 Wenjiao Yang
Wenjiao Yang Yanfei Hou
Yanfei Hou Yu Chen*
Yu Chen* Wenting Liu
Wenting Liu Julan Xiao
Julan Xiao- School of Nursing, Southern Medical University, Guangzhou, China
Previous studies have suggested that certain personality characteristics are associated with emotional distress during pregnancy. However, the underlying mechanism of this association is rarely understood. The current study investigated the links between personality and pregnant women's emotional distress (depressive and anxiety symptoms), tested the chain mediating effects of two resilience factors—social support and positive coping, and explored whether socioeconomic status (SES) could moderate the effects (including direct and/or indirect effects) of personality on their emotional distress. Results of a relatively large sample of pregnant women in China (N = 1157) showed positive associations for psychoticism and neuroticism with depressive and anxiety symptoms as well as negative associations for extraversion with depression and anxiety. After controlling for four important variables (the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy), social support and positive coping acted as chain mediators on the associations of personality with depressive symptoms as well as of personality with anxiety. Overall, the association of personality and depressive symptoms demonstrated invariance across socioeconomic status (SES). However, SES moderated the relationship between personality and anxiety. Specifically, the negative association of positive coping with anxiety symptoms was weaker for low SES women than for high SES ones. Results highlight the importance of social support and positive coping to decrease personality-related depressive and anxiety symptom among pregnant women. Furthermore, identifying other resilience factors that alleviate anxiety in women with low SES is urgently called for.
Introduction
Emotional distress, including the symptoms of depression and anxiety, is very common among pregnant women. For instance, it is estimated that depression symptoms affect ~25% of pregnant women (1) and that anxiety symptoms affect 18.2–24.6% of them [N = 221,974; (2)]. The meta-analysis on perinatal depression among women residing in low-to-middle-income countries indicated that the pooled prevalence estimate of depression across 51 studies was 25.3% (3). The ratio of depressive and anxiety symptoms in the third gestational trimester has been reported to be as high as 73.5% and 58.5%, respectively (4). In China, prevalence rates of 15.04–22.57% for anxiety and 10.3–35.7% for depression have been reported (5, 6). Robust associations have been documented between emotional distress during pregnancy and maternal and newborn outcomes, such as postpartum emotional distress (7), and preterm birth and a reduction in breastfeeding initiation (8–10). Furthermore, emotional distress during pregnancy has far-reaching and adverse effects on an offspring's subsequent mental health (11, 12). Given the prolonged and adverse effects of emotional distress among pregnant women, it is urgently needed to investigate the associated factors and the underlying mechanisms to help clarify potential intervention objectives to prevent or decrease anxiety and depressive symptoms during pregnancy.
Personality Characteristics and Depressive and Anxiety Symptoms Among Pregnant Women
In terms of the factors influencing depression and anxiety symptoms during pregnancy, negative experiences and environmental factors such as childhood abuse, general life stress, unplanned pregnancy, and being a single mother have received great attention in the literature (13–15). In addition to these factors, recent research has indicated the need to explore the relationship between personality characteristics and emotional distress in pregnancy (13, 16, 17).
“Personality characteristics” means a person's psychological and behavioral traits (18). Personality characteristics are relatively stable traits of an individual and include the tendency to respond to various stimuli in the same way (19). From the perspective of Eysenck (18), there are three independent personality characteristics: P (psychoticism; the trend to be aggressive, cold, tough-minded, antisocial, and insensitive to others), E (extraversion; the attitudes of interest, activation, and security for social interaction and the trend to have positive emotions such as enthusiasm, optimism, and happiness), and N (neuroticism; the trend to have strong and frequent negative emotions in the face of stressful situations).
Although the previous literature has shown that a person's personality characteristics might reflect individual differences in responses to environmental cues (20), only a few studies focus on the relationship between personality characteristics and emotional distress during pregnancy. For instance, a small longitudinal study (N = 96) suggested that neuroticism was significantly linked to anxiety levels during pregnancy (21). Bunevicius et al. (22) sampled 230 pregnant women and found that high neuroticism was an independent predictor of antenatal depressive disorders throughout pregnancy. A survey in China also reported that both high psychoticism and neuroticism personality characteristics are risk factors for depressive symptoms among Chinese pregnant women (17). A recent study in 85 pregnant women reported that psychoticism, neuroticism, and low extraversion were all cross-sectionally and longitudinally linked to depression symptoms (16). These limited empirical studies with relatively small samples indicated that the personality characteristics of pregnant women are closely associated with emotional distress and that pregnant women with high levels of neuroticism and psychoticism, as well as low levels of extraversion, might be more likely to experience depressive and/or anxiety symptoms. As personality characteristics may have a life-long effect on emotion, the effects of personality on emotion among pregnant women should be paid more attention.
Recently, research on postnatal women (N = 672) has begun to test the potential mechanisms of the associations between personality characteristics and postnatal depression. Postnatal anxiety is an important mediator in the relationship between the personality characteristic of extraversion and postnatal depression (23). Such research efforts, however, remain scarce. As the personality characteristic of a person is relatively stable and difficult to adjust, the study of intermediate variables (such as mediating and moderating variables) on the relationship between personality and emotion in pregnant women is urgently required, so as to help alleviate personality-related emotional distress through the development of interventions focused on the intermediate variables. Therefore, our study examined how personality characteristics correlated with depression and anxiety symptoms in a large sample of Chinese pregnant women, as well as the potential mediating and moderating mechanisms.
Potential Chain Mediating Roles of Social Support and Coping Style
Previous research indicated that social support might act as a potential resilience resource for decreasing emotional distress of pregnant women (24–26). It is generally defined as material and spiritual supports and the exchange of material and spiritual resources between individuals, such that the individuals perceive that they are respected, loved, and cared for and have available assistance (27, 32). In interdependent cultures like in China, interpersonal harmony receives heavy emphasis (28); hence, the association between social support and depressive and anxiety symptoms among pregnant women has received a lot of recent attention. Results have consistently shown that low levels of subjective support and/or support utilization are important risk factors for depressive and anxiety symptoms in pregnant women (29–31). According to Xiao (32), social support is comprised of objective support, subjective support, and support utilization. Past research has shown that objective support was less determinative and valuable on emotional distress (33). Additionally, and linked with a tendency toward emotional distress, the N personality has been reported to be associated with low subjective support, and E is associated with increased subjective and utilization of support (16, 34, 35). We therefore expected that when pregnant women had higher levels of subjective and utilization of support, the extent to which they experience depression and anxiety decreases.
In addition to social support, coping style may also mediate the associations between individual characteristics and adaptive outcomes (36). Coping refers to the cognitive and behavioral styles adopted by an individual to manage the demands of stressors (37). Specifically, positive coping styles, such as planning, seeking advice, and engaging in activities, can relieve the impact of a stressor and thereby protect against emotional distress (38). Research with pregnant women has indicated that positive coping styles, including engagement in activities, making plans, and positive reframing, are associated with a significantly reduced occurrence of pregnancy complications (39). Negative coping styles, such as self-blame, denial, and substance abuse, correlated with high levels of depressive symptoms among pregnant women (40). Furthermore, there is a close link between individual personality characteristics and coping. For instance, when N is high and persistent, individuals are less likely to adopt positive coping styles (35). Therefore, it is rational to hypothesize that coping style could also play a similar role in assisting pregnant women prevent the adverse effects of negative personality characteristics. Hence, in the present study, we assumed that coping style may play a mediating role in the association between personality and emotional distress among pregnant women.
Furthermore, coping style, such as seeking advice from others, is positively associated with subjective and utilization of support. The buffering effects of social support on emotional distress are often mediated by the coping behaviors (41). For instance, research on pregnant women demonstrated that positive coping and subjective and utilization of support acted as chain mediators on the link of neuroticism and depressive symptoms after earthquake (42) as well as on the link of childhood abuse and emotional distress among them (43). Meanwhile, positive coping and subjective and utilization of support also acted as chain mediators between the relationship of childhood abuse and depressive symptoms on general adults (35). These might be that social support influences the choice of specific coping behaviors and the effectiveness of the behaviors used. Although there was no direct evidence related to the chain mediator effects of coping style and social support on anxiety in pregnant women, anxiety and depressive symptoms often occur simultaneously and have many common risk and protective factors. Therefore, it is reasonable to infer that positive coping and subjective and utilization of support may act as chain mediators on the relationship between personality characteristics and emotional distress (depressive and anxiety symptoms) among pregnant women.
Moderating Role of Socioeconomic Status
The links of socioeconomic status (SES) and the well-being of pregnant women have received considerable attention from researchers (44, 45). Studies have examined several SES factors such as educational and economic levels in relation to antenatal anxiety and depression, but the results are equivocal. A survey of 5,398 pregnant women found that low educational level and low family income not only were directly and positively associated with anxiety and depression symptoms among them but also increased the disadvantageous effects of previous negative life events (46). Nevertheless, a survey on 583 pregnant women in Malawi found that those with more years of schooling tend to experience higher levels of anxiety and depression symptoms (47). Studies that have examined the emotional associations with low income have also reported contradictory results. While some studies found low income or financial difficulties to be related to severe emotional distress in pregnant women (48, 49), such associations have not been found in other studies. For instance, anxiety symptoms in pregnant women were not associated with their educational level (50). Also, there were no significant differences in the incomes of pregnant women with higher depressive symptoms compared with those with lower symptoms (51).
The above contradictory findings might be caused by individual differences among pregnant women such as personality characteristics, coping styles, and social support. Considering SES and personality, a recent meta-analysis and large online study (N = 2,183,377) found that high SES individuals experience fewer stressful events and more supportive environments, which results in more positive personality qualities (52). The individuals whose parents had a higher number of years of schooling were more likely to be open, extraverted, and emotionally stable (53). Another study indicated that positive coping style was significantly and positively correlated with SES, while negative coping was not (54).
Furthermore, according to the stress-buffering model, the adverse effects of stressors on the development of individuals would be weaker for those with plenty of resources (55). The reasons may be that the resources can alleviate the deleterious impacts of stressors. Usually, individuals with high SES perceive less stress (56), adopt more positive coping styles (57), and have more social support (52). Therefore, it was rational to assume that SES could moderate the direct and/or indirect pathways from personality to both depressive and anxiety symptoms. Specifically, compared with pregnant women with a low level of SES, the negative associations of personality characteristics and emotional distress might be smaller for women with a high level of SES.
Present Study
Although there is some research available on the relationships between personality and depression and anxiety in pregnant women, most studies have been conducted in small samples and there has been little attempt to assess the potential mediating roles of social support and coping styles. Hence, to fill these gaps in the literature, our main aim in the present study was to investigate how and under what conditions personality would be linked with emotional distress in a large sample of Chinese pregnant women. Specifically, the current study sought to specify the association between personality and emotional distress by considering social support and coping style as potential mediators and SES as a potential moderator. Based on the previous literature, we assumed that neuroticism and psychoticism would positively correlate, and extraversion would negatively correlate, with pregnant women's depressive and anxiety symptoms (H1: the relationship hypothesis). Furthermore, we expected that higher neuroticism and psychoticism, and lower extraversion, would be associated with higher levels of emotional distress through lower levels of social support and positive coping and that social support and positive coping acted as chain mediators (H2: the mediating hypothesis). Finally, we also assumed that SES would have a moderating role in the direct and/or indirect links between personality and emotional distress (H3: the moderating hypothesis).
Materials and Methods
Participants
Potential participants were pregnant females visiting the obstetrics and gynecology wards at six general hospitals in six cities (N = 314 in Guangzhou city, N = 166 in Foshan city, N = 153 in Zhaoqing city, N = 210 in Huizhou city, N = 177 in Shenzhen city, and N = 137 in Qingyuan city) of Guangdong Province, China, for a conventional examination between March 2018 and July 2019. During the period of waiting for their appointments, they were asked by investigators to participate in the present study. The inclusion criteria included being more than 18 years old and being in any period of pregnancy. A total of 1,250 women gave their consent to be recruited in this study and accomplished a questionnaire in a quiet office which took around 15 min. However, 36 participants withdrew before they completed the questionnaires. Among the 1,214 questionnaires collected, 39 in-completed surveys and 18 questionnaires with implausible answers were excluded from analysis, leaving 1,157 valid questionnaires for the final analysis (reflecting a valid response rate of 95.30%). There was no significant difference in demographic data between included women and excluded women.
The mean age of the pregnant women was 28.91 years (SD = 4.57, range 18–44 years). Most participants were younger than 35 years (n = 1,020, 88.2%). The educational levels were as follows: 379 (32.8%) had completed more than 16 years of education or a bachelor's degree, 404 (34.9%) had completed 14–15 years of education or 2–3 years of college studies, 209 (18.1%) had completed 12 years of education or senior middle school studies, and finally, 165 (14.3%) had not completed either 9 years of education or junior middle school studies. Meanwhile, the education levels of the husbands of participants were as follows: 458 (39.6%) had completed more than 16 years of education or a bachelor's degree, 372 (32.2%) had completed 14–15 years of education or 2–3 years of college studies, 191 (16.5%) had completed 12 years of education or senior middle school studies, and finally, 136 (11.8%) had not completed either 9 years of education or junior middle school studies. Furthermore, the monthly household incomes were reported as follows: 392 (33.9%) had over 10,000 yuan, 470 (40.6%) had 5,000–9,999 yuan, 250 (21.6%) had 3,000–4,999 yuan, and 45 (3.9%) had <2,999 yuan.
Procedure
The procedure was approved by the review board (number 71874075) at Southern Medical University in China before the start of the survey and was in accordance with the ethical standards of the responsible committee on human research of our institution and with the Helsinki Declaration. We have also adhered to standard bio-security and institutional safety procedures. In the preparation period, all investigators have been trained to ensure that they use the same instructions and provide assistance or clarification to participants if needed, so as to guarantee the quality of data collection. Meanwhile, we communicated with the persons-in-charge of the above six hospitals and were approved to conduct research in their institution. Furthermore, before participating in this study, all participants had been informed of the aim of the current study and the nature of voluntary participation. Subjects who agreed to take part in were directed to fill out the questionnaire anonymously in the waiting area.
Measures
The socio-demographic features, personality characteristics, social supports, coping styles, and depressive and anxiety information were gathered using questionnaires. The gathered socio-demographic feature covered age, education level of the pregnant women and their husbands, and monthly household income.
Personality Characteristics
The Chinese version of the Eysenck Personality Questionnaire-Revised Short Form [EPQ-RS; (58)] was used to measure the personality characteristics of the participants. The EPQ-RS was translated from the English-version questionnaire (59). It is comprised of 48 items and assesses the three subscales of P, E, and N, and L was additionally used to measure dissimulation and provide a validity scale. Responses were scored 0 or 1, and some items were reverse-scored. Therefore, the scores of each subscale (P, E, N) ranged from 0 to 12, with higher scores demonstrating higher levels of each personality characteristic. The EPQ-RS has been widely used in China and has acceptable reliability and validity (60, 61). The Cronbach's α coefficient for the subscales were 0.72 (P), 0.79 (N), and 0.76 (E) in this study.
Perceived and Used Social Support
Social support was measured by the Social Support Rating Scale [SSRS; (62)]. The SSRS was specially designed for utilization in the Chinese context. It includes 10 items with three dimensions: objective support (three items), subjective support (fur items), and support utilization (three items). As objective support had less determinative and valuable role on emotional distress (33), it was not included in the present study. The scores of subjective support ranged from 8 to 32, and support utilization scores ranged from 3 to 12. The higher the scores, the higher the level of social support. The SSRS has been widely used among pregnant women in China and has high reliability and validity (35). The Cronbach's α was 0.73 for subjective support and 0.71 for support utilization in the present study.
Positive Coping
The Chinese version of the Simplified Coping Style Questionnaire [SCSQ; (63)] was employed to measure coping tendencies of pregnant women. The SCSQ was modified by Xie according to the Chinese context, on the basis of the Ways of Coping Questionnaire (64). It includes 20 items and two dimensions: positive coping style (12 items) and negative coping style (8 items). Positive coping style emphasizes active coping characteristics, such as engagement in activities, planning, and talking to others, while negative coping style emphasizes the features of passive coping, such as substance use, relying on others, and fantasy. Agreement with each statement is assessed on a three-point Likert-type scale ranging from 0 (none) to 3 (always). The total scores for positive coping and negative coping were calculated separately, with a higher score representing a more frequent utilization of the corresponding coping style. The SCSQ has reported to have good reliability among Chinese pregnant women (65). The Cronbach's alpha was 0.89 for positive coping and 0.70 for negative coping in the present study.
Depressive Symptoms
The depressive symptom over the past week was assessed by the Chinese version of the Edinburgh Postnatal Depression Scale [EPDS; (66)], which was translated from the English version (67). The EPDS contains 10 self-rating items. Agreement with each statement is measured on a four-point Likert-type scale ranging from 0 (none) to 3 (yes, most of the time). Add all the answers together for a total score, and the higher the score, the higher the level of depressive symptoms. It showed good validity and reliability among Chinese pregnant women (68). In the present study, the Cronbach's α was 0.75.
Anxiety Symptoms
The anxiety symptom over the past week was measured through the Chinese version of the Self-Rating Anxiety scale [SAS; (69)]. The SAS was modified from the English-version scale (70). It is a 20-item self-rating instrument, and responses to the items were scored from 1 (none) to 4 (most or all of the time). All the responses were summed up to generate a total score (ranging from 20 to 80). The higher the score, the higher the level of anxiety symptoms. The SAS has been widely adopted among Chinese pregnant samples and has high validity and reliability (5, 71). In this study, the Cronbach's alpha was 0.76.
SES
The SES factors in the current study included education degree of pregnant women, education degree of the husband, and monthly household income (46, 72). Pregnant women were asked to report the education level of themselves and their husbands from 1 to 4 (1 = 9 years of education or below junior middle-school studies, 2 = 12 years of or senior middle-school studies, 3 = 14–15 years of education or 2–3-year college studies, 4 = 16 years of education or over bachelor's degree). Women also reported their monthly household income as either >10,000 yuan, 5,000–9,999 yuan, 3,000–4,999 yuan, or <2,999 yuan, scored as 1–4. The responses to these three questions were added up to generate the total score. Then, according to the median segmentation, the total scores of SES were recorded as a dichotomous variable [high SES group and low SES group; (72)].
Controlling Variables
Controlling variables included the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy, which were reported to influence the emotional distress of pregnant women (73, 74). The former three variables were dummy coded (1 = ever having pregnancy experience, 0 = in the first pregnancy; 1 = having adverse pregnancy experience, 0 = not having adverse pregnancy experience; 1 = unplanned pregnancy, 0 = planned pregnancy), and the number of weeks of pregnancy was a continuous variable. Among the sample in the present study, 688 (59.5%) reported to have pregnancy experience ever and 469 women (40.5%) were in their first pregnancy. Ninety-one women (7.9%) reported to have adverse pregnancy experience, while 1,066 (92.1%) had not. Three hundred one women (26.0) were pregnant as planned, and 856 (74.0%) had unintended pregnancies. The mean pregnancy duration was 27.15 weeks (SD = 9.50, range 6–40 weeks).
Statistical Analysis
Statistical analyses were performed using SPSS 23.0 and AMOS 23.0. Firstly, the data were screened for outliers and to measure the linearity and normality. An absolute skew value below 2 is considered to be within the acceptable range of normality (75). Then, we performed descriptive statistics of the study variables. Furthermore, we performed Pearson correlation analysis to examine the relationships among continuous variables and point-biserial correlation to test the associations between dichotomous variables and continuous variables.
Later, structural equation modeling (SEM) with AMOS 23.0 was adopted to test the potential chain mediating effect assumptions. To decrease collinearity, we mean-centered all continuous variables in the present study. The maximum likelihood estimation method was selected and used for the SEM. According to Wu (76), the overall model fit was assessed using several fit indexes. Specifically, we compared and selected models based on the ratio of χ2 to degrees of freedom (χ2/df) and on these fit indexes: the root mean square error of approximation (RMSEA), the incremental fit index (IFI), the normed fit index (NFI), and the Bentler comparative fit index (CFI). For χ2/df and RMSEA, values below 5 and 0.08 indicate an acceptable model fit separately. For IFI, NFI, and CFI, values over 0.90 indicate a good model fit. In the chain mediation analysis, bootstrapping was used to obtain confidence intervals (CIs) based on 10,000 samples (77).
Finally, we tested SES as the possible moderator of the chain mediating model using multigroup analysis. The SES was recorded into dichotomous variable by means of median splits. Based on Wu (78), the tests of differences in the SEM framework were as follows. Firstly, we tested the hypothesized structure without constraining any parameters in both groups at the same time (named baseline model or unconstrained model). If the baseline model was sufficiently fit, we forced some of the parameters (i.e., measurement residuals, measurement weights, and structural residuals) to be equal for the two groups (called constrained model) and compared the constrained model to the baseline model. If the statistical fit of the constrained model showed a significantly worse solution (the significant increase in χ2 value) than that of the unconstrained model, this indicated that at least one parameter was different between the groups. If multiple models fitted the data model, the final model was selected based on the indexes of Δχ2, AIC, and expected cross-validation index (ECVI).
In both the chain mediating effect test and the moderating test, four important variables (the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy) which might influence emotional distress of pregnant women (73, 74) were set as control variables.
Results
Descriptive Statistics and Univariate Correlations
Descriptive statistics for the study variables are displayed in Table 1. The skewness values of the study variables were all below 2, representing that they were not substantially skewed. Pregnant women's extraversion was positively related to positive coping and social support, while psychoticism and neuroticism were negatively related to these three variables. As expected, positive coping and social support were all negatively correlated with depressive and anxiety symptoms. Pregnant women's extraversion had a negative association with depression and anxiety symptoms, while psychoticism and neuroticism had a positive relationship. The degree of these correlations ranged from mild to moderate. However, negative coping did not significantly correlate with extraversion, subjective support, or support utilization. Therefore, negative coping was excluded in the following mediating and moderation analysis.
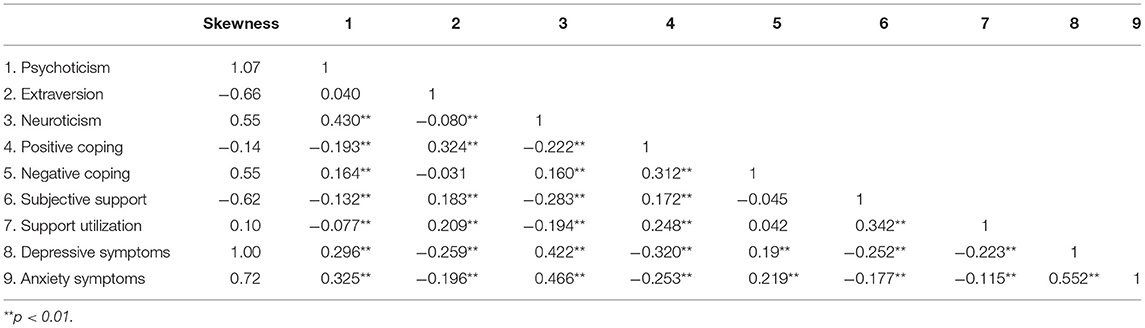
Table 1. Univariate correlations of study variables (N = 1157).
Chain Mediating Effects of Social Support and Positive Coping
We first checked the chain mediating effects of social support and positive coping in the relationship between personality characteristics and depressive symptoms. In order to induce the collinearity, we mean-centered all variables. After controlling for the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy, the associations between psychoticism and social support as well as between neuroticism and positive coping were not significant (ps > 0.05). Therefore, we deleted these two links from the mediating model. Then, the overall fitting index showed that the fitting between the model and the data were acceptable (χ2/df = 4.206; RMSEA = 0.053, 90% CI: 0.043, 0.062; CFI = 0.927, NFI = 0.909, IFI = 0.929). Furthermore, results indicated that neuroticism had a negative association with social support, while extraversion had a significant positive association. Pregnant women's extraversion was positively related to positive coping, while psychoticism was negatively related. Pregnant women's social support and positive coping correlated negatively with depressive symptoms. Meanwhile, social support was positively correlated with their positive coping.
The direct paths from psychoticism, extraversion, and neuroticism to depression were all significant (standardized direct effect = 0.133, 90% BCIs: 0.078, 0.191; −0.150, 90% BCIs: −0.204, −0.099; 0.245, 90% BCIs: 0.182, 0.308). Furthermore, all three personality characteristics correlated significantly and indirectly with depressive symptoms (standardized indirect effect = 0.018, 90% BCIs: 0.009, 0.030; −0.098, 90% BCIs: −0.129, −0.071; 0.086, 90% BCIs: 0.053, 0.130). Furthermore, extraversion and neuroticism correlated significantly and indirectly with positive coping (standardized indirect effect = 0.085, 90% BCIs: 0.053, 0.122; −0.106, 90% BCIs: −0.143, −0.074). Social support also correlated significantly and indirectly with depressive symptoms (standardized indirect effect = −0.033, 90% BCIs: −0.053, −0.017). These indicated that social support and positive coping acted as chain mediators among the relationship of personality and depressive symptoms (Figure 1).
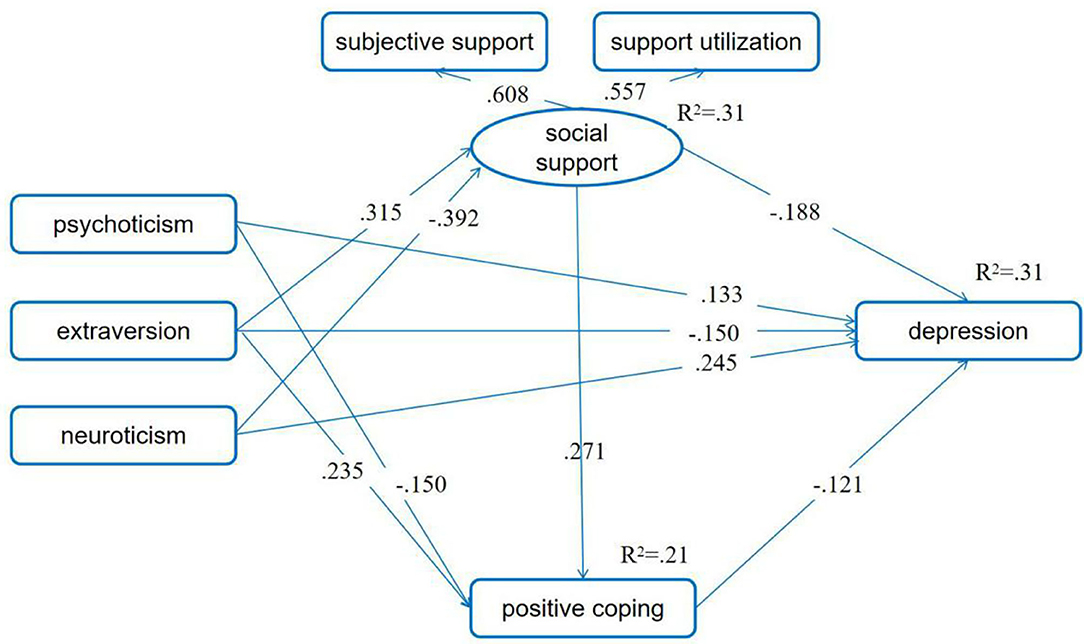
Figure 1. Positive coping and social support as chain mediators between personality and depressive symptoms. Standardized path coefficients are presented in the model (ps < 0.05). The first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy were set as control variables.
We then checked the mediating effect of social support and positive coping in the relationship between personality and anxiety symptoms. After controlling for the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy, the results indicated that the associations between social support and anxiety symptoms, between psychoticism and social support, and between neuroticism and positive coping were not significant (p > 0.05). Therefore, we delete these three links. Then, the fitting indexes indicated that the fitting between the model and the data was acceptable (χ2/df = 4.106; RMSEA = 0.052, 90% CI = 0.043, 0.062; CFI = 0.926, NFI = 0.907, IFI = 0.928). Meanwhile, the results showed that neuroticism had a negative association with social support, while extraversion had a significant positive association. Pregnant women's extraversion was positively related to positive coping, while psychoticism was negatively related. Pregnant women's positive coping correlated negatively with depressive symptoms. Meanwhile, social support was positively correlated with their positive coping.
The direct paths from psychoticism, extraversion, and neuroticism to depression were all significant (standardized direct effect = 0.146, 90% BCIs: 0.094, 0.200; −0.149, 90% BCIs: −0.200, −0.098; 0.369, 90% BCIs: 0.320, 0.414). Furthermore, all three personality characteristics correlated significantly and indirectly with depressive symptoms (standardized indirect effect = 0.013, 90% BCIs: 0.006, 0.023; −0.029, 90% BCIs: −0.046, −0.012; 0.009, 90% BCIs: 0.004, 0.017). Furthermore, extraversion and neuroticism correlated significantly and indirectly with positive coping (standardized indirect effect = 0.085, 90% BCIs: 0.057, 0.122; −0.106, 90% BCIs: −0.143, −0.073). Social support also correlated significantly and indirectly with depressive symptoms (standardized indirect effect = −0.024, 90% BCIs: −0.041, −0.011). These suggested that social support and positive coping acted as chain mediators on the relationship of personality and anxiety symptoms (Figure 2).
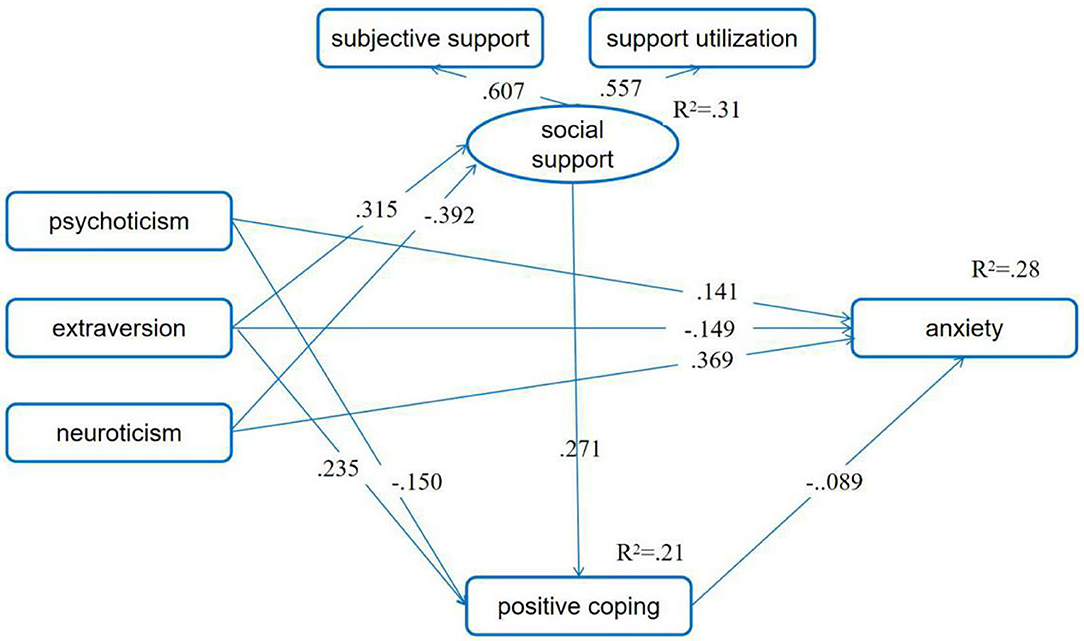
Figure 2. Positive coping as mediator between personality and anxiety symptoms. Standardized path coefficients are presented in the model (ps < 0.05). The first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy were set as control variables.
Moderating Effect of SES: Multigroup Analysis
In order to examine whether the associations between personality and emotional distress found in the whole participant samples are also applicable to the high SES and low SES subgroups, we conducted the multigroup analysis. We also controlled for the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy in the following multigroup analysis.
For the moderating effect of SES in the relationship between personality and depressive symptoms, the unconstrained model and the measurement weight model fit the data well. Although the values of CFI, NFI, and IFI for the structural covariance model and the measurement residual model were < 0.90, the other indexes were good. These suggested that the hypothesized four models were acceptable. We selected the measurement weight model as the final model according to the values of χ2, AIC, and ECVI. Then, we compared path coefficients for women with low SES and those with high SES one by one and found that there were no significant differences between all the path coefficients for the two groups (ps > 0.05). Results of these indicated that the chain meditating model of social support and positive coping in the association between personality and depressive symptoms demonstrated invariance across SES (Figure 3; Table 2).
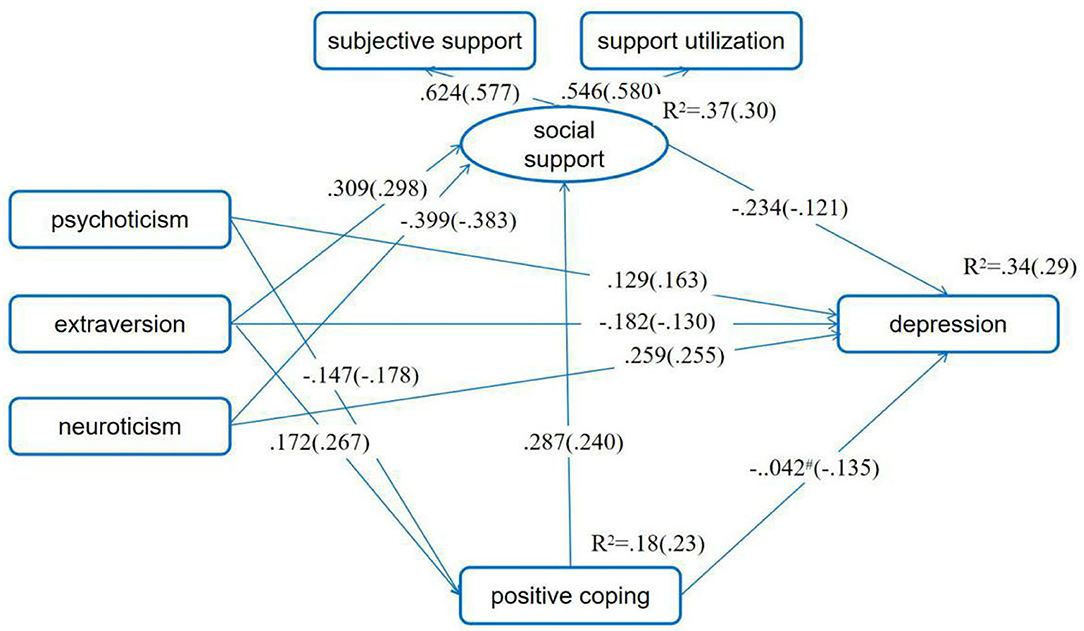
Figure 3. SES as moderator in the chain mediating model of positive coping and social support in the association between personality and depressive symptoms. Standardized path coefficients before parentheses were for the low SES group, and those in the parentheses were for the high SES group. #p > 0.05, while the p-values for other standardized path coefficient were all <0.05. The first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy were set as control variables.
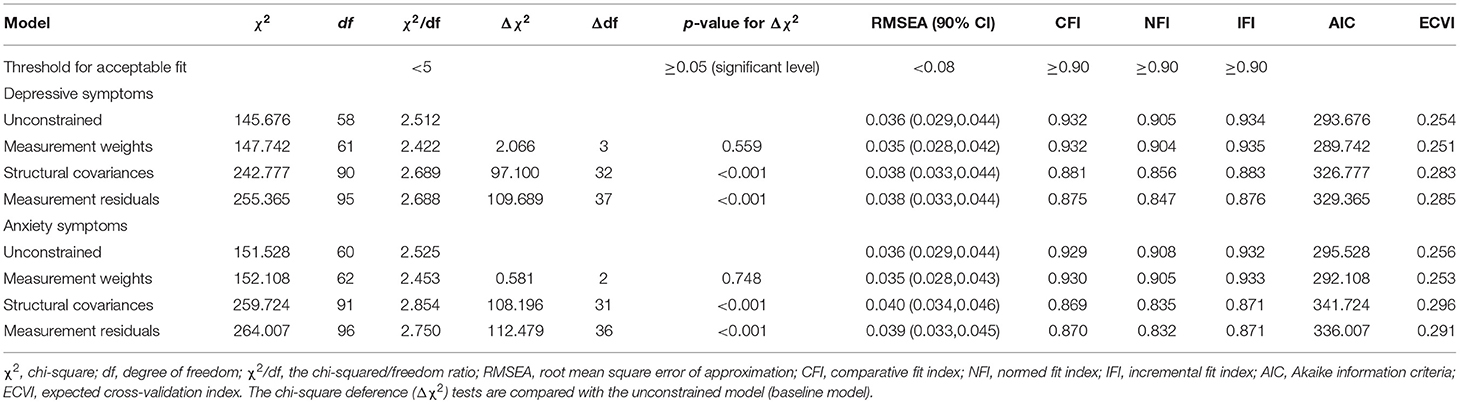
Table 2. Goodness-of-fit indices for model comparisons in moderation analysis on the mediation model.
Concerning the proposed moderating effect of SES in the mediating model of the relationship between personality and anxiety, results showed that both the unconstrained model and the measurement weight model fit the data well. Although the values of CFI, NFI, and IFI for the structural covariance model and the measurement residual model were below 0.90, the other indexes were good. These indicated that the hypothesized models were acceptable. We also selected the measurement weight model as the final model based on the values of χ2, AIC, and ECVI. Through comparing path coefficients for women with low and high SES, we found that the relationship between positive coping and anxiety was not significant for low SES women (standardized direct effect = 0.033, 90% BCIs: −0.061, 0.133, p = 0.455) but was significant for high SES women (standardized direct effect = −0.119, 90% BCIs: −0.191, −0.043, p < 0.001), and the difference in the pathways was significant (t = −2.652, p < 0.01). These suggested that the negative association between positive coping and anxiety symptoms was weaker for pregnant women with low SES than for those with high SES (Figure 4; Table 2).
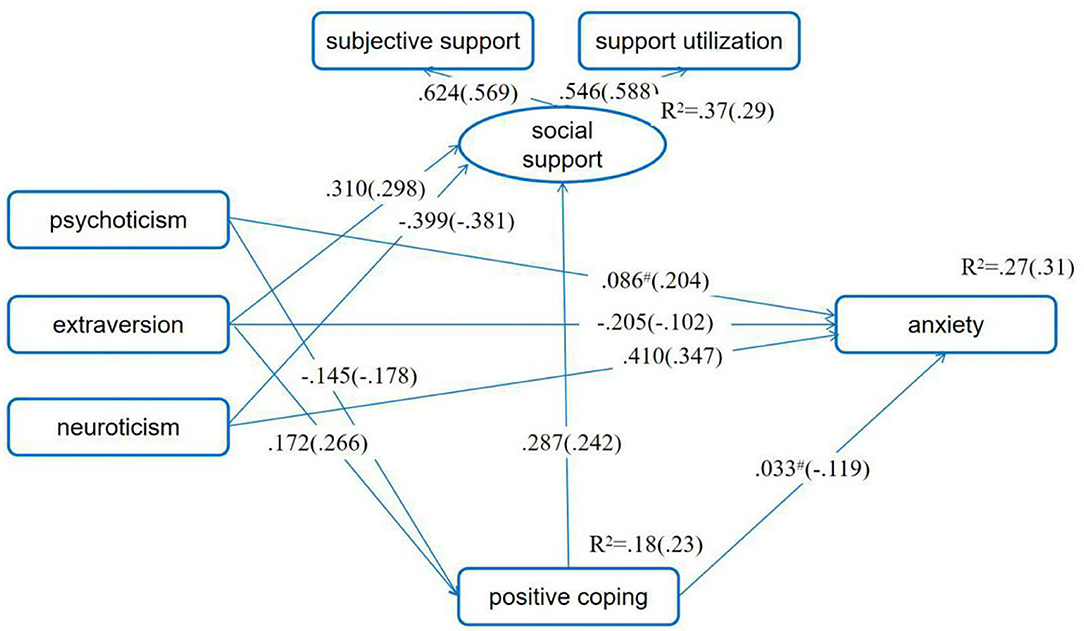
Figure 4. SES as moderator in the mediating model of positive coping in the association between personality and anxiety symptoms. Standardized path coefficients before parentheses were for the low SES group, and those in the parentheses were for the high SES group. #p > 0.05, while the p-values for other standardized path coefficient were all <0.05. The first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy were set as control variables.
Discussion
In line with the relationship hypothesis (H1), the present study indicated that personality characteristics correlated moderately or mildly with depressive and anxiety symptoms among Chinese pregnant women. Also consistent with the mediating hypothesis (H2), after controlling for four important variables (the first pregnancy or not, having adverse pregnancy experience or not, being pregnant as planned or not, and number of weeks of pregnancy), social support and positive coping acted as chain mediators on the link between personality and depressive symptoms as well as between personality and anxiety. As predicted (H3: the moderating hypothesis), SES played a moderating role in the chain mediating model of personality and anxiety symptoms. Specifically, the negative link between positive coping and anxiety symptoms was weaker for low SES women than for high SES ones. However, inconsistent with the assumption, the chain mediating effects of social support and positive coping on the link of personality and depressive symptoms demonstrated invariance across SES.
In light of pregnant women's emotional distress becoming more common (3, 79), our findings indicate that positive coping style and subjective and utilization of support are important mediators on the relationship between personality and emotion among Chinese pregnant women. Furthermore, the mediating effect of positive coping was non-existent in the anxiety model among low SES pregnant women. Therefore, more attention should be paid to the anxiety symptom experienced by this specific group.
In accordance with past research (16, 22), there were positive associations for psychoticism and neuroticism with emotional distresses as well as negative associations for extraversion with emotional distresses among pregnant women. These indicated that when pregnant women had high levels of psychoticism or neuroticism, they were more likely to become depressed and anxious. However, if the pregnant women had high levels of extraversion, they tended to experience less depression and anxiety symptoms. These above results suggest that improving the extroversion and reducing psychoticism and neuroticism are helpful to alleviate the anxiety and depressive symptoms of pregnant women. Furthermore, as personality characteristics are formed in the early years of life and are relatively stable in adulthood (80), it is relatively difficult to adjust them to substantially decrease the likelihood of emotional distress among adult pregnant women. Therefore, it is critical to study the mediators and moderators in the relationships between personality and emotional distress and to provide empirical evidence for the intervention of depressive and anxiety symptoms during pregnancy.
Although empirical findings link personality characteristics and depression symptoms in pregnancy, little attention has been paid to how to explain these relationships in the literature. In the present study, we assessed whether social support and positive coping may explain these associations. Taken together, we found significant chain mediating effects of social support and positive coping on the associations of personality characteristics and depressive symptoms as well as of personality and anxiety. Specifically, when pregnant women were lower in psychoticism and neuroticism, and higher in extraversion, they were more likely to have high levels of social support and/or positive coping, which correlated negatively with depression and anxiety symptoms. This is consistent with past research (42, 43). Results of these are also in line with the psychosocial theory (81). Notably, in this chain mediating model, the psychoticism was not directly related to social support and neuroticism was not directly related to positive coping.
More importantly, to our knowledge, the present study was the first to explore whether SES could moderate the mediated effects of personality characteristics on emotional distress through social support and positive coping. Inconsistent with the assumption, we did not find the moderating effect of SES on the association of personality with depressive symptoms among pregnant women. In other words, the relationships of personality characteristics to emotional distress through social support and positive coping did not vary with SES. This expands the past literature and supports the important roles of both social support and positive coping on alleviating the personality-related depressive symptoms for pregnant women.
Findings from the present study indicated that the negative link between positive coping and anxiety symptoms was weaker for low SES women than for high SES ones. These are consistent with the stress-buffering model (55). In comparison of high SES individuals, those with low SES typically had limited resources [such as receiving less meritorious information and advice as well as obtaining less frequent technological and material assistance; (82, 83)], which might be insufficient to promote the effect of positive coping on personality-influenced emotional distress. Furthermore, individuals with low SES experience more stress than those with high SES backgrounds (84) and stress is linked with emotional distress and other negative outcomes (85). This may mean that low SES pregnant women may suffer more stressful events and have fewer resources. Furthermore, the unexpected null findings in pregnant women with low SES might imply that other unmeasured resilience factors for anxiety symptom associated with the low SES, such as sense of control and life-meaning, may have played more contributory roles than the positive coping.
Furthermore, these results might be explained by the differences in personality characteristics between women with high SES and women with low SES. Women with low SES typically had higher levels of neuroticism, such as lower emotional stability, than high SES women (52). Therefore, for pregnant women with the same level of positive coping, those with low SES would be less likely to relieve the negative relationships of their psychoticism and neuroticism and anxiety, as well as promote the positive association between their extraversion and anxiety symptom. As the latest study stated, pregnancy-specific anxiety, the condition marked by worries, concerns and fears about pregnancy, childbirth, the health of the infant, and future parenting, is an under-recognized area and deserves more attention (86). Findings in the present study also suggest that more research into the associations between personality characteristics and anxiety symptom in low SES pregnant women is urgently called for, especially on the alleviation of the links between negative personality characteristics (psychoticism and neuroticism) and anxiety, and the enhancement of the positive links between positive personality characteristics (extraversion) and anxiety symptom.
Limitations and Conclusions
The current study also has some limitations. First, we relied on self-reports to measure the main constructs. The observations and holistic assessments of various aspects of life among pregnant women are needed to confirm and enhance the current findings. Further studies could also benefit from qualitative interviews to investigate correlations between personality and emotional distress in a more nuanced approach. Second, as with past cross-sectional surveys, the results of the present study could not offer time series or clear causal conclusion. Thus, longitudinal studies are necessary to evaluate potential etiological relationships between personality, coping, support, and emotional distress among pregnant women. Third, the psychiatric assessment was missing in the present study. In future studies, psychiatric assessments should be included to assess and exclude subjects with psychiatric disorders, as psychiatric disorders may affect self-reporting of personality traits. Furthermore, it should be noted that the pregnant women in this study were all from Guangdong province, a relatively developed province in China. Therefore, the moderating role of SES requires to be assessed among pregnant women in relatively poor provinces in China. Finally, the associations between personality and pregnant women's depressive and anxiety symptoms in the present study were relatively mild. However, since personality characteristics have a prolonged effect on each individual's emotion, the mild links found may have a crucial practical impact on pregnant women over time.
Despite these limitations, this study expands the literature on the direct associations of personality characteristics and emotional distress among pregnant women in China. Wu also found that personality characteristics correlate indirectly with emotion through the buffering effect of social support and positive coping. That is, social support and positive coping can serve as beneficial factors on the relationship between personality and emotional distress (depressive and anxiety symptoms) among pregnant women. Furthermore, the chain mediating effects of social support and positive coping on the link of personality characteristics and anxiety varied according to SES. Specifically, for pregnant women with low SES, studies on the impact of other mediators, such as sense of control and life-meaning, on the link between personality characteristics and anxiety symptom are needed. As such, this study highlights the need to comprehensively consider both social support and coping style to prevent depressive and anxiety symptoms among Chinese pregnant women.
The present study has theoretical and practical implications. It contributes to better understandings of how pregnant women's personality characteristics are related to their emotional distress and might increase the possibility of a positive pregnancy experience. This study has also helped to better understand the buffering effects of social support and positive coping in the personality–emotional distress associations. Furthermore, these results are crucial for those who play an important role in women's pregnancy experiences, such as doctors, nurses, and psychotherapists. The results of the current study could also be used to develop clinical intervention and management programs for emotional distress in pregnant women. For instance, for pregnant women with high levels of depressive and anxiety symptoms, training in coping styles and perceiving and using support might help alleviate symptoms of pregnant women.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by the Ethical Review Board of Institute, Southern Medical University. The participants provided their written informed consent to take part in this study.
Author Contributions
YC: study design. WY, FF, JX, and JW: data collection. YH: data analysis. YH, WY, and YC: manuscript preparation. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Natural Science Foundation of China [No. 71874075] and Humanities and Social Sciences of Ministry of Education [No. 18YJAZH008].
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all participants in this study.
References
1. Friedman LE, Gelaye B, Sanchez SE, Williams MA. Association of social support and antepartum depression among pregnant women. J Affect Disord. (2020) 264:201–5. doi: 10.1016/j.jad.2019.12.017
2. Dennis CL, Falah-Hassani K, Shiri R. Prevalence of antenatal and postnatal anxiety: systematic review and meta-analysis. Br J Psychiatry. (2017) 210:315–23. doi: 10.1192/bjp.bp.116.187179
3. Gelaye B, Rondon MB, Araya R, Williams MA. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry. (2016) 3:973–82. doi: 10.1016/S2215-0366(16)30284-X
4. Ferreira CR, Orsini MC, Vieira CR, do Amarante Paffaro AM, Silva RR. Prevalence of anxiety symptoms and depression in the third gestational trimester. Arch Gynecol Obstet. (2015) 291:999–1003. doi: 10.1007/s00404-014-3508-x
5. Ma X, Wang Y, Hu H, Tao XG, Zhang Y, Shi H. The impact of resilience on prenatal anxiety and depression among pregnant women in Shanghai. J Affect Disord. (2019) 250:57–64. doi: 10.1016/j.jad.2019.02.058
6. Yu Y, Li M, Pu L, Wang S, Wu J, Ruan L, et al. Sleep was associated with depression and anxiety status during pregnancy: a prospective longitudinal study. Arch Women's Ment Health. (2017) 20:695–701. doi: 10.1007/s00737-017-0754-5
7. Martínez-Borba V, Suso-Ribera C, Osma J, Andreu-Pejó L. Predicting postpartum depressive symptoms from pregnancy biopsychosocial factors: a longitudinal investigation using structural equation modeling. Int J Environ Res Public Health. (2020) 17:8445. doi: 10.3390/ijerph17228445
8. Howard LM, Khalifeh H. Perinatal mental health: a review of progress and challenges. World Psychiatry. (2020) 19:313–27. doi: 10.1002/wps.20769
9. Glover V. Prenatal mental health and the effects of stress on the foetus and the child. Should psychiatrists look beyond mental disorders? World Psychiatry. (2020) 19:331–2. doi: 10.1002/wps.20777
10. Ritchie-Ewing G, Mitchell AM, Christian LM. Associations of maternal beliefs and distress in pregnancy and postpartum with breastfeeding initiation and early cessation. J Hum Lact. (2019) 35:49–58. doi: 10.1177/0890334418767832
11. Pearson RM, Carnegie RE, Cree C, Rollings C, Rena-Jones L, Evans J, et al. Prevalence of prenatal depression symptoms among 2 generations of pregnant mothers: the Avon longitudinal study of parents and children. JAMA Netw Open. (2018) 1:e180725. doi: 10.1001/jamanetworkopen.2018.0725
12. Rees S, Channon S, Waters CS. The impact of maternal prenatal and postnatal anxiety on children's emotional problems: a systematic review. Eur Child Adolesc Psychiatry. (2019) 28:257–80. doi: 10.1007/s00787-018-1173-5
13. Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. (2016) 191:62–77. doi: 10.1016/j.jad.2015.11.014
14. Brunton R, Dryer R. Child sexual abuse and pregnancy: a systematic review of the literature. Child Abuse Neglect. (2020) 111:104802. doi: 10.1016/j.chiabu.2020.104802
15. Steardo L Jr, Caivano V, Sampogna G, Di Cerbo A, Fico G, Zinno F, et al. Psychoeducational intervention for perinatal depression: study protocol of a randomized controlled trial. Front Psychiatry. (2019) 10:55. doi: 10.3389/fpsyt.2019.00055
16. Andreu-Pejó L, Martínez-Borba V, Suso-Ribera C, Osma J. Can we predict the evolution of depressive symptoms, adjustment, and perceived social support of pregnant women from their personality characteristics? a technology-supported longitudinal study. Int J Environ Res Public Health. (2020) 17:3439. doi: 10.3390/ijerph17103439
17. Zeng Y, Cui Y, Li J. Prevalence and predictors of antenatal depressive symptoms among Chinese women in their third trimester: a cross-sectional survey. BMC Psychiatry. (2015) 15:66. doi: 10.1186/s12888-015-0452-7
18. Barrett PT, Petrides KV, Eysenck SB, Eysenck HJ. The Eysenck personality questionnaire: an examination of the factorial similarity of P, E, N, and L across 34 countries. Pers Individ Dif. (1998) 25:805–19. doi: 10.1016/S0191-8869(98)00026-9
19. Goldberg LR. An alternative “description of personality”: the big-five factor structure. J Pers Soc Psychol. (1990) 59:1216–29. doi: 10.1037//0022-3514.59.6.1216
20. Corr PJ. Reinforcement sensitivity theory of personality questionnaires: structural survey with recommendations. Pers Individ Dif. (2016) 89:60–4. doi: 10.1016/j.paid.2015.09.045
21. Canals J, Espar ó G, Fernández-Ballart JD. How anxiety levels during pregnancy are linked to personality dimensions and sociodemographic factors. Pers Individ Diff. (2002) 33, 253–259. doi: 10.1016/S0191-8869(01)00149-0
22. Bunevicius R, Kusminskas L, Bunevicius A, Nadisauskiene RJ, Jureniene K, Pop VJ. Psychosocial risk factors for depression during pregnancy. Acta Obstet Gynecol Scand. (2009) 88:599–605. doi: 10.1080/00016340902846049
23. Roman M, Bostan CM, Diaconu-Gherasim LR, Constantin T. Personality traits and postnatal depression: the mediated role of postnatal anxiety and moderated role of type of birth. Front Psychol. (2019) 10:1625. doi: 10.3389/fpsyg.2019.01625
24. Brunton R, Wood T, Dryer R. Childhood abuse, pregnancy-related anxiety and the mediating role of resilience and social support. J Health Psychol. (2020) 6:1359105320968140. doi: 10.1177/1359105320968140
25. Degirmenci F, Vefikuluçay Yilmaz D. The relationship between psychosocial health status and social support of pregnant women. J Psychosom Obstet Gynecol. (2019) 41:290–7. doi: 10.1080/0167482X.2019.1678021
26. Nath A, Venkatesh S, Balan S, Metgud CS, Krishna M, Murthy GVS. The prevalence and determinants of pregnancy-related anxiety amongst pregnant women at less than 24 weeks of pregnancy in Bangalore, Southern India. Int J Women's Health. (2019) 11:241–8. doi: 10.2147/IJWH.S193306
27. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. (1988) 52:30–41. doi: 10.1207/s15327752jpa5201_2
28. Huang LL. Interpersonal harmony and conflict for chinese people: a yin-yang perspective. Front Psychol. (2016) 7:847. doi: 10.3389/fpsyg.2016.00847
29. Tang X, Lu Z, Hu D, Zhong X. Influencing factors for prenatal Stress, anxiety and depression in early pregnancy among women in Chongqing, China. J Affect Disord. (2019) 253:292–302. doi: 10.1016/j.jad.2019.05.003
30. Yu M, Qiu T, Liu C, Cui Q, Wu H. The mediating role of perceived social support between anxiety symptoms and life satisfaction in pregnant women: a cross-sectional study. Health Qual Life Outcomes. (2020) 18:203. doi: 10.1186/s12955-020-01479-w
31. Yue C, Liu C, Wang J, Zhang M, Wu H, Li C, et al. Association between social support and anxiety among pregnant women in the third trimester during the coronavirus disease 2019 (COVID-19) epidemic in Qingdao, China: The mediating effect of risk perception. Int J Soc Psychiatry. (2020) 67:120–7. doi: 10.1177/0020764020941567
32. Xiao SY. The theoretical basis and application of social support questionnaire. J Clin Psychol Med. (1994) 4:98–100.
33. Santini ZI, Koyanagi A, Tyrovolas S, Mason C, Haro JM. The association between social relationships and depression: a systematic review. J Affect Disord. (2015) 175:53–65. doi: 10.1016/j.jad.2014.12.049
34. Swickert R. Personality and social support processes. In: Corr PJ, Matthews G, editors. The Cambridge Handbook of Personality Psychology. New York, NY: Cambridge University Press (2012). p. 524–540.
35. Zhou J, Feng L, Hu C, Pao C, Xiao L, Wang G. Associations among depressive symptoms, childhood abuse, neuroticism, social support, and coping style in the population covering general adults, depressed patients, bipolar disorder patients, and high risk population for depression. Front Psychol. (2019) 10:1321. doi: 10.3389/fpsyg.2019.01321
36. Lv H., Tao H., Wang Y., Zhao Z., Liu G., Li L., et al. Impact of type D personality on major adverse cardiac events in patients undergoing percutaneous coronary intervention: the mediating role of cognitive appraisal and coping style. J Psychosom Res. (2020) 136:110192. doi: 10.1016/j.jpsychores.2020.110192
37. Folkman S, Moskowitz JT. Coping: Pitfalls and promise. Annu Rev Psychol. (2004) 55:745–74. doi: 10.1146/annurev.psych.55.090902.141456
38. Gutiérrez-Zotes A, Labad J, Martín-Santos R, García-Esteve L, Gelabert E, Jover M, et al. Coping strategies and postpartum depressive symptoms: a structural equation modelling approach. Eur Psychiatry. (2015) 30:701–8. doi: 10.1016/j.eurpsy.2015.06.001
39. Shamsaei F, Maleki A, Shobeiri F, Soltani F, Ahmadi F, Roshanaei G. The relationship between general health and coping style with perceived stress in primigravida healthy pregnant women: using the PATH model. Women Health. (2019) 59:41–54. doi: 10.1080/03630242.2018.1434587
40. De Tychey C, Spitz E, Briançon S, Lighezzolo J, Girvan F, Rosati A, et al. Pre-and postnatal depression and coping: a comparative approach. J Affect Disord. (2005) 85:323–6. doi: 10.1016/j.jad.2004.11.004
41. Kim MY, Johnson JL, Sawatzky R. Relationship between types of social support, coping strategies, and psychological distress in individuals living with congenital heart disease. J Cardiovasc Nurs. (2019) 34:76–84. doi: 10.1097/JCN.0000000000000531
42. Ren J, Jiang X, Yao J, Li X, Liu X, Pang M, et al. Depression, social support, and coping styles among pregnant women after the Lushan Earthquake in Ya'an, China. PLoS ONE. (2015) 10:e0135809. doi: 10.1371/journal.pone.0135809
43. Zhang X, Li JH, Wang J, Li J, Long ZT, Cao FL. Childhood neglect and psychological distress among pregnant women: the chain multiple mediation effect of perceived social support and positive coping. J Nerv Ment Dis. (2020) 208:764–70. doi: 10.1097/NMD.0000000000001210
44. Atif N, Nazir H, Zafar S, Chaudhri R, Atiq M, Mullany LC, et al. Development of a psychological intervention to address anxiety during pregnancy in a low-income country. Front Psychiatry. (2019) 10:927. doi: 10.3389/fpsyt.2019.00927
45. McEachan RRC, Prady SL, Smith G, Fairley L, Cabieses B, Gidlow C, et al. The association between green space and depressive symptoms in pregnant women: moderating roles of socioeconomic status and physical activity. J Epidemiol Commun Health. (2016) 70:253–9. doi: 10.1136/jech-2015-205954
46. Verbeek T, Bockting CL, Beijers C, Meijer JL, van Pampus MG, Burger H. Low socioeconomic status increases effects of negative life events on antenatal anxiety and depression. Women Birth. (2019) 32:e138–43. doi: 10.1016/j.wombi.2018.05.005
47. Stewart RC, Umar E, Tomenson B, Creed F. A cross-sectional study of antenatal depression and associated factors in Malawi. Arch Women's Ment Health. (2014) 17:145–54. doi: 10.1007/s00737-013-0387-2
48. Bright KS, Norris JM, Letourneau NL, King Rosario M, Premji SS. Prenatal maternal anxiety in South Asia: a rapid best-fit framework synthesis. Front Psychiatry. (2018) 9:467. doi: 10.3389/fpsyt.2018.00467
49. Katz J, Crean HF, Cerulli C, Poleshuck EL. Material hardship and mental health symptoms among a predominantly low income sample of pregnant women seeking prenatal care. Matern Child Health J. (2018) 22:1360–7. doi: 10.1007/s10995-018-2518-x
50. Faisal-Cury A, Menezes PR. Prevalence of anxiety and depression during pregnancy in a private setting sample. Arch Women's Mental Health. (2007) 10:25–32. doi: 10.1007/s00737-006-0164-6
51. Abuidhail J, Abujilban S. Characteristics of Jordanian depressed pregnant women: a comparison study. J Psychiatr Ment Health Nurs. (2014) 21:573–9. doi: 10.1111/jpm.12125
52. Ayoub M, Gosling SD, Potter J, Shanahan M, Roberts BW. The relations between parental socioeconomic status, personality, and life outcomes. Soc Psychol Personal Sci. (2018) 9:338–52. doi: 10.1177/1948550617707018
53. Sutin AR, Luchetti M, Stephan Y, Robins RW, Terracciano A. Parental educational attainment and adult offspring personality: an intergenerational life span approach to the origin of adult personality traits. J Pers Soc Psychol. (2017) 113:144–66. doi: 10.1037/pspp0000137
54. Li JB, Delvecchio E, Lis A, Nie YG, Di Riso D. Positive coping as mediator between self-control and life satisfaction: Evidence from two Chinese samples. Pers Individ Dif. (2016) 97:130–3. doi: 10.1016/j.paid.2016.03.042
55. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
56. Milas G, Klarić IM, Malnar A, Šupe-Domić D, Slavich GM. Socioeconomic status, social-cultural values, life stress, and health behaviors in a national sample of adolescents. Stress Health. (2019) 35:217–24. doi: 10.1002/smi.2854
57. Glasscock DJ, Andersen JH, Labriola M, Rasmussen K, Hansen CD. Can negative life events and coping style help explain socioeconomic differences in perceived stress among adolescents? a cross-sectional study based on the West Jutland cohort study. BMC Public Health. (2013) 13:532. doi: 10.1186/1471-2458-13-532
58. Qian MY, Wu GC, Zhu RC, Zhang S. Revision of Eysenck Personality Questionnaire short scale for Chinese (EPQ-RSC). Acta Psychol Sin. (2000) 32:317–23.
59. Eysenck SB, Eysenck HJ, Barrett P. A revised version of the psychoticism scale. Pers Individ Dif. (1985) 6:21–9. doi: 10.1016/0191-8869(85)90026-1
60. Yao N, Qian M, Jiang Y, Elhai JD. The influence of intolerance of uncertainty on anxiety and depression symptoms in chinese-speaking samples: structure and validity of the chinese translation of the intolerance of uncertainty scale. J Pers Assess. (2020) 103:406–15. doi: 10.1080/00223891.2020.1739058
61. Li H, Zou Y, Wang J, Yang X. Role of stressful life events, avoidant coping styles, and neuroticism in online game addiction among college students: a moderated mediation model. Front Psychol. (2016) 7:1794. doi: 10.3389/fpsyg.2016.01794
63. Xie Y. The initial exploration of reliability and validity of simplified Coping Styles Questionnaire. Chin J Clin Psychol. (1998) 6:114–5.
64. Folkman S, Lazarus RS, Gruen RJ, DeLongis A. Appraisal, coping, health status, and psychological symptoms. J Pers Soc Psychol. (1986) 50:571–9. doi: 10.1037/0022-3514.50.3.571
65. Li Y, Zeng Y, Zhu W, Cui Y, Li J. Path model of antenatal stress and depressive symptoms among Chinese primipara in late pregnancy. BMC Pregnancy Childbirth. (2016) 16:180. doi: 10.1186/s12884-016-0972-2
66. Jin Y, Peng T, Wang L, Zhang Q. Screening criteria and pathogenic factors of postpartum depression. Maternal Child Health Care China. (1995) 10:32–3.
67. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
68. Mak JK, Lee AH, Pham NM, Tang L, Pan XF, Xu ZP, et al. Physical activity during early pregnancy and antenatal depression: a prospective cohort study. Ment Health Phys Act. (2019) 16:54–9. doi: 10.1016/j.mhpa.2019.04.003
70. Zung WW. A rating instrument for anxiety disorders. Psychosom J Consult Liaison Psychiatry. (1971) 12:371–379. doi: 10.1016/S0033-3182(71)71479-0
71. Dong H, Hu R, Lu C, Huang D, Cui D, Huang G, et al. Investigation on the mental health status of pregnant women in China during the Pandemic of COVID-19. Arch Gynecol Obstet. (2020) 303:463–9. doi: 10.1007/s00404-020-05805-x
72. Hou Y, Xiao R, Yang X, Chen Y, Peng F, Zhou S, et al. Parenting style and emotional distress among chinese college students: a potential mediating role of the zhongyong thinking style. Front Psychol. (2020) 11:1774. doi: 10.3389/fpsyg.2020.01774
73. Jairaj C, Fitzsimons CM, McAuliffe FM, O'Leary N, Joyce N, McCarthy A, et al. A population survey of prevalence rates of antenatal depression in the Irish obstetric services using the Edinburgh Postnatal Depression Scale (EPDS). Arch Women's Mental Health. (2019) 22:349–55. doi: 10.1007/s00737-018-0893-3
74. Wu Y., Zhang C., Liu H., Duan C., Li C., Fan J., et al. (2020). Perinatal depressive and anxiety symptoms of pregnant women along with COVID-19 outbreak in China. Am J Obstet Gynecol. 223:240–9. doi: 10.1016/j.ajog.2020.05.009
75. Kim HY. Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restor Dent Endodont. (2013) 38:52–4. doi: 10.5395/rde.2013.38.1.52
76. Wu M. Structural Equation Modeling: The Application of AMOS. Chong Qing: Chong Qing University Press (2009).
77. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
78. Wu M. Structural Equation Modeling: The Advancement of AMOS. Chong Qing: Chong Qing University Press (2013).
79. Woody CA, Ferrari AJ, Siskind DJ, Whiteford HA, Harris MG. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. (2017) 219:86–92. doi: 10.1016/j.jad.2017.05.003
80. Gustavsson JP, Weinryb RM, Göransson S, Pedersen NL, Åsberg M. Stability and predictive ability of personality traits across 9 years. Pers Individ Dif. (1997) 22:783–91. doi: 10.1016/S0191-8869(96)00268-1
81. Jeong HG, Lim JS, Lee MS, Kim SH, Jung IK, Joe SH. The association of psychosocial factors and obstetric history with depression in pregnant women: focus on the role of emotional support. Gen Hosp Psychiatry. (2013) 35:354–8. doi: 10.1016/j.genhosppsych.2013.02.009
82. Fingerman KL, Kim K, Davis EM, Furstenberg FF Jr, Birditt KS, Zarit SH. “I'll give you the world”: socioeconomic differences in parental support of adult children. J Marriage Fam. (2015) 77:844–65. doi: 10.1111/jomf.12204
83. Gallo LC, Bogart LM, Vranceanu AM, Matthews KA. Socioeconomic status, resources, psychological experiences, and emotional responses: a test of the reserve capacity model. J Pers Soc Psychol. (2005) 88:386–99. doi: 10.1037/0022-3514.88.2.386
84. Algren MH, Ekholm O, Nielsen L, Ersbøll AK, Bak CK, Andersen PT. Associations between perceived stress, socioeconomic status, and health-risk behaviour in deprived neighbourhoods in Denmark: a cross-sectional study. BMC Public Health. (2018) 18:250. doi: 10.1186/s12889-018-5170-x
85. Collin V, O'Selmo E, Whitehead P. Stress, psychological distress, burnout and perfectionism in UK dental students. Br Dent J. (2020) 229:605–14. doi: 10.1038/s41415-020-2281-4
Keywords: personality, depressive symptoms, anxiety symptoms, pregnant women, socioeconomic status (SES)
Citation: Yang W, Hou Y, Chen Y, Liu W, Fang F, Xiao J and Wang J (2021) Personality Characteristics and Emotional Distress Among Chinese Pregnant Women: A Moderated Mediation Model. Front. Psychiatry 12:645391. doi: 10.3389/fpsyt.2021.645391
Received: 23 December 2020; Accepted: 15 October 2021;
Published: 18 November 2021.
Edited by:
Giorgio Di Lorenzo, University of Rome Tor Vergata, ItalyReviewed by:
Jean Lillian Paul, Medizinische Universität Innsbruck, AustriaMario Luciano, University of Campania Luigi Vanvitelli, Italy
Copyright © 2021 Yang, Hou, Chen, Liu, Fang, Xiao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Chen, truelife2010@126.com
†These authors have contributed equally to this work