and 21.7% (5/23) of cases, respectively (Table 5).
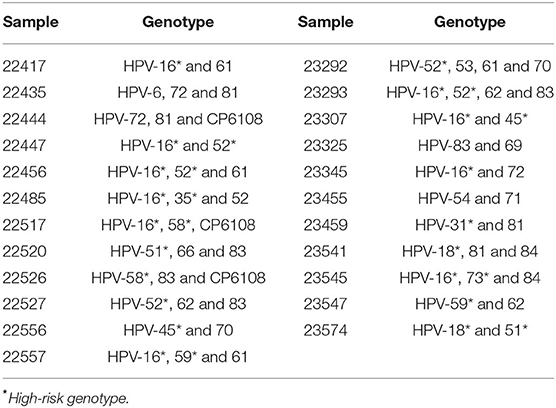
Table 5. Distribution of HPV genotypes identified in a group of women infected with multiple genotypes and co-infected with HIV who were seen at the UREDIPE in the period of April 2010 to December 2012.
The classification of species according to oncogenic potential showed that 72.3% (34/47) of the infections were high-, 21.3% low-, and 6.4% intermediate-risk genotypes. Among the samples with infections by multiple genotypes, 39.1% (9/23) exhibited more than one high-risk genotype (Table 5). There were no statistically significant differences between levels of CD4+ or CD8+ T lymphocytes, plasma HIV viral load and HPV infection.
Discussion
In Brazil, according to data of the National Cancer Institute (30), cervical cancer is the most common cancer type together with breast cancer among women of the North Region of the country, with an estimated risk of 26,24 cases per 100 thousand women. Many studies have shown that an infection by an HPV of high oncogenic risk, especially HPV-16 and 18, is closely related with the development of cervical cancer, with a higher chance of occurrence among HIV-positive women (14).
According to studies in the literature, HPV infection occurs in the first two consecutive years after first sexual intercourse, given that the incidence is higher among women below 25 years of age (13, 17). In the present study, among the group of HPV-infected women, the mean age was of 36 years, and infection was predominant among women of reproductive age, with a trend to reduced prevalence with increasing age. Similar data have been described in other Brazilian cities (31–33). The results of the present study suggest that the reduced prevalence of infection in the group of women aged 39 years and above is due to marriage and, thus, reductions in both the number of partners and exposure to HPV.
Several epidemiological and reproductive health factors have been related with the development of cervical cancer, including HPV, smoking, genetic predisposition, number of sex partners, age of first sexual intercourse, parity, miscarriages, and age at menarche (34). With respect to HPV infection, with the exception of immunosuppression caused by HIV, the literature is controversial with regard to establishing the risk factors for the acquisition of infection.
Studies on the general population of the North Region of Brazil have found diverging epidemiological associations between the examined population groups. In the Brazilian Eastern Amazon, there were strong associations between HPV infection and marital status, the use of condoms and the number of sex partners throughout life and in the past year (14, 15). The association between HPV infection and age range has been described in women of the general population, in female inmates in the Metropolitan Region of Belém (35) and in women in the municipality of Tomé-Açu (36).
Based on the results of the present study, even the regular use of condoms does not seem to provide total protection against microbial infection, given that the condom does not fully cover the male reproductive organ, hence leaving areas potentially harboring infectious particles or subclinical lesions, in the case of HPV, exposed during sexual intercourse associated to this perception we can observe the possibility that not all patients given the true response about his real behavior inserting a trend in this analysis that we cannot measure but is prudent to consider. A history of multiple sex partners is an important risk factor for the acquisition of HPV because the higher the number of partners, drive more probability to interact with a contaminated partner (3, 35, 36).
The innate immune system is known to have many protection mechanisms in the vaginal tissue against infections by pathogens, in part by ensuring the survival of the normal vaginal microbiota, which constitutes an important factor in the production of lactic acid and hydrogen peroxide, thus inhibiting pathogen growth. The acquisition of STIs promotes an imbalance in the vaginal microbiota, altering the pH and also possibly causing lesions in the lining epithelium of the cervix and vaginal wall. These changes might contribute to the development of inflammation and pathogen penetration, including HPV (37, 38). In addition to the observed association between a previous history of STIs and HPV infection, the present study found that many women exhibited clinical features compatible with bacterial vaginosis, candidiasis and trichomoniasis, suggesting that the establishment of these infections might contribute to the acquisition and onset of HPV infection. Similar data have been reported by Grinsztejn et al. (31) in Rio de Janeiro, whereas Gonçalves et al. (36) found that age was the only variable associated with HPV infection in anogenital samples from HIV-positive women.
The global prevalence of HPV infection among HIV-1-positive women in the present study corroborates the findings of Gonçalves et al. (36) but is lower than the rates observed in other Brazilian regions (32, 39). Among immunocompetent women of the North Region, the prevalence rate of HPV infection varies between 6, 9, and 18% (35, 36, 40) showing that the incidence of HPV infection is high in the population of HIV-positive women.
The majority of HPV infections are clinically unapparent or asymptomatic in immunocompetent individuals (14, 41). However, the immunosuppression caused by HIV seems to favor infection by multiple HPV genotypes, which, if oncogenic, might contribute to the progression of intraepithelial lesions to CIN (15). According to Luque et al. (42) the presence of multiple HPV genotypes in HIV-positive women is a poor indicator of prognosis in cases of CIN. In the present study, 49% (23/47) of the studied population exhibited infections by multiple genotypes, and, of these, 39.1% exhibited more than one high-risk genotype. Some samples that were positive in the nested-PCR could not be genotyped due to the fact that samples were exhausted in the first method and did not have enough quantity to be used in the Linear Array. On the other hand, nested-PCR can really overestimate the positive amplification that is not corroborated in genotyping.
Previous studies have shown that the prevalence rates of lesions and CIN are higher among HIV-positive women compared to women from the general population (16, 18, 39, 43) HIV infection is thought to change the natural history of HPV infection, favoring higher HPV persistence, reduced lesion regression rates and, consequently, progression to high-grade, or invasive squamous intraepithelial lesions (25, 44–46).
Some studies suggest that the persistence of HPV is inversely proportional to CD4+ T lymphocyte count and directly proportional to HIV viral load, which can also be influenced by ART (44, 46, 47). However, there was no association between markers of HIV infection and HPV infection or between the different grades of intraepithelial lesions in the present study. These data corroborate other studies on HIV-positive women from the Southeast Region of Brazil (19, 31–33). Thus, it is suggested that ART is efficient in the maintenance of low levels of HIV replication, avoiding the abrupt depletion of CD4+ T lymphocyte levels. However, the effect of ART on the persistence of HPV infection has not yet been characterized in the literature due to the absence of studies on that topic (20, 21).
Our study has some limitations. As mentioned in flowchart in Figure 1, the authors invited 300 women from a reference center in Pará state, however only 169 could be recruited due to inclusion criteria, so it did not include a truly population-based design. Our sample included women who all had a prolonged ART use, had history of STI, had genital warts, had pre-malignant alterations, median age between 19 and 38 years and presented a co-infection between HIV-HPV. This study is a cross sectional design study, which allows only presentation of baseline information, and the differences with the results presented by this study from other studies might be partly explained by information bias. Indeed, the study design used does not allow differentiating statistically significant relationships between HPV infection and the variables age, marital status and education level. Another possible bias is the none correlation between known cancer risk factors as drinking, smoking and illegal drug use with infection by HPV.
The data obtained in the present study show the high prevalence of HPV infection among HIV-positive women and reinforce the notion that immunocompromised women tend to develop infections by multiple high-risk HPV genotypes. Thus, the importance of molecular diagnosis of HPV infection associated with oncotic cytology in the early detection of cases, with the aim of avoiding progression to CIN, is reinforced.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
This project was approved by the Research Ethics Committee of the Institute of Health Sciences of the Federal University of Pará, under protocol number 1765/10. All participants signed a consent form.
Author Contributions
JM and LM: conceptualization. TF, LR, RF, and AS: data curation. IP, RS, and AS: investigation and methodology. RS, SG, and LM: formal analysis. AV, RI, and LM: writing-original draft. RF, AV, RI, and LM: writing-review and editing. JM and LM: project administration. All authors read and approved the final manuscript and contributed to the development of research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We acknowledge all subjects enrolled in this study and UREDIPE and Executive Secretariat of Public Health of the State of Pará.
References
1. Van Doorslaer K, Chen Z, Bernard HU, Chan PKS, DeSalle R, Dillner J, et al. ICTV virus taxonomy profile: papillomaviridae. J Gen Virol. (2018) 99:989–90. doi: 10.1099/jgv.0.001105
2. International Human Papillomavirus Reference Center. Reference Clones. Stockholm: Karolinska Institutet (2021). Available online at: https://www.hpvcenter.se/human_reference_clones/ (accessed march 5, 2021).
3. Bohlius J, Foster C, Naidu G, Sengayi M, Turkova A. Cancer in adolescents and young adults living with HIV. Curr Opin HIV AIDS. (2018) 13:196–203. doi: 10.1097/COH.0000000000000460
5. Shavit O, Raz R, Stein M, Chodick G, Schejter E, Ben-David Y, et al. Evaluating the epidemiology and morbidity burden associated with human papillomavirus in Israel: accounting for CIN1 and genital warts in addition to CIN2/3 and cervical cancer. Appl Health Econ Health Policy. (2012) 10:87–97. doi: 10.2165/11594780-000000000-00000
6. Cortés-Alaguero C, González-Mirasol E, Morales-Roselló J, Poblet-Martinez E. Do clinical data and human papilloma virus genotype influence spontaneous regression in grade I cervical intraepithelial neoplasia? J Turk Ger Gynecol Assoc. (2017) 18:1–8. doi: 10.4274/jtgga.2016.0138
7. Paluszkiewicz A, Pruski D, Iwaniec K, Kedzia W. Comparison of the diagnostic value of cervical cytology and HPV HR DNA testing for the diagnosis of low-grade and high-grade squamous intraepithelial lesions across different age groups. Ginekologia Polska. (2017) 88:141–6. doi: 10.5603/GP.a2017.0027
8. Dunne E, Markowitz L. Emerging infections: genital human papillomavirus infection. Clin Infect Dis. (2006) 43:624–9. doi: 10.1086/505982
9. Garnett T, Duerksen-Hughes P. Modulation of apoptosis by human papillomavirus (HPV) oncoproteins. Arch Virol. (2006) 151:2321–35. doi: 10.1007/s00705-006-0821-0
10. de Sanjosé S, Quint WG, Alemany L, Geraets DT, Klaustermeier JE, Lloveras B, et al. Retrospective international surveyand HPV time trends study group human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study. Lancet Oncol. (2010) 11:1048–56. doi: 10.1016/S1470-2045(10)70230-8
11. Dueñas-González A, Lizano M, Candelaria M, Cetina L, Arce C, Cervera E. Epigenetics of cervical cancer. Na overview and therapeutic perspectives. Mol Cancer. (2005) 4:38. doi: 10.1186/1476-4598-4-38
12. Schiffman M, Cliffford G, Buonaguro F. Classification of weakly carcinogenic human papillomavirus types: addressing the limits of epidemiology at the borderline. Infect Agent Cancer. (2009) 4:8. doi: 10.1186/1750-9378-4-8
13. Konopnicki D, Manigart Y, Gilles C, Barlow P, De Marchin J, Feoli F, et al. High-risk human papillomavirus genotypes distribution in a cohort of HIV-positive women living in Europe: epidemiological implication for vaccination against human papillomavirus. AIDS. (2016) 30:425–33. doi: 10.1097/QAD.0000000000000929
14. Teixeira M, Sabidó M, Leturiondo A, de Oliveira Ferreira C, Torres K, Benzaken A. High risk human papillomavirus prevalence and genotype distribution among women infected with HIV in Manaus, Amazonas. Virol J. (2018) 15:36. doi: 10.1186/s12985-018-0942-6
15. Hidalgo-Tenorio C, de Jesus S, Esquivias J, Pasquau J. High prevalence and incidence of HPV-related anal cancer precursor lesions in HIV-positive women in the late HAART era. Enferm Infecc Microbiol Clin. (2018) 36:555–62. doi: 10.1016/j.eimc.2017.10.014
16. Minkoff H, Feldman J, DeHovitz J, Landesman S, Burk R. A longitudinal study of human papillomavirus carriage in human immunodeficiency virus–infected and human immunodeficiency virus–uninfected women. Am J Obstet Gynecol. (1998) 178:982–6. doi: 10.1016/S0002-9378(98)70535-6
17. Moscicki A. HPV Infections in adolescents. Dis Markers. (2007) 23:229–34. doi: 10.1155/2007/136906
18. Ng'andwe C, Lowe J, Richards P, Hause L, Wood C, Angeletti P. The distribution of sexually-transmitted human papillomaviruses in HIV positive and negative patients in Zambia, Africa. BMC Infect Dis. (2007) 7:77. doi: 10.1186/1471-2334-7-77
19. Chatha Z, Rashid U, Olsen S, Din F, Khan A, Nawaz K, et al. Pharmacist-led counselling intervention to improve antiretroviral drug adherence in Pakistan: a randomized controlled trial. BMC Infect Dis. (2020) 20:874. doi: 10.1186/s12879-020-05571-w
20. Musumari P, Srithanaviboonchai K, Tangmunkongvorakul A, Dai Y, Sitthi W, Rerkasem K, et al. Predictors of health-related quality of life among older adults living with HIV in Thailand: results from the baseline and follow-up surveys. AIDS Care. (2021) 33:10–9. doi: 10.1080/09540121.2019.1707472
21. Ahmed A, Saqlain M, Bashir N, Dujaili J, Hashmi F, Mazhar F, et al. Health-related quality of life and its predictors among adults living with HIV/AIDS and receiving antiretroviral therapy in Pakistan. Qual Life Res. (2021) 13. doi: 10.1007/s11136-021-02771-y
22. Wentzensen N, Schiffman M, Dunn S, et al. Grading the severity of cervical neoplasia based on combined histopathology, cytopathology, and HPV genotype distribution among 1,700 women referred to colposcopy in Oklahoma. Int J Cancer. (2009) 124:964–9. doi: 10.1002/ijc.23969
23. Strickler HD, Palefsky JM, Shah KV, Anastos K, Klein RS, Minkoff H, et al. Human papillomavirus type 16 and immune status in human immunodeficiency virus-seropositive women. J Natl Cancer Inst. (2003) 95:1062–71. doi: 10.1093/jnci/95.14.1062
24. Mbulawa Z, Marais D, Johnson L, Coetzee D, Williamson A. Impact of human immunodeficiency virus on the natural history of human papillomavirus genital infection in South African men and women. J Infect Dis. (2012) 206:15–27. doi: 10.1093/infdis/jis299
25. Seyler L, Lacor P, Allard S. Current challenges in the treatment of HIV. Pol Arch Intern Med. (2018) 128:609–16. doi: 10.20452/pamw.4357
26. Instituto Nacional do Câncer. (2020). Relatório da Consulta Pública - Nomenclatura do Exame Citopatológico do Colo do Útero. Available online at: https://www.inca.gov.br/publicacoes/relatorios/relatorio-da-consulta-publica-nomenclatura-do-exame-citopatologico-do-colo-do (accessed at: March 8, 2020).
27. Green MR, Sambrook J. Molecular Cloning: A Laboratory Manual, 4th Edn. New York, NY: Cold Spring Harbor Laboratory Press (2012). p. 47–53.
28. Muñoz N, Bosch FX, de Sanjosé S, Herrero R, Castellsagué X, Shah KV, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. (2003) 348:518–27. doi: 10.1056/NEJMoa021641
29. Demathe A, Bernabé DG, Garcia JF, Nunes CM, Miyahara GI. Comparação entre dois métodos de detecção de DNA de papilomavírus humano em carcinoma epidermoide de lábio. J Bras Patol Med Lab. (2010) 46:85–90. doi: 10.1590/S1676-24442010000200003
30. Instituto Nacional do Câncer. Estimativa 2020: Incidência De Câncer No Brasil. (2020). Available online at: https://www.inca.gov.br/publicacoes/livros/estimativa-2020-incidencia-de-cancer-no-brasil (accessed at: March 8, 2020).
31. Grinsztejn B, Veloso VG, Levi JE, Velasque L, Luz PM, Friedman RK, et al. Factors associated with increased prevalence of human papillomavirus infection in a cohort of HIV-infected Brazilian women. Int J Infect Dis. (2009) 13:72–80. doi: 10.1016/j.ijid.2008.03.031
32. Entiauspe L, Teixeira L, Mendoza-Sassi R, Gonçalves C, Gonçalves P, Martinez A. Papilomavírus humano: prevalência e genótipos encontrados em mulheres HIV positivas e negativas, em um centro de referência no extremo Sul do Brasil. Rev Soc Bras Med Trop. (2010) 43:260–3. doi: 10.1590/S0037-86822010000300009
33. Corrêa CM, Teixeira NC, Araújo AC, Carvalho N, Castillo DM, Campos RR, et al. Prevalence and multiplicity of HPV in HIV women in Minas Gerais, Brazil. Rev Assoc Med Bras. (2011) 57:425–30. doi: 10.1590/S0104-42302011000400017
34. Pinto D, Fuzii H, Quaresma J. Prevalência de infecção genital pelo HPV em populações urbana e rural da Amazônia Oriental Brasileira. Cadernos de Saúde Pública. (2011) 27:769–78. doi: 10.1590/S0102-311X2011000400016
35. Prazeres B. Prevalência de HPV em material cérvico-uterino de mulheres de Tomé-Açu, Pará. (2011). Belém, PA: University of Pará.
36. Gonçalves MA, Randi G, Arslan A, Villa LL, Burattini MN, Franceschi S, et al. HPV type infection in different anogenital sites among HIV-positive Brazilian women. Infect Agent Cancer. (2008) 14:3–5. doi: 10.1186/1750-9378-3-5
37. Zeier M, Botha M, Engelbrecht S, Machekano R, Jacobs G, Isaacs S, et al. Combination antiretroviral therapy reduces the detection risk of cervical human papilloma virus infection in women living with HI. AIDS. (2015) 29:59–66. doi: 10.1097/QAD.0000000000000512
38. Kelly H, Sawadogo B, Chikandiwa A, Segondy M, Gilham C, Lompo O, et al. Epidemiology of high-risk human papillomavirus and cervical lesions in African women living with HIV/AIDS: effect of anti-retroviral therapy. AIDS. (2017) 31:273–85. doi: 10.1097/QAD.0000000000001301
39. Noronha V, Cruz E, Pinho C, Mello W, Villa L, Russomano F. Human papillomavirus (HPV) in women screened to cervical uterine cancer, Belém – Pará – Brazil. J bras Doeno̧as Sex Transm. (2011) 23:5–11. doi: 10.5533/2177-8264-201123103
40. Oliveira-Silva M, Lordello C, Zardo L, Bonvicino C, Moreira M. Human papillomavirus in Brazilian women with and without cervical lesions. Virol J. (2011) 8:1–6. doi: 10.1186/1743-422X-8-4
41. Rocha D, Barbosa Filho R, de Queiroz F, dos Santos C. High Prevalence and genotypic diversity of the human papillomavirus in Amazonian women, Brazil. Infect Dis Obstet Gynecol. (2013) 2013:514859. doi: 10.1155/2013/514859
42. Luque AE, Jabeen M, Messing S, Lane CA, Demeter LM, Rose RC, et al. Prevalence of human papillomavirus genotypes and related abnormalities of cervical cytological results among HIV-1-infected women in Rochester, New York. J Infect Dis. (2006) 194:428–34. doi: 10.1086/505876
43. Smits PH, Bakker R, Jong E, Mulder JW, Meenhorst PL, Kleter B, et al. High prevalence of human papillomavirus infections in urine samples from human immunodeficiency virus-infected men. J Clin Microbiol. (2005) 43:5936–9. doi: 10.1128/JCM.43.12.5936-5939.2005
44. Joshi SN, Gopalkrishna V, Kumar BK, Dutta S, Nyaynirgune P, Thakar M, et al. Cervical squamous intra-epithelial changes and human papillomavirus infection in women infected with human immunodeficiency virus in Pune, India. J Med Virol. (2005) 76:470–5. doi: 10.1002/jmv.20385
45. Tanaka L, Latorre M, Gutierrez E, Heumann C, Herbinger K, Froeschl G. Trends in the incidence of AIDS-defining and non-AIDS-defining cancers in people living with AIDS: a population-based study from São Pãulo, Brazil. Int J Std AIDS. (2017) 28:1190–8. doi: 10.1177/0956462417692924
46. Palefsky J. Biology of HPV in HIV infection. Adv Dent Res. (2006) 19:99–105. doi: 10.1177/154407370601900120
Keywords: HPV, HIV/AIDS, sexually transmitted disease, epidemiology, amazon region
Citation: Monteiro JC, Fonseca RRdS, Ferreira TCdS, Rodrigues LLS, da Silva ARB, Gomes ST, Silvestre RVD, Silva ANMR, Pamplona I, Vallinoto ACR, Ishak R and Machado LFA (2021) Prevalence of High Risk HPV in HIV-Infected Women From Belém, Pará, Amazon Region of Brazil: A Cross-Sectional Study. Front. Public Health 9:649152. doi: 10.3389/fpubh.2021.649152
Received: 07 January 2021; Accepted: 24 March 2021;
Published: 29 April 2021.
Edited by:
Álvaro Borges, Statens Serum Institut (SSI), DenmarkReviewed by:
José Eduardo Levi, University of São Paulo, BrazilAmjad Khan, Quaid-i-Azam University, Pakistan
Copyright © 2021 Monteiro, Fonseca, Ferreira, Rodrigues, da Silva, Gomes, Silvestre, Silva, Pamplona, Vallinoto, Ishak and Machado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luiz Fernando Almeida Machado, lfam@ufpa.br