Are you Concerned? Patient Testimonials in Medical Communication Affect Healthy Recipients' Emotions and Memory
 Claudia Sassenrath
Claudia Sassenrath Hannah Greving2
Hannah Greving2  Kai Sassenberg
Kai Sassenberg- 1Social Processes Lab, Leibniz-Institut für Wissensmedien, Tübingen, Germany
- 2Knowledge Construction Lab, Leibniz-Institut für Wissensmedien, Tübingen, Germany
- 3School of Science, University of Tübingen, Tübingen, Germany
Medical communication and health care intervention programs often include testimonials (i.e., an account of individuals' experiences) when addressing health-related topics. Numerous findings provide evidence of the effectiveness of such testimonials on intentions for health behavior change. However, little is known about whether and how testimonials affect healthy lay people's reception of health information (e.g., in journalistic reports about medical innovations). The present studies tested whether using patients vs. doctors as testimonial protagonists in communication affects unconcerned recipients' affective experiences and their memory performance regarding text content. Two experiments (Prestudy: N = 43; Main Experiment: N = 97, university student samples) demonstrated that using patients as protagonists elicited stronger negative and weaker positive emotions in recipients than using doctors as protagonists. Results of one of the experiments further suggested that the affective experience influenced recipients' memory performance so that less positive and more negative DBS-related information was remembered when patients were protagonists, due to elicited negative emotions. The findings are discussed with regard to their implications for medical communication.
Introduction
Medical communication and health care intervention programs often include testimonials (i.e., accounts of individuals' experiences, commonly from a first-person perspective; cf. Winterbottom et al., 2008), because they affect individuals' health behavior decisions, such as their intention to change their health behavior. For example, a testimonial report can increase individuals' perceptions of salience of risky health behaviors (e.g., Rothman et al., 1999). Moreover, testimonials seem to affect recipients' decisions and intentions for behavioral change if they are vivid and come from a person who is much like the recipient with whom the recipient can identify (Dillard and Main, 2013). Subsequently, perceived barriers to health care prevention activities involving effort are reduced (Dillard et al., 2010). Finally, testimonials can even affect actual behavior: After reading a testimonial about colorectal cancer, recipients in a study by Lipkus et al. (2003) reported perceiving the disease as more severe compared to a control group, and were then more likely to undergo a screening test 6 months later.
Therefore, testimonials are frequently used in medical communication and health behavior change in recipients affected by the topic in question. However, information about diseases and treatments is also consumed by unconcerned individuals. For instance, many newspapers have a regular page on health issues and medical research is frequently covered by different media (e.g., McCauley et al., 2013). What healthy and unconcerned lay people take from this communication might affect their future behavior (e.g., they may be concerned with the respective disease despite their health or they may want to give advice to somebody else). Research has not yet studied the impact of testimonials on unconcerned recipients of health communication. Therefore, the current studies aimed to fill this gap. In addition, we also aimed to systematically investigate the impact of testimonials on recipients' experienced affect and their memory regarding the reported contents. This was in order to identify potential candidates for the underlying mechanisms by which testimonials assert a specific influence on recipients.
In summary, it is not yet known whether and how including testimonials affects knowledge transfer in unconcerned recipients. The present studies therefore systematically examine whether and how including different types of testimonials (doctors vs. patients) in medical communication affects unconcerned recipients' affective experiences and their memory performance as an indicator of knowledge transfer. The studies extend existing literature, because the effect of testimonials (a) on unconcerned lay people (i.e., healthy individuals) in contrast to potentially concerned individuals (i.e., individuals who might be concerned with the medical content) is investigated and (b) the processes underlying this specific effect are studied.
Experts vs. Lay Persons Testimonials in Medical Communication
In the context of medical treatments, patients and doctors are natural protagonists of testimonials. The first are likely perceived as lay persons and the latter as experts, who differ in factual knowledge (Ericsson and Smith, 1991; e.g., Bromme et al., 2004). According to French et al. (1959) classical model of the basis of social power, doctors should be perceived as more powerful (compared to patients) by unconcerned individuals, due to their factual knowledge. Construal level theory (e.g., Trope and Liberman, 2010) argues that power increases the social distance and powerholders are represented more abstractly due to this distance (Smith and Trope, 2006; Liviatan et al., 2008). For the current context, this theoretical approach implies that unconcerned individuals will perceive doctors as more psychologically distant to themselves and that they will represent doctors and what they say in a more abstract manner (compared to patients).
Both perceived distance and abstractness of representations should elicit the same effect in recipients. Specifically, regarding the effects of social distance, the theories of self-expansion (cf. Aron and Aron, 1996) and cognitive interdependence (cf. Agnew et al., 1998) are informative. They posit that the closer individuals are to each other the more likely they are to empathize with each other's perspectives (Aron et al., 1992). In the case of medical communication the difference in perceived distance or closeness between doctors and patients as testimonials, should result in more perspective taking for patient testimonials than for doctor testimonials. Thus, unconcerned individuals should resonate more when learning about the experiences of a patient than when learning about the experiences of a doctor. Specifically, positive or negative information about a certain medical treatment given by a patient as testimonial should influence recipients' emotions more than the same reports given by a doctor as a testimonial. This is due to the doctors' expert status and accordingly their power which leads to a perception of greater distance between them and the recipients. This, in turn, renders perspective taking and shared emotions less likely compared to when the information is reported by a patient as a testimonial.
To be more specific, if a patient (compared to a doctor) reports feeling disappointed and negative about a medical treatment, this should more likely elicit empathy. In turn, patients' reports should also elicit negative feelings regarding the treatment. In general, the differential effects of reports using proximate vs. distant testimonials (i.e., lay people vs. experts) should elicit positive and negative emotions. However, in the specific contexts of medical innovations, the proximate others are patients and thus individuals that are in a negative state (as they are in need of medical treatment). This led us to the following predictions:
Hypothesis 1: Recipients will experience stronger negative and weaker positive emotions when they are faced with negative reports from patients (compared to doctors) as testimonials. Emotions will differ less in response to patients and doctors in case of positive reports.
We predicted the lack of a difference in case of positive reports, because the positive effect of the treatment we used as topic of medical communication in our study is that it at best reduces suffering (i.e., it is a palliative treatment), but it does not cure the disease.
Recall of Medical Communication
Research has addressed different factors facilitating recall of health-related information. For instance, the less complex the language and the more concrete presentations of health-related information (e.g., by including adequate visual cues and illustrations), the better the information are better recalled, especially by older adults (Kessels, 2003; cf. van Weert et al., 2011; Bol et al., 2014). However, rather than focusing on the language or content of the health-related messages, we aimed at contributing to the understanding to the impact of affective responses to the messages.
Regarding the impact of recipients' affective experiences on information processing, we base our predictions on the associative network model (e.g., Bower, 1981; Blaney, 1986; Parrott and Sabini, 1990; Parrott, 1991; Rafienia et al., 2008). The model predicts that human memory is coordinated as an associative network and the content that is associated in the network is often simultaneously activated. This theoretical approach also implies that information of the same valence is co-activated. Based on these notions, we predict that if recipients experience more negative and less positive emotions when listening to patients (vs. doctor) testimonials, this will likely result in a better memory for information of a negative valence.
Furthermore, research in the tradition of the counter-regulatory principle (Rothermund et al., 2011) indicates that information of the opposite valence is preferably processed in certain emotional states (e.g., under threat, individuals preferably process positive information). However, it is important to note that the counter-regulatory principle only applies if individuals experience “hot” (i.e., intense) emotional states, because only then is it functional to regulate these states by processing information of the opposite valence regarding the current emotional state. Counter-regulation effects have been shown with concerned (but not with unconcerned) participants (Greving and Sassenberg, 2015; Greving et al., 2015; Sassenberg and Greving, 2016).
In case of the present research, we believe that unconcerned recipients do not experience any intense emotional state when listening to a patient reporting her/his experiences of DBS as treatment, because those individuals are not personally affected by the reported content (i.e., they personally are not in need of DBS as treatment). Hence, resonating with the patient's experience should result in a mild affective experience congruent with the patient's experiences. In other words, recipients share the patient's affective state, but this affect is less intense in recipients than in actual patients (Rothermund et al., 2011; cf. Sassenberg et al., 2015). This results in the following predictions.
Hypothesis 2: Recipients should recall more information congruent with the affective tone of a message but not more information of incongruent valence.
Hypothesis 3: Reports from patients (but less so from doctors) should elicit more recall of negative and less recall of positive information when containing negative (compared to positive) content, due to the emotions they elicit. In other words, we hypothesize a conditional indirect effect of content valence on memory via experienced emotions moderated by the testimonial protagonist type.
We investigated how using testimonials affects recipients' emotions and, subsequently, their memory regarding the transmitted information. This is important because it is likely that the recalled medical information will guide later medical decisions. Thus, it is plausible that testimonials affected recipients' screening behavior 6 months later (cf. Lipkus et al., 2003), because including testimonials in health information very likely affects recipients' emotions and should thus have an impact on their memory for the specific screening procedure.
The Current Studies: Deep Brain Stimulation as Topic of Medical Communication
Two studies tested the three above derived hypotheses regarding information about Deep Brain Stimulation (DBS). DBS is an invasive treatment during which brain electrodes are implanted using stereotactic guidance, the electrodes being connected to subcutaneously implanted impulse generators (Voges et al., 2009). Hence, electrodes are implemented in patients' brain while they are awake (however anesthetized). After the intervention, the patient can activate the electrodes whenever needed; thereby regulating the activation of brain areas. Neurological symptoms related to essential tremor, Parkinson's disease, obsessive compulsive disorder, and epilepsy can be treated with DBS. DBS is a modern but highly contended invasive treatment. Whilst its effectiveness is documented for movement-related disorders such as Parkinson's disease or essential tremor, its effectiveness is at best controversial for other diseases such as Major Depression (Gilbert and Ovadia, 2011; cf. Südmeyer et al., 2012). This is important to note, because it renders DBS an ideal research topic to investigate our hypotheses. Obviously, DBS has the potential to elicit strong emotional reactions. Moreover, the current mixed evidence for its effectiveness allows for varying the tone between positive and negative valence. In our view, this makes it highly suitable to investigate the impact of patient vs. doctors as testimonials on recipients' emotional experiences and information processing, because it is plausible to emphasize either the advantages or the disadvantages of the treatment.
We also deliberately chose DBS as topic of medical communication because we were interested in information processing and knowledge transfer with regard to a topic relatively unknown (and likely of little relevance) to recipients. Accordingly, what we present as information regarding DBS is unlikely to interfere with participants' already formed health attitudes and health behavior to date. Moreover, if our research yielded results indicating that using testimonials for this topic of presumably little personal relevance still leads to emotional reactions and memory biases in recipients, this would demonstrate the significance and impact of testimonials in medical communication.
We tested our hypotheses in a prestudy (Hypothesis 1) and a main experiment (Hypotheses 1–3) following a procedure similar to that of Sassenrath et al. (2017). Recipients listened to an audio recording of DBS-related content. We used auditory recordings because they are a common format in the radio and on the web, (e.g., in podcasts and multimedia sections of online newspapers). The valence of the content (positive vs. negative) and the testimonial protagonist (patient vs. doctor) were varied between experimental conditions. It is to be noted that we deliberately use the term protagonist here instead of, for example, message source, because we did not vary the information about the communicator who created the whole message (e.g., scientists vs. pharmaceutical company). We rather want that the protagonist presented within the message as source of reported experiences is varied.
A computer-based questionnaire measured recipients' emotions regarding the DBS-related information (in the prestudy and main experiment) and their recall of information from a text about DBS read after they had heard the audio file which served to manipulate the valence of content and the protagonist (main experiment).
Ethics Statement
Both the Prestudy and the Main Experiment were approved by the Ethics Commission of the Knowledge Media Research Center (Ethics Committee, IWM, Schleichstraße 6, 72076 Tübingen, Germany) and all participants in both studies have given written informed consent prior to participating in the studies.
Prestudy
Method
Participants and Design
Forty-three under-graduate students (31 female, Mage = 23.63, SDage = 4.48, range: 18–42) participated in an experiment with a 2 (patient vs. doctor) × 2 (positive contents vs. negative contents) design and were randomly allocated an experimental condition (see Table 1 for detail). Participants were university students who were recruited from a large university campus of a Southern German university. They received a chocolate bar for compensation.
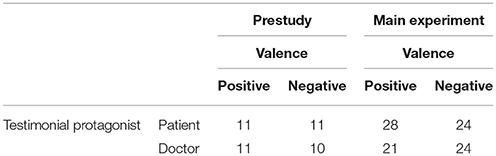
Table 1. Number of participants (N) per cell for each condition in both the Prestudy (N = 43) and the Main Experiment (N = 97).
Procedure and Measures
The study took place in the university library. The materials and the procedure are similar to those used by Sassenrath et al. (2017). After providing consent, participants heard an audio recording (length 337 to 377 words) of information on DBS. To implement the experimental manipulations, the content was presented either from a doctor's perspective or from a patient's perspective. The information waseither predominantly positive or predominantly negative. The audio recordings for all four conditions used identical acoustical conditions and the same speaker who was blind to research goals and hypotheses.
After participants had listened to the audiofile, emotions regarding DBS were assessed. These emotions were measured with 12 items (e.g., Sassenberg and Hansen, 2007). Six items each assessed positive emotions (relaxed, excited, eased, enthusiastic, optimistic, relieved; α = 0.89) and negative emotions (scared, disappointed, afraid, sad, depressed, disturbed; α = 0.90). Participants rated these items on a 9-point Likert scale ranging from 1 (not at all) to 9 (very much) in response to the question “When I am thinking about DBS, I am …”. Finally, participants were thanked, debriefed, and compensated1.
Results and Discussion
We hypothesized (Hypothesis 1) that reports containing mainly negative information (but not reports containing positive information) presented with a patient as protagonist would elicit stronger negative and weaker positive emotions than the same information presented with doctors as protagonists. To test this prediction, we conducted a mixed analysis of variance (ANOVA) with valence of emotions (positive emotions vs. negative emotions) as within-subjects factor and testimonial protagonist (patient vs. doctor) and valence of contents (positive contents vs. negative contents) as between-subjects factors. Analysis revealed a main effect for valence of emotions, F(1, 39) = 8.36, p = 0.006, ηp2 = 0.177, a valence of emotions × perspective interaction, F(1, 39) = 5.48, p = 0.024, = 0.123, and a valence of emotions × valence of contents interaction, F(1, 39) = 31.19, p < 0.001, = 0.444. However, these effects were qualified by the expected three-way interaction of valence of emotions, protagonist, and valence of contents, F(1, 39) = 4.53, p = 0.040, = 0.104 (for descriptives see Table 2). The results support Hypothesis 1, as reports presenting mainly negative information from a patient's perspective elicited stronger negative DBS-related emotions in participants (M = 4.98, SD = 1.95) than reports presenting mainly negative information from a doctor's perspective (M = 3.12, SD = 0.86), F (1, 39) = 7.82, p = 0.008, = 0.167. Additionally, reports presenting mainly negative information from a patient's perspective also elicited marginally less positive emotions (M = 2.70, SD = 1.40) than reports presenting mainly negative information from a doctor's perspective (M = 3.68, SD = 1.05), F (1, 39) = 2.88, p = 0.098, = 0.069. Testimonial protagonist had no effect on participants' DBS-related emotions when reports presented mainly positive information regarding DBS (all Fs < 1.03). No other effects reached statistical significance.
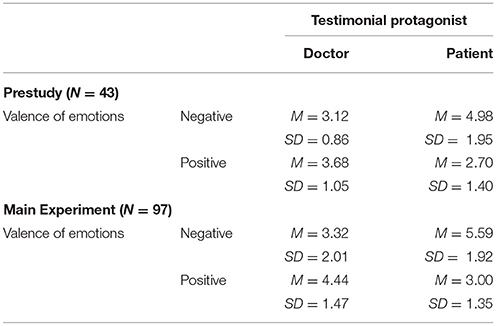
Table 2. Summary of main results regarding experienced valence of emotions when presenting information of negative content in the Prestudy (N = 43) and the Main Experiment (N = 97).
Results of this prestudy indicate that reports presenting mainly negative information on DBS from a patient's perspective more strongly influence participants' emotions (both positive and negative) than reports presenting either positive or negative information from a doctor's perspective. Hypothesis 1 was supported by the results of this prestudy. However, the small sample size calls for a replication of the effect. This is what we aimed for in the main experiment using the same research design as in the prestudy and using exactly the same materials. To be able to test Hypotheses 2 and 3, we included a free recall task which aimed at assessing participants' memory performance with regard to DBS-related information. Thereby, we sought to demonstrate that emotions elicited emotions in recipients that in turn affect their memory performance, when reports contain patients as testimonials but not when they contain doctors as testimonials.
Main Experiment
Method
Participants and Design
Ninety-seven participants (68 female, Mage = 23.24, SDage = 3.91, range: 18–35) participated in an experiment with a 2 (patient vs. doctor) × 2 (positive contents vs. negative contents) design. They were randomly assigned to the experimental conditions (see Table 1 for details). This study was the first in a 1-h lab session. Participants were university students who were recruited by a recruitment email announcing the study sent out via the university student email pool. Participants were compensated with €8 (approximately $9).
Procedure and Materials
The experiment was conducted in a laboratory with private and soundproof cubicles. First, participants listened to the same recording as in the preliminary study, involving the same manipulation of protagonist and valence. The audio files used in this experiment were identical to the ones used in the pre-study. In this study, every effort was made to ensure that the conditions under which participants listened to the information were identical. Specifically, all texts were recorded using the same microphone under the same recording conditions and the speaker of the texts was the same in all conditions. This speaker was a person from another lab and, thus, completely uninvolved in this study. The headphones that participants used were all from the same type and participants were able to adjust the volume to their preferred volume level.
After participants had listened to the text, emotions regarding DBS were assessed as in the prestudy. Next and following the procedure of Sassenrath et al. (2017), some exploratory measures were taken: Interest in DBS (2 items), attitude regarding DBS (3 items), evaluation of the audio materials for plausibility and comprehensibility (5 items), ability to focus on the text, motivation to read the text and how much fun it was to read the text. We included these items to increase the temporal distance between the manipulations and the text which participants had read and were to recall later. Answering the questions (in combination with the questions regarding DBS-related emotions) did not take longer than 3–4 min.
Thereafter, all participants read on a screen the same information about DBS as treatment of Parkinson patients (450 words) which provided in a first paragraph information about the operating principles of DBS. The four following paragraphs contained alternatingly positive and negative information about DBS (e.g., positive: patients' increased psychological well-being as an outcome of the treatment; negative: low success-rate - only 50% - and the negative experience of the surgery). After participants had read the text, they performed another filler task which took about 5 min and was implemented to prevent recency-effects for the following free recall task. Specifically, participants saw a drawing made of lines (Andrewes, 2001) and had to count all triangles that were formed by the lines in the drawing. This task was followed by a free recall of the text participants had read. They were requested to write down all information about DBS they could remember. This free recall task was not announced beforehand to avoid that participants focused on memorizing the text and, thus, behaved strategically. Finally, they were thanked, debriefed, and compensated.
Measures
Emotions toward DBS
Positive and negative emotions regarding DBS were measured exactly as in the pre-study (positive emotions: α = 0.87; negative emotions: α = 0.92).
Recall of information
Participants' responses in the free recall task were coded by two independent raters. The text contained 77 meaningful pieces of information about DBS that were categorized into a neutral (15 pieces), positive (31 pieces), or negative category (31 pieces). Any statement that literally or contentwise resembled one of the 77 pieces of information was coded as correctly recalled. These correct recalls were counted separately for positive, neutral, and negative pieces of information. These scores were highly correlated between raters—range: r (97) = 0.81 to r (97) = 0.99 - which indicates a very high interrater reliability (Landis and Koch, 1977). In the main analysis reported below mean scores across the two raters for the number of positive and negative pieces of information served as dependent variables. Participants recalled on average M = 2.42 (SD = 1.74, range: 0–7.5) pieces of positive information and M = 6.33 (SD = 3.47, range: 0–16) pieces of negative information.
Results
We hypothesized that reports presenting mainly negative information on DBS and using patients as protagonists would elicit less positive and more negative emotions in recipients than reports using doctors as protagonists. No such differences were expected for reports presenting mainly positive information (Hypothesis 1). Furthermore, we hypothesized that more information in line with recipient emotions would be recalled (Hypothesis 2). Overall, more negative information and less positive information on DBS should be recalled when the report presented negative information and used a patient's perspective compared to the other conditions due to the emotions elicited (Hypothesis 3).
Emotions Toward DBS
To test Hypothesis 1 we conducted a mixed ANOVA with valence of emotions (positive emotions vs. negative) as within-subjects factor and protagonist (patient vs. doctor) and valence of contents (positive contents vs. negative) as between-subjects factors. There was a significant main effect of valence of emotions, F(1, 93) = 18.91, p < 0.001, = 0.169, a valence of emotions × protagonist interaction, F (1, 93) = 19.88, p < 0.001, = 0.176, and a valence of emotions × valence of contents interaction, F(1, 93) = 53.58, p < 0.001, = 0.366, which were qualified by the predicted three-way interaction between valence of emotions, protagonist, and valence of contents, F(1, 93) = 9.15, p = 0.003, = 0.090 (see Table 2). As expected, reports presenting mainly negative information from a patient's perspective elicited stronger negative emotions (M = 5.59, SD = 1.92) than reports presenting mainly negative information from a doctor's perspective (M = 3.32, SD = 2.01), F (1, 93) = 21.52, p < 0.001, = 0.188. Accordingly, reports presenting mainly negative information from a patient's perspective also elicited less positive emotions (M = 3.00, SD = 1.35) than reports presenting mainly negative information from a doctor's perspective (M = 4.44, SD = 1.47), F (1, 93) = 14.02, p < 0.001, = 0.131. As in the prestudy, the testimonial protagonist had no effect on participants' DBS-related emotions when reports presented mainly positive information (all Fs < 1). These effects support Hypothesis 1. No other main effects and interaction effects occurred, all F's < 1.6, all p's > 0.20.2
Indirect Effect Analyses of Testimonial Protagonist on Memory via Emotion
Hypotheses 2 and 3 addressed participants' memory performance regarding DBS-related information. Specifically, we hypothesized that reports with negative (but not with positive) content using patients as testimonials (compared to doctors) would elicit stronger negative and weaker positive emotions in recipients which in turn affects recipients' memory performance regarding DBS-related content. Specifically, we expected recipients to remember more negative and less positive DBS-related information due to the elicited negative emotions.
Hence, we tested for a conditional indirect effect of valence of contents and testimonial via the two potential mediators of negative and positive emotions on the recall of negative pieces of information separately from the recall of positive pieces of information. To further test for the conditional indirect effects, we used the SPSS macro PROCESS (Preacher and Hayes, 2008).3 The conditional indirect effect analyses with Valence (positive vs. negative) as the independent variable, Negative Emotion as mediating variable, Testimonial Protagonist (patient vs. doctor) as moderating variable, and recall of negative DBS-related pieces of information as the dependent variable provided evidence for a significant indirect effect via negative emotions [b = 0.17, SE = 0.10, 95% CI [0.008; 0.400]]. Specifically, listening to an audiofile with patient protagonists and negative (vs. positive) content led to more negative emotions and in turn to the recall of more negative information [see Figure 1, lower row (2)]. Importantly, this relation did not occur for participants who had listened to doctors' negative reports on DBS [b = 0.05, SE = 0.05, 95% CI [−0.003; 0.185]; see Figure 2 lower row (2)].
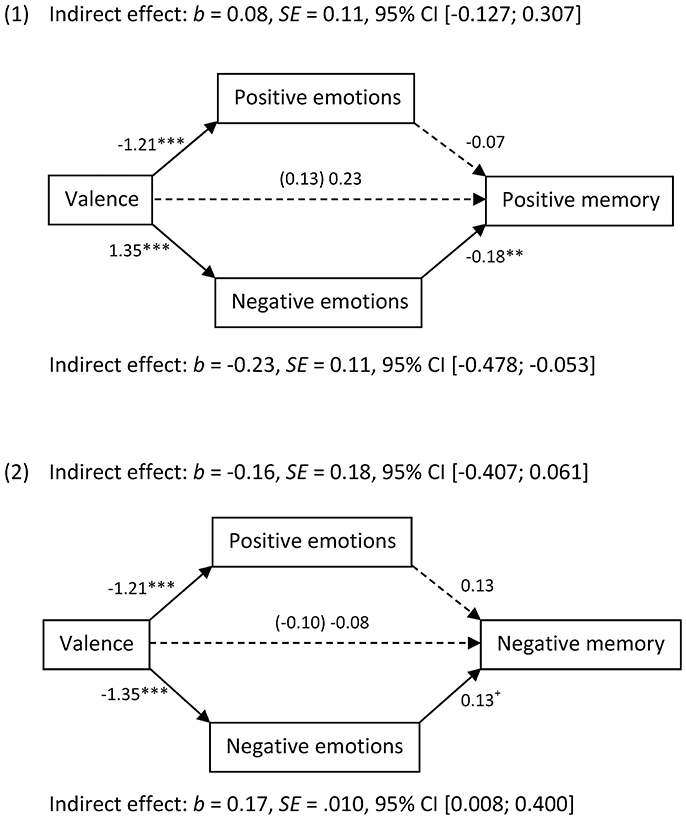
Figure 1. Unstandardized coefficients of bootstrapping analyses of the effect of using patient testimonials on memory performance regarding positive (1) or negative (2) DBS-related information via elicited positive or negative emotions.
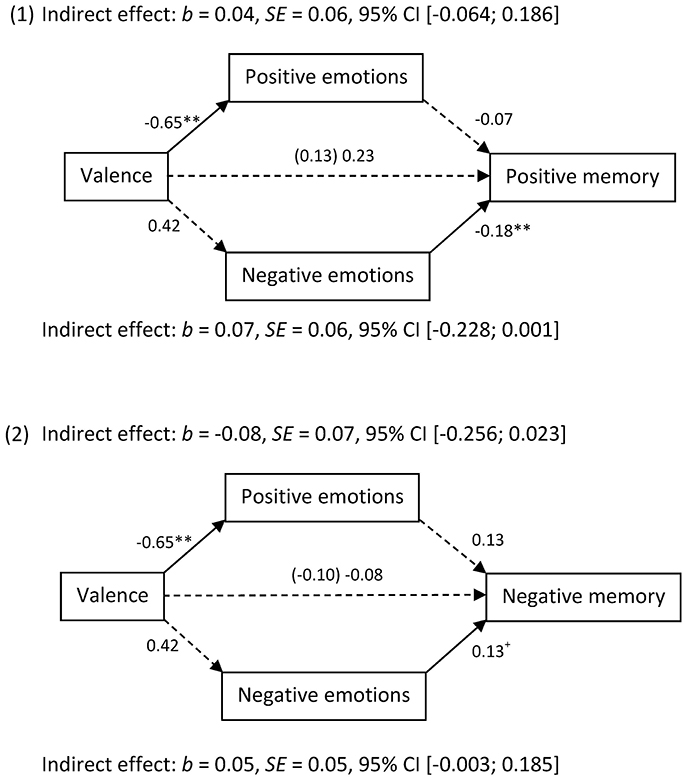
Figure 2. Unstandardized coefficients of bootstrapping analyses of the effect of using doctors testimonials on memory performance regarding positive (1) or negative (2) DBS-related information via elicited positive or negative emotions.
Another set of conditional indirect effect analyses with Valence (positive vs. negative) as the independent variable, Negative Emotion as a mediating variable, Testimonial Protagonist (patient vs. doctor) as a moderating variable, and recall of positive DBS-related pieces of information as the dependent variable revealed a significant indirect effect for negative emotions (the confidence interval excluded zero). That is, participants recalled less positive information regarding DBS because they experienced stronger negative emotions when they listened to patients' reports with negative information on DBS [b = −0.23, SE = 0.11, 95% CI [−0.478; −0.053] see Figure 1, upper row (1)]. Importantly, this relation did not occur for participants who listened to doctors' reports containing negative information on DBS. [b = −0.07, SE = 0.06, 95% CI [−0.228; 0.001]; see Figure 2 upper part (1)].4 Accordingly, we do not find any effect when using recipients' reported positive feelings regarding DBS as mediating variable. Recipients' positive emotions regarding DBS did not have any effect on their memory.
In sum, these results support Hypothesis 3 regarding the negative emotions—patients' testimonials reporting negative DBS-related information elicited the recall of more negative and less positive information due to stronger negative but not due to lower positive information. This is because negative emotions but not positive emotions predicted the recall of positive and negative information (see Figures 1, 2). In other words, Hypothesis 2 was only supported for negative but not for positive emotions.5
General Discussion
The current studies aimed to test the impact of patient or doctor testimonials in reports about medical innovations on unconcerned recipients' emotions (Hypothesis 1) and in turn on memory (Hypotheses 2 and 3). Two studies tested the impact of these testimonials in a report on medical treatment with DBS. The findings showed that when laypeople listen to DBS-related information using patients as protagonists, they experience more negative and less positive emotions toward DBS than when they listen to the same information using doctors as protagonists. Negative emotions toward DBS led recipients to remember less positive and more negative DBS-related information. Accordingly, the stylistic means of using testimonials when disseminating medical information (e.g., in healthcare intervention programmes or in media coverage, cf. Winterbottom et al., 2008) causes biased information transfer.
Put differently, the present results suggest that using a patient's first-person perspective to report on a medical topic leads recipients to relate to the patients and, thereby, empathize with the patients' reported affective experiences. Importantly, information processing is also influenced by this process in that emotionally congruent content is primarily remembered by recipients. Therefore, the present findings should be related to research on the influence of protagonists in health communication. A study by Lipkus et al. (2003) found for instance that the more a report about a disease makes recipients believe that it is severe, the more likely are these recipients to complete a screening test in the 6 months after having read the report. Based on our results, one might assume that the effect reported by Lipkus et al. was driven by negative emotions toward the disease and memory for negative information about the disease. In other words, our studies contributed to the understanding of the mechanisms underlying this and other similar studies. Considering that knowledge regarding a certain subject often predicts future behavior with regard to the respective topic subject (e.g., Ouellette and Wood, 1998; Strack and Deutsch, 2004), it is likely that information recalled from health communication influences health behavior and medical decisions. When this information is biased supposedly informed decisions are rather misinformed decisions.
Additionally, our findings indicate that patient testimonials conveying negatively valenced information affect recipients' emotions and memory. This finding is noteworthy considering that previous findings often used positive and encouraging testimonials in order to motivate concerned individuals to engage in disease prevention procedures or health behavior (e.g., Dillard et al., 2010; Dillard and Main, 2013).
The present results indicate that using patient testimonials has the potential to cause biased information transfer of medical information to unconcerned recipients (cf. Winterbottom et al., 2008). This is noteworthy, because scientific advancements such as invasive medical treatments are often transferred to a broader public by media coverage (cf., McCauley et al., 2013) in which techniques for making the reported content more vivid and appealing (i.e., emotion-eliciting) are popular (cf. Gilbert and Ovadia, 2011). To be more precise, journalists may feel incited to report medical advancements in a vivid and tangible way (e.g., by including personalized testimonials) instead of reporting about these topics based on technical details and in a matter-of-fact way (Kimmerle et al., 2015; cf. Abrams et al., 2015). They might aim to reach a large audience. Articles and reports eliciting emotions might be functional with regard to this aim. However, our findings suggest that this vivid and tangible way of disseminating medical information leads to misperceptions in recipients (i.e., they mainly process and remember negative aspects of the treatment). An unbalanced knowledge formation resulting from unbalanced processing of medical information may lead to biased public opinion (e.g., Sapp et al., 2013). If public opinion is distorted so that that mainly negative aspects of DBS as medical treatment are salient in the community, this may lead politicians to decide not to promote research on and development of DBS, mainly because they fear not being (re)elected by potential voters who do not regard DBS as worthwhile investment. This would be a tragic consequence given that DBS has the potential to aid a wider range of patients if these opportunities are tested in further research.
In addition to these rather practical implications, the present findings contribute to research on expert—lay person communication. Specifically, one might assume that experts (in our case doctors) exert a stronger impact on recipients as they have more expertise than lay people (in our case patients) which likely renders them more trustworthy. However, when reviewing the existing literature on the perceived trust in experts as information sources it becomes clear that the relation between expert status and trust in the expert is not as straightforward as one might think (see, e.g., Hendriks et al., 2016; Thomm and Bromme, 2016; Jucks and Thon, 2017; Thon and Jucks, 2017). Although experts certainly receive more trust due to their expertise, several contextual factors influence this relation. For instance, although information by experts is, on average, perceived as more credible, this does not necessarily imply that recipients endorse the expert's opinion to a stronger degree (cf., Thomm and Bromme, 2016). Furthermore, different levels of expertise do not inevitable translate in different levels of trust by recipients (Thomm and Bromme, 2016). Moreover, the informational content of what the expert reveals also affects perceived trustworthiness (e.g., Hendriks et al., 2016).
We did not focus on how recipients perceived source credibility of experts (doctors) vs. patients here. Instead, we were interested in how unconcerned recipients react with regard to their affective experiences to the same information presented either by an expert (doctor) or a concerned lay person (patient). Furthermore, we wanted to know whether these affective experiences influenced what recipients remembered with regard to the topic addressed (in our case DBS). Although recipients may give more credibility to what an expert has to say, it seems that they may more easily relate to what a concerned lay person has to say regarding a medical topic. This is in line with what we would expect considering that experts are likely to be perceived as powerful by lay persons (French et al., 1959; cf. Bromme et al., 2004), simply because they have more factual knowledge in the respective area. According to construal level theory (e.g., Trope and Liberman, 2010) this power difference causes distance which in turn prevents perspective taking and sharing testimonials' emotions. Our results are in line with this theory.
Unexpectedly, the effects on memory, or more precisely the prediction of memory by emotions, did not occur for positive and negative valence as predicted by the associative network model (e.g., Bower, 1981; Blaney, 1986; Parrott, 1991; Rafienia et al., 2008). In contrast, it was only found for negative emotions in Study 2. The lack of an effect of positive emotions on memory might be due to the topic. Information about DBS always also includes information about severe diseases. Specifically, DBS is an invasive and only palliative treatment for severe diseases such as Morbus Parkinson, Major Depression, or Essential Tremor. This context might be too strongly charged with negative associations in healthy lay individuals to elicit intense positive emotions with the potential to influence memory performance. Put differently, the elicited positive emotions might simply not have been positive and activating enough to affect memory processes. However, at this point this explanation is highly speculative and should thus be tested in future research.
Limitations of the Resent Research
The present findings certainly have limitations and only represent an illustration of which effects features frequently applied in journalistic articles about medical information and in health communication can have. In particular, it might have been helpful to focus on a better male-to-female ratio in both our samples, as there might be gender differences with regard to how individuals emotionally resonate with the testimonial's report on DBS-related information. Specifically, we believe that patients as protagonists of testimonials foster perspective taking and the literature has indicated that women are more emotionally sensitive than men (e.g., Hall, 1978; Eisenberg and Lennon, 1983).
Furthermore, we used young student samples in both of our studies which might be detrimental considering that these individuals are not only unconcerned as we intended. They are also generally less preoccupied with health topics. The level of being preoccupied or personally concerned with medical subjects presents an important moderator of our observed effects: As argued above, effects of emotions should differ depending on whether personal threat is elicited (likely the case for concerned recipients) or whether milder emotions result from perspective taking (likely the case for unconcerned recipients). In the case of threat, counter-regulation (Rothermund et al., 2011) should be elicited and more experienced threat will lead to more recall of positive information (Greving et al., 2015). In the case of emotions resulting from perspective taking (as in our studies), the opposite effect is more likely according to the associative network model. In other words, the effects of emotions on memory should vary depending on participants' concern by the topic or perhaps even by their preoccupation with health issues in general.
However and most crucially, with our studies we aimed to show how unconcerned individuals process medical information. Specifically, we examined information processing and knowledge transfer with regard to a topic relatively unknown (and likely of little relevance) for recipients. The information we presented was therefore unlikely to interfere with participants' already formed health attitudes and health behavior hereto. This is important, because we believe it is a strength of our study. Using testimonials for this topic of presumably little personal relevance still leads to emotional reactions and memory biases in recipients. Therefore, we demonstrated the significance and impact of testimonials in medical communication. In addition, in both of our studies reports on DBS were presented via audio file. Research suggests that auditory material elicits stronger emotions in recipients, since it allows for more vividness compared to written material (cf. Gitter et al., 1972; Wogalter and Young, 1991). Hence, it is an open question whether the effects reported here apply only to the multimedia materials that are more frequently used in online newspapers or whether they would also occur if only written materials were received.
Furthermore, it is also open for future research to systematically investigate whether the present findings are limited to the messages we used. More precisely, we did not use multiple messages per condition as our main focus was not to test the effect of different messages. Instead, we systematically varied features that affect vividness and tangibility of testimonials often used in reports on medical information and in medical education. We systematically investigated how these features affect information processing regarding the reported contents.
Conclusion
Taken together, the present research suggests that a widespread stylistic device used to communicate scientific and medical advancements to the broader public in a tangible and appealing manner is indeed successful– but may have unintended side effects. Including patient testimonials led to recipients empathizing with the patient testimonial's perspective as they reported affective experiences congruent with the patient's report. In our view, this suggests that recipients took on the patient's perspective which is likely to make the transferred information more accessible and less abstract to them. This also suggested that the recipient processes the incoming information in a certain way, namely from the position of the person concerned. Importantly, this biased information processing implies biased information transfer of scientific developments to the public (who are comparable to the ones we included as participants in our studies). This, in turn, may affect politics regarding the promotion of certain scientific developments and thus would have an impact on the society as a whole.
Author Contributions
CS analyzed the data, wrote introduction, method, results and general discussion of the manuscript, HG collected the data and supported data analyses and KS provided conceptual input during all stages of the manuscript reparation—data collection and analyses, writing and revising of the complete manuscript.
Funding
Research reported in this article was funded by the German Federal Ministry of Education and Research (Grant number: 01GP1306B).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
1. ^In addition, we assessed the following emotions for exploratory puposes: Anxiety (scared, frightened, full of fear; α = 0.89), hope (hopeful, confident, of good cheer; α = 0.90), anger (hostile, angry, upset; α = 0.87), disgust (disgusting, disgusted; r = 0.87), and threatened (helpless, threatened, without control; α = 0.70).
2. ^For the additional emotions we assessed, we found the same pattern of results. That is, negative reports from the patient's perspective elicited more negative emotions and less positive emotions than negative reports from the doctor's perspective (anxiety: Mpatient = 5.54, SD = 2.07; Mdoctor = 3.18, SD = 2.41; anger: Mpatient = 4.25, SD = 1.93; Mdoctor = 1.90, SD = 1.21; disgust: Mpatient = 4.60, SD = 2.71; Mdoctor = 2.13, SD = 1.90; threatened: Mpatient = 4.89, SD = 2.01; Mdoctor = 3.36, SD = 2.15; hope: Mpatient = 3.33, SD = 1.74; Mdoctor = 5.39, SD = 1.77; all Fs (1, 93) > 8.5, all ps < 0.005, all s > 0.08). In positive valence condition, there was no difference between the patient's and the doctor's perspective regarding the positive and negative emotions (anxiety: Mpatient = 2.88, SD = 1.75; Mdoctor = 2.89, SD = 1.86; anger: Mpatient = 1.92, SD = 1.26; Mdoctor = 1.78, SD = 1.05; disgust: Mpatient = 1.70, SD = 1.67; Mdoctor = 1.98, SD = 1.54; threatened: Mpatient = 2.81, SD = 1.48; Mdoctor = 2.87, SD = 1.46; hope: Mpatient = 6.38, SD = 1.58; Mdoctor = 6.86, SD = 1.16; all Fs (1, 93) < 1.1, ns).
3. ^In our analyses of the recalled information, we controlled for those pieces of information that were in the audio texts AND in the balanced recall text. Thus, the subsequent analyses only used those pieces of information that participants recalled exclusively from the balanced recall text.
4. ^For the additional emotions, we found the same mediation results for “threatened” as for the negative emotions. Regarding the positive pieces of recalled information, the analysis revealed that there was an indirect effect only for the patient's perspective (b = −0.19, SE = 0.09, 95% CI [−0.410; −0.058]), but not for the doctor's perspective (b = −0.04, SE = 0.05, 95% CI [−0.188; 0.037]). The same was found for the recall of negative pieces of information. That is, there was an indirect effect for the patient's perspective (b = 0.12, SE = 0.08, 95% CI [0.002; 0.304]), but not for the doctor's perspective (b = 0.03, SE = 0.04, 95% CI [−0.022; 0.149]). This means that, due to the threat that negative contents from a patient's perspective elicited, participants recalled less positive pieces of information and more negative pieces of information.
5. ^We also ran our analyses with the total number of remembered pieces of information. Here, we only found a marginally significant effect of our valence factor on overall memory performance, F(1, 96) = 3.23, p = 0.076, = 0.034. Recipients remember marginally more information overall when having listened to a negatively valenced report (M = 12.47, SD = 5.03) compared to a positively valenced report (M = 10.76, SD = 3.94). No other main or interaction effect reached statistical significance (all ps > 0.294).
References
Abrams, K. M., Zimbres, T., and Carr, C. (2015). Communicating sensitive scientific issues: the interplay between values, attitudes, and euphemisms in communicating livestock slaughter. Sci. Commun. 37, 485–505. doi: 10.1177/1075547015588599
Agnew, C. R., Van Lange, P. A., Rusbult, C. E., and Langston, C. A. (1998). Cognitive interdependence: commitment and the mental representation of close relationships. J. Pers. Soc. Psychol. 74, 939–954. doi: 10.1037/0022-3514.74.4.939
Aron, A., and Aron, E. N. (1996). “Self and self-expansion in relationships,” in Knowledge Structures in Close Relationships: A Social Psychological Approach, eds. G. J. O. Fletcher and J. Fitness (New York, NY: Psychology Press), 325–344.
Aron, A. U., Aron, E. N., and Smollan, D. (1992). Inclusion of other in the self scale and the structure of interpersonal closeness. J. Pers. Soc. Psychol. 63, 596–612. doi: 10.1037/0022-3514.63.4.596
Blaney, P. H. (1986). Affect and memory: a review. Psychol. Bull. 99, 229–246. doi: 10.1037/0033-2909.99.2.229
Bol, N., van Weert, J. C., de Haes, H. C., Loos, E. F., de Heer, S., Sikkel, D., et al. (2014). Using cognitive and affective illustrations to enhance older adults' website satisfaction and recall of online cancer-related information. Health Commun. 29, 678–688. doi: 10.1080/10410236.2013.771560
Bromme, R., Jucks, R., and Rambow, R. (2004). “Experten-Laien-Kommunikation im Wissensmanagement,” in Der Mensch im Wissensmanagement: Psychologische Konzepte zum besseren Verständnis und Umgang mit Wissen, eds G. Reinmann and H. Mandl (Göttingen: Hogrefe), 176–188.
Dillard, A. J., Fagerlin, A., Dal Cin, S., Zikmund-Fisher, B. J., and Ubel, P. A. (2010). Narratives that address affective forecasting errors reduce perceived barriers to colorectal cancer screening. Soc. Sci. Med. 71, 45–52. doi: 10.1016/j.socscimed.2010.02.038
Dillard, A. J., and Main, J. L. (2013). Using a health message with a testimonial to motivate colon cancer screening associations with perceived identification and vividness. Health Educ. Behav. 40, 673–682. doi: 10.1177/1090198112473111
Eisenberg, N., and Lennon, R. (1983). Sex differences in empathy and related capacities. Psych. Bull. 94, 100–131. doi: 10.1037/0033-2909.94.1.100
Ericsson, K. A., and Smith, J. (1991). “Prospects and limits of the empirical study of expertise: an introduction,” in Toward a General Theory of Expertise: Prospects and Limits, eds K. A. Ericsson and J. Smith (Cambridge, UK: Cambridge University Press), 1–33.
French, J. R., Raven, B., and Cartwright, D. (1959). The bases of social power. Classics Organ. Theory 7, 311–320.
Gilbert, F., and Ovadia, D. (2011). Deep brain stimulation in the media: over-optimistic media portrayals call for a new strategy involving journalists and scientists in the ethical debate. Front. Integr. Neurosci. 5:16. doi: 10.3389/fnint.2011.00016
Gitter, A. G., Kozel, N. J., and Mostofsky, D. T. (1972). Perception of emotion: the role of race, sex, and presentation mode. J. Soc. Psychol. 88, 213–222. doi: 10.1080/00224545.1972.9918677
Greving, H., and Sassenberg, K. (2015). Counter-regulation online: threat biases retrieval of information during internet search. Comput. Hum. Behav. 50, 291–298. doi: 10.1016/j.chb.2015.03.077
Greving, H., Sassenberg, K., and Fetterman, A. (2015). Counter-regulating on the internet: threat elicits preferential processing of positive information. J. Exp. Psycho. Appl. 21, 287–299. doi: 10.1037/xap0000053
Hall, J. A. (1978). Gender effects in decoding nonverbal cues. Psych. Bull. 85, 845–857. doi: 10.1037/0033-2909.85.4.845
Hendriks, F., Kienhues, D., and Bromme, R. (2016). Evoking vigilance: would you (dis) trust a scientist who discusses ethical implications of research in a science blog?. Public Underst. Sci. 25, 992–1008. doi: 10.1177/0963662516646048
Jucks, R., and Thon, F. M. (2017). Better to have many opinions than one from an expert? Social validation by one trustworthy source versus the masses in online health forums. Comput. Human Behav. 70, 375–381. doi: 10.1016/j.chb.2017.01.019
Kessels, R. P. (2003). Patients' memory for medical information. J. Roy. Soc. Med. 96, 219–222. doi: 10.1177/014107680309600504
Kimmerle, J., Flemming, D., Feinkohl, I., and Cress, U. (2015). How laypeople understand the tentativeness of medical research news in the media: an experimental study on the perception of information about deep brain stimulation. Sci. Commun. 37, 173–189. doi: 10.1177/1075547014556541
Landis, J. R., and Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics 33, 159–174. doi: 10.2307/2529310
Lipkus, I. M., Green, L. G., and Marcus, A. (2003). Manipulating perceptions of colorectal cancer threat: implications for screening intentions and behaviors. J. Health Commun. 8, 213–228. doi: 10.1080/10810730305684
Liviatan, I., Trope, Y., and Lieberman, N. (2008). Interpersonal similarity as a social distance dimension: implications for perception of others' actions. J. Exp. Soc. Psychol. 44, 1256–1269. doi: 10.1016/j.jesp.2008.04.007
McCauley, M., Minsky, S., and Viswanath, K. (2013). The H1N1 pandemic: media frames, stigmatization and coping. BMC Public Health. 13:1116. doi: 10.1186/1471-2458-13-1116
Ouellette, J. A., and Wood, W. (1998). Habit and intention in everyday life: the multiple processes by which past behavior predicts future behavior. Psychol. Bull. 124, 54–74.
Parrott, W. G. (1991). Mood induction and instructions to sustain moods: a test of the subject compliance hypothesis of mood congruent memory. Cogn. Emot. 5, 41–52. doi: 10.1080/02699939108411022
Parrott, W. G., and Sabini, J. (1990). Mood and memory under natural conditions: evidence for mood incongruent recall. J. Pers. Soc. Psychol. 59, 321–336. doi: 10.1037/0022-3514.59.2.321
Preacher, K. J., and Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 40, 879–891. doi: 10.3758/BRM.40.3.879
Rafienia, P., Azadfallah, P., Fathi-Ashtiani, A., and Rasoulzadeh-Tabatabaiei, K. (2008). The role of extraversion, neuroticism and positive and negative mood in emotional information processing. Pers. Individ. Dif. 44, 392–402. doi: 10.1016/j.paid.2007.08.018
Rothermund, K., Gast, A., and Wentura, D. (2011). Incongruency effects in affective processing: automatic motivational counter-regulation or mismatch-induced salience? Cogn. Emot. 25, 413–425. doi: 10.1080/02699931.2010.537075
Rothman, A. J., Kelly, K. M., Weinstein, N. D., and O'Leary, A. (1999). Increasing the salience of risky sexual behavior: promoting interest in HIV antibody testing among heterosexually active young adults. J. Appl. Soc. Psychol. 29, 531–551. doi: 10.1111/j.1559-1816.1999.tb01400.x
Sapp, S. G., Korsching, P. F., Arnot, C., and Wilson, J. J. (2013). Science communication and the rationality of public opinion formation. Sci Commun. 35, 734–757. doi: 10.1177/1075547013480491
Sassenberg, K., and Greving, H. (2016). Internet searching about disease elicits a positive perception of own health when severity of illness is high: a longitudinal questionnaire study. J. Med. Internet Res. 18:e56. doi: 10.2196/jmir.5140
Sassenberg, K., and Hansen, N. (2007). The impact of regulatory focus on affective responses to social discrimination. Eur. J. Soc. Psychol. 37, 421–444. doi: 10.1002/ejsp.358
Sassenberg, K., Sassenrath, C., and Fetterman, A. (2015). Threat ≠ prevention, challenge ≠ promotion: the impact of threat, challenge, and regulatory focus on attention to negative stimuli. Cogn. Emot. 29, 188–195. doi: 10.1080/02699931.2014.898612
Sassenrath, C., Greving, H., and Sassenberg, K. (2017). It has to be first-hand: the effect of first-person testimonials in medical communication on recipients' emotions and memory. Cogent Med. 4:1354492. doi: 10.1080/2331205X.2017.1354492
Smith, P. K., and Trope, Y. (2006). You focus on the forest when you're in charge of the trees: power priming and abstract information processing. J. Pers. Soc. Psychol. 90, 578–596. doi: 10.1037/0022-3514.90.4.578
Südmeyer, M., Volkmann, J., Wojtecki, L., Deuschl, G., Schnitzler, A., and Möller, B. (2012). Tiefe hirnstimulation–erwartungen und bedenken [Deep brain stimulation–expectations and doubts. A nationwide questionnaire study of patients with Parkinson's disease and their family members]. Nervenarzt 83, 481–486. doi: 10.1007/s00115-011-3400-x
Strack, F., and Deutsch, R. (2004). Reflective and impulsive determinants of social behavior. Personal. Soc. Psychol. Rev. 8, 220–247. doi: 10.1207/s15327957pspr0803_1
Thomm, E., and Bromme, R. (2016). How source information shapes lay interpretations of science conflicts: interplay between sourcing, conflict explanation, source evaluation, and claim evaluation. Read. Writ. 29, 1629–1652. doi: 10.1007/s11145-016-9638-8
Thon, F. M., and Jucks, R. (2017). Believing in expertise: how authors' credentials and language use influence the credibility of online health information. Health Commun. 32, 828–836. doi: 10.1080/10410236.2016.1172296
Trope, Y., and Liberman, N. (2010). Construal-level theory of psychological distance. Psychol. Rev. 117, 440–463. doi: 10.1037/a0018963
van Weert, J. C., van Noort, G., Bol, N., van Dijk, L., Tates, K., and Jansen, J. (2011). Tailored information for cancer patients on the Internet: effects of visual cues and language complexity on information recall and satisfaction. Pat. Ed. Coun. 84, 368–378. doi: 10.1016/j.pec.2011.04.006
Voges, J., Kiening, K., Krauss, J. K., Nikkhah, G., and Vesper, J. (2009). Neurochirurgische Standards bei tiefer Hirnstimulation [Neurosurgical standards in deep brain stimulation]. Nervenarzt 80, 666–672. doi: 10.1007/s00115-009-2698-0
Winterbottom, A., Bekker, H.l, Conner, M., and Mooney, A. (2008). Does narrative information bias individual's decision making? a systematic review. Soc. Sci. Med. 67, 2079–2088. doi: 10.1016/j.socscimed.2008.09.037
Keywords: medical communication, deep brain stimulation, testimonials, emotions, memory
Citation: Sassenrath C, Greving H and Sassenberg K (2018) Are you Concerned? Patient Testimonials in Medical Communication Affect Healthy Recipients' Emotions and Memory. Front. Commun. 3:18. doi: 10.3389/fcomm.2018.00018
Received: 14 November 2017; Accepted: 19 April 2018;
Published: 10 August 2018.
Edited by:
Rukhsana Ahmed, University of Ottawa, CanadaReviewed by:
Patrick J. Dillon, Kent State University at Stark, United StatesMahati Chitem, Indian Institute of Technology Hyderabad, India
Copyright © 2018 Sassenrath, Greving and Sassenberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudia Sassenrath, claudia.sassenrath@uni-ulm.de