Diet as a Risk Factor for Early-Onset Colorectal Adenoma and Carcinoma: A Systematic Review
 Kaitlin L. Carroll
Kaitlin L. Carroll Andrew D. Frugé
Andrew D. Frugé Martin J. Heslin2
Martin J. Heslin2  Elizabeth A. Lipke
Elizabeth A. Lipke Michael W. Greene
Michael W. Greene- 1Department of Nutrition, Dietetics and Hospitality Management, Auburn University, Auburn, AL, United States
- 2Mitchell Cancer Institute, University of South Alabama, Mobile, AL, United States
- 3Department of Chemical Engineering, Auburn University, Auburn, AL, United States
Background: Colorectal cancer in adults 50 years old and younger is increasing in incidence worldwide. Diet may be a modifiable risk factor. The objective of this study was to examine evidence regarding the association between diet and the risk of developing early-onset colorectal cancer (EOCRC) and early-onset colorectal adenomas in young adults.
Methods: PUBMED, Web of Science, and Embase were systematically searched for studies examining dietary intake as a risk factor for EOCRC and early-onset colorectal adenomas. Results were synthesized narratively due to the heterogeneity of the studies.
Results: Of the 415 studies identified, ten met the inclusion criteria. Of these ten studies, four provided data on dietary risk factors for early-onset colorectal adenomas and six provided data on dietary risk factors for EOCRC. The four studies that measured colorectal adenoma occurrence reported an increased incidence with high sugar sweetened beverage intake, a higher pro-inflammatory diet, a higher Western diet score and higher sulfur microbial diet score. A protective effect against early-onset colorectal adenomas was observed in those who had a higher Prudent diet score or higher adherence to other health dietary approaches (Dietary Approaches to Stop Hypertension, Alternative Healthy Eating Index-2010, or the alternative Mediterranean diet). Those who consumed large amounts of deep-fried foods, refined foods, followed a high fat diet, consumed large amounts of sugary drinks and desserts, and had low folate and fiber consumption had a significantly higher occurrence of EOCRC. A protective effect against EOCRC was observed for those who consumed more fruits and vegetables, high amounts of micronutrients and those who adhered to a vegetarian diet.
Conclusions: The results of this study reveal various dietary habits may be risk factors or protective against early-onset colorectal cancer and adenomas. Future research should focus on large prospective cohort studies with long-term follow-up to confirm published results and further examine whether differences in diet quality are associated with EOCRC risk.
Introduction
Colorectal cancer (CRC) is the 2nd leading cause of cancer deaths and 3rd most commonly diagnosed cancer globally (1). By 2030, the global burden of CRC is expected to increase to more than 2.2 million cases and 1.1 million cancer deaths annually (2). Due to increases in screening, rates among adults aged 50 and older have been decreasing in recent years; however, incidence of cases in those under 50 years old have increased at an alarming rate (3, 4). Early-onset colorectal cancer (EOCRC), defined as colorectal cancer in patients under the age of 50, accounts for ~10% of all newly diagnosed CRC cases (5, 6). The reason for this increase in incidence is unclear.
EOCRC occurs most often in the distal colon and rectum (7). EOCRC is typically discovered at a more advanced stage and more aggressive tumor histology at diagnosis than traditional CRC (6). EOCRC typically arises from neoplasia following the conventional adenoma-carcinoma sequence, therefore, colorectal adenomas are likely common precursors for early onset colorectal cancer (8). A lack of screening and education targeted toward younger adults has contributed to key symptoms and colorectal adenomas going undetected, hindering a recognition and removal process which could likely prevent colorectal cancer (6, 9).
Over 50% of CRC cases diagnosed after age 55 are attributable to modifiable risk factors (10). Known risk factors for traditional CRC include family history, inflammatory bowel disease, low levels of physical activity, cigarette smoking, increased BMI, diabetes and poor dietary habits (11). High consumption of foods that have been shown to increase the risk of CRC include red meat and processed meat, while high intakes of fruits and vegetables, whole grains and dairy products have been associated with a decreased incidence of CRC (12). The risk factors for developing EOCRC are less clear. In countries such as the United States (13), Canada (14), Australia (15) and Japan (16), the rise in early-onset CRC cases occurs mainly in individuals born during or after the 1960s. This strongly indicates that the upward trend in early onset cases could be explained by population-level changes in early-life exposure, such as diet and lifestyle (6, 17). In the US, diet quality declined steadily from 1985 to 2006 (18) and has remained steady since. Worldwide, simple sugar intake has greatly increased in recent decades, mainly due to increased consumption of sugar sweetened beverages (19). Similarly, Western-like dietary habits are increasingly being adopted by non-Western countries. While evidence connecting diet and other modifiable risk factors to traditional CRC is strong, evidence is lacking when it comes to EOCRC due to the expensive cost and difficulties associated with studies that follow young people for an extensive period of time.
It is pertinent to understand the driving factors behind the increase of EOCRC cases, as it typically presents at a more advanced stage, with a greater risk of metastasis and less favorable prognosis (7). Identifying risk factors associated with EOCRC may lead to more effective prevention methods and improve screening efforts for high-risk populations. Even though the traditional risk factors for CRC and their association with precursors for EOCRC and EOCRC risk have been extensively studied, there is a lack of published research articles examining diet alone as a risk factor for EOCRC. Thus, the objective of this systematic review was to examine published research articles on early-onset colorectal cancer and adenomas for risk factors or preventative behaviors related to food choices and dietary habits.
Methods
Search Strategy
The methodology follows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Databases searched include PubMed and Web of Science. The databases were searched using the following key words: risk, early-onset colorectal cancer, diet, young-onset colorectal cancer, risk factors. “And” and “or” were used to combine the keywords listed and to minimize search duplications. There were no language restrictions on the searches. A backwards search was also conducted, i.e., references of accessed studies were evaluated for relevant studies that may have been missed through the database search. A gray literature search of Google was performed. Finally, the Embase database was searched for any articles missed from the above searches. No new articles were found in Embase. Searches were conducted between August 2021 and September 2021.
The primary outcome of this review was the examination of dietary habits that may be risk factors or preventative factors for developing early-onset colorectal cancer and adenomas.
Inclusion and Exclusion Criteria and Selection Process
The population, interventions, comparators, outcomes and study designs (PICOS) scheme was used for assessing eligibility (Table 1). One reviewer (K.C.) performed an independent quality assessment of the studies to assess eligibility. Eligible studies were peer-reviewed original case-control and cohort studies including men and women diagnosed with early-onset colorectal cancer or colorectal adenoma before age 55. The age eligibility was chosen so that EOCRC studies that did not follow EOCRC being defined as diagnosis at or before age 50 (6) would be included in the current analysis. All cases of colorectal cancer and adenomas were histologically confirmed by a doctor. All studies needed to include a dietary assessment and use the dietary information to examine the association with diet and risk. Excluded study types include reviews, books and book chapters, letters, abstracts, animal studies, cross-sectional studies, and comments on an article.
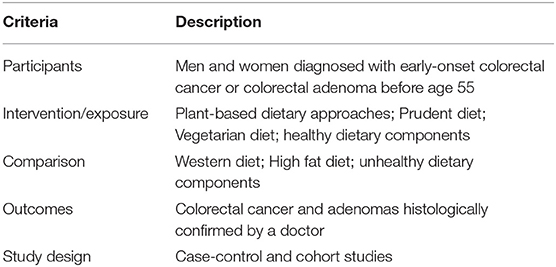
Table 1. The population, interventions, comparators, outcomes and study designs (PICOS) scheme used for assessing eligibility.
Potential sources were first screened by title and study type to match inclusion criteria. Sources that appeared to match inclusion criteria were then accessed and abstracts were screened. Full-text versions of any remaining articles fitting the inclusion criteria were accessed and assessed.
Data Collection and Effect Measures
One reviewer (K.C.) collected data from the included reports. All relevant data was compiled into a study characteristics table (Table 2) and independently reviewed by all the investigators.

Table 2. Characteristics of included studies (early-onset colorectal adenomas).
Relevant data included any measures that assessed EOCRC and early-onset adenoma risk with specific foods, dietary habits or specified diets. Additionally, data on alcoholic beverages alone was excluded; however, two studies included alcoholic beverages in their diet score (Alternative Mediterranean and Sulfur Microbial Diet Score), and therefore were not excluded. Data on BMI, weight and obesity levels were not included in this review. Data regarding participant recruitment methods, participant demographics and dietary assessment methods was assessed.
The effect estimates such as odds ratios (OR) and hazard ratios (HR), 95% confidence intervals (CI) and p-values (when available) for exposure categories of all dietary factors assessed were extracted. Odds ratios that were adjusted for multi-variables such as age, sex or other risk factors of CRC were the preferred forms of data extracted. All of the extracted data was stored in an electronic table.
Synthesis of Results
As a result of the significant heterogeneity of the included studies with regard to study design, outcome measures and nutrition assessments, a quantitative synthesis was not possible.
Results
In total, 413 studies were identified using the keyword searches. All articles were found on PubMed. Web of Science did not provide any additional articles not already found on PubMed. Two additional studies were identified through backwards searching. After removing duplicates and articles excluded by study type, 301 articles remained for screening. Of these studies, 188 were excluded based on their abstract. From these studies, 113 were assessed for eligibility based on the inclusion and exclusion criteria previously described. One hundred and three of these studies were excluded for lacking inclusion criteria (no dietary assessment). Ultimately, ten articles were included in the final analysis (Figure 1).
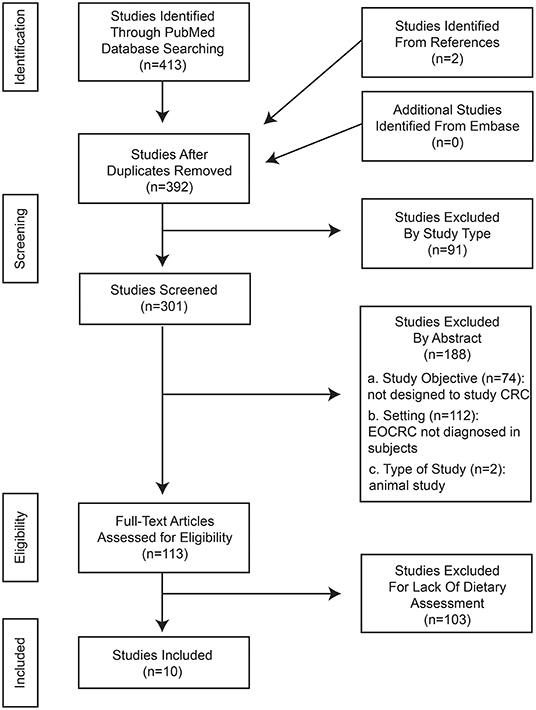
Figure 1. PRISMA flow chart.
Study Characteristics and Participants
Of the ten studies included, five were prospective cohort studies (20–24) and five were a case-control studies (25–29). Four studies examined the relationship between early onset colorectal adenomas (Table 2) and potential risk factors, including diet (20–23) and six examined risk factors, including diet, for developing early onset colorectal cancer (24–29) (Table 3). The geographic location of the studies were as follows: seven studies used participants in the United States (20–25, 29); two studies used participants from Canada (25, 27); one study included participants from Australia (25); two studies used participants from Asia (25, 28); and two studies used participants in Europe (25, 26). The number of subjects ranged from 74 to 94,217. Ages of the subjects ranged from 19 to 55, apart from two studies which compared early-onset cases to older onset cases (23, 25). All studies used a food frequency questionnaire (FFQ) to assess dietary habits from 1 to 2 years before diagnosis except one, which utilized a high school food frequency questionnaire (HS-FFQ) to assess dietary habits during adolescence and the association with risk (20).
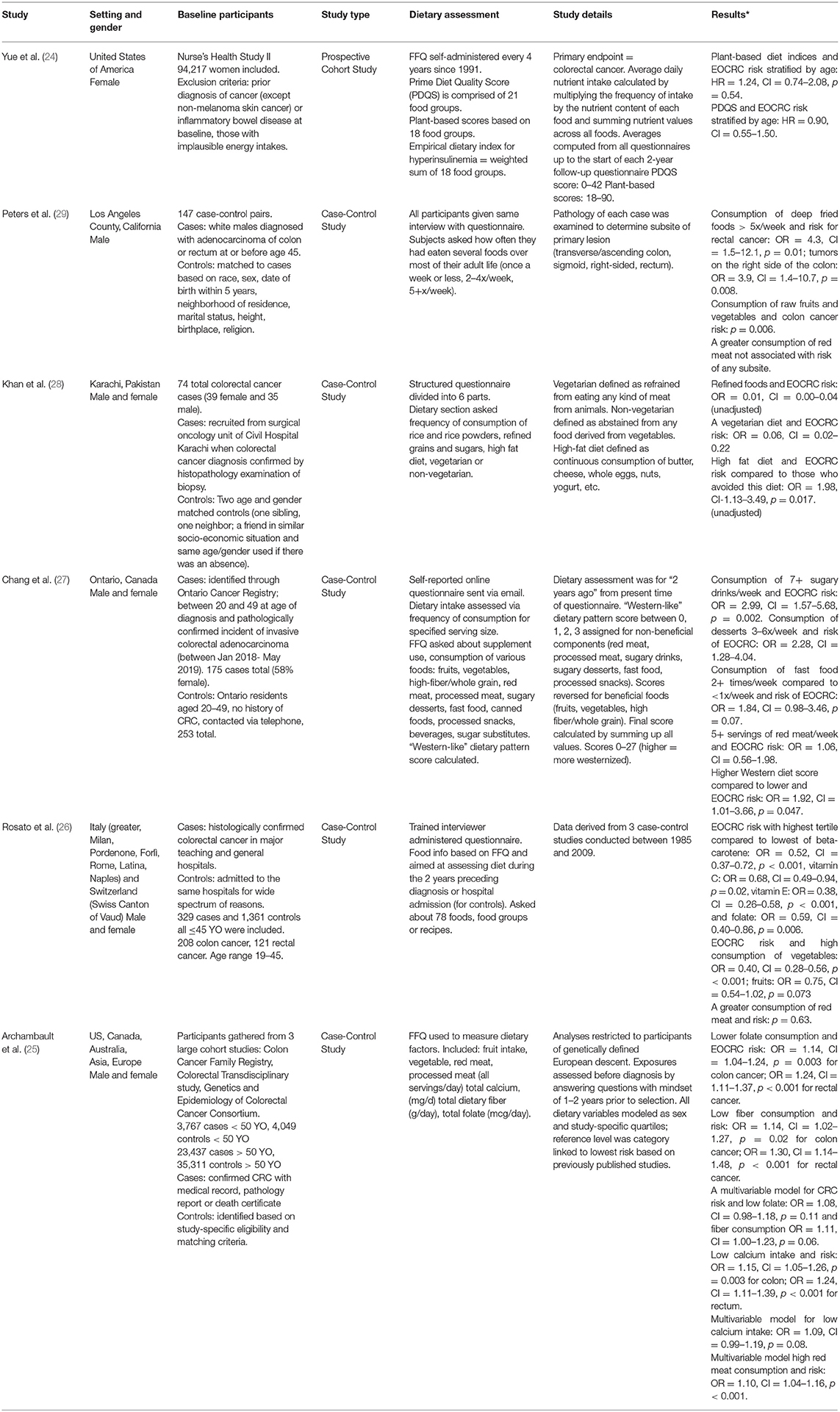
Table 3. Characteristics of included studies (early-onset colorectal cancer).
Relationship Between Dietary Patterns and Early Onset Colorectal Adenoma Risk
Two prospective cohort studies explored the relationship between dietary patterns and the risk of developing pre-cancerous colorectal adenomas (20, 23). One study investigated if women's sugar sweetened beverage consumption during adolescence had an impact on adenoma risk during adulthood (20). Results revealed a higher sugar sweetened beverage intake (per 1 serving/day) was significantly associated with increased risk of high adenomas (OR = 1.134, CI = 1.01–1.79, p = 0.044). Higher total fructose intake (per 5% of calories) during adolescence was associated with an increased risk of high-risk adenomas (OR = 1.30, CI = 1.06–1.60, p = 0.012). No significant relationship was observed for artificially sweetened beverages or fruit juice during adolescence and adenoma risk, nor sugar and sugar sweetened beverages during adulthood. The positive associations with sugar intake and adenoma risk were stronger in women who had low fruit intake (<1.3 servings/day) during adolescence than women with high fruit intake. The second study compared dietary patterns of those under 50 years old to those over 50 years old with metachronous colorectal adenomas, defined as sequential adenomas that develop more than 6 months after the initial adenoma, to identify if any foods were significantly associated with a higher risk (23). Compared to adults over 50 years old, men and women under 50 years old who developed colorectal adenomas were more likely to have a high intake of protein (p = 0.03), total fat (p < 0.00), monounsaturated fat (p = 0.001), polyunsaturated fat (p = 0.049), red meat (p = 0.001) and consume a more pro-inflammatory diet than those over 50 years old (p < 0.001). However, a multivariate logistic regression model stratified by age group showed no effect that a high red meat consumption (>511 g/week) was associated with risk of developing metachronous colorectal adenomas for those under 50 years old (OR = 0.84, CI = 0.233–3.021, p = 0.79) (23).
Relationship Between Diet Quality and Early Onset Colorectal Adenoma Risk
Two prospective cohort studies examined the relationship between diet quality and adenoma risk (21, 22), and showed that the overall quality of the diet was inversely associated with risk. Zheng et al. categorized diets into either Western or Prudent, as well as derived scores for the Dietary Approaches to Stop Hypertension Diet (DASH), Alternative Mediterranean diet (AMED) and Alternative Healthy Eating Index-2010 (AHEI-2010) (22). Scores were derived by categorizing FFQ data into groups and performing a factor analysis. Those in the highest quintile for the Western diet has an increased risk of early-onset adenomas with a higher malignant potential, whereas the DASH, AMED, Prudent and AHEI-2010 showed significant inverse associations for risk of developing early-onset high-risk adenomas (OR = 1.67, CI = 1.18–2.37, p = 0.01; OR = 0.65, CI = 0.45–0.93, p = 0.009; OR = 0.55, CI = 0.38–0.79, p = 0.007; OR = 0.69, CI = 0.48–0.98, p = 0.03, OR = 0.71, CI = 0.51–1.01, p = 0.01, respectively) (22). The Western, Prudent, DASH and AHEI-2010 diets showed significant associations for the risk of advanced adenomas in the distal colon and rectum (OR = 1.65, CI = 1.14–2.38, p = 0.01; OR = 0.68, CI = 0.47–0.99, p = 0.04; OR = 0.63, CI = 0.42–0.94, p = 0.01; OR = 0.71, CI = 0.49–1.03, p = 0.02, respectively).
Through the use of scoring diets for their potential to enrich sulfur-metabolizing bacteria, Nguyen et al. found women in the highest quartile of sulfur microbial diets (most enrichment potential) had an increased risk of early-onset adenomas (OR = 1.13, CI = 1.10–1.56, p = 0.02) (21). Adenomas in the proximal colon and those characterized with a tubulovillous or villous histology showed a larger association with adherence to a high sulfur microbial diet (OR = 1.58, CI = 1.17–2.14, p = 0.01; OR = 1.65, CI = 1.12–2.43, p = 0.04, respectively) (21).
Association Between Micronutrients and Early Onset Colorectal Cancer Risk
The relationship between micronutrient intake and the risk of developing EOCRC was explored in two studies (25, 26). In a case-control study, Rosato et al. found those in the highest tertile of consumption of beta-carotene, vitamin C, vitamin E and folate had a protective effect against EOCRC risk compared to those in the lowest tertile (OR = 0.52, CI = 0.37–0.72, p < 0.001; OR = 0.68, CI = 0.49–0.94, p = 0.02; OR = 0.38, CI = 0.26–0.58, p < 0.001; OR = 0.59, CI = 0.40–0.86, p = 0.006, respectively) (26). Archambault et al. found that lower folate consumption was linked to a greater risk of EOCRC by subsite (OR = 1.14, CI = 1.04–1.24, p = 0.003 for colon cancer, OR = 1.24, CI = 1.11–1.37, p < 0.001 for rectal cancer), as well as lower fiber consumption (OR = 1.14, CI = 1.02–1.27, p = 0.02 for colon cancer, OR = 1.30, CI = 1.14–1.48, p < 0.001 for rectal cancer) (25). However, a multivariable model adjusted for age, sex, study, family history and total energy consumption failed to show significance for low folate and fiber consumption, but trended toward an increased colorectal cancer risk (p = 0.11 and p = 0.06, respectively) (25). Archambault observed an increased risk of colon cancer and rectal cancer for low calcium intake (OR = 1.15, CI = 1.05–1.26, p = 0.003; OR = 1.24, CI = 1.11–1.39, p < 0.001, respectively) and a trend toward higher risk was observed in a multivariable model (OR = 1.09, CI = 0.99–1.19, p = 0.08) (25).
Relationship Between Dietary Patterns and Early Onset Colorectal Cancer Risk
Four studies explored how different dietary patterns were associated with EOCRC risk (26–29). In a case control study, consumption of deep fried foods > 5x/week was associated with an elevated risk for rectal cancer and tumors on the right side of the colon (OR = 4.3, CI = 1.5–12.1, p = 0.01; OR = 3.9, CI = 1.4–10.7, p = 0.008, respectively) (29). Consumption of refined foods including corn flakes, pastas, noodles, pizza and refined sugars, appeared protective against EOCRC as reported in the Khan et al. case-control study (OR = 0.01, CI = 0.00–0.04) (28). Greater consumption of sugary drinks (7+ drinks/week) and desserts (3–6x/week) was associated with an elevated risk of EOCRC (OR = 2.99, CI = 1.57–5.68, p = 0.002; OR = 2.28, CI = 1.28–4.04) (27). Consumption of fast food two or more times/week showed a suggestive, but not significant, association with increased risk of EOCRC compared to consumption <1x/week (OR = 1.84, CI = 0.98–3.46, p = 0.07) (27). Two studies categorized diets according to their adherence to a plant-based diet. Khan et al. found a vegetarian diet contributed a protective affect against EOCRC (OR = 0.06, CI = 0.02–0.22) (28); however, a plant-based diet was not associated with CRC (HR = 1.24, CI = 0.72–2.16, p = 0.54) in a study with only female participants (24). Two studies observed a protective effect against EOCRC for increased citrus fruit and vegetable consumption (p = 0.006) (29) (Vegetables: OR = 0.40, CI = 0.28–0.56, p < 0.001, Citrus Fruits: OR = 0.61, CI = 0.45–0.84, p = 0.002) (26). A greater consumption of red meat was associated with an increased risk of EOCRC in a study with only female participants (OR = 1.10, CI = 1.04–1.16, p < 0.001) (25); however, three studies that included male participants showed no association (26, 27, 29).
Relationship Between Diet Quality and Early Onset Colorectal Cancer Risk
Two studies examined the relationship between diet quality and EOCRC risk (27, 28) and showed that the overall quality of the diet was inversely associated with the risk of developing CRC at a young age. Categorizing and scoring diets according to their similarities to a Western diet showed an elevated risk of developing EOCRC for those with the higher Western diet score compared to lower (OR = 1.92, CI = 1.01–3.66, p = 0.047) (27). Additionally, a high fat diet was significantly associated with a higher chance of developing EOCRC compared to those who did not consume this diet (OR = 1.98, CI = 1.13–3.49, p = 0.017) (28).
Discussion
Currently, there is extensive evidence pointing to an association between certain dietary factors and risk for developing older-onset colorectal cancer. However, there is much less known about the modifiable risk factors for developing early-onset colorectal cancer. As such, it has been difficult to identify groups of people at risk for EOCRC based on modifiable risk factors, such as dietary patterns, and flag them for early screening or other preventative actions. Unlike other published systematic reviews, this systematic review focused solely on diet as a risk factor for developing or preventing early-onset colorectal cancer and colorectal adenomas.
Approximately 85% of early-onset colorectal cancer cases develop through the conventional adenoma-carcinoma sequence (20). Therefore, it was important to investigate dietary risk factors for both potentially precancerous early-onset colorectal adenomas and EOCRC. One of the four studies that analyzed risk factors for colorectal adenomas focused on sugar sweetened beverage (SSB) consumption both during high school and adult life (20). It was shown that a high SSB and fructose consumption during high school significantly increased the risk of developing colorectal adenomas before the age of 50. Additionally, women who consumed less fruit during adolescence were shown to have stronger associations for adenoma risk than those who consumed more. Fruits and liquid fructose have different intestinal release rates due to the fiber content and other cellular components of whole fruits (20). Liquid fructose is rapidly digested, and large amounts of fructose at one time can exceed small intestine uptake capacity and overflow to the colon (20). In addition to the study looking at adenomas, one study found similar results for SSB consumption and EOCRC risk. A higher consumption of sugar sweetened beverages was significantly associated with an increased risk of EOCRC (27). It is believed an overall unhealthy diet combined with excessive sugar intake may exacerbate chronic insulin release, thereby promoting colorectal carcinogenesis. High fructose corn syrup, the main sweetener in beverages since the 1980s, has negative impacts on insulin sensitivity and the gut microbiota, which may play a role in EOCRC etiology (27).
One study investigated how a diet which promotes sulfur-metabolizing bacteria influences early-onset adenoma risk. It was found that a high sulfur microbial diet score significantly increased the risk of developing a colorectal adenoma before age 50 (21). A higher score indicated that a participant consumed more foods associated with the enrichment of sulfur-metabolizing microbes in the gut, which may lead to a higher production of pro-carcinogenic hydrogen sulfide (21). Processed meats were included in the category of foods positively associated with the enrichment of sulfur-metabolizing bacteria. Plant-based sulfur sources are distinct from animal-based sources because they are composed of primarily cancer protective compounds, such as glucosinolate, and are negatively associated with the enrichment of the bacteria (21).
Red meat and processed meat are well documented risk factors for colorectal cancer (23) due to their genotoxic effects (30). Despite this, red meat consumption was not shown to be a risk factor for early-onset colorectal adenomas and results were mixed for EOCRC. It was speculated that the lack of significance may have been due to the fact that individuals under 50 years old have experienced a shorter duration of meat exposure, which may not be long enough to produce a significant effect (23). Three large cohort studies agree that red meat consumption may not impact adenoma development until later in life (23, 31, 32). It has not yet been confirmed at what stage of carcinogenesis red meat plays its largest role. However, processed, barbequed and cured meats did increase the risk of EOCRC (27, 29). This is consistent with the hypothesis that N-nitroso compound formation increases CRC risk (29), and that N-nitroso compounds are highly genotoxic (33). Existing evidence is in line with the findings that processed meat is directly associated to EOCRC risk (26, 34).
It has been well established in Westernized countries but also globally over the past several decades that dietary patterns in younger generations are shifting toward more unhealthy diets, such as a Western diet (25). Diets are becoming increasingly heavy in meat, fats, oils, added sugars and sweeteners while vegetables, fruits and whole grain consumption is decreasing (22, 25). The Western diet is characterized by low-fiber, high fat and high sugar, and is known to be more pro-inflammatory than it is anti-inflammatory (27). In the studies reviewed, a high Western diet score was associated with an increased risk of adenoma development, specifically those in the distal colon and rectum (22). A recent cohort study found that a Western diet induces both inflammation and gut dysbiosis, potentially explaining its role in increasing early onset colorectal adenoma risk (27). Consistent with the studies on adenoma risk, a Western-like diet was related to an increased risk of EOCRC (27). A Western diet is more strongly associated with tumors of molecular subtypes common in EOCRC (22). These molecular subtypes are more likely to originate through the conventional adenoma-carcinoma sequence (21), therefore it is not surprising that a Western diet was consistent with an increased risk of both EOCRC and adenomas. Western diets have also been shown to be associated with traditional CRC (22). The results of a Western diet on EOCRC risk suggest overall poor diet quality may also be a risk factor for early-onset CRC (27), which is currently considered a putative risk factor for traditional CRC.
In line with the findings that poor diet quality is a risk factor for EOCRC are studies reporting that a high-fat diet was associated with an increased risk for EOCRC (28), and common among those who developed adenomas before age 50 (23). This is consistent with data that found an increased risk of EOCRC to be associated with a high intake of processed foods, as these foods are often high in fat (29). Unhealthy diets, characterized by high fat and processed food consumption, are linked to obesity which has been shown to be associated with the risk of EOCRC in previous studies (22, 35). However, direct evidence for the effect of consuming a high-fat diet on EOCRC risk is needed.
Healthy diets, as indicated by recommendation based dietary indices, have been shown to be associated with a lower risk of traditional CRC (24). Adherence to the Prudent diet, alternative Mediterranean diet, AHEI-2010 and DASH diet, were shown to have an inverse association with early onset colorectal adenoma risk in both the distal colon and rectum. The DASH diet is characterized by being high in low fat dairy, which is a good source of calcium. High calcium intake has been shown to be inversely related with distal colon cancer, potentially because of its capability to reduce cell proliferation and promote cell differentiation and apoptosis (22). This is in agreement with the two studies included in this review which found low calcium intakes increased EOCRC risk (25). The protective effect of calcium is consistent with evidence for traditional CRC, signifying calcium may have implications for chemoprevention research (27).
It is important to note alcohol consumption was considered when scoring both the sulfur microbial diet and the alternative Mediterranean diet (21, 22). This review excluded most data related to alcohol consumption; however, the intake of these beverages was not able to be separated out of the published results. It cannot be ruled out that the significance seen in these studies' results may have been influenced by the alcoholic beverage consumption, a known risk factor for CRC (36). The sulfur microbial diet score was influenced by liquor and beer intake. Liquor was considered one of the food groups positively associated with the enrichment of sulfur-metabolizing bacteria. Beer was included in the group of foods negatively associated with the enrichment of sulfur-metabolizing bacteria. A higher sulfur microbial diet score indicates one's diet is more enriched for sulfur-metabolizing bacteria, which could enhance the production of pro-carcinogenic compounds (21). Therefore, liquor was considered to be more harmful when it comes to enhancing the risk of CRC and adenomas, and beer may be more protective. Zheng et al. measured alcohol consumption when scoring diets according to the AMED score (22). A traditional Mediterranean diet includes moderate consumption of ethanol, typically in the form of wine (37). Resveratrol, found in the skin and seeds of grapes, is one of multiple polyphenolic compounds found in wine. Polyphenolic content is higher in red wines but varies by the grape varietal and the vinification process (38). Resveratrol's proposed cancer protecting properties include defending against reactive oxidative species induced damage and repressing platelet aggregation (39). Resveratrol in combination with other polyphenolic compounds is believed to be useful in advanced stages of cancer through its ability to deregulate many pathways affecting cancer cell growth and oncogenic signaling (40). Additionally, resveratrol has been shown to have beneficial effects for tumor prevention (41, 42). A greater adherence to a Mediterranean diet has been linked to lower levels of cancer mortality (43). Previously published studies have demonstrated mixed results when it comes to alcohol consumption and traditional CRC. A retrospective analysis performed by Crockett et al. found that moderate intake of wine was inversely associated with CRC (44). However, multiple meta-analyses have found that alcohol increases CRC risk in a linear dose-related manner (45–47). According to the study included in this review, a higher AMED score was associated with a lower risk of early-onset colorectal adenomas, although the amount of alcohol consumed by participants was not listed (22).
Other micronutrients shown to lower the risk for EOCRC include beta-carotene, vitamin, C, vitamin E and folate (26). A second study found that low folate and fiber intake increased the risk for developing EOCRC (25). It was unsurprising high intakes of citrus fruits and vegetables also appeared protective against EOCRC because they are high in fiber and micronutrients, like the ones described previously (26, 29). The positive association between fruit and vegetable intake and EOCRC risk is in line with existing evidence (26). The anti-inflammatory compounds found in various fruits and vegetables may help modulate cancer cell proliferation and apoptosis (28). One study found the consumption of fresh fruit and raw vegetables to be protective in the colon, but not the rectum, which is in agreement with previous case-control studies (29, 48). Despite the positive results from fruit and vegetable consumption, vegetarian diets produced mixed results. One study found a vegetarian diet to be protective, whereas another saw no effect (24, 28). It is possible that the plant-based diet indices used to measure vegetarian diets in one study is tailored more toward critical factors for heart disease, and therefore may be less important for cancer (24).
Many of the studies examined colorectal cancer and adenoma by subsite. The subdivisions of the colorectal area have different blood supplies, patterns of motility and physiological function (29). It has been hypothesized that the specific mechanisms of carcinogenesis parallel the physiological differences (29). This may explain why different areas of the colorectal region were affected by different dietary habits. Because EOCRC typically occurs in the distal colon and rectum, it may be more important to focus on the dietary habits which exhibit risk factors for cancers occurring in these regions. From the studies investigated in this review, the Western diet was associated with an increase in colorectal adenoma risk in the distal and rectal regions (22). The Prudent, DASH and AHEI-2010 diets were protective against adenoma risk in distal and rectal region (22). Low folate, fiber and calcium intakes were related to a higher risk of early-onset rectal cancer, as well as high levels of fast food consumption (25, 29).
Listed in Table 4 are the covariates adjusted for in the included studies. Half of the studies in this review included BMI as a covariate adjustment. BMI was considered a potential confounder due to the link between obesity and traditional CRC, as well as data suggesting obesity is significantly associated with increased EOCRC risk (10, 49). The five studies which did not adjust for obesity cannot rule out the possibility that participants BMI may have impacted their findings. It has been hypothesized that obesity is linked to EOCRC cases because the increasing prevalence of obesity parallels the increasing incidence of EOCRC (49). Obesity has been shown to be associated with earlier onset of metabolic conditions and diseases such as insulin resistance, type 2 diabetes, high blood pressure and dyslipidemia (50). These metabolic conditions may be underlying mechanisms for colorectal neoplasia. The time of BMI measurement relative to disease diagnosis is important when studying EOCRC, as weight loss is a common symptom (6). Therefore, BMI measured at the time of diagnosis may not be as relevant to BMI before diagnosis (49).
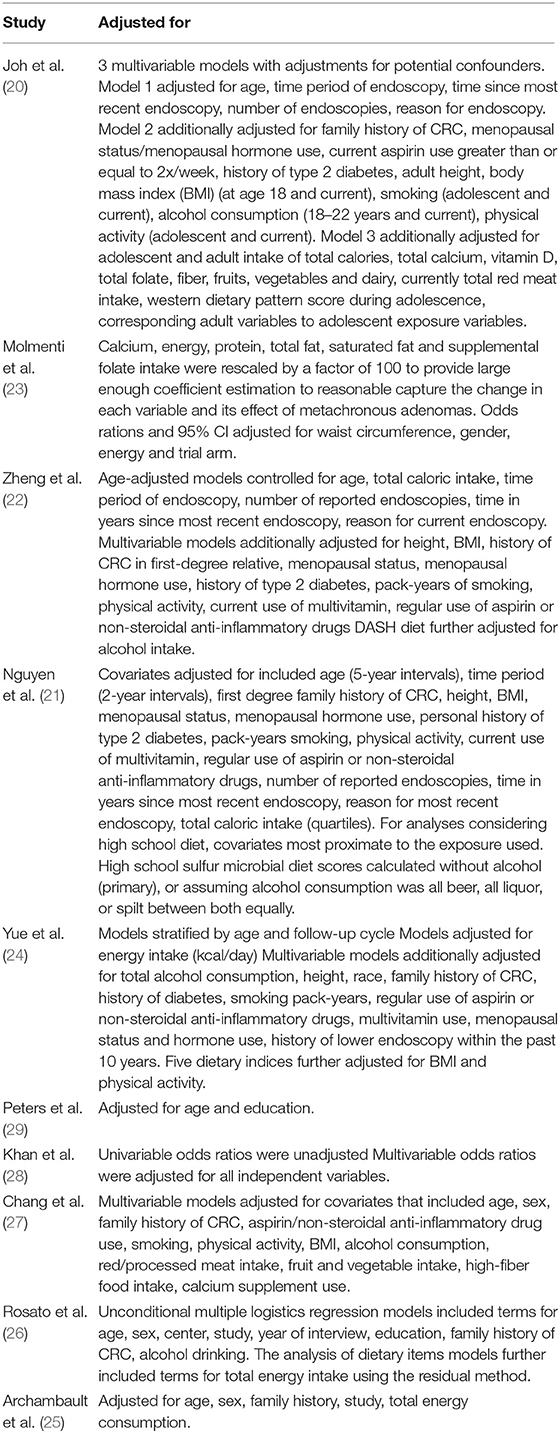
Table 4. Data adjustments for included studies.
Of the ten included studies, four exclusively included women (20–22, 24), four were over 50% women (25–28), one exclusively included males (29), and one was predominantly men (62% of participants under 50 years old and 68% of participants over 50 years old were male) (23). EOCRC differs from older-onset CRC in that it affects men and women equally; however, it has not been determined if they also share the same risk factors (36). Due to the heterogeneity of the studies and their range of dietary measures, it was difficult to determine if specific diet components or approaches affected men and women's risk differently. A study with 62% male participants (23) and two studies with 100% female participants (22, 27) both found a pro-inflammatory diet to increase the risk of EOCRC and adenomas. Furthermore, red meat's effect on EOCRC and adenoma risk was not statistically significant when comparing results from men and women (23, 25, 27, 29). When analyzing the demographics of the included studies', nine out of the ten studies included mostly white males and females (20–27, 29), and the tenth included only Pakistani participants (28). The studies with mostly white participants consistently found pro-inflammatory diets, such as the Western diet, and unhealthy foods including SSB, fast food and desserts to have a negative impact of EOCRC and early-onset adenoma risk (20, 22, 23, 27, 29). Healthy dietary choices such as fruits, vegetables and consuming high levels of various micronutrients appeared to be protective against EOCRC and adenoma risk in the studies with white participants (24–26, 29). When comparing the two predominant demographics of the included studies, refined foods and high fat foods increased EOCRC and adenoma risk, and a more plant-focused diet was protective against EOCRC and adenoma risk in both demographics (23, 26–29). The lack of diversity in the studies' participants limited the generalizability of the results, making it difficult to determine if similar dietary habits would affect other races in a comparable manner.
The strengths of this systematic review include reporting according to the PRISMA guidelines. Several limitations exist as well. While this review provides a summary of the most current evidence regarding diet and early-onset colorectal cancer, there were a limited number of studies included, and a meta-analysis could not be conducted due to the heterogeneity of the studies. A lack of dietary assessment of patients with EOCRC is a limitation of the published research. The age range of included participants is a limitation of this review. Currently, there is no clear or widely accepted consensus for a definition of age groups for EOCRC (51). This study intended to adhere to the definition of early-onset as before screening age, i.e., < 50 years old, however; it was difficult due to the limited number of published studies. The mean age of cases in one study was 52.2, with 76.5% of cases being diagnosed before age 55 (20). The average age of cases in a second study was 41.47, with the standard deviation of ages from the mean was 15.54, therefore adults up to the age of 57 were included (28). Long follow-up studies with young individuals are cost-prohibitive; therefore there is a lack of diverse populations studied for EOCRC and adenomas. Four of the included studies utilized the NHSII cohort for their data, limiting the diversity of the populations studied (20–22, 24). Many of the included studies share similar limitations. While FFQs are commonly used in nutrition research, they still are associated with recall bias, misclassification and measurement error. Though multiple countries were included across the studies, most participants were white and often female, reducing the generalizability of these results. It appears EOCRC is similar between males and females, therefore the predominant inclusion of females is not a limitation of the results (7, 52, 53). The possibility of residual confounding factors cannot be ruled out in the observational studies due to the nature of the studies.
The rising incidence in early-onset colorectal cancer cases makes identifying risk factors imperative. More detailed studies on the differences in dietary index and CRC risk by anatomic sites in young adults are needed. Large prospective cohort studies with long follow-ups are needed to confirm results and to help screen for strategies that can be targeted at this sub-population. Elucidating modifiable risk factors for early-onset colorectal cancer, such as diet, is necessary to help slow the rising incidence and preserve life years for the population.
Conclusions
This review demonstrated that various dietary habits, some of which are already confirmed risk factors for traditional colorectal cancer, may be risk factors or protective against early-onset colorectal cancer and adenomas. These results should be interpreted with caution, as a meta-analysis was not able to be conducted and the generalizability of the results is limited to the populations studied. The lack of knowledge on EOCRC risk factors make the associations identified in this review helpful starting points for dietary habits to be examined in future studies. By identifying modifiable risk factors for EOCRC, such as the dietary choices analyzed in this review, high-risk populations can be targeted for early intervention and prevention methods.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Author Contributions
MG conceived of the work, contributed to the writing, and offered critical comments. KC performed data analysis and wrote the first draft of the manuscript. AF, MH, and EL provided critical revisions to the content. All authors contributed to the article and approved the submitted version.
Funding
This material is based upon work that was supported by the National Institute of Food and Agriculture, U.S. Department of Agriculture, Hatch/Multistate project Accession ALA044-1-18037 to MG. Research reported in this publication was supported by the National Center for Advancing Translational Research of the National Institutes of Health under award number UL1TR003096 to MG and EL.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. (2017) 66:683–91. doi: 10.1136/gutjnl-2015-310912
3. Saad El Din K, Loree JM, Sayre EC, Gill S, Brown CJ, Dau H, et al. Trends in the epidemiology of young-onset colorectal cancer: a worldwide systematic review. BMC Cancer. (2020) 20:288. doi: 10.1186/s12885-020-06766-9
4. Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. (2020) 70:145–64. doi: 10.3322/caac.21601
5. Venugopal A, Stoffel EM. Colorectal cancer in young adults. Curr Treat Options Gastroenterol. (2019) 17:89–98. doi: 10.1007/s11938-019-00219-4
6. Siegel RL, Jakubowski CD, Fedewa SA, Davis A, Azad NS. Colorectal cancer in the young: epidemiology, prevention, management. Am Soc Clin Oncol Educ Book. (2020) 40:1–14. doi: 10.1200/EDBK_279901
7. Yeo H, Betel D, Abelson JS, Zheng XE, Yantiss R, Shah MA. Early-onset colorectal cancer is distinct from traditional colorectal cancer. Clin Colorectal Cancer. (2017) 16:293–9.e6. doi: 10.1016/j.clcc.2017.06.002
8. Cavestro GM, Mannucci A, Zuppardo RA, Di Leo M, Stoffel E, Tonon G. Early onset sporadic colorectal cancer: worrisome trends and oncogenic features. Dig Liver Dis. (2018) 50:521–32. doi: 10.1016/j.dld.2018.02.009
9. Ahnen DJ, Wade SW, Jones WF, Sifri R, Mendoza Silveiras J, Greenamyer J, et al. The increasing incidence of young-onset colorectal cancer: a call to action. Mayo Clin Proc. (2014) 89:216–24. doi: 10.1016/j.mayocp.2013.09.006
10. Vajdic CM, MacInnis RJ, Canfell K, Hull P, Arriaga ME, Hirani V, et al. The future colorectal cancer burden attributable to modifiable behaviors: a pooled cohort study. JNCI Cancer Spectr. (2018) 2:pky033. doi: 10.1093/jncics/pky033
11. Johnson CM, Wei C, Ensor JE, Smolenski DJ, Amos CI, Levin B, et al. Meta-analyses of colorectal cancer risk factors. Cancer Causes Control. (2013) 24:1207–22. doi: 10.1007/s10552-013-0201-5
12. Schwingshackl L, Schwedhelm C, Hoffmann G, Knüppel S, Laure Preterre A, Iqbal K, et al. Food groups and risk of colorectal cancer. Int J Cancer. (2018) 142:1748–58. doi: 10.1002/ijc.31198
13. Stoffel EM, Murphy CC. Epidemiology and mechanisms of the increasing incidence of colon and rectal cancers in young adults. Gastroenterology. (2020) 158:341–53. doi: 10.1053/j.gastro.2019.07.055
14. Brenner DR, Ruan Y, Shaw E, De P, Heitman SJ, Hilsden RJ. Increasing colorectal cancer incidence trends among younger adults in Canada. Prev Med. (2017) 105:345–9. doi: 10.1016/j.ypmed.2017.10.007
15. Feletto E, Yu XQ, Lew JB, St John DJB, Jenkins MA, Macrae FA, et al. Trends in colon and rectal cancer incidence in Australia from 1982 to 2014: analysis of data on over 375,000 cases. Cancer Epidemiol Biomarkers Prev. (2019) 28:83–90. doi: 10.1158/1055-9965.EPI-18-0523
16. Chung RY, Tsoi KKF, Kyaw MH, Lui AR, Lai FTT, Sung JJ. A population-based age-period-cohort study of colorectal cancer incidence comparing Asia against the West. Cancer Epidemiol. (2019) 59:29–36. doi: 10.1016/j.canep.2019.01.007
17. Hofseth LJ, Hebert JR, Chanda A, Chen H, Love BL, Pena MM, et al. Early-onset colorectal cancer: initial clues and current views. Nat Rev Gastroenterol Hepatol. (2020) 17:352–64. doi: 10.1038/s41575-019-0253-4
18. Sijtsma FP, Meyer KA, Steffen LM, Shikany JM, Van Horn L, Harnack L, et al. Longitudinal trends in diet and effects of sex, race, and education on dietary quality score change: the Coronary Artery Risk Development in Young Adults study. Am J Clin Nutr. (2012) 95:580–6. doi: 10.3945/ajcn.111.020719
19. Marriott BP, Cole N, Lee E. National estimates of dietary fructose intake increased from 1977 to 2004 in the United States. J Nutr. (2009) 139:1228s−35s. doi: 10.3945/jn.108.098277
20. Joh HK, Lee DH, Hur J, Nimptsch K, Chang Y, Joung H, et al. Simple sugar and sugar-sweetened beverage intake during adolescence and risk of colorectal cancer precursors. Gastroenterology. (2021) 161:128–42 e20. doi: 10.1053/j.gastro.2021.03.028
21. Nguyen LH, Cao Y, Hur J, Mehta RS, Sikavi DR, Wang Y, et al. The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors. Gastroenterology. (2021) 161:1423–32.e4. doi: 10.1053/j.gastro.2021.07.008
22. Zheng X, Hur J, Nguyen LH, Liu J, Song M, Wu K, et al. Comprehensive assessment of diet quality and risk of precursors of early-onset colorectal cancer. J Natl Cancer Inst. (2021) 113:543–52. doi: 10.1093/jnci/djaa164
23. Molmenti CLS, Hibler EA, Yang J, Kolb JM, Yang J, Hussain M, et al. Characteristics and risk factors for early-onset metachronous colorectal adenoma. Colorectal Cancer. (2020) 9:CRC33. doi: 10.2217/crc-2020-0019
24. Yue Y, Hur J, Cao Y, Tabung FK, Wang M, Wu K, et al. Prospective evaluation of dietary and lifestyle pattern indices with risk of colorectal cancer in a cohort of younger women. Ann Oncol. (2021) 32:778–86. doi: 10.1016/j.annonc.2021.03.200
25. Archambault AN, Lin Y, Jeon J, Harrison TA, Bishop DT, Brenner H, et al. Nongenetic determinants of risk for early-onset colorectal cancer. JNCI Cancer Spectr. (2021) 5:pkab029. doi: 10.1093/jncics/pkab029
26. Rosato V, Bosetti C, Levi F, Polesel J, Zucchetto A, Negri E, et al. Risk factors for young-onset colorectal cancer. Cancer Causes Control. (2013) 24:335–41. doi: 10.1007/s10552-012-0119-3
27. Chang VC, Cotterchio M, De P, Tinmouth J. Risk factors for early-onset colorectal cancer: a population-based case-control study in Ontario, Canada. Cancer Causes Control. (2021) 32:1063–83. doi: 10.1007/s10552-021-01456-8
28. Khan NA, Hussain M, ur Rahman A, Farooqui WA, Rasheed A, Memon AS. Dietary practices, addictive behavior and bowel habits and risk of early onset colorectal cancer: a case control study. Asian Pac J Cancer Prev. (2015) 16:7967–73. doi: 10.7314/APJCP.2015.16.17.7967
29. Peters RK, Garabrant DH, Yu MC, Mack TM. A case-control study of occupational and dietary factors in colorectal cancer in young men by subsite. Cancer Res. (1989) 49:5459–68.
30. Pelland-St-Pierre L, Sernoskie SC, Verner M-A, Ho V. Genotoxic effect of meat consumption: a mini review. Mutat Res Genetic Toxicol Environ Mutagen. (2021) 863–4:503311. doi: 10.1016/j.mrgentox.2021.503311
31. Nimptsch K, Bernstein AM, Giovannucci E, Fuchs CS, Willett WC, Wu K. Dietary intakes of red meat, poultry, and fish during high school and risk of colorectal adenomas in women. Am J Epidemiol. (2013) 178:172–83. doi: 10.1093/aje/kwt099
32. Ruder EH, Thiébaut AC, Thompson FE, Potischman N, Subar AF, Park Y, et al. Adolescent and mid-life diet: risk of colorectal cancer in the NIH-AARP Diet and Health Study. Am J Clin Nutr. (2011) 94:1607–19. doi: 10.3945/ajcn.111.020701
33. Kobayashi J. Effect of diet and gut environment on the gastrointestinal formation of N-nitroso compounds: a review. Nitric Oxide. (2018) 73:66–73. doi: 10.1016/j.niox.2017.06.001
34. Huxley RR, Ansary-Moghaddam A, Clifton P, Czernichow S, Parr CL, Woodward M. The impact of dietary and lifestyle risk factors on risk of colorectal cancer: a quantitative overview of the epidemiological evidence. Int J Cancer. (2009) 125:171–80. doi: 10.1002/ijc.24343
35. Liu PH, Wu K, Ng K, Zauber AG, Nguyen LH, Song M, et al. Association of obesity with risk of early-onset colorectal cancer among women. JAMA Oncol. (2019) 5:37–44. doi: 10.1001/jamaoncol.2018.4280
36. Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. (2019) 16:713–32. doi: 10.1038/s41575-019-0189-8
37. Willett WC, Sacks F, Trichopoulou A, Drescher G, Ferro-Luzzi A, Helsing E, et al. Mediterranean diet pyramid: a cultural model for healthy eating. Am J Clin Nutr. (1995) 61:1402S−6S. doi: 10.1093/ajcn/61.6.1402S
38. Cordova AC, Sumpio BE. Polyphenols are medicine: is it time to prescribe red wine for our patients? Int J Angiol. (2009) 18:111–7. doi: 10.1055/s-0031-1278336
39. Kuršvietiene L, Stanevičiene I, Mongirdiene A, Bernatoniene J. Multiplicity of effects and health benefits of resveratrol. Medicina. (2016) 52:148–55. doi: 10.1016/j.medici.2016.03.003
40. Singh CK, George J, Ahmad N. Resveratrol-based combinatorial strategies for cancer management. Ann N Y Acad Sci. (2013) 1290:113–21. doi: 10.1111/nyas.12160
41. Tsunoda T, Ishikura S, Doi K, Matsuzaki H, Iwaihara Y, Shirasawa S. Resveratrol induces luminal apoptosis of human colorectal cancer HCT116 cells in three-dimensional culture. Anticancer Res. (2014) 34:4551–5.
42. Kontou N, Psaltopoulou T, Soupos N, Polychronopoulos E, Xinopoulos D, Linos A, et al. Alcohol consumption and colorectal cancer in a Mediterranean population: a case-control study. Dis Colon Rectum. (2012) 55:703–10. doi: 10.1097/DCR.0b013e31824e612a
43. Thomson CA, McCullough ML, Wertheim BC, Chlebowski RT, Martinez ME, Stefanick ML, et al. Nutrition and physical activity cancer prevention guidelines, cancer risk, and mortality in the women's health initiative. Cancer Prev Res. (2014) 7:42–53. doi: 10.1158/1940-6207.CAPR-13-0258
44. Crockett SD, Long MD, Dellon ES, Martin CF, Galanko JA, Sandler RS. Inverse relationship between moderate alcohol intake and rectal cancer: analysis of the North Carolina Colon Cancer Study. Dis Colon Rectum. (2011) 54:887–94. doi: 10.1007/DCR.0b013e3182125577
45. Bagnardi V, Blangiardo M, La Vecchia C, Corrao G. A meta-analysis of alcohol drinking and cancer risk. Br J Cancer. (2001) 85:1700–5. doi: 10.1054/bjoc.2001.2140
46. Corrao G, Bagnardi V, Zambon A, La Vecchia C. A meta-analysis of alcohol consumption and the risk of 15 diseases. Prev Med. (2004) 38:613–9. doi: 10.1016/j.ypmed.2003.11.027
47. Cho E, Smith-Warner SA, Ritz J, van den Brandt PA, Colditz GA, Folsom AR, et al. Alcohol intake and colorectal cancer: a pooled analysis of 8 cohort studies. Ann Intern Med. (2004) 140:603–13. doi: 10.7326/0003-4819-140-8-200404200-00007
48. Kune S, Kune GA, Watson LF. Case-control study of dietary etiological factors: the Melbourne Colorectal Cancer Study. Nutr Cancer. (1987) 9:21–42. doi: 10.1080/01635588709513908
49. O'Sullivan DE, Sutherland RL, Town S, Chow K, Fan J, Forbes N, et al. Risk factors for early-onset colorectal cancer: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2021) 20:1229–40.e5. doi: 10.1016/j.cgh.2021.01.037
50. Nimptsch K, Wu K. Is timing important? The role of diet and lifestyle during early life on colorectal neoplasia. Curr Colorectal Cancer Rep. (2018) 14:1–11. doi: 10.1007/s11888-018-0396-7
51. Mauri G, Sartore-Bianchi A, Russo AG, Marsoni S, Bardelli A, Siena S. Early-onset colorectal cancer in young individuals. Mol Oncol. (2019) 13:109–31. doi: 10.1002/1878-0261.12417
52. Low EE, Demb J, Liu L, Earles A, Bustamante R, Williams CD, et al. Risk factors for early-onset colorectal cancer. Gastroenterology. (2020) 159:492–501.e7. doi: 10.1053/j.gastro.2020.01.004
Keywords: colorectal cancer, early-onset, diet, dietary habits, risk factors
Citation: Carroll KL, Frugé AD, Heslin MJ, Lipke EA and Greene MW (2022) Diet as a Risk Factor for Early-Onset Colorectal Adenoma and Carcinoma: A Systematic Review. Front. Nutr. 9:896330. doi: 10.3389/fnut.2022.896330
Received: 14 March 2022; Accepted: 16 May 2022;
Published: 09 June 2022.
Edited by:
Fatima Baltazar, University of Minho, PortugalReviewed by:
Meghit Boumediene Khaled, University of Sidi-Bel-Abbès, AlgeriaMostafa Waly, Sultan Qaboos University, Oman
Copyright © 2022 Carroll, Frugé, Heslin, Lipke and Greene. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael W. Greene, mwg0006@auburn.edu