 Lijuan Huo1†
Lijuan Huo1† Yongjie Zhou2†
Yongjie Zhou2† Shen Li3
Shen Li3 Yuping Ning1,4Lingyun Zeng2
Yuping Ning1,4Lingyun Zeng2 Zhengkui Liu5Wei Qian5Jiezhi Yang6Xin Zhou7Tiebang Liu2*
Zhengkui Liu5Wei Qian5Jiezhi Yang6Xin Zhou7Tiebang Liu2* Xiang Yang Zhang5*
Xiang Yang Zhang5*- 1Department of Psychiatry, Affiliated Brain Hospital of Guangzhou Medical University (Guangzhou Huiai Hospital), Guangzhou, China
- 2Department of Psychiatric Rehabilitation, Shenzhen Kangning Hospital, Shenzhen, Guangdong, China
- 3Department of Psychiatry, College of Basic Medical Sciences, Tianjin Medical University, Tianjin, China
- 4The First School of Clinical Medicine, Southern Medical University, Guangzhou, China
- 5CAS Key Laboratory of Mental Health, Institute of Psychology, Chinese Academy of Sciences, Beijing, China
- 6Shenzhen Health Development Research Center, Shenzhen, China
- 7Research Center for Psychological and Health Sciences, China University of Geosciences, Wuhan, China
Objective: The large-scale epidemic of Coronavirus Disease 2019 (COVID-19) has triggered unprecedented physical and psychological stress on health professionals. This study aimed to investigate the prevalence and risk factors of burnout syndrome, and the relationship between burnout and depressive symptoms among frontline medical staff during the COVID-19 epidemic in China.
Methods: A total of 606 frontline medical staff were recruited from 133 cities in China using a cross-sectional survey. The Maslach Burnout Inventory (MBI) was used to assess the level of burnout. Depressive symptoms were assessed by the Patient Health Questionnaire Depression (PHQ-9).
Results: During the COVID-19 pandemic, 36.5% of the medical staff experienced burnout. Personal and work-related factors were independently associated with burnout, including age (OR = 0.68, 95% CI: 0.52–0.89, p = 0.004), family income (OR = 0.72, 95% CI: 0.53–0.99, p = 0.045), having physical diseases (OR = 2.16, 95% CI: 1.42–3.28, p < 0.001), daily working hours (OR = 1.35, 95% CI: 1.03–1.77, p = 0.033), and profession of nurse (OR = 2.14, 95% CI: 1.12–4.10, p = 0.022). The correlation coefficients between the scores of each burnout subscale and the scores of depressive symptoms were 0.57 for emotional exhaustion, 0.37 for cynicism, and −0.41 for professional efficacy (all p < 0.001).
Conclusions: Our findings suggest that the prevalence rate of burnout is extremely high among medical staff during the COVID-19 pandemic, which is associated with other psychological disorders, such as depression. Psychological intervention for medical staff is urgently needed. Young and less experienced medical staff, especially nurses, should receive more attention when providing psychological assistance.
Introduction
The outbreak of coronavirus disease 2019 (COVID-19) first appeared in Wuhan, China in December 2019, and has since swept the world at an incredible speed. As of December 2020, there have been more than 70 million confirmed cases and more than 1.7 million deaths1. Due to high contagion and possible asymptomatic transmission, as well as a lack of knowledge of the virus, the demand and pressure on frontline medical staff have increased dramatically, especially in the early stages of the pandemic (Hu B. et al., 2020; Li et al., 2020). This condition has seriously aggravated the mental fatigue of healthcare professionals.
According to the latest World Health Organization’s International Disease Classification (ICD-11), burnout is officially classified as an occupational health syndrome, which is characterized by emotional and mental exhaustion due to long-term workplace stress and negative job perception. The most recognized definition of burnout is the three-dimensional psychological syndrome proposed by Maslach and Jackson (1981) that includes emotional exhaustion, cynicism, and reduced professional efficacy. Medical staff are susceptible to job burnout, which has attracted more and more attention recently (Dzau et al., 2018). Meta-analyses have shown that the pooled prevalence of burnout among medical staff is estimated to be about or more than 30% (Dimou et al., 2016; Gómez-Urquiza et al., 2017; O’Connor et al., 2018; Rezaei et al., 2018), a rate of more than twice compared with professionals in other fields (Dzau et al., 2018). Because of the nature of their work, medical staff often face a lot of pressure and negative emotions, such as heavy workload, poor doctor-patient relationship (especially in mainland China), and accumulated frustration in the face of death (He and Qian, 2016; Alharbi et al., 2019). Job burnout reduces working efficiency and increases medical errors (Patel et al., 2018; Tawfik et al., 2019). To make matters worse, burnout may lead to other severe mental disorders, including alcohol abuse/dependence, depression, and an increased risk of suicide (Dyrbye et al., 2008; Johnson et al., 2018).
The unprecedented outbreak of COVID-19 has further damaged the mental health of health care workers. During this pandemic, many social and environmental factors lead to burnout of medical staff, such as isolation, expanded workloads, life-threatening workplaces, concern about infecting relatives or colleagues, and some personal factors (Lai et al., 2020). A number of insightful commentaries have been published to appeal to the mental burden of medical staff, and to propose guidelines and expert consensus on mental health services (Greenberg et al., 2020; Liu et al., 2020; Raudenská et al., 2020). Many surveys have also reported that health care workers exposed to COVID-19 suffered from serious psychological disturbances, the most common of which were depression, anxiety, insomnia, and fear (Lai et al., 2020; Que et al., 2020; Tan et al., 2020a; Zhang W. R. et al., 2020). However, so far, few quantitative studies have investigated the symptoms of job burnout among medical staff (Hu D. et al., 2020; Matsuo et al., 2020; Tan et al., 2020b; Zhang Y. et al., 2020). These studies evaluated burnout symptoms, and focused on frontline nurses instead of estimating prevalence (Hu D. et al., 2020; Zhang Y. et al., 2020), or collecting information in one single institution (Matsuo et al., 2020; Zhang Y. et al., 2020). Tan et al. (2020b) started the survey half a year after the outbreak of the pandemic in China and 4 months after the outbreak in Singapore. At that time, the pressure of medical staff was different (Tan et al., 2020b). Further, they did not separately analyze the three recognized dimensions of burnout due to the use of other tools.
The purposes of this study were: (1) to explore the prevalence of burnout in the frontline medical staff in China during the early stage of COVID-19 epidemic; (2) to identify the individual and job-related determinants of burnout in this population, and (3) to determine the relationship between burnout and depressive symptoms.
Materials and Methods
Study Design and Participants
This was a cross-sectional survey designed to assess the job burnout and other mental conditions of frontline medical workers in China during the COVID-19 epidemic. In order to avoid face-to-face interaction, an online questionnaire was constructed and distributed via WeChat, one of the most important social tools in mainland China. Data were collected from February 14 to March 29, 2020. A total of 606 frontline medical workers were recruited from 133 cities across the country. Doctors, nurses, or medical technicians in hospitals, aged 18 years or above were included in this study.
The study was approved by the Institute of Psychology, Chinese Academy of Sciences. Each participant signed an electronic informed consent form before the survey. The information of all respondents was confidential.
Assessments for Burnout and Depressive Symptoms
Demographic and work-related information was collected, including residence, age, sex, height, weight, ethnicity, marital status, education, annual family income, occupation, department, length of service, and daily working hours. At the same time whether relatives or friends were infected, financial loss, and whether they had experienced SARS outbreaks were also collected.
The Chinese version of the Maslach Burnout Inventory-General Survey (MBI-GS)(Maslach and Jackson, 1981; Schutte et al., 2000) was used to assess job burnout, which has been widely used among healthcare workers in China, and has satisfactory reliability and validity (Wu et al., 2007). The MBI-GS consists of 15 items, measuring three dimensions of occupational burnout: emotional exhaustion (EE), which means being emotionally depleted at work; cynicism (CY), which means negative or cynical attitudes toward work; professional efficacy (PE), which means a positive sense of success/achievement at work. Each item is scored using a 7-point frequency range scale (0 = never to 6 = daily). The total score of each subscale is stratified into high, moderate, or low tertiles. Based on the previous large sample studies on Chinese healthcare workers (Wu et al., 2014), the cutoffs for each tertile of burnout were determined as follows: low EE < 9, moderate EE 9–13, high EE > 13; low CY < 3, moderate CY 3–9, high CY > 9; low PE > 30, moderate PE 30–18, high PE < 18. A score in the highest tertiles of EE, in combination with the highest tertiles of CY or the lowest tertiles of PE indicates burnout syndrome, according to the “exhaustion + 1” criterion (Brenninkmeijer and VanYperen, 2003). Since the definition of burnout varies considerably in the literature, the prevalence of burnout was also calculated using an alternative formula, a more restrictive definition, that is, a combination of a high EE and high CY and low PE subscale score (Lin et al., 2019). Patient Health Questionnaire-9 (PHQ-9) was applied to assess depressive symptoms (Kroenke et al., 2001). PHQ-9 consists of 9 items, each with a score from 0 to 3. People with a total score of 4 or more are identified to have depressive symptoms.
Statistical Analysis
The chi-square test and analysis of variance (ANOVA) were used to compare the demographic and work-related variables of participants between the burnout group and the non-burnout group. The binary logistic regression model was used to find out factors independently related to burnout experience. Then, in order to further identify the independent factors associated with MBI-GS scores, stepwise multivariate linear regression models were used, with the MBI-GS subscores as dependent variables, and other variables with potential correlation (p < 0.1) with MBI-GS scores as independent factors. Associations between MBI-GS subscale scores and PHQ-9 scores were examined using Pearson correlation analysis and then linear regression model. Bonferroni corrections were applied to adjust multiple tests. A two-tailed test at p < 0.05 was set to be statistically significant. All statistical analyses were conducted using SPSS (version 24.0).
Results
Demographic Characteristics
Among all the participants, 492 (81.2%) were female and 114 (18.8%) were male. The age of participants ranged from 22 to 65 years old, with an average age of 35.77 ± 8.13 years. The average BMI was 23.34 ± 5.61 Kg/m2. More detailed information about the demographic and job-related characteristics of participants is shown in Table 1.
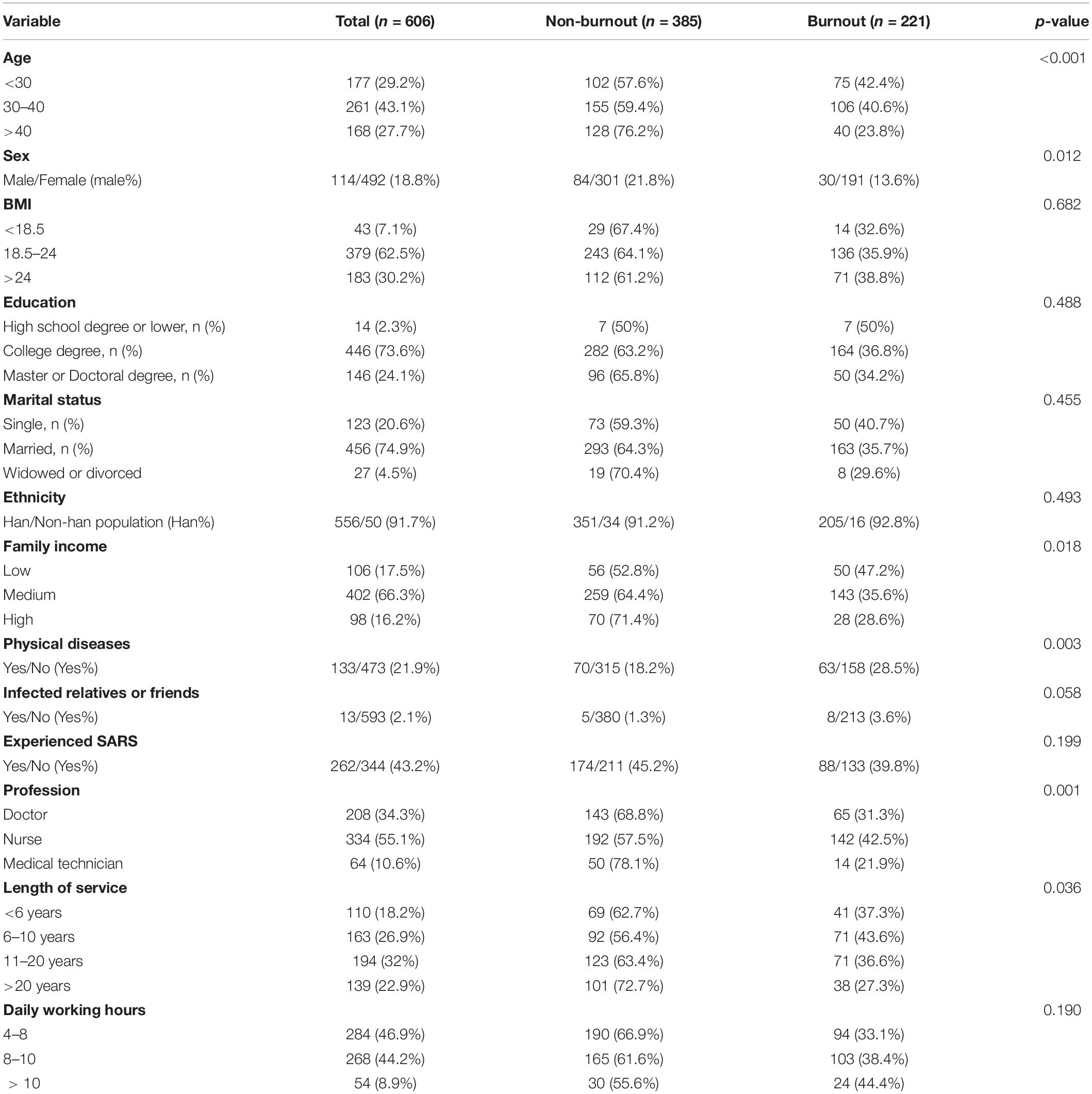
Table 1. Demographic data of participants with and without burnout.
Prevalence of Burnout in Medical Staffs
Burnout was defined as a high EE combing with a high CY or low PE subscale scores. During the epidemic of COVID-19, 36.5% of medical staff met the criteria for burnout in our sample. The prevalence of burnout in female workers was significantly higher than that in male workers, whether it was the inclusive criteria (38.8% vs. 26.3%, χ2 = 6.25, p = 0.012) or the restrictive one (30.5% vs. 16.7%, χ2 = 8.79, p = 0.003). For each component of burnout, the prevalence of EE, CY, and PE was 40.9, 63.7, and 46%, respectively. In addition, under the strictest definition, combining the highest level of EE and CY and the lowest level of PE, the overall prevalence of burnout was 27.8%.
Chi-squared tests also revealed that there were significant differences between burnout and non-burnout groups in terms of age, annual family income, physical disease, occupation, and service time (all p < 0.05). The burnout rates of each type of variables were shown in Table 1. Specifically, medical staff with younger age, female gender, lower family income, more severe physical disease, shorter service, and nursing profession had more severe syndrome of burnout. Individuals having relatives or friends infected with COVID-19 were at a marginally higher risk experiencing burnout (p = 0.058). There was no significant difference in BMI, education, marital status, ethnicity, experienced SARS or not, and daily working hours (all p > 0.05) between the burnout and non-burnout groups.
Further, the binary logistic regression model revealed that the following variables were independently associated with burnout, including age (OR = 0.68, 95% CI: 0.52–0.89, p = 0.004), family income (OR = 0.72, 95% CI: 0.53–0.99, p = 0.045), having physical disease (OR = 2.16, 95% CI: 1.42–3.28, p < 0.001), daily working hours (OR = 1.35, 95% CI: 1.03–1.77, p = 0.033), and profession of nurse (OR = 2.14, 95% CI: 1.12–4.10, p = 0.022).
Factors Associated With Burnout and Its Three Components in Medical Staffs
The average burnout score was 11.94 ± 6.47 on EE subscale, 10.27 ± 4.74 on CY subscale, and 19.25 ± 6.72 on PE subscale. MBI-GS subscale scores after grouping according to demographics and work-related variables were present in Table 2. Then multiple linear regressions were performed to identify independent related factors to each MBI-GS subscore. EE was independently correlated with age (β = −0.13, t = −2.87, p = 0.004), physical diseases (β = 0.12, t = 3.0, p = 0.003), professional role of nurses (β = 0.09, t = 2.16, p = 0.031), and daily working hours (β = 0.14, t = 3.57, p < 0.001). CY was independently correlated with professional role of nurses (β = 0.21, t = 4.90, p < 0.001), age (β = −0.11, t = −2.45, p = 0.015), and family income (β = −0.10, t = −2.40, p = 0.017). PE was independently correlated with age (β = 0.13, t = 3.06, p = 0.002) and professional role of nurses (β = −0.30, t = −7.18, p < 0.001). Taken together, younger age and nursing profession were independently correlated with all dimensions of burnout.
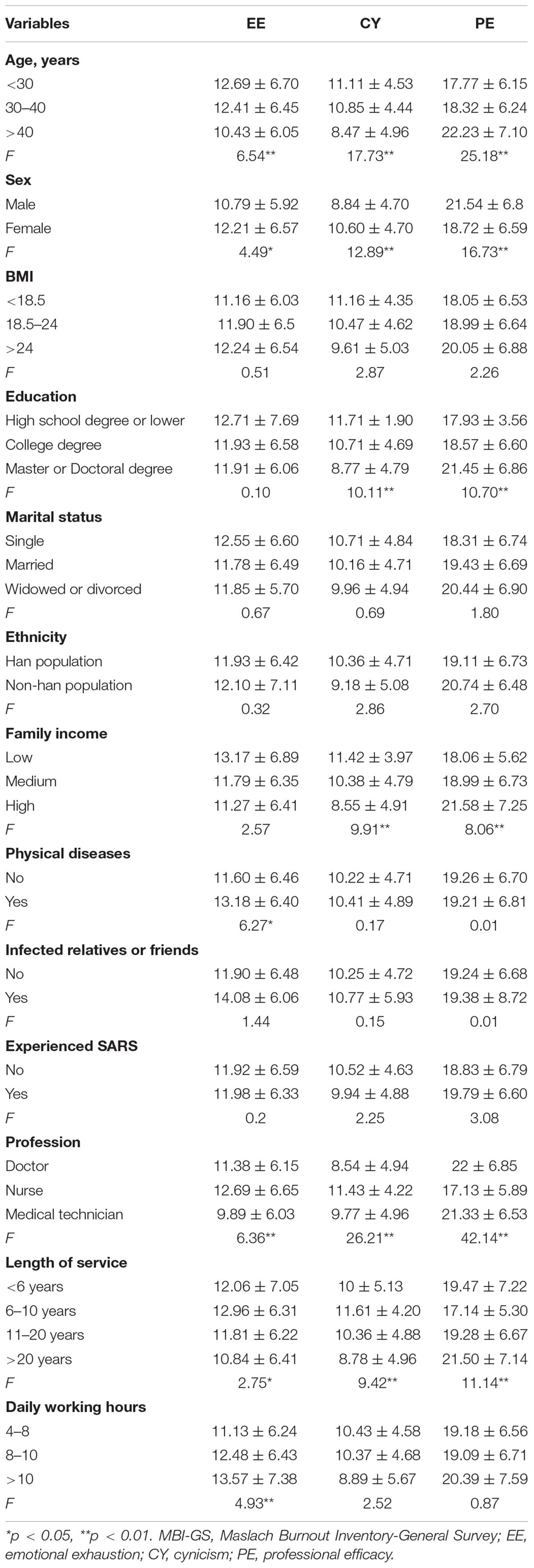
Table 2. MBI-GS subscale scores in grouped demographics and work-related variables.
The Association Between Burnout and Depressive Symptoms in Medical Staffs
The mean score of PHQ-9 was 6.46 ± 5.57. With the cut-off score of 4, the overall prevalence of depressive symptoms in medical staff was 57.6%. The correlation coefficients between the score of each MBI-GS subscale and the score of PHQ-9 were 0.57 for EE, 0.37 for CY, and −0.41 for PE (all p < 0.001, Figure 1). These associations remained significant after Bonferroni corrections. Stepwise multiple regression model showed that scores of EE (β = 0.51, t = 12.12) and PE (β = 0.51, t = 12.12) were independently associated with PHQ-9 score. These two components of burnout together accounted for 32.8% of the variance (adjusted R2) in PHQ-9 (F = 148.75, p < 0.001).
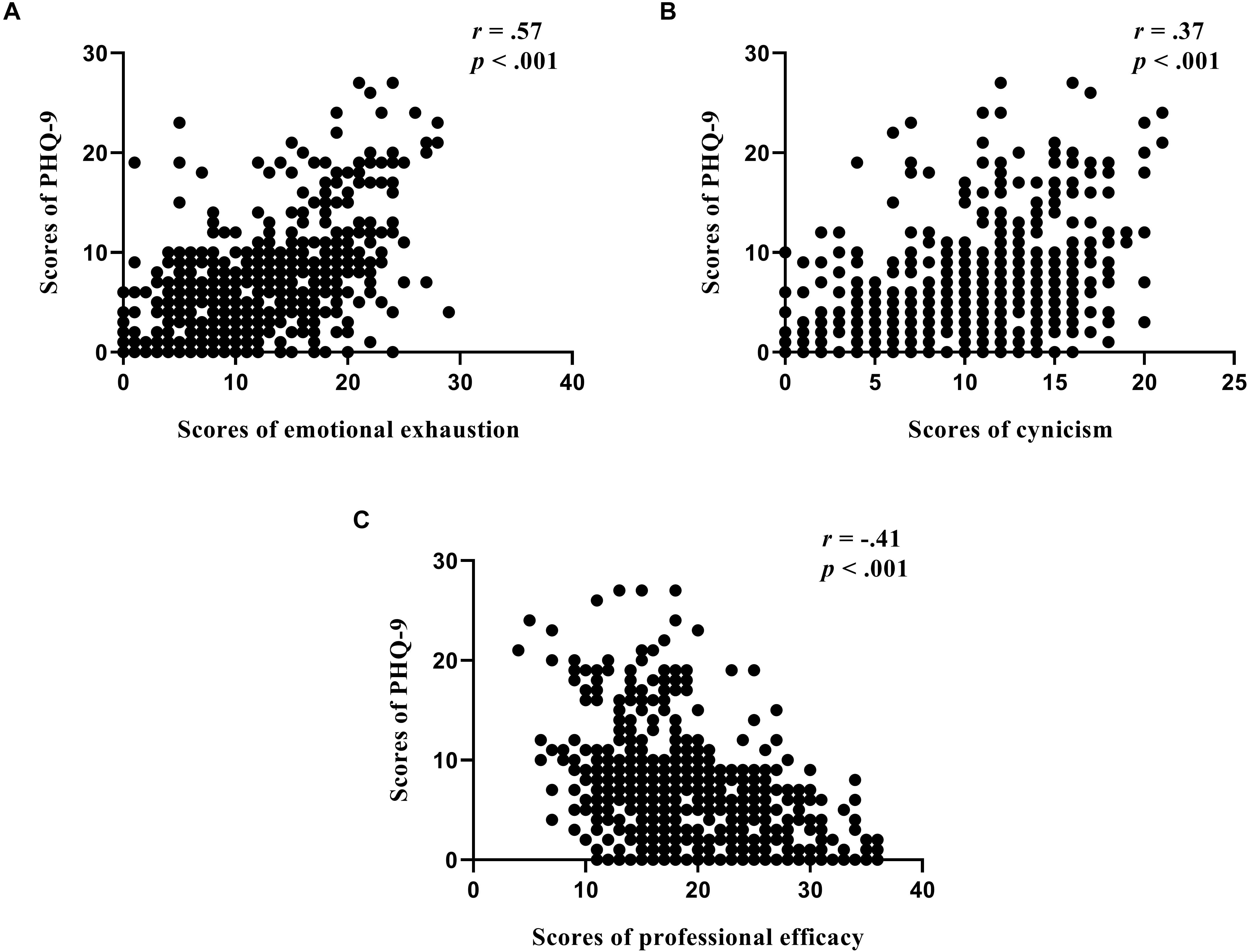
Figure 1. Three dimensions of burnout (A) emotional exhaustion, (B) cynicism, and (C) professional efficacy were associated with depressive symptoms (PHQ-9) in medical staff.
Discussion
Although there has been a large number of studies on mental health problems caused by the COVID-19 pandemic, only a few have investigated burnout syndrome, which was particularly prevalent in medical staff even before this pandemic. To our knowledge, this is the first nationwide cross-sectional survey on job burnout of medical staff during the COVID-19 pandemic, with a total of 606 participants. The main findings of this study were: (1) up to 36.5% of the respondents met the criteria of burnout; (2) personal factors (i.e., age, sex, physical diseases, and family income) and job-related factors (daily working hours, length of service, and nursing profession) were associated with burnout; (3) the burnout levels were associated with the severity of depressive symptoms.
Our results showed an extremely high prevalence (36.5%) of burnout, which made medical workers psychologically vulnerable in this pandemic. Consistently, previous studies have revealed that medical workers are particularly prone to burnout. The prevalence of burnout in healthcare professions varies from 12.6 to 76.9% in different studies (Abdulla et al., 2014; Adriaenssens et al., 2015; Elmore et al., 2016; Wen et al., 2016; Gómez-Urquiza et al., 2017). The huge differences across studies not only result from regional disparities but also result from different approaches to define burnout (Rotenstein et al., 2018). It is still in dispute whether the concept of burnout should be regarded as a unidimensional or multidimensional construct. Some research defined burnout as a multidimensional construct, so individuals were considered burnout when meeting the criterion of one of the three MBI dimensions (Elmore et al., 2016; Gómez-Urquiza et al., 2017). While other studies combine different dimensions into a unidimensional burnout, which also develop many formulas (Adriaenssens et al., 2015; Wen et al., 2016). To solve this problem, Brenninkmeijer and VanYperen (2003) tested different approaches and concluded that “exhaustion + 1” is the most recommended approach. This means that individuals are determined as burned out when having high levels of exhaustion and either high levels of cynicism or low levels of professional efficacy. This approach is in line with the idea that exhaustion is the core symptom of burnout, also the only dimension present in all different definitions and assessment tools for burnout. Therefore, exhaustion is a necessary symptom to set the “diagnosis” of burnout.
Due to the substantially various definitions and the impossibility to compare burnout prevalences across studies, we also directly compared the burnout scores between our results and studies using the same tool. Compared with the specific burnout scores of medical staff in different studies in China, this study found that the scores of medical staff on the EE and CY subscale were extremely higher, while the score on the PE subscale was lower (Wu et al., 2008, 2011, 2013, 2014; He et al., 2019). Taken together, it is speculated that there is a significant negative correlation between the long-term COVID-19 pandemic and the burnout experience of medical staff, although the criteria for the diagnosis of burnout are different.
Among the related factors of job burnout, job-related factors are the most concerned and discussed in detail under the burden of the COVID-19 pandemic. First of all, the occupation was closely related to job burnout. Compared with doctors and medical technicians, nurses are most likely to experience job burnout, which is consistent with many previous studies (Alacacioglu et al., 2009; Wu et al., 2011; Chou et al., 2014; Schooley et al., 2016) and the latest surveys conducted during the COVID-19 pandemic (Hu D. et al., 2020; Matsuo et al., 2020; Zhang Y. et al., 2020). Nursing job burnout has become a global phenomenon. In hospitals in the United States, there is a shortage of nursing staff, resulting in a high patient-to-nurse ratio, persistent emotional exhaustion, and job dissatisfaction (Aiken et al., 2002). A cross-sectional study of 12 European countries found that longer shifts (12 h or more) were associated with job burnout (Dall’Ora et al., 2015). The difference in working environment between countries limits the promotion of research in western countries. According to the few pieces of literature in China, the sense of professional efficacy of nurses is lower than that of doctors (Wu et al., 2013, 2014). For Chinese nurses, the large population base leads to a high nurse-patient ratio. Compared with doctors and medical technicians, nursing is a relatively low-paid profession in China. The reform of health care system policy and management strategy is accompanied by economic reform, which aggravates the great pressure and burnout of nurses (Wu et al., 2010). To make matters worse, in the early days of COVID-19 pandemic, medical personnel were not equipped with protective equipment and tested for coronavirus. As the main caregivers of patients, nurses have direct contact with infected patients many times a day when performing their duties. Therefore, compared with other medical staff, nurses face greater health risks, and consequently bear more psychological burden. Another explanation may be that nurses are mainly women, and they may bear more psychopathological burdens in outbreaks that threaten the health of family members or affect the care of children. Previous studies have demonstrated that women are more likely to suffer from Posttraumatic Stress Disorder (PTSD) and Posttraumatic Stress Symptoms (PTSS), and have more depressive and anxiety symptoms in the face of every coronavirus outbreak (Buselli et al., 2020; Carmassi et al., 2020).
The length of service was significantly correlated with every dimension of the burnout experience. Less than 20 years of service was risky for job burnout. The medical staff with a working life of 6–10 years had the strongest sense of emotional exhaustion and cynicism and the lowest sense of professional efficacy. Rich work experience after long service may contribute to higher esteem and better emotional regulation. It is reasonable that medical staff with work experience had enhanced psychological preparation and knowledge of infection control, and reduced the level of job burnout. The previous studies found that experienced nurses had a lower risk of violence in the workplace and a higher tolerance for patient aggression (Whittington, 2002; Edward et al., 2014). Young and inexperienced employees may be more nervous about highly contagious diseases.
Interestingly, we found that prolonged daily working hours were only associated with emotional exhaustion, not with cynicism and professional efficacy. As the relationship between excessive workload and a higher level of burnout has been well proved, many studies have proposed limiting working hours as the first step to prevent burnout (Gopal et al., 2005; Martini et al., 2006; Dugani et al., 2018). It should be noted that reducing working hours may not necessarily reduce cynicism and improve professional effectiveness. Moreover, during the COVID-19 epidemic, the huge number of infections and the exponential spread of coronavirus made the workload impossible to reduce. Therefore, during the pandemic, other more feasible methods are needed to alleviate the burnout experience.
Another important finding is that during the COVID-19 outbreak, job burnout of medical staff was positively correlated with depression. The latest report has demonstrated that during the COVID-19 outbreak, medical workers are twice as likely to suffer from depressive symptoms and other psychological disorders as the general population (Lu et al., 2020). The bi-directional link between burnout and depression has been widely recognized. Longitudinal studies have shown that an increase in burnout levels can predict a subsequent increase in depressive symptoms (Bianchi et al., 2015). As a result, the increase in depression is likely to be the result of exposure to unprecedented work-related stress during the COVID-19 pandemic, and vice versa. It is worth noting that due to the cross-sectional design, this study did not prove the causal relationship between burnout and depression.
This study has several limitations. First, this cross-sectional survey conducted at a single time point could not compare burnout levels before and after the outbreak. Moreover, there was relatively limited information on the specific factors of outbreaks that contribute to an increase in the prevalence of burnout. Therefore, our findings cannot reveal the causal relationship between the COVID-19 outbreak and high levels of job burnout. Second, as there is no consensus on the diagnosis of job burnout, it is difficult to directly compare the prevalence of job burnout. A recent review found that the existing literature used at least 47 different definitions of the prevalence of burnout when using the MBI tool to measure burnout (Rotenstein et al., 2018). Therefore, it is necessary in future studies to reach a consensus on how to classify different degrees of job burnout. Third, the levels of job burnout in the health care profession were not be compared with that of other occupations, as other industries were almost completely shut down during the pandemic. Therefore, the special impact of the COVID-19 epidemic on medical staff was not investigated. Fourth, there may be a sampling bias. The sample was composed of most female subjects who were more vulnerable to traumatic events. Hence, caution should be taken when extending our findings to other populations. Fifth, psychiatric evaluation of the samples was not performed before the study. As previously reported, pre-existing mental illness or susceptibility may have affected the development of burnout and depressive symptoms during the COVID-19 pandemic (Fiorillo et al., 2020). Sixth, the existence of burnout was investigated using an online self-administered questionnaire, which may compromise the reliability and validity of the measurement.
In summary, our report showed that there was a high rate of burnout among medical staff in China, which is likely to intensify during the COVID-19 pandemic. Occupation, length of service, working hours, and several individual variables, including age, sex, pre-existing physical diseases, and family income, are determinants of job burnout scores. The experience of burnout hinders the fight against the epidemic situation of COVID-19 and has a lasting negative impact on mental health. During and after the COVID-19 pandemic, intervention measures such as mindfulness-based decompression are urgent to deal with stress and solve the job burnout of medical staff. Psychological evaluation and psychological counseling should be carried out for medical staff on a long-term and regular basis. Our study suggests that when providing mental health services, more attention should be paid to young and less experienced medical staff, especially nurses. Compared with western countries, there are relatively few studies on job burnout of medical staff in China. Therefore, even after the COVID-19 pandemic, it is necessary to conduct more investigations on the causes and consequences of burnout and take effective intervention measures to prevent burnout.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Institute of Psychology, Chinese Academy of Sciences. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LH and YZ were responsible for statistical analysis and manuscript drafting. TL and XYZ were responsible for study design and writing review. YN, SL, ZL, and WQ were involved in statistical analysis and the manuscript revision. LZ, JY, and XZ were responsible for data acquirement. All the authors critically reviewed the manuscript and gave final approval for its publication.
Funding
This work was supported by the Sanming Project of Medicine in Shenzhen (No. SZSM202011014), Shenzhen Fund for Guangdong Provincial Highlevel Clinical Key Specialties (No. SZGSP013), and Shenzhen Key Medical Discipline Construction Fund (No. SZXK072).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
References
Abdulla, L., Al-Qahtani, D. M., and Al-Kuwari, M. G. (2014). Prevalence and determinants of burnout syndrome among primary healthcare physicians in Qatar. South Afr. Fam. Pract. 53, 380–383. doi: 10.1080/20786204.2011.10874118
Adriaenssens, J., De Gucht, V., and Maes, S. (2015). Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int. J. Nurs. Stud. 52, 649–661. doi: 10.1016/j.ijnurstu.2014.11.004
Aiken, L. H., Clarke, S. P., Sloane, D. M., Sochalski, J., and Silber, J. H. (2002). Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA 288, 1987–1993. doi: 10.1001/jama.288.16.1987
Alacacioglu, A., Yavuzsen, T., Dirioz, M., Oztop, I., and Yilmaz, U. (2009). Burnout in nurses and physicians working at an oncology department. Psychooncology 18, 543–548. doi: 10.1002/pon.1432
Alharbi, J., Jackson, D., and Usher, K. (2019). Compassion fatigue in critical care nurses. An integrative review of the literature. Saudi Med. J. 40, 1087–1097. doi: 10.15537/smj.2019.11.24569
Bianchi, R., Schonfeld, I. S., and Laurent, E. (2015). Burnout-depression overlap: a review. Clin. Psychol. Rev. 36, 28–41. doi: 10.1016/j.cpr.2015.01.004
Brenninkmeijer, V., and VanYperen, N. (2003). How to conduct research on burnout: advantages and disadvantages of a unidimensional approach in burnout research. Occup. Environ. Med. 60(Suppl. 1):i16. doi: 10.1136/oem.60.suppl_1.i16
Buselli, R., Corsi, M., Baldanzi, S., Chiumiento, M., Del Lupo, E., Dell’Oste, V., et al. (2020). Professional quality of life and mental health outcomes among health care workers exposed to sars-cov-2 (covid-19). Int. J. Environ. Res. Public Health 17:6180. doi: 10.3390/ijerph17176180
Carmassi, C., Foghi, C., Dell’Oste, V., Cordone, A., Bertelloni, C. A., Bui, E., et al. (2020). PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: what can we expect after the COVID-19 pandemic. Psychiatry Res. 292:113312. doi: 10.1016/j.psychres.2020.113312
Chou, L.-P., Li, C.-Y., and Hu, S. C. (2014). Job stress and burnout in hospital employees: comparisons of different medical professions in a regional hospital in Taiwan. BMJ Open 4:e004185. doi: 10.1136/bmjopen-2013-004185
Dall’Ora, C., Griffiths, P., Ball, J., Simon, M., and Aiken, L. H. (2015). Association of 12 h shifts and nurses’ job satisfaction, burnout and intention to leave: findings from a cross-sectional study of 12 European countries. BMJ Open 5:e008331. doi: 10.1136/bmjopen-2015-008331
Dimou, F. M., Eckelbarger, D., and Riall, T. S. (2016). Surgeon burnout: a systematic review. J. Am. Coll. Surg. 222, 1230–1239. doi: 10.1016/j.jamcollsurg.2016.03.022
CrossRef Full Text PubMed | PubMed Abstract | Google Scholar
Dugani, S., Afari, H., Hirschhorn, L., Ratcliffe, H., Veillard, J., Martin, G., et al. (2018). Prevalence and factors associated with burnout among frontline primary health care providers in low- and middle-income countries: a systematic review [version 3; peer review: 2 approved]. Gates Open Res. 2:4. doi: 10.12688/gatesopenres.12779.3
Dyrbye, L. N., Thomas, M. R., Massie, F. S., Power, D. V., Eacker, A., Harper, W., et al. (2008). Burnout and suicidal ideation among U.S. medical students. Ann. Intern. Med. 149, 334–341. doi: 10.7326/0003-4819-149-5-200809020-00008
Dzau, V. J., Kirch, D. G., and Nasca, T. J. (2018). To care is human - collectively confronting the clinician-burnout crisis. N. Engl. J. Med. 378:312. doi: 10.1056/nejmp1715127
Edward, K.-I., Ousey, K., Warelow, P., and Lui, S. (2014). Nursing and aggression in the workplace: a systematic review. Br. J. Nurs. 23, 653–659. doi: 10.12968/bjon.2014.23.12.653
Elmore, L. C., Jeffe, D. B., Jin, L., Awad, M. M., and Turnbull, I. R. (2016). national survey of burnout among US general surgery residents. J. Am. Coll. Surg. 223, 440–451. doi: 10.1016/j.jamcollsurg.2016.05.014
Fiorillo, A., Sampogna, G., Giallonardo, V., Del Vecchio, V., Luciano, M., Albert, U., et al. (2020). Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 63:e87.
Gómez-Urquiza, J. L., De la Fuente-Solana, E. I., Albendín-García, L., Vargas-Pecino, C., Ortega-Campos, E. M., and Cañadas-De la Fuente, G. A. (2017). Prevalence of burnout syndrome in emergency nurses: a meta-analysis. Crit. Care Nurse 37, e1–e9. doi: 10.4037/ccn2017508
Gopal, R., Glasheen, J. J., Miyoshi, T. J., and Prochazka, A. V. (2005). Burnout and internal medicine resident work-hour restrictions. Arch. Intern. Med. 165, 2595–2600. doi: 10.1001/archinte.165.22.2595
Greenberg, N., Docherty, M., Gnanapragasam, S., and Wessely, S. (2020). Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 368:m1211. doi: 10.1136/bmj.m1211
He, A. J., and Qian, J. (2016). Explaining medical disputes in Chinese public hospitals: the doctor–patient relationship and its implications for health policy reforms. Health Econ. Policy Law 11, 359–378. doi: 10.1017/S1744133116000128
He, S.-C., Wu, S., Du, X.-D., Jia, Q., Wang, C., Wu, F., et al. (2019). Interactive effects of corticotropin-releasing hormone receptor 1 gene and work stress on burnout in medical professionals in a Chinese Han population. J. Affect. Disord. 252, 1–8. doi: 10.1016/j.jad.2019.03.084
Hu, B., Guo, H., Zhou, P., and Shi, Z.-L. (2020). Characteristics of SARS-CoV-2 and COVID-19. Nature Rev. Microbiol. 1–14. doi: 10.1038/s41579-020-00459-7
Hu, D., Kong, Y., Li, W., Han, Q., Zhang, X., Zhu, L. X., et al. (2020). Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. EClinicalMedicine 24:100424. doi: 10.1016/j.eclinm.2020.100424
Johnson, J., Hall, L. H., Berzins, K., Baker, J., Melling, K., and Thompson, C. (2018). Mental healthcare staff well-being and burnout: a narrative review of trends, causes, implications, and recommendations for future interventions. Int. J. Ment. Health Nurs. 27, 20–32. doi: 10.1111/inm.12416
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). The PHQ−9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lai, J., Ma, S., Wang, Y., Cai, Z., Hu, J., Wei, N., et al. (2020). Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
Li, Q., Guan, X., Wu, P., Wang, X., Zhou, L., Tong, Y., et al. (2020). Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 382, 1199–1207.
Lin, M., Battaglioli, N., Melamed, M., Mott, S. E., Chung, A. S., and Robinson, D. W. (2019). High prevalence of burnout among US emergency medicine residents: results from the 2017 national emergency medicine wellness survey. Ann. Emerg. Med. 74, 682–690. doi: 10.1016/j.annemergmed.2019.01.037
Liu, S., Yang, L., Zhang, C., Xiang, Y.-T., Liu, Z., Hu, S., et al. (2020). Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 7, e17–e18. doi: 10.1016/S2215-0366(20)30077-8
Lu, W., Wang, H., Lin, Y., and Li, L. (2020). Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. 288:112936. doi: 10.1016/j.psychres.2020.112936
Martini, S., Arfken, C. L., and Balon, R. (2006). Comparison of burnout among medical residents before and after the implementation of work hours limits. Acad. Psychiatry 30, 352–355. doi: 10.1176/appi.ap.30.4.352
Maslach, C., and Jackson, S. E. (1981). The measurement of experienced burnout. J. Organ. Behav. 2, 99–113. doi: 10.1002/job.4030020205
Matsuo, T., Kobayashi, D., Taki, F., Sakamoto, F., Uehara, Y., Mori, N., et al. (2020). Prevalence of health care worker burnout during the coronavirus disease 2019 (COVID-19) pandemic in Japan. JAMA Netw. Open 3:e2017271. doi: 10.1001/jamanetworkopen.2020.17271
O’Connor, K., Muller Neff, D., and Pitman, S. (2018). Burnout in mental health professionals: A systematic review and meta-analysis of prevalence and determinants. Eur. Psychiatry 53, 74–99. doi: 10.1016/j.eurpsy.2018.06.003
Patel, R. S., Bachu, R., Adikey, A., Malik, M., and Shah, M. (2018). Factors related to physician burnout and its consequences: a review. Behav. Sci. 8:98. doi: 10.3390/bs8110098
Que, J., Le Shi, J. D., Liu, J., Zhang, L., Wu, S., Gong, Y., et al. (2020). Psychological impact of the COVID-19 pandemic on healthcare workers: a cross-sectional study in China. Gen. Psychiatry 33:e100259.
Raudenská, J., Steinerová, V., Javůrková, A., Urits, I., Kaye, A. D., Viswanath, O., et al. (2020). Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 34, 553–560. doi: 10.1016/j.bpa.2020.07.008
Rezaei, S., Karami Matin, B., Hajizadeh, M., Soroush, A., and Nouri, B. (2018). Prevalence of burnout among nurses in Iran: a systematic review and meta-analysis. Int. Nurs. Rev. 65, 361–369. doi: 10.1111/inr.12426
Rotenstein, L. S., Torre, M., Ramos, M. A., Rosales, R. C., Guille, C., Sen, S., et al. (2018). Prevalence of burnout among physicians: a systematic review. JAMA 320, 1131–1150. doi: 10.1001/jama.2018.12777
Schooley, B., Hikmet, N., Tarcan, M., and Yorgancioglu, G. (2016). Comparing burnout across emergency physicians, nurses, technicians, and health information technicians working for the same organization. Medicine (Baltimore) 95:e2856. doi: 10.1097/md.0000000000002856
Schutte, N., Toppinen, S., Kalimo, R., and Schaufeli, W. (2000). The factorial validity of the Maslach Burnout Inventory-General Survey (MBI-GS) across occupational groups and nations. J. Occup. Organ. Psychol. 73, 53–66. doi: 10.1348/096317900166877
Tan, B. Y. Q., Chew, N. W. S., Lee, G. K. H., Jing, M., Goh, Y., Yeo, L. L. L., et al. (2020a). Psychological Impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 173, 317–320. doi: 10.7326/M20-1083
Tan, B. Y. Q., Kanneganti, A., Lim, L. J. H., Tan, M., Chua, Y. X., Tan, L., et al. (2020b). Burnout and associated factors among health care workers in singapore during the COVID-19 pandemic. J. Am. Med. Dir. Assoc. 21, 1751–1758.e5. doi: 10.1016/j.jamda.2020.09.035
Tawfik, D. S., Scheid, A., Profit, J., Shanafelt, T., Trockel, M., Adair, K. C., et al. (2019). Evidence relating health care provider burnout and quality of care. Ann. Intern. Med. 171, 555–567. doi: 10.7326/M19-1152
Wen, J., Cheng, Y., Hu, X., Yuan, P., Hao, T., and Shi, Y. (2016). Workload, burnout, and medical mistakes among physicians in China: a cross-sectional study. Biosci. Trends 10, 27–33. doi: 10.5582/bst.2015.01175
Whittington, R. (2002). Attitudes toward patient aggression amongst mental health nurses in the ‘zero tolerance’ era: associations with burnout and length of experience. J. Clin. Nurs. 11, 819–825. doi: 10.1046/j.1365-2702.2002.00659.x
Wu, H., Chi, T.-S., Chen, L., Wang, L., and Jin, Y.-P. (2010). Occupational stress among hospital nurses: cross-sectional survey. J. Adv. Nurs. 66, 627–634. doi: 10.1111/j.1365-2648.2009.05203.x
Wu, H., Liu, L., Sun, W., Zhao, X., Wang, J., and Wang, L. (2014). Factors related to burnout among Chinese female hospital nurses: cross-sectional survey in Liaoning Province of China. J. Nurs. Manag. 22, 621–629. doi: 10.1111/jonm.12015
Wu, H., Liu, L., Wang, Y., Gao, F., Zhao, X., and Wang, L. (2013). Factors associated with burnout among Chinese hospital doctors: a cross-sectional study. BMC Public Health 13:786. doi: 10.1186/1471-2458-13-786
Wu, S., Zhu, W., Li, H., Wang, Z., and Wang, M. (2008). Relationship between job burnout and occupational stress among doctors in China. Stress Health 24, 143–149. doi: 10.1002/smi.1169
Wu, S., Zhu, W., Wang, Z., Wang, M., and Lan, Y. (2007). Relationship between burnout and occupational stress among nurses in China. J. Adv. Nurs. 59, 233–239. doi: 10.1111/j.1365-2648.2007.04301.x
Wu, S.-Y., Li, H.-Y., Wang, X.-R., Yang, S.-J., and Qiu, H. A. (2011). Comparison of the effect of work stress on burnout and quality of life between female nurses and female doctors. Arch. Environ. Occup. Health 66, 193–200. doi: 10.1080/19338244.2010.539639
Zhang, W. R., Wang, K., Yin, L., Zhao, W. F., Xue, Q., Peng, M., et al. (2020). Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother. Psychosom. 89, 242–250. doi: 10.1159/000507639
Keywords: prevalence, medical staff, COVID-19, depression, burnout
Citation: Huo L, Zhou Y, Li S, Ning Y, Zeng L, Liu Z, Qian W, Yang J, Zhou X, Liu T and Zhang XY (2021) Burnout and Its Relationship With Depressive Symptoms in Medical Staff During the COVID-19 Epidemic in China. Front. Psychol. 12:616369. doi: 10.3389/fpsyg.2021.616369
Received: 12 October 2020; Accepted: 08 February 2021;
Published: 04 March 2021.
Edited by:
Andrew E. P. Mitchell, University of Chester, United KingdomReviewed by:
Claudia Carmassi, University of Pisa, ItalyJelena Bakusic, KU Leuven, Belgium
Hakan Eren, Ankara University, Turkey
Copyright © 2021 Huo, Zhou, Li, Ning, Zeng, Liu, Qian, Yang, Zhou, Liu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tiebang Liu, liutb530@163.com; Xiang Yang Zhang, zhangxy@psych.ac.cn
†These authors have contributed equally to this work