Corrigendum: Violent Behavior During Psychiatric Inpatient Treatment in a German Prison Hospital
 P. Seidel1
P. Seidel1 N. Konrad2
N. Konrad2 V. Negatsch2
V. Negatsch2 D. Dezsö2
D. Dezsö2 I. Kogan2U. Gauger2B. Neumann2
I. Kogan2U. Gauger2B. Neumann2 A. Voulgaris3†
A. Voulgaris3† A. Opitz-Welke2*†
A. Opitz-Welke2*†- 1Justizvollzugskrankenhaus, JVA Plötzensee, Berlin, Germany
- 2Institut für Forensische Psychiatrie, Charité, Berlin, Germany
- 3Institut für Sexualforschung und Forensische Psychiatrie, Universitätsklinikum Hamburg Eppendorf, Hamburg, Germany
Violent behavior in correctional facilities is common and differs substantially in type, target, implication, and trigger. Research on frequency and characteristics of violent behavior in correctional facilities and psychiatric hospitals is limited. Results from recent research suggest that comorbidity of severe mental disorder, personality disorder, and diagnosis of substance abuse is related to a higher risk of violent behavior. In the Berlin prison hospital, a database was created to collect data from all violent incidences (n=210) between 1997 and 2006 and between 2010 and 2016. In a retrospective, case-control study, we analyzed specific socioeconomic data and psychiatric diagnosis and compared the group of prisoners with violent behavior with randomly selected prisoners of the same department without violent behavior (n = 210). Diagnosis of schizophrenia, non-German nationality, no use of an interpreter, no children, and no previous sentence remained significantly associated with the dependent variable violent behavior. There were no significant differences regarding age and legal statuses. Practical implications for clinical work are discussed.
Introduction
Violent behavior is a complex phenomenon linked to biological, psychological, and social factors (1), and it constitutes a common problem in mental health care settings, as well as in correctional facilities. Altogether, there is limited evidence on the prevalence of violent behavior in medical and mental health settings and even less evidence for prison environments. Regarding facilities of community-based mental health care, violent behavior was reported in about 2–7% of all admissions in psychiatric hospitals in Germany (2, 3). Recently, Müller et al. reported a moderate increase in violent behavior against staff members in psychiatric inpatient settings between 2008 and 2015, with an average increase in violent incidences of 4% per year (4). A recent meta-analysis, including 23.972 hospitalized psychiatric patients, reported that 17% had at least once acted violently during their hospital stay (5). Staggs et al. described no changes from 2007 to 2013 regarding the frequency of violent assaults in U.S. American psychiatric wards (6), but reports from other countries are lacking.
The literature suggests a higher risk of violent behavior in individuals suffering from a severe mental disorder (7–9). Results from a prospective cohort study in Finland (1997) including 12.058 unselected individuals born in 1966 revealed an odds ratio of 3.1 for any criminal offense and an odds ratio of 7.0 for violent offenses in people with schizophrenia (10). Analyzing data of more than 18.000 cases of schizophrenia and other psychosis, Fazel et al. pointed out that the risk for violent behavior was increased compared to the risk of the general population. Furthermore, they described a significant increase in risk for comorbid substance abuse disorder (8). In terms of specific factors for violent behavior in general psychiatry, a history of violent offending, non-adherence to therapy (psychotherapy and/or medication), younger age, male gender, coming from a disadvantaged neighborhood, and recent alcohol misuse were described as risk factors (11) while depressive symptoms and better clinical insight regarding the symptoms were predictors of non-violent behavior (12).
Since the 1960s in Europe and North America, efforts were made to transfer the treatment of individuals suffering from mental disorders from segregated institutions to outpatient treatment facilities placed in the communities. During the last decades, this so-called “deinstitutionalization” was accompanied by a constant reduction of psychiatric beds (13). There is an ongoing discussion of whether the reduction of beds in psychiatric hospitals leads to an increase of severe mentally disordered individuals in prison (14, 15). In a review including 33.588 prisoners in 24 countries, the prevalence of psychotic disorder did not appear to be increasing over time (16). Comparing the level of distress in long- and short-term prisoners in Germany revealed a clinically significant level of depression, paranoid ideation, and psychosis in long-time prisoners (17).
Within the prison system of Berlin, Germany, specialist care is provided for mentally disordered prisoners in the department for psychiatry in the Berlin prison hospital. Admission is possible during every aspect of prisoner life, during remand prison and for the duration of the regular sentence. Typical clinical indications for admission are (exacerbation of) psychosis, suicidal ideation, violent behavior of unclear origin, depression, and adjustment disorders with comorbid personality disorders and substance abuse disorders. Due to the limited size, a waiting list system is implemented to manage the admission process. Also, weekly outpatient treatment is possible directly in the prisons. During the inpatient treatment, a personalized treatment plan includes, e.g., pharmacological treatment and psychotherapy and different options of group therapy including occupational therapy, art therapy, music therapy, addiction therapy, athletic training, and team sports. For severely disordered patients, the possibility of time-limited isolation in specific treatment rooms is available.
In general, in Berlin, male prisoners with a mental disorder are not transferred to a general psychiatric ward outside of the prison system.
If, however, during the trial period, the criminal responsibility of a remand prisoner is found to be diminished, he can be transferred to a forensic psychiatric hospital and, thus, leaves the prison system. Due to regulation through the department of justice, only male prisoners are treated in the department of psychiatry. Female prisoners are treated inside the women prison facility via outpatient service or are transferred to a specific forensic psychiatric ward outside of the prison system.
In a current review, the lack of intervention research regarding the prevention of violence in forensic psychiatric settings was identified (18). Regarding prison psychiatry specifically, research on trends and risk factors for violent behavior is rare.
Aims of Our Study
The first aim of our study was to provide a description of frequency, trends, and pattern of violent behavior in patients of a psychiatric ward in a prison hospital. In a second step, we aim to identify possible risk or protective factors regarding violent behavior in patients of the psychiatric ward in the Berlin prison hospital. Furthermore, we were interested in the changes in the incidence of violent behavior during the last decades.
Our hypothesizes were:
Regarding risk factors for violent behavior research suggests that criminal behavior in the past, younger age, and diagnosis of schizophrenia are risk factors for violent behavior (8, 11, 19–21).
1. We hypothesized that patients with violent behavior were young, had more previous prison sentences, and suffered more often from schizophrenia.
Due to the often discussed “forensification” of psychiatric patients and the relocation of bed capacity between general and forensic psychiatry (13, 22),
2. We assumed a higher level of violent behavior in the patients of the psychiatric ward of the Berlin Prison Hospital in comparison to known rates from psychiatric inpatients in community hospital care.
3. We expected an increase in patients with a diagnosis of schizophrenia during the study period.
4. We expected that violent behavior in the prison hospital increased during the last 20 years.
Material and Methods
As part of the routine documentation in German prisons, specific incidents such as violent behavior are reported through a system called “official message” (German: “Dienstliche Meldung”). After 2007, the Berlin prison hospital was no longer an independent unit, but part of the Prison Plötzensee (“JVA Plötzensee”). Consequently, due to administrative changes, the “official message” system was no longer part of medical documentation. From 2010 onwards, new medical files were employed to record patient data. For our study, “official messages” were used to identify patients with violent behavior on the psychiatric ward of the Berlin prison hospital from 1997 to 2006. From 2010 to 2016, we identified violent patients by evaluating medical records. Although a change of the recording system took place during the study period, the basic principles for the assessment of violent behavior remained unchanged.
Between 1997 and 2006, 1,502 “official messages” were documented by the staff members of the psychiatric ward of the Berlin prison hospital. The “official messages” were categorized as “physical violence,” “self-harm,” “verbal violence,” “damage to property,” and “not categorized.” The “not categorized” cases applied when patients offended general prison rules, e.g., behaving noisy, using the telephone without permission, drinking alcohol, or taking drugs. In this study, we only included the cases categorized as “physical violence.”
Altogether, we identified 244 incidents of violent behavior during the period examined, committed by 210 individuals. We compared this group with an equal number of patients who did not demonstrate this behavior during their stay. For the comparison group, we selected the first non-violent individual who was admitted subsequently to each violent individual. For all individuals who generated more than one official message because of violent behavior, we chose the non-violent individual who was admitted directly after the first violent episode as a control. For the actual analysis, the following items were ascertained for both groups: year of the violent act, age of the offender, nationality, using a language interpreter, status of imprisonment (remand or sentenced), previous sentences, self-harming behavior, psychiatric diagnoses, and parenthood/existence of children. The variable “using a language interpreter” was rated as positive when a language interpreter had to be ordered into the prison hospital to translate between the patient and the medical personnel. The variable “parenthood/existence of children” was extracted by analyzing the medical files of the patients. The other variables were rated using both the medical and prison files. Diagnoses were coded using the ICD-10 Manual. For the data from 2010 to 2016, we used a data set that was extracted for research purposes from routine data (23). The data for the same items regarding the period from 1997 to 2006 were extracted from medical files.
The proportion of violent patients of all patients admitted was assessed for each year from 1997 to 2006 and 2010 to 2016. We performed hierarchical linear modeling to test for annual fluctuations in our results. Fisher’s exact test was applied to detect the significance of differences observed between the groups. The impact of all independent variables on the dependent variable “violent behavior” was calculated using a logistic regression model. The subset of all variables that minimize the AIC (Akaike information criterion) was determined by a stepwise elimination procedure to derive a final model. All tests were based on a significance level of p < 0.05. Analyses were performed with the statistical software R, Version 3.5.1. It is important to note that only male prisoners were included in the study.
Results
Table 1 displays the absolute number of patients admitted to the psychiatric ward of the Berlin prison hospital with recorded violent behavior, the number of patients diagnosed with schizophrenia, and the relative share per year. While the percentages of patients with violent behavior in 1997 to 2006 ranged from approximately 4.7 to 9.3%, the percentages of patients exhibiting violent behavior in 2010 to 2016 were subject to more considerable fluctuations (3.2–15.9%). Despite the increase in patients with violent incidences in the last 2 years, test results showed no statistically significant increase over time (p = 0.1543), but the number of individuals in the study group diagnosed with schizophrenia increased significantly (p = 0.0348) (see Figure 1).
TABLE 1
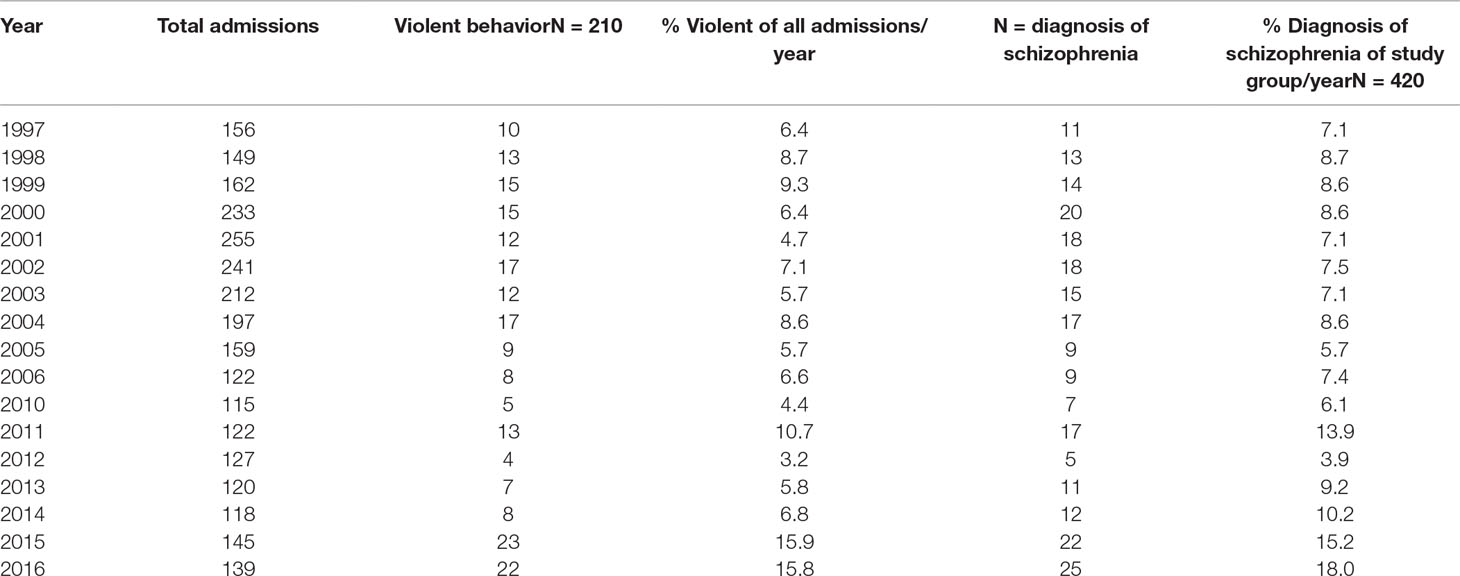
Table 1 Admissions, violent behavior, and diagnosis over time.
FIGURE 1
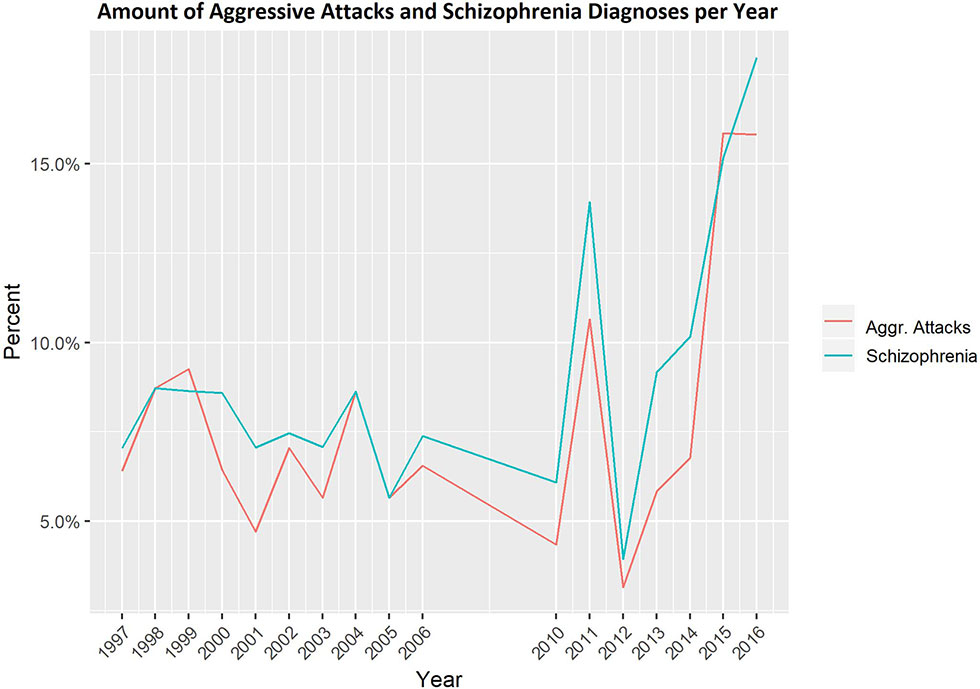
Figure 1 Percentage of admissions of patients with violent behavior per year and of violent patients with schizophrenia per year.
The univariate analysis of variables associated with violent behavior demonstrated statistically significant results for the items age, previous sentences, nationality, use of an interpreter, children, and diagnosis of a mental disorder (schizophrenia, substance use disorder, and adjustment disorder). While 71.9% of all patients who had displayed violent behavior had no previous convictions, the same only applied to 40.2% of all patients without recorded violent acts (p < 0.001). Having children was also highly significant (p < 0.001), whereas 89.5% of patients with violent behavior did not have children. Also, using the services of an interpreter was significantly lower (p < 0.001) among patients with violent behavior (5.26%) than in patients without recorded incidences (14.3%). Significantly, more patients with a diagnosis of schizophrenia had displayed violent behavior (68.1 vs. 47.6%).
All variables outlined above (Table 2), including the patient’s age, were entered into a logistic regression model.
TABLE 2
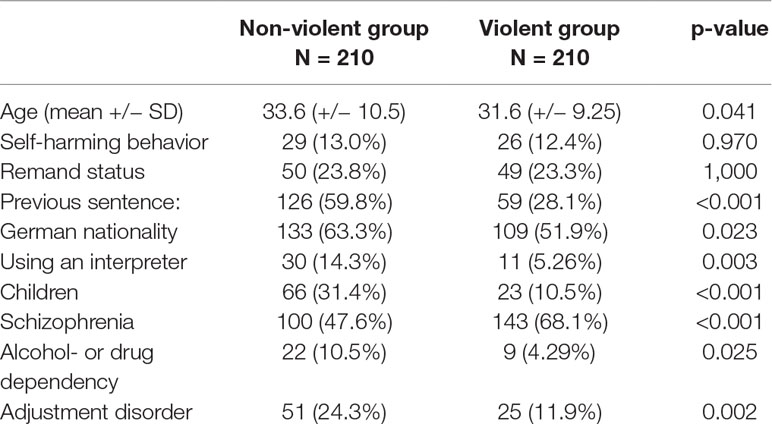
Table 2 Univariate analysis of variables associated with violent behavior.
After a stepwise selection of variables using the Akaike information criterion, the final model was developed (Table 3). In this, the variable diagnosis of schizophrenia, non-German nationality, no use of an interpreter, no children, and no previous sentence remained significantly associated with the dependent variable violent behavior (p < 0.05). Note that “age” is not among the independent variables.
TABLE 3
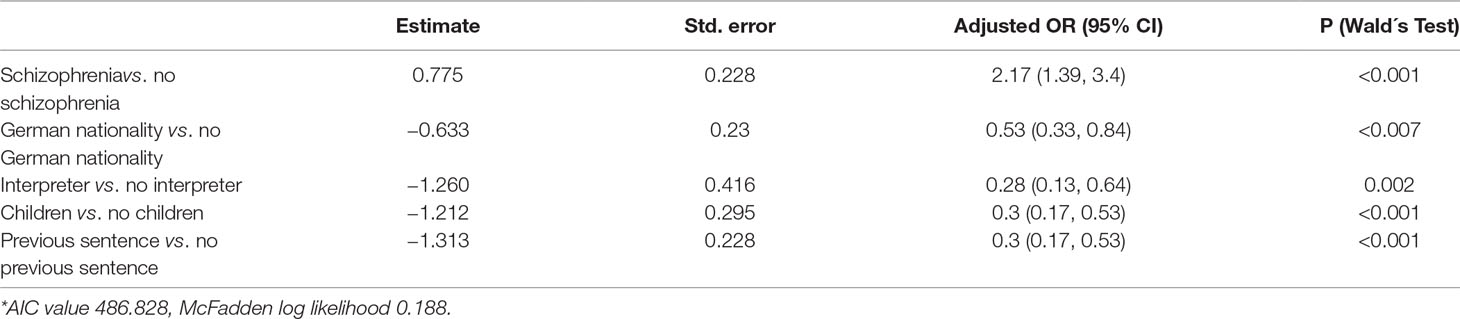
Table 3 Final logistic regression model of variables associated with violent behavior (final model)*.
Our results present a rate for patients that demonstrated violent behavior in a prison hospital that ranged from 3.2 to 15.9%. This rate is in the range of rates reported from psychiatric inpatients in community hospital care (2–4). Regarding trends, there was no statistically significant increase in violent behavior in the last 20 years regarding the psychiatric ward of the Berlin prison hospital. Our findings did not support our hypothesis regarding an increase in violent behavior.
Looking for risk and/or protective factors regarding violent behavior, the main findings of our study are that the group of patients that demonstrated violent behavior in the specific setting of a psychiatric ward of a prison hospital differed statistically significant from the non-violent group regarding diagnoses of schizophrenia, nationality, previous sentences, the existence of children, and the use of an interpreter for communication. Interestingly, after logistic regression, there were no group differences for violent behavior regarding age.
Altogether, our findings suggest a strong relationship between suffering from schizophrenia and the frequency of violent incidents but do not support the hypothesis that violent incidents have increased during the study period or are in total more frequent than in community mental health care.
During the last two decades, there is a lively discussion going on whether changes in the provision of mental health care may lead to marginalization and “forensification” of mentally disordered patients. The process of psychiatric deinstitutionalization has changed the structure of psychiatric care during the study period in Germany, in most European countries and the United States (24). Psychiatric beds in community care were closed, and psychiatric care transferred to community-based outpatient service. This process was accompanied by an increase of placements in forensic psychiatric care (25–27), and this finding revived interest in the validity of the “Penrose hypothesis,” which postulates an inverse relationship between the number of psychiatric hospital beds and the size of the prison populations (28). According to Blüml et al., the number of psychiatric beds decreased by 12.6% in Germany between 1993 and 2011, and the prison population increased by 14.8%. Nevertheless, the authors argue that statistical analyses point to a more complicated process and that the “Penrose hypothesis” is a univariate simplification of a complex and multifactorial relationship (29). Our findings of an increase in patients with schizophrenia in the group of violent patients may cautiously support the “Penrose hypothesis.”
Due to German law, individuals with mental disorders that committed severe offenses can be admitted directly to forensic psychiatric hospitals instead of prison. It is important to note that bed capacity in forensic psychiatric hospitals increased continuously during our study period (26). Interestingly, in forensic psychiatric hospitals, the literature suggests an increase in violent incidents (21, 22). Maybe, we did not detect a significant increase in violent behavior due to a shift of the most violent subgroup of prisoners with schizophrenia to the care of the local forensic hospital.
Schizophrenia proved to be a statistically significant marker for the patients in the violent group what is in accordance to the international literature on psychosis, substance abuse, and violent behavior (8, 11, 30). Interestingly, rates of violent behavior did not exceed the reported rates from general psychiatry (2–4). Wolf et al. recently reported results suggesting that, in specific forensic psychiatric populations, risk factors differ in comparison to general psychiatric populations (31). While in general psychiatric populations, the diagnosis is associated with violent behavior, in forensic psychiatric settings, this is the case regarding gender and previous violent behavior.
There were more patients without a previous sentence in the violent group than in the non-violent group, which contradicted our hypothesis. We hypothesized that there would be a greater percentage of patients with previous sentences in the violent group than in the non-violent group, due to a potentially higher share of patients with antisocial tendencies in the group of individuals with previous sentences and the findings in the literature that criminal problematic behavior in the past is a risk factor for future behavior (8, 19–21, 31). A possible explanation is that the item “previous sentences” may indicate more individual experience in prison settings and, thus, the “shock” of being imprisoned is not as severe as in the group of “first-timers.” It seems understandable that being imprisoned for the first time in combination with a mental disorder is especially traumatizing. After multivariate testing, this item remained statistically significant. As a possible implication for the clinical work, our results suggest that, in a psychiatric prison setting, a detailed medical history should always include the personal criminal record and past experiences with the penal system. To the best of our knowledge, specific studies on this item as a potentially protective factor against violent behavior in prison hospital settings do not exist.
In our sample, most individuals that demonstrated violent behavior had no children of their own, in contrast to the non-violent group. It seems reasonable that the existence of children may be understood as an indirect marker for general social skills such as social competence, the capability of building romantic relationships, and social networking. The international literature on protective factors suggests competencies in these life areas, such as relationships, family, work, and prosocial attitudes (32, 33). Our data supported our hypothesis that the existence of children for an individual may be regarded as a protective factor for violent behavior in a prison hospital setting.
In the violent group, there were significantly more patients of non-German nationality. This variable was significant after logistic regression analyses. Higher incidence of mental disorder, including schizophrenia in migrants, when compared to the resident population, has been reported consistently (34–36). According to current research, reasons for the increased incidence was multifactorial including higher prevalence rates in origin countries, the experience of an elevated level of stress, isolation, exposure to racism, and lower use of medication for psychotic disorders (37–39). In a past analysis regarding the characteristics of psychiatric inpatients in the Berlin prison hospital, there were no hints for an elevated prevalence of psychotic disorders in non-German prisoners (23). The differences in the frequency of violent behavior between German and non-German patients may be attributed to stress-related factors as well as to differences in the acceptance of antipsychotic medication. A limitation of our study regarding the item “mental disorder” was that we did not test for treatment adherence or the specific phase of the psychosis (acute, chronic). The available literature on these topics suggests a relationship between the severity of psychosis and violent or otherwise problematic behavior (11, 12, 40, 41).
Regarding the use of a language interpreter due to the lack of German language skills, this was the case statistically significantly more often in the non-violent group than in the violent group. This result supported our hypothesis that the use of language interpreters could have had a positive influence on violent behavior in our specific patient population. Psychiatric patients with additional deficits in the German language may demonstrate violent behavior more frequently, due to the lack of proper means for communication. The literature on the necessity of a language translator in prison settings concerning problematic behavior is, to our knowledge, minimal (42, 43). The regular interaction through language translators may have positive effects on the patient in the prison environment because; in comparison to the German staff, there is an opportunity for the patient to fully communicate with and through the translator, who is often of the same cultural background.
Regarding the patients in the violent group, it may be possible that the staff was unable to organize interpreters as often or as quick as in the non-violent group, although we did not test for that. Also, maybe due to the initial violent behavior of the patient, a proper appointment with an interpreter was difficult because of specific circumstances (e.g., isolation). Our results suggest a positive influence of language interpreters in a psychiatric prison setting.
International literature suggests that young age is a risk factor for violent behavior in psychiatric patients (44) and the general population. In our prison hospital setting, in the group of violent patients, there were more patients of younger age, but after multivariate analysis, age was not significantly associated with violent behavior. A possible reason for this may be that patients in our prison hospital are less heterogeneous regarding age than in a general psychiatric ward in the community. Still, in our population, patients that showed violent behavior were slightly younger.
Being in remand prison is known to be very stressful for individuals in prison with a significantly higher rate for suicide ideation, self-harm events, and mental distress (45, 46). Our hypothesis that remand prisoners who would be violent more often in our sample did not stand ground after multivariate analysis. In both groups, nearly a fourth of the individuals were remand prisoners. A possible reason could be that patients, once admitted into remand prison, are not always transferred to the prison hospital as soon as possible due to, e.g., lack of capacity. During this critical phase, agitated patients receive treatment in remand prison via outpatient psychiatric care and, thus, were not included in our population. It would be interesting to investigate the occurrence of violent behavior in the remand prison system and compare it to the prison hospital and the general prison population. Studies on these issues are missing.
Several limitations must be considered when interpreting our findings. The retrospective design may have led to various biases, such as a variation of the awareness for violent behavior. The fact that reorganization of routine documentation took place during the study period may have caused different rates of reporting violent incidents. Also, our study included only men and excluded women due to the structure of the specific psychiatric ward in the prison hospital in Berlin. Regarding the diagnosis, we did not check for current medication, the severity of symptoms, or the phase of the disorder. Due to incomplete data, we were unable to include the effects of specific personality disorders on violent behavior. High prevalence of personality disorders in prisoners is known, so this could be a focus for future research. Besides, although we covered a rather long time-span of 20 years, the years between 2007 and 2009 were not included due to missing data (see above).
In summary, to the best of our knowledge, this is the first study that explores violent behavior in the setting of a psychiatric ward in a German prison hospital. In our opinion, this is a vital field of research because the professionals in this field are confronted regularly with high-risk populations for violent behavior and because optimization of individual treatment may benefit the long-term outcome for the patient, as well as for the general society. We share the opinion that further research is needed in the area of prison psychiatry, preferably in an international context.
Data Availability Statement
All datasets generated for this study are included in the article/ supplementary materials.
Ethics Statement
According to current legal regulation, the study was approved by the local ethic committee at Charité–Universitätsmedizin Berlin.
Author Contributions
PS, AO-W, AV, and NK designed the study. PS, VN, IK, DD, and AO-W collected the data. PS, AO-W, AV, UG, and BN analyzed and interpreted the data. PS, AV, and AO-W wrote the final draft of the manuscript. PS, AO-W, and NK had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of data analysis. All authors have contributed to, read, and approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Fund of Charité–Universitätsmedizin Berlin.
References
1. Rubio-Valera M, Luciano JV, Ortiz JM, Salvador-Carulla L, Gracia A, Serrano-Blanco A. Health service use and costs associated with aggressiveness or agitation and containment in adult psychiatric care: a systematic review of the evidence. BMC Psychiatry (2015) 15:35. doi: 10.1186/s12888-015-0417-x
2. Steinert T, Vogel WD, Beck M, Kehlmann S. [Aggression by psychiatric patients in the clinic. A one-year study of four state hospitals]. Psychiatr Prax (1991) 18:155–61.
3. Spiessl H, Krischker S, Cording C. [Aggression in the psychiatric hospital. A psychiatric basic documentation based 6-year study of 17,943 inpatient admissions]. Psychiatr Prax (1998) 25:227–30.
4. Muller MJ, Olschinski C, Jochim D, Feldhordt M. [Assessment of aggressive assaults by patients from 2008 to 2015 in two german psychiatric hospitals: results and implications]. Psychiatr Prax (2017) 44:258–65. doi: 10.1055/s-0042-105177
5. Iozzino L, Ferrari C, Large M, Nielssen O, de Girolamo G. Prevalence and risk factors of violence by psychiatric acute inpatients: a systematic review and meta-analysis. PLoS One (2015) 10:e0128536. doi: 10.1371/journal.pone.0128536
6. Staggs VS. Trends victims, and injuries in injurious patient assaults on adult, geriatric, and child/adolescent psychiatric units in US hospitals, 2007-2013. Res Nurs Health (2015) 38:115–20. doi: 10.1002/nur.21647
7. Völlm BA, Clarke M, Herrando VT, Seppänen AO, Gosek P, Heitzman J, et al. European psychiatric association (EPA) guidance on forensic psychiatry: Evidence based assessment and treatment of mentally disordered offenders. Eur Psychiatry (2018) 51:58–73. doi: 10.1016/j.eurpsy.2017.12.007
8. Fazel S, Gulati G, Linsell L, Geddes JR, Grann M. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med (2009) 6:e1000120. doi: 10.1371/journal.pmed.1000120
9. Kudumija Slijepcevic M, Jukic V, Novalic D, Zarkovic-Palijan T, Milosevic M, Rosenzweig I. Alcohol abuse as the strongest risk factor for violent offending in patients with paranoid schizophrenia. Croat Med J (2014) 55:156–62. doi: 10.3325/cmj.2014.55.156
10. Tiihonen J, Isohanni M, Rasanen P, Koiranen M, Moring J. Specific major mental disorders and criminality: a 26-year prospective study of the 1966 northern Finland birth cohort. Am J Psychiatry (1997) 154:840–5. doi: 10.1176/ajp.154.6.840
11. Witt K, van Dorn R, Fazel S. Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS One (2013) 8:e55942. doi: 10.1371/journal.pone.0055942
12. Ekinci O, Ekinci A. Association between insight, cognitive insight, positive symptoms and violence in patients with schizophrenia. Nord J Psychiatry (2013) 67:116–23. doi: 10.3109/08039488.2012.687767
13. Chow WS, Priebe S. How has the extent of institutional mental healthcare changed in Western Europe? Analysis of data since 1990. BMJ Open (2016) 6:e010188. doi: 10.1136/bmjopen-2015-010188
14. Priebe S, Frottier P, Gaddini A, Kilian R, Lauber C, Martínez-Leal R, et al. Mental health care institutions in nine European countries, 2002 to 2006. Psychiatr Serv (2008) 59:570–3. doi: 10.1176/ps.2008.59.5.570
15. Dressing H, Salize HJ. Pathways to psychiatric care in European prison systems. Behav Sci Law (2009) 27:801–10. doi: 10.1002/bsl.893
16. Fazel S, Seewald K. Severe mental illness in 33,588 prisoners worldwide: systematic review and meta-regression analysis. Br J Psychiatry (2012) 200:364–73. doi: 10.1192/bjp.bp.111.096370
17. Otte S, Vasic N, Nigel S, Streb J, Ross T, Spitzer C. Different yet similar? Prisoners versus psychiatric patients - A comparison of their mental health. Eur Psychiatry (2017) 44:97–103. doi: 10.1016/j.eurpsy.2017.04.006
18. Fazel S, Wolf A. A Systematic review of criminal recidivism rates worldwide: current difficulties and recommendations for Best Practice. PLoS One (2015) 10:e0130390. doi: 10.1371/journal.pone.0130390
19. Bonta J, Law M, Hanson K. The prediction of criminal and violent recidivism among mentally disordered offenders: a meta-analysis. Psychol Bull (1998) 123:123–42. doi: 10.1037/0033-2909.123.2.123
20. Blais J, Bonta J. Tracking and managing high risk offenders: A Canadian initiative. Law Hum Behav (2015) 39:253–65. doi: 10.1037/lhb0000109
21. Fazel S, Wolf A, Palm C, Lichtenstein P. Violent crime, suicide, and premature mortality in patients with schizophrenia and related disorders: a 38-year total population study in Sweden. Lancet Psychiatry (2014) 1:44–54. doi: 10.1016/S2215-0366(14)70223-8
22. Bowers L, Stewart D, Sigh I. Conflict and Containment Research Programme. In: Inpatient Violence and aggression: A literature review. (2011). Section of Mental Health Nursing, Kings College London: Amsterdam.
23. Opitz-Welke A, Konrad N. Inpatient treatment in the psychiatric department of a German prison hospital. Int J Law Psychiatry (2012) 35:240–3. doi: 10.1016/j.ijlp.2012.02.015
24. Seppanen A, Tormanen I, Shaw C, Kennedy H. Modern forensic psychiatric hospital design: clinical, legal and structural aspects. Int J Ment Health Syst (2018) 12:58. doi: 10.1186/s13033-018-0238-7
25. Franke I, Vogel T, Eher R, Dudeck M. Prison mental healthcare: recent developments and future challenges. Curr Opin Psychiatry (2019) 32:342–7. doi: 10.1097/YCO.0000000000000504
26. Chow WS, Ajaz A, Priebe S. What drives changes in institutionalised mental health care? A qualitative study of the perspectives of professional experts. Soc Psychiatry Psychiatr Epidemiol (2019) 54:737–44. doi: 10.1007/s00127-018-1634-7
27. Konrad N, Lau S. Dealing with the mentally ill in the criminal justice system in Germany. Int J Law Psychiatry (2010) 33:236–40. doi: 10.1016/j.ijlp.2010.06.005
28. Watt DC. L. S., Penrose FRS (1898–1972). Psychiatrist and professor of human genetics. Br J Psychiatry (1998) 173:458–61. doi: 10.1192/bjp.173.6.458
29. Bluml V, Waldhor T, Kapusta ND, Vyssoki B. Psychiatric hospital bed numbers and prison population sizes in 26 european countries: A critical reconsideration of the penrose hypothesis. PLoS One (2015) 10:e0142163. doi: 10.1371/journal.pone.0142163
30. Wilson JA, Wood PB. Dissecting the relationship between mental illness and return to incarceration. J Crim Just (2014) 42:527–77. doi: 10.1016/j.jcrimjus.2014.09.005
31. Wolf A, Fanshawe TR, Sariaslan A, Cornish R, Larsson H, Fazel S. Prediction of violent crime on discharge from secure psychiatric hospitals: A clinical prediction rule (FoVOx). Eur Psychiatry (2018) 47:88–93. doi: 10.1016/j.eurpsy.2017.07.011
32. Borowsky IW, Hogan M, Ireland M. Adolescent sexual aggression: risk and protective factors. Pediatrics (1997) 100:E7. doi: 10.1542/peds.100.6.e7
33. Willis GM, Grace RC. The quality of community reintegration planning for child molesters: effects on sexual recidivism. Sex Abuse (2008) 20:218–40. doi: 10.1177/1079063208318005
34. Patel K, Kouvonen A, Close C, Vaananen A, O’Reilly D, Donnelly M. What do register-based studies tell us about migrant mental health? A scoping review. Syst Rev (2017) 6:78. doi: 10.1186/s13643-017-0463-1
35. Norredam M, Garcia-Lopez A, Keiding N, Krasnik A. Risk of mental disorders in refugees and native Danes: a register-based retrospective cohort study. Soc Psychiatry Psychiatr Epidemiol (2009) 44:1023–9. doi: 10.1007/s00127-009-0024-6
36. Jensen NK, Norredam M, Priebe S, Krasnik A. How do general practitioners experience providing care to refugees with mental health problems? A qualitative study from Denmark. BMC Fam Pract (2013) 14:17. doi: 10.1186/1471-2296-14-17
37. Cantor-Graae E, Pedersen CB, McNeil TF, Mortensen PB. Migration as a risk factor for schizophrenia: a Danish population-based cohort study. Br J Psychiatry (2003) 182:117–22. doi: 10.1192/bjp.182.2.117
38. Straiton M, Reneflot A, Diaz E. Immigrants' use of primary health care services for mental health problems. BMC Health Serv Res (2014) 14:341. doi: 10.1186/1472-6963-14-341
39. Anderson KK, Cheng J, Susser E, McKenzie KJ, Kurdyak P. Incidence of psychotic disorders among first-generation immigrants and refugees in Ontario. CMAJ (2015) 187:E279–E86. doi: 10.1503/cmaj.141420
40. Imai A, Hayashi N, Shiina A, Sakikawa N, Igarashi Y. Factors associated with violence among Japanese patients with schizophrenia prior to psychiatric emergency hospitalization: a case-controlled study. Schizophr Res (2014) 160:27–32. doi: 10.1016/j.schres.2014.10.016
41. Large MM, Nielssen O. Violence in first-episode psychosis: a systematic review and meta-analysis. Schizophr Res (2011) 125:209–20. doi: 10.1016/j.schres.2010.11.026
42. Stolk Y, Ziguras S, Saunders T, Garlick R, Stuart G, Coffey G. Lowering the language barrier in an acute psychiatric setting. Aust N Z J Psychiatry (1998) 32:434–40. doi: 10.3109/00048679809065538
43. Igarashi Y, Hayashi N, Ebata K, Kaneko T. [A social psychiatric study on foreign-born inpatients at Tokyo Metropolitan Matsuzawa hospital]. Seishin Shinkeigaku Zasshi (1994) 96:513–29.
44. Howner K, Andiné P, Bertilsson G, Hultcrantz M, Lindström E, Mowafi F. Mapping systematic reviews on forensic psychiatric care: a systematic review identifying knowledge Gaps. Front Psychiatry (2018) 9:452. doi: 10.3389/fpsyt.2018.00452
45. Hassan L, Birmingham L, Harty MA, Jarrett M, Jones P, King C, et al. Prospective cohort study of mental health during imprisonment. Br J Psychiatry (2011) 198:37–42. doi: 10.1192/bjp.bp.110.080333
Keywords: violent behavior, mental disorder, prison hospital, schizophrenia, age
Citation: Seidel P, Konrad N, Negatsch V, Dezsö D, Kogan I, Gauger U, Neumann B, Voulgaris A and Opitz-Welke A (2019) Violent Behavior During Psychiatric Inpatient Treatment in a German Prison Hospital. Front. Psychiatry 10:762. doi: 10.3389/fpsyt.2019.00762
Received: 31 December 2018; Accepted: 23 September 2019;
Published: 31 October 2019.
Edited by:
Thomas Masterman, Karolinska Institute (KI), SwedenReviewed by:
Axel Haglund, Swedish National Board of Forensic Medicine, SwedenPeter Andiné, University of Gothenburg, Sweden
Copyright © 2019 Seidel, Konrad, Negatsch, Dezsö, Kogan, Gauger, Neumann, Voulgaris and Opitz-Welke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: A. Opitz-Welke, Annette.opitz-welke@charite.de
†These authors have contributed equally to this work