Case Report
Intermittent Left Bundle Branch Block: What is the Mechanism?

Hussam Ali1* and Riccardo Cappato2
1Arrhythmia & Electrophysiology Unit II, Humanitas Gavazzeni Clinics, Bergamo, Italy
2Arrhythmia & Electrophysiology Research Center, Humanitas Clinical & Research Center, Rozzano (Milan), Italy
*Address for Correspondence: Hussam Ali, MD, FESC, FEHRA, Arrhythmia and Electrophysiology Unit II, Humanitas Gavazzeni Clinics, Via M. Gavazzeni 21-24125 Bergamo (BG), Italy, Tel: +39 0354204005; Fax: +39 0282246453; E-mail: hussamali.ep@gmail.com
Dates: Submitted: 26 December 2016; Approved: 18 January 2017; Published: 20 January 2017
How to cite this article: Ali H, Cappato R. Intermittent Left Bundle Branch Block: What is the Mechanism? J Cardiol Cardiovasc Med. 2017; 2: 001-002.
DOI: 10.29328/journal.jccm.1001004
Copyright License: © 2017 Ali H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Left Bundle branch block; Functional block; Linking Phenomenon
CASE PRESENTATION
A 73-year-old male underwent cardiologic evaluation for an incidental electrocardiographic finding of left bundle branch block (LBBB). He was asymptomatic and had no relevant cardiac history. Physical examination and transthoracic echocardiogram revealed no abnormalities.
12-lead Holter ECG showed constant sinus rhythm, preserved AV conduction (PR at the upper normal limit) and no brady/tachyarrhythmias. Complete LBBB was observed during prolonged phases of the recording, but occasionally it was intermittent (Figure 1). What is the most likely mechanism of the intermittent LBBB showed in this figure?
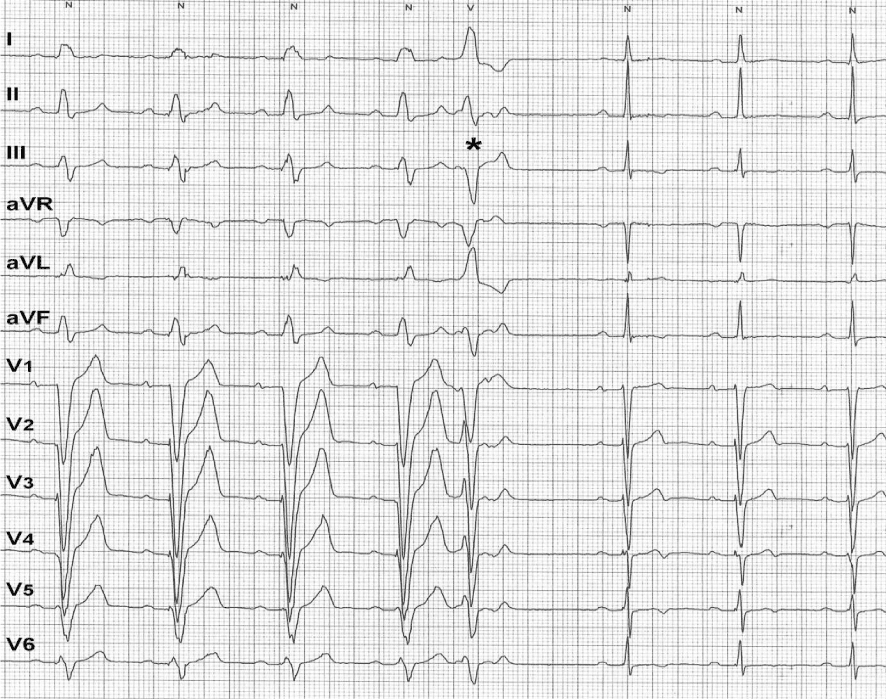
Figure 1:12-lead ECG showing intermittent LBBB. Aberrant conduction disappeared following a premature ventricular complex (the asterisk). Please see text for discussion.
DISCUSSION
The first half of the figure showed 12-lead ECG with sinus rhythm at 65 bpm conducted with complete LBBB (QRS duration ≈ 160 ms) and PR interval at the upper normal limit (200 ms). The absence of a typical LBBB pattern in V5,6 was probably due to the electrodes positioning (Holter recording). The second half of the figure showed sinus rhythm conducted without LBBB at nearly the same heart rate. Interestingly, the disappearance of LBBB was triggered by a premature ventricular complex (PVC/the asterisk) probably originating from the right ventricle. The interruption of aberrant conduction by a single PVC is highly indicative of a «linking» phenomenon as the underlying mechanism with repetitive concealed retrograde penetration of the left bundle by impulses propagating anterogradely through the right bundle. Linking phenomenon has been used to indicate the mechanism for perpetuation of functional anterograde bundle branch block by repetitive transseptal retrograde concealed penetration by impulses propagating along the contralateral bundle [1].
There are probably two factors that may play a role in LBBB disappearance after a single PVC. First, the post-extrasystolic pause that may allow more time for the blocked bundle to recover from its refractoriness with QRS normalization for the only first subsequent beat. Secondly, the elimination of the retrograde penetration of the LBB by transeptal concealed conduction through the contralateral bundle «linking effect». This concealed retrograde penetration of the left bundle prolonged and delayed the onset of its refractoriness relatively to that of the right bundle. The PVC caused a kind of «reset» and interruption of this phenomenon and, hence, the subsequent impulses propagated simultaneously through the both bundles and their refractory periods started synchronously. On the other hand, the appearance of bundle branch block after a single PVC might have given further confirmation of this functional phenomenon.
Occasionally, ablation of the right bundle may unmask some degree of antegrade conduction capabilities over the left bundle in patients with a preexistent complete LBBB due to eliminating this linking effect [2]. Functional LBBB may occur at faster heart rates (3 phase block, e.g. during supraventricular tachycardia) or even during bradycardia (4 phase block). In this case, heart rate was nearly the same (65 bpm) with and without LBBB making the hypothesis of rate-dependent block unlikely [3]. In this case, an electrophysiology study was not performed, but it is still the gold standard to exclude conduction disease (e.g. HV interval prolongation or infra-hisian block).
However, LBBB may indicate a serious cardiac pathology as ischemic coronary disease or dilated cardiomyopathy that should be excluded. Furthermore, it may provide the substrate for bundle branch reentrant ventricular tachycardia or infra-hisian block leading to syncope. LBBB may also alter left ventricular function with a negative impact on ventricular remodeling and performance [3].
Finally, patients with LBBB should undergo careful evaluation since this conduction disturbance may be associated with serious cardiac pathologies and may have an adverse impact on ventricular function. Nevertheless, careful analysis of electrocardiographic features with emphasis on the onset/offset of LBBB may reflect its functional and benign nature as in the presented case.
REFERENCES
- Lehmann MH, Denker S, Mahmud R, Addas A, Akhtar M. Linking: a dynamic electrophysiologic phenomenon in macroreentry circuits. Circulation. 1985; 71: 254-265. Ref.: https://goo.gl/lAZ74H
- Ali H, Lupo P, Foresti S, De Ambroggi G, Epicoco G, et al. Is it complete left bundle branch block? Just ablate the right bundle. Ann Noninvasive Electrocardiol. 2016. Ref.: https://goo.gl/vLQq6h
- Bazoukis G, Tsimos K, Korantzopoulos P. Episodic left bundle branch block-A comprehensive review of the literature. Ann Noninvasive Electrocardiol. 2016; 2: 117-125. Ref.: https://goo.gl/KVtwbc