 Yaolin Song
Yaolin Song Lili Wang
Lili Wang Xiaoming Xing
Xiaoming Xing- Department of Pathology, The Affiliated Hospital of Qingdao University, Qingdao, China
Colorectal cancer (CRC) has become a major health concern in China due to its increasing incidence and mortality. This study aimed to clarify the relationship between tumor locations and the clinicopathological molecular marker features in eastern China CRC patients. We continuously collected data on 2,356 CRC patients who underwent surgical resection from January 2017 to April 2019. Right-sided colorectal cancer (RCC), was located from the cecum to the transverse colon and left-side colorectal cancer (LCRC) was located from the splenic flexure to the rectum. The clinicopathological indices (including age, sex, pTNM stage, mucinous production, and distant metastasis) and frequency of molecular markers such as KRAS, NRAS, BRAF, and microsatellite instability (MSI) were statistically analyzed between the RCC and LCRC groups. The associations between clinicopathological characters and molecular markers were also investigated. LCRC and RCC proportions in eastern China CRC patients were 81.75% and 18.25%, respectively. RCC (vs. LCRC) was more frequently observed with higher frequencies of MSI-high (MSI-H) and BRAF mutations in female and younger patients, and was closely associated with metastasis, poor differentiation, and mucinous tumors. Tumor location also showed significant differences in bowel wall infiltration degree and pTNM stage. Mutation rates of KRAS, NRAS, MSI, and BRAF were 40.15%, 3.85%, 6.31%, and 2.30%, respectively. Patients with a KRAS mutation tended to be female, had mucinous, perineural invasive, and polypoid tumor. Those with NRAS mutation tended to develop well-differentiated ulcerative tumors. The BRAF mutation was more relevant with lymph node involvement, deeper infiltration of the bowel wall, mucinous, poorly-differentiated tumor with thrombus, and perineural invasion. Furthermore, MSI-H was more commonly found in younger patients with deeper bowel wall infiltration and a poorly-differentiated polypoid tumor, whereas MSS patients tended to develop lymph node involvement, and a mucinous and perineural invasive tumor. In our study, we found that LCRC and RCC showed different features on the clinicopathological and molecular markers in eastern China CRC patients. Since our data differ from those of Western countries and other regions in China, further studies are required to clarify the regional differences of the clinicopathological and molecular markers in CRC patients.
Introduction
Colorectal cancer (CRC) is the third most common cancer, with the fourth most common cancer-related mortality worldwide (Zhang et al., 2017). In China, the incidence, mortality, and burden of CRC are all increasing due to the transition to a westernized lifestyle with obesity and physical inactivity (Center et al., 2009; Gu et al., 2018). Among Chinese patients, CRC shows the fifth highest cancer incidence in men, the fourth in women; and is fifth in cancer-related deaths in men (8.0%) and third in women (9.8%) (Feng et al., 2019).
Both genetic and environmental factors are involved in the tumorigenesis of CRC. For the past decades, studies have demonstrated that genetic molecular markers such as microsatellite instability (MSI), 18q loss of heterozygosity, and CpG island methylator phenotype (CIMP), RAS, and BRAF, among others, are closely associated with the tumorigenesis and prognosis of CRC (Sanz-Garcia et al., 2017; Saeed et al., 2019).
MSI is a genetic hypermutability condition resulting from deficient DNA mismatch repair. It is involved in various types of cancers, including colon cancer, ovarian cancer, skin cancer, and gastric cancer, among others. MSI is most frequently associated with the development of CRC and is found in about 15% of CRC tumors. RAS belongs to the proto-oncogene family that encodes three small GTPase proteins including KRAS, NRAS, and HRAS. RAS gene mutation presents in about 30% of all human cancers, and the mutation proportions of KRAS, NRAS, and HRAS are around 85%, 11-15%, and 1%, respectively (Cox et al., 2014; Chang et al., 2016). KRAS functions downstream in the epidermal growth factor receptor (EGFR) signaling pathway and is involved in cell proliferation, mutation, and cell death. KRAS mutation plays an important role in carcinogenesis, about 30-50% CRC is known to have KRAS gene mutation and the mutation positions are most frequently in codons 12 and 13, in exon 1 (Wagner et al., 2019). NRAS is closely related with KRAS; and its mutation in CRC, which is mainly located at codons 12, 13, or 61 is approximately 1-6% (Vaughn et al., 2011). BRAF is a serine kinase, downstream of KRAS, and in the MAPK signaling pathway. The most frequent mutation point of BRAF is V600E. The incidence of the BRAF V600E mutation is estimated to be about 8-10% in CRC patients (Bahrami et al., 2018; Myte et al., 2019).
CRC is anatomically divided into the right (RCC) and left CRC (LCRC) according to the location of the tumor by the border of the splenic flexure. Past studies have observed the relationship of tumor location with the development, clinicopathological characteristics, treatment, and prognosis of CRC. However, the effect of tumor location on the molecular markers of CRC still remains unclear. Recently, several studies have reported that the clinicopathological and molecular biomarkers of CRC were divergent in different regions (Giraldez et al., 2012; Perea et al., 2015). It is of great value to clarify the correlation between tumor location and genetic markers for patients in different regions. Today, most reports that study differences in molecular markers in RCC and LCRC hail from Western countries, with very few studies from eastern China.
In this study we collected data on 2,356 CRC cases from the affiliated hospital of Qingdao University, a medical center that mainly provides medical care to eastern China patients. We summarized the clinical features and molecular characteristics using RCC and LCRC. Our study provides valuable guidance and reference for the diagnosis and treatment of CRC patients in eastern China.
Materials and Methods
Patients
We continuously collected data on 2,566 CRC patients who underwent surgical resection at the Affiliated Hospital of Qingdao University from January 2017 to April 2019. RCC was defined as CRC from the cecum to the transverse colon, while LCRC was located from the splenic flexure to the rectum. As summarized in Figure 1, patients who were treated with radiotherapy or chemotherapy before surgery and who lacked accurate tumor location were excluded. Finally, 2,356 cases were selected for this study analysis. For patients who developed two or more colorectal tumors, the more advanced one was selected for this study. Informed consent was obtained from all patients, and the Ethics Committee of Qingdao University approved this study.
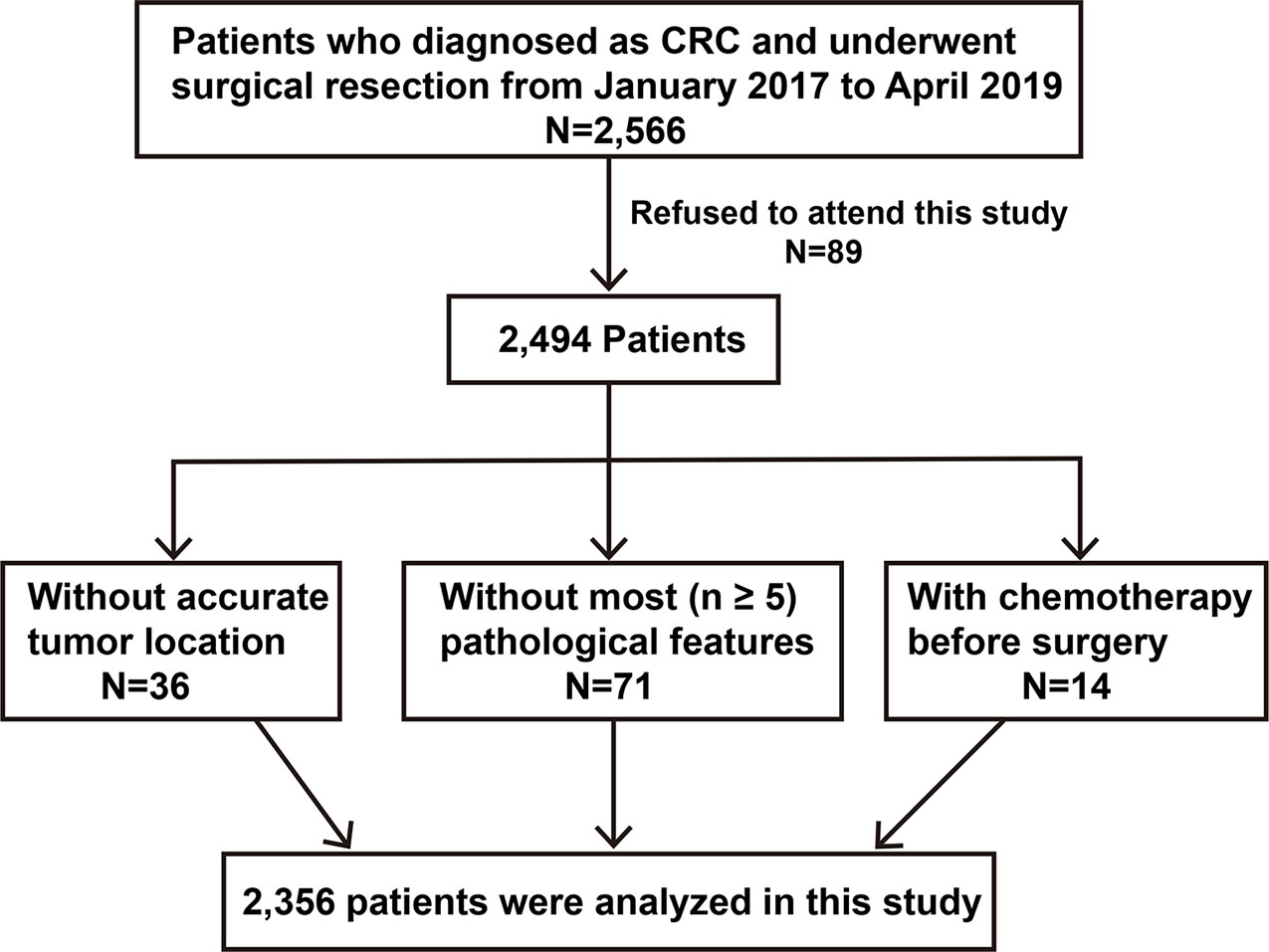
Figure 1 Diagram for the selection of CRC patients for this study. CRC, colorectal cancer.
Genomic DNA Extraction
Fresh CRC and corresponding normal tissues were fixed by 4% paraformaldehyde at 4°C overnight, paraffin embedded, and sectioned at 5 μm for hematoxylin and eosin (HE) staining for later use. The HE section was observed under the microscope; areas that were rich in tumor cells (the proportion of tumor cells was over 20%) were selected, while non-tumor areas and necrotic areas were avoided as much as possible. Tumor tissues were scraped in a clean Eppendorf tube according to the HE section, and the genomic DNA in paraffin tissues was extracted using a Tiangen paraffin embedded tissue DNA extraction kit (Tiangen Biotech, Beijing, China), according to the manufacturer’s instructions.
Microsatellite Instability
Microsatellite status was defined by six microsatellite markers (NR21, NR24, NR27, BAT25, BAT26, and MONO-27) and detected by an MSI detection kit (Microread, Beijing, China). Polymerase chain reaction (PCR) amplification was performed as follows: a total volume of 10 µl reaction mixture contained 20 ng of genomic DNA, 1 X PCR buffer, 1 X MSI Primer Mix, and Taq DNA Polymerase I. The running protocol was set up as follows: 5 min at 95°C once; 30 s at 94°C, 1 min at 60°C, and 1 min at 70°C for 30 cycles; 30 min at 60°C and forever at 15°C. The PCR production was diluted 1:6 and mixed with 9 µl ROX500 and HI-DI; after denaturation for 3 min at 96°C, the reaction complex was analyzed by DNA fragmentation assays (Applied Biosystems 3500DX, Massachusetts, USA). Allelic sizes were evaluated by GeneMapper software ver 4.1 (Thermo Fisher, Massachusetts, USA). MSI status was classified as Microsatellite stable (MSS), MSI-low (MSI-L, 1 marker unstable) and MSI-high (MSI-H, over 2 markers unstable).
Mismatch Repair (MMR) Protein Immunohistochemistry
Immunohistochemistry for mismatch repair (MMR) proteins was performed as previously described (Zhang et al., 2018). Briefly, tissues were paraffin embedded and sectioned at 3 μm. Immunohistochemistry staining for MLH1, PMS2, MLH2, and MSH6 (Ventana Medical Systems Inc, Tucson, AZ, USA) was accomplished on a BenchMark XT automated staining system (Ventana Medical Systems, Inc., Tucson, AZ, USA). Two pathologists evaluated the staining results and the standards for diagnosis were as follows: expressions of all proteins were considered proficient MMR, loss of expression of one or more of the MLH1, PMS2, MLH2, and MSH6 proteins indicating DNA mismatch repair.
KRAS, NRAS, and BRAF
Patients were tested for KRAS (codons 12 and 13), NRAS (codons 12, 13, and 61), and BRAF (V600E) to detect gene mutation; detailed detection variants are shown in Table 1. Genomic DNA was extracted from paraffin embedded tissues using a Tiangen kit (Tiangen Biotech, Beijing, China). RAS and BRAF mutations were detected by the Human RAS and BRAF mutation detection kit with PCR fluorescence probe, according to the manufacturer’s instructions (AmoyDx, Xiamen, China). Briefly, for each gene analysis, 25 µl total volume of complex mixture containing 0.3 μm primers and Taqman probes, 200 μm dNTPs, 200 μm Taq polymerase, and 90 ng of DNA. PCR amplification were set up using ABI 7500 as follows: 42°C, 5 min; 94°C, 3 min (94°C, 15 s; 60°C, 60 s); 40 cycles. The running data were analyzed by 7500 software ver 2.3 (Applied Biosystems, Massachusetts, USA).
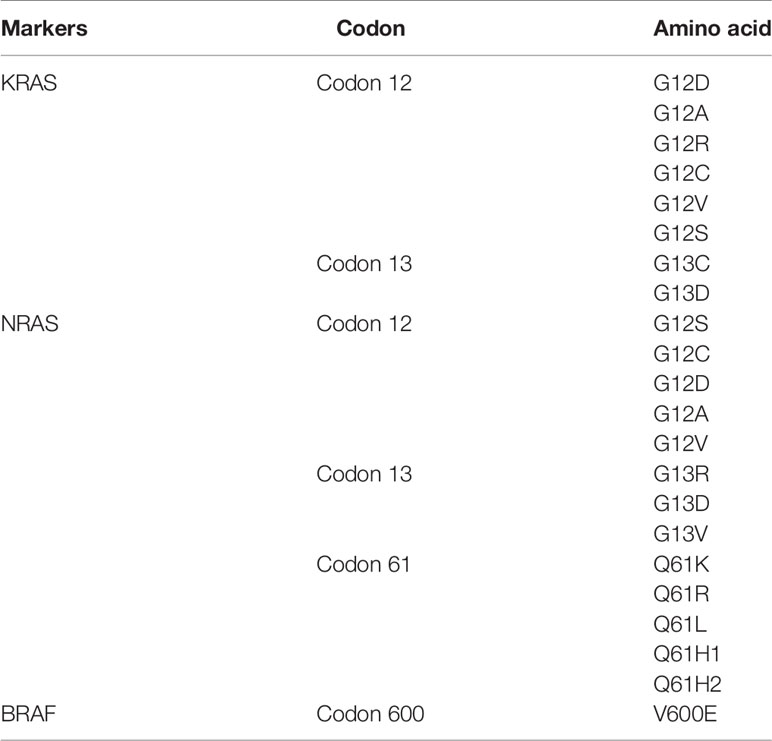
Table 1 Detection of the amino acid (AA) alternations of KRAS, NRAS, and BRAF.
Statistical Analysis
All data were analyzed by SPSS 19.0.0 statistical analysis software (IBM Corp., Armonk, NY, USA). The relationship between the two groups (RCC and LCRC) was evaluated using a standard chi-square test. Data that were not qualified for the chi-square test, were merged into the groups to reach the standard. p < 0.05 was defined as statistically significant.
Results
Clinicopathological Characteristics by RCC and LCRC
The summary of the basic clinicopathological indices with respect to the tumor location is shown in Table 2 and Figure 2. Of the 2,356 CRC patients, 81.75% (95% confidence interval [CI]: 79.8-83.7%) were LCRC and 18.25% (95% CI: 16.3-20.2%) were RCC. RCC was more frequently associated with younger female patients (p = 0.000), a higher risk of metastasis (p = 0.003), poorly-differentiated carcinoma (p = 0.000), and mucin production (p=0.000). Tumor location was also involved in the infiltration degree of the bowel wall and pTNM stage. In contrast, LCRC and RCC showed no significant differences in lymph node involvement, polypoid gross type, tumor, and perineural invasion.
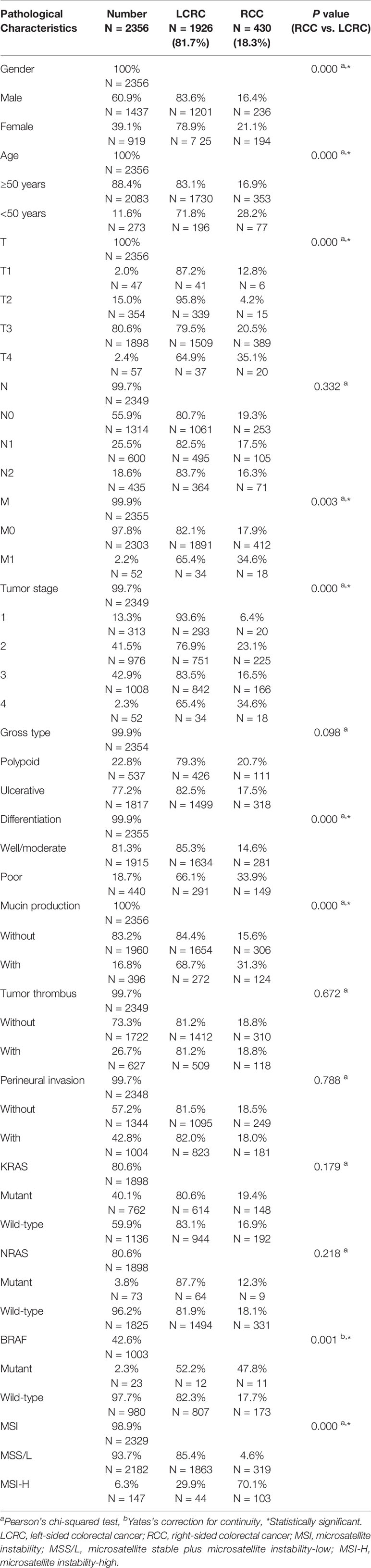
Table 2 Clinicopathological characteristics and tumor location.
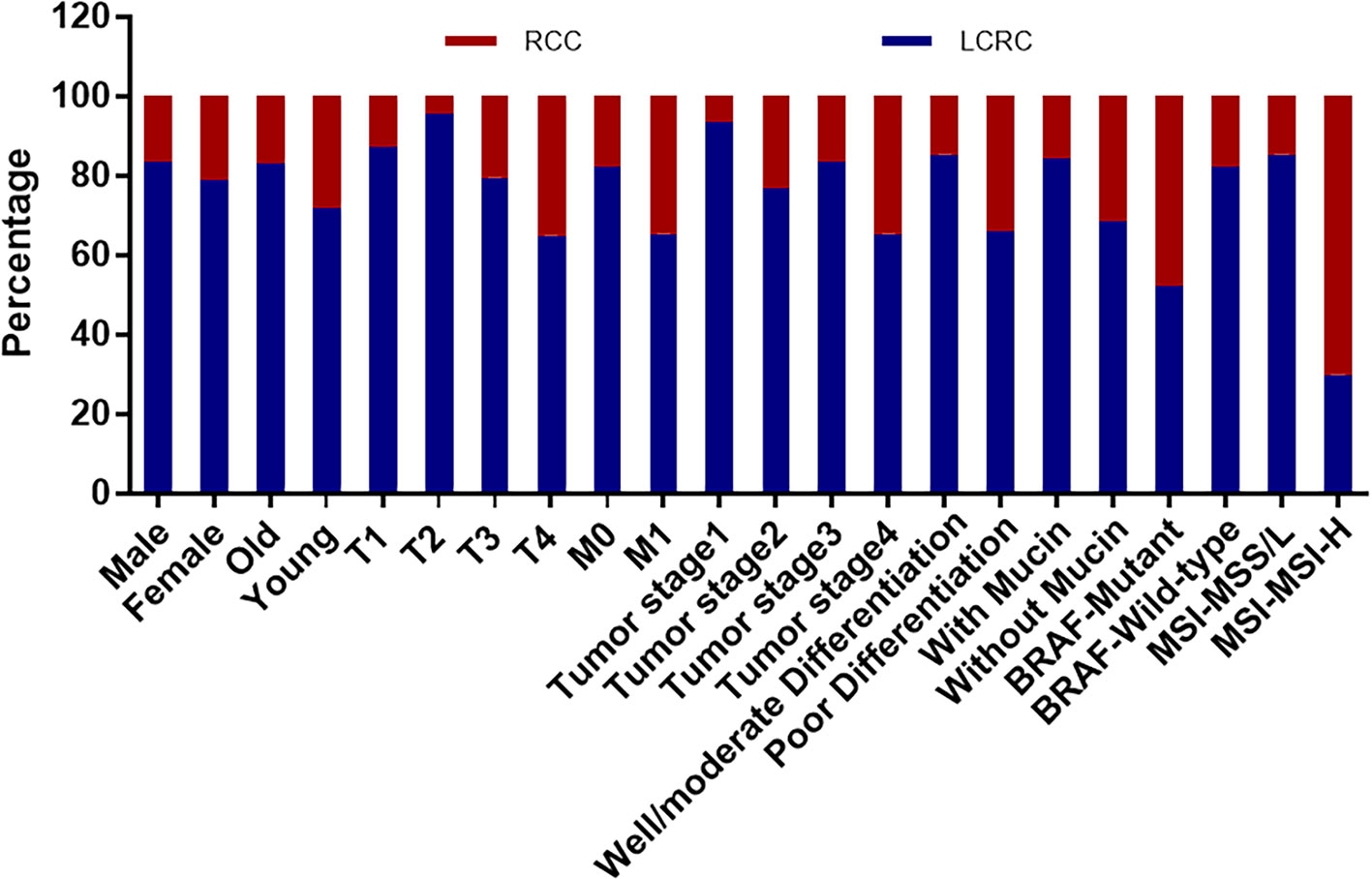
Figure 2 The correlation between clinicopathological characteristics and tumor locations that shows statistically significant difference. Compared with LCRC, RCC is more relevant with higher frequencies of MSI-high (MSI-H) and BRAF mutation, and higher incidence in female and younger patients, and was closely associated with bowel wall invasion, metastasis, poor differentiation, and mucinous tumors. (LCRC, left-sided colorectal cancer; RCC, right-sided colorectal cancer; MSI, microsatellite instability; MSS/L, microsatellite stable plus microsatellite instability-low; MSI-H, microsatellite instability-high; Old, ≥50 years old; Young, <50 years old; T, bowel wall invasion; M, metastasis).
Molecular Differences in RCC and LCRC
We checked the MSI, KRAS, NRAS, and BRAF mutation status in this study. For MSI detection, among the 2,329 cases, 757 cases were analyzed by immunohistochemistry staining for MMR proteins and 1,572 cases were analyzed by PCR; both DNA mismatch repair and MSI-H results were considered. Since MSI-L CRC showed no difference with the MSS tumor (Pawlik et al., 2004), we merged the MSI-L (n = 3) and MSS (n = 2179) tumor as MSS/L, which differed from MSI-H (n = 147). Among the 2,356 patients with CRC, the detection rates of molecular markers were 80.56% for KRAS and NRAS, 42.57% for BRAF, and 98.85% for MSI. The mutation rates for these molecular markers were 40.15%, 3.85%, 2.30%, and 6.31% for KRAS, NRAS, BRAF, and MSI, respectively. RCC was significantly associated with higher incidence of MSI-H (p = 0.000) and BRAF mutation (p = 0.001) compared with LCRC. However, there was no measurable difference between RCC and LCRC on the KRAS and NRAS mutation. Furthermore, we checked the correlation between the genetic markers and found that the KRAS mutation was accompanied with a lower mutation rate of NRAS, while the mutation status of KRAS and BRAF was incompatible, no association was found between the KRAS mutations and the BRAF mutation.
Associations Between Molecular Markers and Clinicopathological Features
We further analyzed the relationship between molecular markers and clinicopathological features. As Table 3 and Figure 3 shows, KRAS mutation more frequently occurred in female CRC patients (p = 0.003), with mucinous (p = 0.000), perineural invasive (p = 0.046), and polypoid tumor (p = 0.004). On the contrary, NRAS mutation was significantly associated with ulcerative (p = 0.043) and well/moderately-differentiated tumor (p = 0.040). BRAF mutation was more related with lymph node metastasis (p = 0.030), bowel wall invasion, mucin production (p = 0.010), tumor thrombus (p = 0.002), perineural invasion (p = 0.018), poor differentiation (p = 0.001) and MSI status including MSS/L and MSI-H. MSI-H status was more frequently involved in patients below the age of 50 (p = 0.000), had deeper bowel wall infiltration (p = 0.001), polypoid gross type (p = 0.001), and a poorly-differentiated (p = 0.000) tumor. Whereas, MSS/L status was more commonly associated with lymph node involvement (p = 0.000), mucinous (p = 0.000), and a perineural invasion (p = 0.007) tumor.
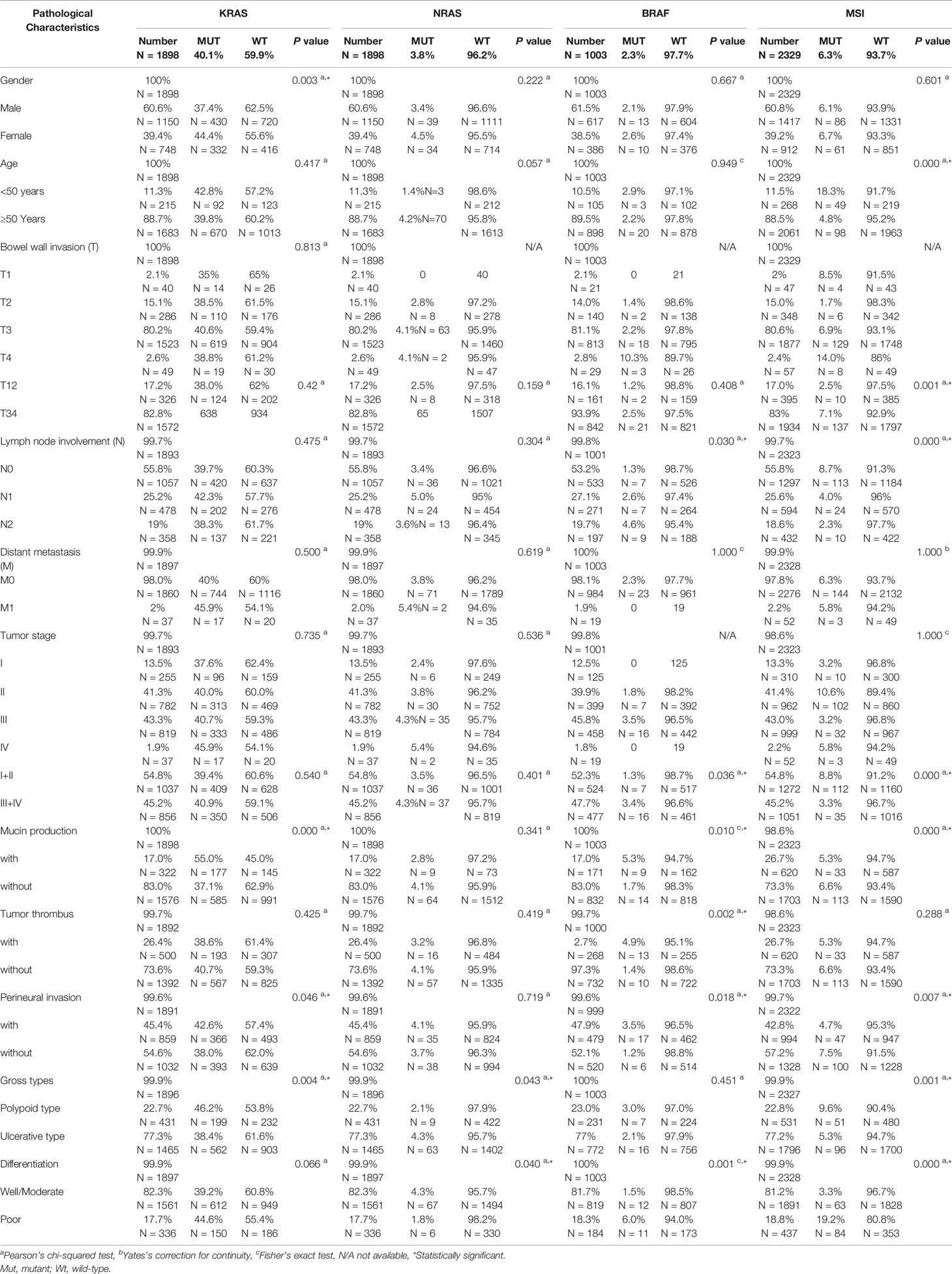
Table 3 Correlation between clinicopathological characteristics and molecular marker status.

Figure 3 The correlation between clinicopathological characteristics and molecular markers that shows statistically significant difference. KRAS mutation more commonly occurred in female patients with a mucinous, perineural invasive, and polypoid tumor while NRAS mutation is more associated with well-differentiated ulcerative tumors. BRAF mutation was more relevant to lymph node involvement, deeper infiltration of the bowel wall, mucinous, a poorly-differentiated tumor with thrombus, and perineural invasion. MSI-H was more commonly found in younger patients with deeper bowel wall infiltration and a poorly-differentiated polypoid tumor. (MSI, microsatellite instability; MSS/L, microsatellite stable plus microsatellite instability-low; MSI-H, microsatellite instability-high; Old, ≥50 years old; Young, <50 years old; T, bowel wall invasion; N, lymph node involvement; M, metastasis).
BRAF Mutation was Specifically Low in Eastern China CRC Patients
Among the 1,003 CRC patients with BRAF test, 23 patients with a positive BRAF mutation was found with a mutation rate of 2.29% - much lower than that in the published data of 8-10% (Bahrami et al., 2018; Myte et al., 2019). This result indicated that BRAF mutation rate was specifically low in eastern China patients. Also, with respect to the tumor location, the mutation rates for LCRC and RCC were 1.49% and 6.36%, respectively. We analyzed the mutation rate of BRAF in each pTNM stage and found that it was mostly detected in stage III (n = 18/23, 78.26%).
Discussion
RCC and LCRC were first proposed as two distinct tumors by Bufill (1990), from the perspective of molecular genetics. The clinical performance, prognosis, and sensitivity to targeted therapy differs significantly depending on the tumor location. For the past decade, the role of molecular markers in the diagnosis and prognosis of cancer has been increasingly prominent. Since the indices of cancer vary in different regions and people, clarifying the effect of colorectal tumor location on clinicopathological features and molecular markers in regional areas is of great value for clinicians.
In this study, for the eastern China patients, the frequency of RCC was 18.25%, lower than in previous reports from other regions in China such as Shanghai (24.4% and 25.3%), Shantou (36.9%), Tianjin (50.6%), and Guangdong (17.5%), as well as Japan (26.3% and 29.3%) (Xu et al., 2010; Watanabe et al., 2012; Liu et al., 2017; Peng et al., 2017; Qin et al., 2017; Natsume et al., 2018; Guo et al., 2019), whereas the RCC frequency in the United States was as high as 42% (Siegel et al., 2014). This finding indicates that the distribution of RCC in eastern China patients might be different compared to those of other regions in China and Western countries.
For the RCC and LCRC clinicopathological characteristics, our findings were similar to those in published data. RCC was more frequently associated with female patients, metastasis, mucinous, poorly-differentiated carcinoma, and a higher correspondence with the BRAF mutation and MSI-H status (Wangefjord et al., 2013; Li et al., 2015; Fu et al., 2019). Furthermore, our results showed that RCC was more common in younger patients who were under 50 years old, providing a diagnostic reference for clinicians.
For the molecular markers in CRC, the mutation rates of MSI-H, KRAS, and NRAS were reported to be 6-15% (Horvat and Stabuc, 2011; Gelsomino et al., 2016; Chang et al., 2017; Samstein and Chan, 2017), 38.5-40% (Natsume et al., 2018), and 1-6% respectively (Downward, 2003). In our study, the frequencies of the MSI-H (6.31%), KRAS (40.15%), and NRAS (3.85%) mutation were in accordance with those in the Western countries and other regions in China, whereas the BRAF (2.29%) mutation was specifically lower. The BRAF mutation rate was reported to be around 2.5%-6.15% in different regions of China (Peng et al., 2017; Wang et al., 2018), and 3.7-11.3% in other Asian countries (Lee et al., 2015; Fujiyoshi et al., 2017; Natsume et al., 2018), for the eastern China patients, this incidence was 2.23%, much lower than those of Western countries, reported as 17-19.4% (Hutchins et al., 2011; Loupakis et al., 2015). We analyzed the pTNM stage and found that the BRAF mutation was mostly detected at stage III which was in line with previous data (Sayagues et al., 2018). The low mutation rate in eastern China patients might be due to the regional difference and varying genetic predispositions. Further studies need to be completed to investigate the effect of environmental and genetic factors on the molecular markers. Furthermore, several reports showed that the frequency of the BRAF mutation in RCC was around 4-10% in Asia, and in our data at around 6.36%, in agreement with the published data. RCC more frequently corresponded with a higher mutation rate of MSI-H and BRAF but had no association with the KRAS and NRAS mutation. Also, as Table 4 shows, we checked the mutation status of RAS and BRAF and found them to be irreconcilable, this was in accordance with previous reports (De Roock et al., 2010).
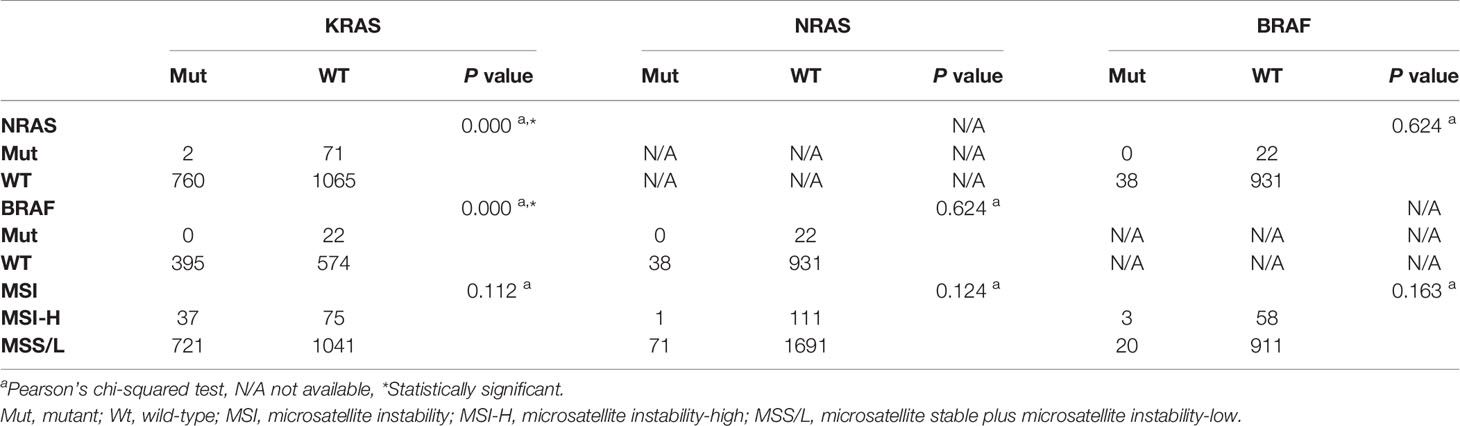
Table 4 The interactions between molecular marker status.
We additionally analyzed the correlation between the molecular markers and basic pathological features. The KRAS mutated tumor was reported to be more frequent in female patients with mucinous differentiation and polypoid growth (Wangefjord et al., 2013; Li et al., 2015). In our study, we found it was more frequently observed in female patients, accompanied with perineural invasion, mucin production, and polypoid gross type tumor, which is mainly consistent with the published data from Western countries. As another member of the RAS family, NRAS mutation is rare and shows no significant relevance with histologic features (Irahara et al., 2010); nevertheless, we discovered that it was associated with a well/moderate differentiation grade and ulcerative carcinoma. The BRAF-mutated tumor was more often related with pathologic characteristics such as a location on the right-side, lymph-node metastases, mucin component, tumor thrombus, perineural invasion, and low differentiation grade. These findings were in agreement with existing studies (Li et al., 2015). The MSI-H phenotype has been reported to be involved in poor differentiation, mucinous histology, and right-sided colon location (Battaglin et al., 2018). Moreover, we found that it was regularly observed in younger patients (<50 years old, p = 0.000), a deeper infiltration of bowel wall, and polypoid gross type tumor. The distribution of the correlations between molecular markers and histologic features in our study were not completely in accordance with the published data of Western countries and other regions in China, and we assume that this difference is a consequence of multiple sample sizes and regional diversity.
For the treatment of potentially resectable colon cancer with RAS and BRAF wild-type status, LCRC with FOLFOXIRI ± cetuximab is recommended to patients, while FOLFOXIRI ± bevacizumab is recommended for RCC patients. For patients with RAS or BRAF mutation, regardless of tumor location, FOLFOXIRI ± bevacizumab is recommended (Falcone et al., 2007).
For the palliative treatment of colon cancer, further classification has been made with respect to the tumor location. In first line treatment, patients with both KRAS, NRAS, and BRAF wild-type are suitable for intense medical treatment, doublet chemotherapy plus cetuximab is recommended to the LCRC patients and doublet chemotherapy plus bevacizumab is preferred for RCC patients (Tejpar et al., 2017). For those who are not suitable to undergo intense care but have an MSH status, immune checkpoint inhibitors are recommended. In second line treatment, despite the status of the RAS/BRAF gene, immune checkpoint inhibitors are recommended for patients with an MSH status (Diaz and Le, 2015; Overman et al., 2018). Patients who are RAS wild-type and BRAF V600E mutated are recommended a VIC regimen. In third line treatment, despite the status of the RAS and BRAF gene, fruquinitinib is recommended (Li et al., 2018; Yuan et al., 2019).
There were several limitations in our study: (1) a single medical center study; (2) lack of clinical treatment data such as applications of target drugs, chemotherapy, or radiotherapy; (3) no track of survival data; and (4) other molecular markers like CIMP, 18q loss of heterozygosity, CIMP were not included in this research.
In summary, our study collected data on 2,356 cases of CRC and analyzed the relationship between tumor location, clinicopathological, and molecular features. We found that RCC (vs LCRC) was significantly associated with a higher incidence of the MSI-H and BRAF mutation but showed no measurable difference on the KRAS and NRAS mutation. Considering the limited reports published on the correlation between tumor location and molecular markers for eastern China patients, our study provides a valuable reference for physicians and researchers to study CRC.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
Informed consent of all patients was obtained and the Ethic Committee of Qingdao University approved this study.
Author Contributions
YS and XX conceived and designed the study. XX contributed reagents, protocols, and materials. WR, GL, YX, and XW conducted the experiments and analyzed the raw experimental data. LZ provided pathological diagnosis. YS and LW collected and statistically analyzed the data. YS wrote the paper. XX modified the manuscript.
Funding
This work was supported with funding from the National Natural Science Foundation of China (Grant No.81201947, 81972329); the Natural Science Foundation of Shandong (Grant No. ZR2009CM014); the Excellent Young Scientist Foundation of Shandong Province (Grant No. 2006BSB14001); and the Qingdao minsheng science and technology project (Grant No. 17-3-3-38-nsh).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank all the patients and their families.
Abbreviations
CIMP, CpG island methylator phenotype; CRC, colorectal cancer; HE, hematoxylin and eosin; LCRC, left-sided colorectal cancer; MMR, mismatch repair; MSI, microsatellite instability; MSI-H, microsatellite instability-high; MSS/L, microsatellite stable plus microsatellite instability-low; PCR, polymerase chain reaction; RCC, right-sided colorectal cancer.
References
Bahrami, A., Hesari, A., Khazaei, M., Hassanian, S. M., Ferns, G. A., Avan, A. (2018). The therapeutic potential of targeting the BRAF mutation in patients with colorectal cancer. J. Cell Physiol. 233, 2162–2169. doi: 10.1002/jcp.25952
Battaglin, F., Naseem, M., Lenz, H. J., Salem, M. E. (2018). Microsatellite instability in colorectal cancer: overview of its clinical significance and novel perspectives. Clin. Adv. Hematol. Oncol. 16, 735–745.
Bufill, J. A. (1990). Colorectal cancer: evidence for distinct genetic categories based on proximal or distal tumor location. Ann. Intern. Med. 113, 779–788. doi: 10.7326/0003-4819-113-10-779
Center, M. M., Jemal, A., Smith, R. A., Ward, E. (2009). Worldwide variations in colorectal cancer. CA Cancer J. Clin. 59, 366–378. doi: 10.3322/caac.20038
Chang, Y. Y., Lin, P. C., Lin, H. H., Lin, J. K., Chen, W. S., Jiang, J. K., et al. (2016). Mutation spectra of RAS gene family in colorectal cancer. Am. J. Surg. 212, 537–544 e533. doi: 10.1016/j.amjsurg.2016.02.013
Chang, L., Chang, M., Chang, H. M., Chang, F. (2017). Expending role of microsatellite instability in diagnosis and treatment of colorectal cancers. J. Gastrointest. Cancer. 48, 305–313. doi: 10.1007/s12029-017-9991-0
Cox, A. D., Fesik, S. W., Kimmelman, A. C., Luo, J., Der, C. J. (2014). Drugging the undruggable RAS: mission possible? Nat. Rev. Drug Discov. 13, 828–851. doi: 10.1038/nrd4389
De Roock, W., Claes, B., Bernasconi, D., De Schutter, J., Biesmans, B., Fountzilas, G., et al. (2010). Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol. 11, 753–762. doi: 10.1016/S1470-2045(10)70130-3
Diaz, L. A., Jr., Le, D. T. (2015). PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 373, 1979. doi: 10.1056/NEJMc1510353
Downward, J. (2003). Targeting RAS signalling pathways in cancer therapy. Nat. Rev. Cancer. 3, 11–22. doi: 10.1038/nrc969
Falcone, A., Ricci, S., Brunetti, I., Pfanner, E., Allegrini, G., Barbara, C., et al. (2007). Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: the gruppo oncologico nord ovest. J. Clin. Oncol. 25, 1670–1676. doi: 10.1200/JCO.2006.09.0928
Feng, R. M., Zong, Y. N., Cao, S. M., Xu, R. H. (2019). Current cancer situation in China: good or bad news from the 2018 global cancer statistics? Cancer Commun. (Lond). 39, 22. doi: 10.1186/s40880-019-0368-6
Fu, X., Huang, Y., Fan, X., Deng, Y., Liu, H., Zou, H., et al. (2019). Demographic trends and KRAS/BRAF(V600E) mutations in colorectal cancer patients of South China: a single-site report. Int. J. Cancer. 144, 2109–2117. doi: 10.1002/ijc.31973
Fujiyoshi, K., Yamamoto, G., Takahashi, A., Arai, Y., Yamada, M., Kakuta, M., et al. (2017). High concordance rate of KRAS/BRAF mutations and MSI-H between primary colorectal cancer and corresponding metastases. Oncol. Rep. 37, 785–792. doi: 10.3892/or.2016.5323
Gelsomino, F., Barbolini, M., Spallanzani, A., Pugliese, G., Cascinu, S. (2016). The evolving role of microsatellite instability in colorectal cancer: a review. Cancer Treat. Rev. 51, 19–26. doi: 10.1016/j.ctrv.2016.10.005
Giraldez, M. D., Lopez-Doriga, A., Bujanda, L., Abuli, A., Bessa, X., Fernandez-Rozadilla, C., et al. (2012). Susceptibility genetic variants associated with early-onset colorectal cancer. Carcinogenesis 33, 613–619. doi: 10.1093/carcin/bgs009
Gu, M. J., Huang, Q. C., Bao, C. Z., Li, Y. J., Li, X. Q., Ye, D., et al. (2018). Attributable causes of colorectal cancer in China. BMC Cancer 18, 38. doi: 10.1186/s12885-017-3968-z
Guo, D., Li, X., Xie, A., Cao, Q., Zhang, J., Zhang, F., et al. (2019). Differences in oncological outcomes and inflammatory biomarkers between right-sided and left-sided stage I-III colorectal adenocarcinoma. J. Clin. Lab. Anal. e23132, 1–11. doi: 10.1002/jcla.23132
Horvat, M., Stabuc, B. (2011). Microsatellite instability in colorectal cancer. Radiol. Oncol. 45, 75–81. doi: 10.2478/v10019-011-0005-8
Hutchins, G., Southward, K., Handley, K., Magill, L., Beaumont, C., Stahlschmidt, J., et al. (2011). Value of mismatch repair, KRAS, and BRAF mutations in predicting recurrence and benefits from chemotherapy in colorectal cancer. J. Clin. Oncol. 29, 1261–1270. doi: 10.1200/JCO.2010.30.1366
Irahara, N., Baba, Y., Nosho, K., Shima, K., Yan, L., Dias-Santagata, D., et al. (2010). NRAS mutations are rare in colorectal cancer. Diagn. Mol. Pathol. 19, 157–163. doi: 10.1097/PDM.0b013e3181c93fd1
Lee, D. W., Kim, K. J., Han, S. W., Lee, H. J., Rhee, Y. Y., Bae, J. M., et al. (2015). KRAS mutation is associated with worse prognosis in stage III or high-risk stage II colon cancer patients treated with adjuvant FOLFOX. Ann. Surg. Oncol. 22, 187–194. doi: 10.1245/s10434-014-3826-z
Li, W., Qiu, T., Zhi, W., Shi, S., Zou, S., Ling, Y., et al. (2015). Colorectal carcinomas with KRAS codon 12 mutation are associated with more advanced tumor stages. BMC Cancer. 15, 340. doi: .10.1186/s12885-015-1345-3
Li, J., Qin, S., Xu, R. H., Shen, L., Xu, J., Bai, Y., et al. (2018). Effect of fruquintinib vs placebo on overall survival in patients with previously treated metastatic colorectal cancer: the FRESCO randomized clinical trial. JAMA 319, 2486–2496. doi: 10.1001/jama.2018.7855
Liu, S. S., Shi, Q., Li, H. J., Yang, W., Han, S. S., Zong, S. Q., et al. (2017). Right- and left-sided colorectal cancers respond differently to traditional Chinese medicine. World J. Gastroenterol. 23, 7618–7625. doi: 10.3748/wjg.v23.i42.7618
Loupakis, F., Yang, D., Yau, L., Feng, S., Cremolini, C., Zhang, W., et al. (2015). Primary tumor location as a prognostic factor in metastatic colorectal cancer. J. Natl. Cancer Inst. 107, 1–9. doi: 10.1093/jnci/dju427
Myte, R., Gylling, B., Haggstrom, J., Haggstrom, C., Zingmark, C., Lofgren Burstrom, A., et al. (2019). Metabolic factors and the risk of colorectal cancer by KRAS and BRAF mutation status. Int. J. Cancer. 145, 327–337. doi: 10.1002/ijc.32104
Natsume, S., Yamaguchi, T., Takao, M., Iijima, T., Wakaume, R., Takahashi, K., et al. (2018). Clinicopathological and molecular differences between right-sided and left-sided colorectal cancer in Japanese patients. Jpn. J. Clin. Oncol. 48, 609–618. doi: 10.1093/jjco/hyy069
Overman, M. J., Lonardi, S., Wong, K. Y. M., Lenz, H. J., Gelsomino, F., Aglietta, M., et al. (2018). Durable clinical benefit with nivolumab plus ipilimumab in DNA mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer. J. Clin. Oncol. 36, 773–779. doi: 10.1200/JCO.2017.76.9901
Pawlik, T. M., Raut, C. P., Rodriguez-Bigas, M. A. (2004). Colorectal carcinogenesis: MSI-H versus MSI-L. Dis. Markers 20, 199–206. doi: 10.1155/2004/368680
Peng, J., Huang, D., Poston, G., Ma, X., Wang, R., Sheng, W., et al. (2017). The molecular heterogeneity of sporadic colorectal cancer with different tumor sites in Chinese patients. Oncotarget 8, 49076–49083. doi: 10.18632/oncotarget.16176
Perea, J., Cano, J. M., Rueda, D., Garcia, J. L., Inglada, L., Osorio, I., et al. (2015). Classifying early-onset colorectal cancer according to tumor location: new potential subcategories to explore. Am. J. Cancer Res. 5, 2308–2313.
Qin, Q., Yang, L., Sun, Y. K., Ying, J. M., Song, Y., Zhang, W., et al. (2017). Comparison of 627 patients with right- and left-sided colon cancer in China: Differences in clinicopathology, recurrence, and survival. Chronic Dis. Transl. Med. 3, 51–59. doi: 10.1016/j.cdtm.2017.02.004
Saeed, O., Lopez-Beltran, A., Fisher, K. W., Scarpelli, M., Montironi, R., Cimadamore, A., et al. (2019). RAS genes in colorectal carcinoma: pathogenesis, testing guidelines and treatment implications. J. Clin. Pathol. 72, 135–139. doi: 10.1136/jclinpath-2018-205471
Samstein, R. M., Chan, T. A. (2017). Dissecting microsatellite instability in colorectal cancer: one size does not fit all. Genome Med. 9, 45. doi: 10.1186/s13073-017-0438-9
Sanz-Garcia, E., Argiles, G., Elez, E., Tabernero, J. (2017). BRAF mutant colorectal cancer: prognosis, treatment, and new perspectives. Ann. Oncol. 28, 2648–2657. doi: 10.1093/annonc/mdx401
Sayagues, J. M., Del Carmen, S., Del Mar Abad, M., Corchete, L. A., Bengoechea, O., Anduaga, M. F., et al. (2018). Combined assessment of the TNM stage and BRAF mutational status at diagnosis in sporadic colorectal cancer patients. Oncotarget 9, 24081–24096. doi: 10.18632/oncotarget.25300
Siegel, R., Desantis, C., Jemal, A. (2014). Colorectal cancer statistics 2014. CA Cancer J. Clin. 64, 104–117. doi: 10.3322/caac.21220
Tejpar, S., Stintzing, S., Ciardiello, F., Tabernero, J., Van Cutsem, E., Beier, F., et al. (2017). Prognostic and predictive relevance of primary tumor location in patients with RAS wild-type metastatic colorectal cancer: retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA Oncol. 3, 194–201. doi: 10.1001/jamaoncol.2016.3797
Vaughn, C. P., Zobell, S. D., Furtado, L. V., Baker, C. L., Samowitz, W. S. (2011). Frequency of KRAS, BRAF, and NRAS mutations in colorectal cancer. Genes Chromosomes Cancer. 50, 307–312. doi: 10.1002/gcc.20854
Wagner, S., Vlachogiannis, G., De Haven Brandon, A., Valenti, M., Box, G., Jenkins, L., et al. (2019). Suppression of interferon gene expression overcomes resistance to MEK inhibition in KRAS-mutant colorectal cancer. Oncogene 38, 1717–1733. doi: 10.1038/s41388-018-0554-z
Wang, Y., Liu, H., Hou, Y., Zhou, X., Liang, L., Zhang, Z., et al. (2018). Performance validation of an amplicon-based targeted next-generation sequencing assay and mutation profiling of 648 Chinese colorectal cancer patients. Virchows Arch. 472, 959–968. doi: 10.1007/s00428-018-2359-4
Wangefjord, S., Sundstrom, M., Zendehrokh, N., Lindquist, K. E., Nodin, B., Jirstrom, K., et al. (2013). Sex differences in the prognostic significance of KRAS codons 12 and 13, and BRAF mutations in colorectal cancer: a cohort study. Biol. Sex Differ. 4, 17. doi: 10.1186/2042-6410-4-17
Watanabe, T., Itabashi, M., Shimada, Y., Tanaka, S., Ito, Y., Ajioka, Y., et al. (2012). Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 17, 1–29. doi: 10.1007/s10147-011-0315-2
Xu, A. G., Yu, Z. J., Jiang, B., Wang, X. Y., Zhong, X. H., Liu, J. H., et al. (2010). Colorectal cancer in Guangdong Province of China: a demographic and anatomic survey. World J. Gastroenterol. 16, 960–965. doi: 10.3748/wjg.v16.i8.960
Yuan, Y., Wang, X., Chen, G., Wang, Y., Sheng, W., Li, X., et al. (2019). Updates in version 2019 of CSCO guidelines for colorectal cancer from version 2018. Chin. J. Cancer Res. 31, 423–425. doi: 10.21147/j.issn.1000-9604.2019.03.03
Zhang, Y., Chen, Z., Li, J. (2017). The current status of treatment for colorectal cancer in China: a systematic review. Med. (Baltimore) 96, e8242. doi: 10.1097/MD.0000000000008242
Keywords: colorectal cancer, tumor location, clinicopathological character, RAS, BRAF, microsatellite instability
Citation: Song Y, Wang L, Ran W, Li G, Xiao Y, Wang X, Zhang L and Xing X (2020) Effect of Tumor Location on Clinicopathological and Molecular Markers in Colorectal Cancer in Eastern China Patients: An Analysis of 2,356 Cases. Front. Genet. 11:96. doi: 10.3389/fgene.2020.00096
Received: 27 September 2019; Accepted: 28 January 2020;
Published: 25 February 2020.
Edited by:
Xianwen Ren, Peking University, ChinaReviewed by:
Fuhai Li, Washington University in St. Louis, United StatesYongcui Wang, Northwest Institute of Plateau Biology (CAS), China
Copyright © 2020 Song, Wang, Ran, Li, Xiao, Wang, Zhang and Xing. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoming Xing, edithxing@126.com; Xingxm@qduhospital.cn