INTRODUCTION
Lower extremity musculoskeletal injuries (MSK-Is) occur frequently in collegiate athletics, particularly within sports that require constant acceleration, deceleration, and quick directional changes across the court or field of play.1 Epidemiological reports have shown these injuries to be especially common in female athletes, with many occurring from non-contact mechanisms.2–6 Specifically, injuries to the lower extremity account for 69.3 and 72.7% of all practice-related injuries in field hockey4 and lacrosse,5 respectively; they represent 45.3 and 61.1% of all game-related injuries within these sports. Regarding sex-comparable sports (e.g., soccer, basketball, and lacrosse), females have a higher frequency of severe injuries, or those restricting participation for > 21 days, to the knee and lower leg, ankle, or foot,7 as well injuries specific to the anterior cruciate ligament (ACL).8 These injury rates have led researchers to develop clinical assessment tools to identify potentially modifiable risk factors for injury, so that targeted injury prevention strategies can be implemented in effort to reduce injury risk.
The Landing Error Scoring System (LESS) is a reliable9,10 and valid10 standardized scoring rubric used to identify aberrant trunk and lower extremity movement patterns during performance of a jump-landing task. Although originally developed to identify individuals at elevated risk for non-contact ACL injuries,10,11 more recent work has investigated the association between LESS and risk of all injuries.12,13 To date, conflicting findings have been reported regarding the relationship between LESS scores and risk of injury,12,13 including those to the ACL.11,14 However, only Smith et al.14 included collegiate athletes as participants though the injury definition was specific to non-contact ACL injury only. Findings revealed that the LESS total score was not associated with an increased risk of non-contact ACL injury. Notably, the LESS evaluates numerous specific lower extremity and trunk biomechanical movement patterns (individual LESS items) in addition to providing a composite score. The identification of individual LESS item errors that are related to injury may be useful in overall injury prevention efforts as specific faulty movement patterns can be targeted with appropriate intervention programs. Yet, only one study to date has compared the frequency of errors on individual LESS items by injury status.11 Further, it is important to consider that LESS performance may be associated with any lower extremity injury and not just specific to the ACL. The one published study evaluating LESS scores and the incidence of any lower extremity injury in an athletic population found no differences in LESS total scores between the injured and uninjured groups.15 However, the study was limited by a small sample size and no analysis of an association between total LESS scores and injury was presented. Overall, there are limited data on LESS performance and injury incidence in collegiate athletes.14,15 One potential limitation of the LESS is that it requires trained evaluators to score video-recorded jump-landing trials following the completion of testing.10Therefore, this time-intensive process may limit its application for examining large groups of athletes, which is typical in collegiate athletic settings. The use of marker-less motion capture technology has been presented as an alternative time-expedient and objective method for scoring the LESS as scores are generated automatically following each trial. Notably, prior studies have shown this technology to have similar reliability to expert raters using the LESS to score jump-landing task performance.16,17
To date, no study has evaluated the association between LESS performance (total score and individual items) and incidence of any lower extremity injury in female collegiate athletes across multiple sports. Therefore, the purpose of this study was to examine the association between LESS performance as measured with a markerless motion-capture system and lower extremity injury in female collegiate athletes. It was hypothesized that higher total LESS scores would be associated with an increased odds of lower extremity injury in female collegiate athletes.
METHODS
Study Design
This study utilized a prospective cohort design. Between August 2017 and January 2018, female collegiate student-athletes from one NCAA Division I university completed a standardized jump-landing test prior to the start of their respective sport’s competitive season. Participants were subsequently followed throughout their competitive seasons (fall, winter, or spring sports) for incidence of lower extremity injuries.
Participants
In total, 116 student-athletes completed LESS testing prior to the start of their competitive seasons. Of those, data from five participants were excluded due to participants departure from their teams before the completion of the competitive season and one for data collection error (failure of system to record all three trial reps). This resulted in a final sample of 110 participants (age = 19.6 ± 1.5 years, age range 18 – 24 years; height = 168.2 ± 8.8 cm; mass = 67.6 ± 10.2 kg) from the following sports: basketball (n = 12), field hockey (n = 17), gymnastics (n = 14), lacrosse (n = 27), softball (n = 23), and volleyball (n = 17). The inclusion criterion was medical clearance to perform the jump-landing assessment. Participants were excluded if they had any current injury and/or musculoskeletal pain that limited their ability to complete the assessment as determined by the university sports medicine staff.18 All participants were educated on the study design and procedures and provided written informed consent before testing. This study was approved by the institutional review board at Towson University.
Procedures
All testing was conducted within the university’s performance laboratory prior to the start of each sport’s competitive season. Participants were shod and wore self-selected athletic attire (e.g., shorts or spandex, t-shirts) during performance of the jump-landing assessment. Following confirmation of study inclusion criteria, participant characteristics, including age, height, and weight were recorded. The jump-landing test was performed using a standardized protocol adapted from previous studies.10,17 The participants began the assessment standing on a 30-cm-high box and jumped to a designated mark located 90 cm in front of the box. Participants were instructed to (1) jump forward off the box and not vertical, and to ensure the that both limbs left the box simultaneously; (2) land on both feet just past the designated mark; and (3) perform a maximal vertical jump immediately upon landing. Prior to testing, participants were provided a visual demonstration and asked if they understood the directions; all subsequent questions were answered by a study investigator. Participants completed a minimum of one practice trial followed by three successful trials of the jump-landing test. Participants were permitted to rest as necessary between trials. A trial was excluded and repeated if the participant failed to complete the jump as instructed or did not complete the movement in a fluid motion, or if the motion capture system was unable to score the trial based on capturing error. Additional trials were needed for 16.4% (18 of 110) of participants based on these criteria. Roughly half (44.4%; 8 of 18) of these participants required additional trials due to improper jump performance; 55.6% (10 of 18) were due to machine error. The majority (88.9%; 16 of 18) of participants required one additional trial while two (11.1%) completed two extra jumps.
A Kinect v2 sensor was used to capture all kinematic variables. The depth camera (Kinect, version 2; Microsoft Corp, Redmond, WA, USA) was placed 3.4m in front of the box at a height of 0.84m from the floor on a commercially available tripod, and was controlled by a standard laptop computer. Athlete Movement Assessment software (PhysiMax Technologies Ltd, Herzliya, Israel) was used to examine the depth-camera data. As previously described, this marker-less motion capture system (‘PhysiMax system’) automatically captures and processes depth camera data using proprietary kinematic machine-learning algorithms. The system tracks and refines virtual markers on the participant’s body to measure joint angles during performance of various movement assessments.16,17 For the LESS, the system captures and uses kinematic data to assess each test item and automatically computes a total score. Findings from a recent validation study revealed overall moderate agreement between the ‘PhysiMax system’ and a traditional 3-dimensional motion capture system for lower extremity and trunk angles during performance of a jump landing task (Intraclass correlation coefficient (ICC) average = 0.58). Specifically, better agreement was reported for sagittal (ICC average = 0.84) than frontal plane (ICC average = 0.35) kinematics.19Further, the ‘PhysiMax system’ has been validated against expert LESS raters (average κ = 0.48 ± 0.40; prevalence and bias-adjusted average κ = 0.71 ± 0.27; percentage agreement = 0.85 ± 0.14) using the LESS to score performance on a standardized jump landing task.17
The LESS Score
The LESS is a standardized screening tool used to identify aberrant movement patterns during performance of a jump-landing test.10 The LESS has been shown to have good interrater and excellent intrarater reliability.20Further, the ability of the LESS to assess jump-landing movement patterns has been validated against traditional 3-dimensional motion capture systems.9,10 In its original form, the LESS scoring rubric is comprised of 17 items that evaluate lower extremity and trunk kinematics at initial contact with the ground and the time between initial ground contact and maximal knee flexion.10 More recently, examiners have expanded the scoring rubric to include five additional items, increasing the total possible items scored to 22.17,21 A higher LESS score equates to a greater number of landing errors or presence of aberrant moving patterns during performance of the jump landing test. In the present study, a modified scoring rubric adapted from the 22-item LESS scoring system was used to ensure that only items automatically scored by the ‘PhysiMax system’ were included. Ultimately, this led to the omission of two items from the total score calculation. First, the marker-less motion capture system did not provide scores for the item assessing knee “wobble” upon landing. Second, the system is unable to provide a score for the “overall impression” item as this is a subjective assessment of the movement in its entirety. However, the PhysiMax system does provide the examiner the option to manually input a score for this item at the conclusion of each trial. Given the subjective nature of this 2-point scoring item and the potential for evaluator bias, this item was omitted from the total score calculation. Therefore, the maximum total LESS score in the present study was 21.
Injury Data
Throughout each team’s competitive season, university sports medicine staff members recorded injury data for all participants into an electronic medical record database (Athletic Training Systems; Keffer Development Services, Grove City, PA, USA). Injury characteristics included body part (e.g., hip, knee, ankle), injury type (e.g., sprain, strain, stress fracture), activity at time of injury (practice, game, conditioning session, or insidious onset), mechanism (contact or non-contact), and days of time loss. An “injury” was defined as any injury to the lower extremity that occurred during or as result from participation in an organized practice, game, or conditioning session, required medical intervention by an athletic trainer, and resulted in complete restriction from one or more practices or games.15,22 Participants were included in the injury group following an initial injury incidence; multiple injuries to the same participant were not included. All injury data were abstracted from the electronic medical record database by one of the authors.
Statistical Analyses
The marker-less motion capture system automatically scored all 20 items for each leg. An error was included in the final data set when it was recorded for an individual LESS item on at least two of three trials for either leg. The total score was computed as the sum of errors (0 or 1) across all included items. Descriptive statistics were calculated for demographic and total LESS scores. A Receiver Operating Characteristic (ROC) curve was calculated to determine the optimal cutpoint for the total LESS score for predicting lower extremity injury. Based on the ROC curve analysis, a cut-score of 5.5 was used to dichotomize LESS performance as “good” or “poor” (≤ 5 vs. > 5). Pearson’s Chi squared statistics were used to examine the association between lower extremity injury and LESS total scores > 5. In addition, logistic regression was used to examine the odds of injury with LESS total score as a continuous variable. For both analyses, “injured/uninjured” was the dependent variable. Finally, the Fisher exact test was used to determine differences between the injured and uninjured groups for the frequency of receiving an error on each individual LESS test item. An alpha level of ≤ 0.05 was used to determine statistical significance. Data analyses were performed using Statistical Package for the Social Sciences version 25.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
Twenty-five participants suffered a lower-extremity injury during their competitive seasons. The ankle was the most commonly injured body segment (28.0%, n = 7), followed by the lower leg (20%, n = 5), thigh (20%, n = 5), foot (20%, n = 5), and knee (12.0%, n = 3). Sprains (n = 9) and muscle strains (n = 7) comprised 64.0% of all injuries. Non-contact and contact injuries represented 76.0% (n = 19) and 24.0% (n = 6) of all injuries, respectively. Almost half of the injuries occurred during practice (48.0%, n = 12), while the remaining were recorded as occurring during a game (16.0%, n = 4), conditioning session (12.0%, n = 3), or having an insidious onset (24%, n = 6). Seventeen injuries (68.0%) resulted in time loss ≤ 1 week while three (12.0%) led to time loss between eight days and one month; five (25.0%) resulted in time loss of ≥ 1 month.
The mean LESS score for all participants was 5.67 ± 1.85. Table 1 presents the descriptive statistics for total LESS scores by sport.
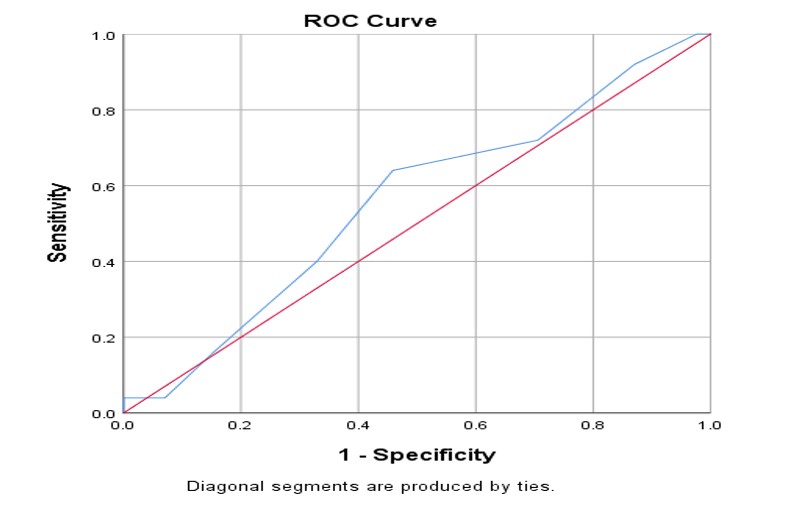
The ROC curve for the total LESS score was not significant (AUC = 0.56, SE = 0.07, p = 0.396, 95% CI = 0.43, 0.68) (Figure 1). The cut-point score was maximized at 5.5 (sensitivity = 64.0%, specificity = 54.1%), which is what determined the total LESS score of >5 to be used in this study for further analysis. Notably, this cut-point is consistent with prior studies that used either the traditional 17-item11,13 or expanded 22-item LESS scoring rubric12 to examine the relationship between LESS performance and injury.

The association between lower extremity injury and a total LESS score > 5 is presented in Table 2. As shown, female collegiate athletes with total LESS scores > 5 were not more likely to be injured than those with scores ≤ 5 (χ2 = 2.53, p = 0.111). The relative risk of injury to this group was 1.78 (95% CI = 0.86, 3.68) while the odds ratio was 2.10 (95% CI = 0.83, 5.27). No significant association was found between total LESS score as a continuous variable and lower extremity injury (OR = 1.12; 95% CI = 0.88, 1.42; p = 0.376).
Table 3 presents the frequency of errors on individual test items between injured and uninured participants. As shown, the uninjured group was more likely to receive an error on lateral trunk flexion at initial contact than the injured group (FET, p = 0.023).
DISCUSSION
The purpose of this study was to examine the association between LESS performance and lower extremity injury incidence in a cohort of female collegiate athletes across multiple sports. A key finding was that the LESS total score was not associated with an increased odds of lower extremity injury. To date, conflicting findings regarding the association between total LESS scores and future injury risk have been reported,11–14 which may be attributed to the methodological heterogeneity across studies. Notably, the present study is the first to examine the association between LESS total scores and incidence of any lower extremity injury in female collegiate athletes with findings suggesting that LESS performance is not related to injury in this population. These results are aligned with recent systematic reviews that have questioned the ability of clinical movement assessments, including the LESS, to identify future MSK-I risk in some athletic and military populations.20,23
Since the LESS evaluates kinematics during the landing phase of a jump from a standardized height, adequate neuromuscular control is required for satisfactory performance, as determined by fewer identified errors. Markedly, ineffective neuromuscular control has been reported as a risk factor for non-contact ACL24,25 and other lower extremity injuries,26,27 and therefore has been a target of prior injury prevention efforts.28–30 To date, two prospective studies have examined the ability of the LESS (17-item scoring rubric) to identify athletes at increased risk for non-contact ACL injury.11,14 Padua et al.11 reported that elite-youth soccer players with a total LESS score of five or higher were at increased risk for non-contact ACL injuries than those scoring below this cutpoint. Further, the mean LESS score was higher in ACL-injured athletes than the non-injured group (6.24 ± 1.75 vs. 4.43 ± 1.71). In contrast, Smith et al.14 reported no significant associations between total LESS scores and risk of non-contact ACL injury in cohorts of high school and collegiate athletes. Given the methodological differences between these two investigations and the present study, such as our use of a modified 20-item scoring rubric and broader injury definition, comparisons across studies are limited. The rationale for including an injury definition that included all lower extremity injuries irrespective of injury mechanism was two-fold and warrants acknowledgement. First, non-contact ACL injuries represent only a small portion of all injuries8 and thus including a more comprehensive injury definition allowed for the examination of the relationship between LESS scores and injury across the entire lower extremity. Second, the LESS, like most clinical screening tools, allows for the evaluation of specific lower extremity and trunk biomechanical movement patterns (individual LESS items), that may be related to numerous lower extremity pathologies.31 Nonetheless, it is worth noting that of the 25 injured participants in the present study, one sustained a non-contact ACL injury and was recorded of having a total LESS score of three. Regarding injury mechanism, it is also notable that of the 25 documented injuries, 19 (76.0%) were recorded as occurring from non-contact mechanisms. Consistent with the findings presented in Table 2, a secondary data analysis revealed no significant association between total LESS score ≥ 5 and odds of non-contact lower extremity injury (OR = 1.91; 95%CI = 0.69, 5.30).
The present study is the first to examine the association between LESS performance and incidence of any lower extremity injury in female collegiate athletes across multiple sports. In a previous study, no significant difference in total LESS scores (17-item rubric) was found between male and female collegiate soccer players who sustained a lower extremity injury and those who remained uninjured across one season of play.15 However, the authors did not present a measure of association between LESS scores and injury. Given this omission, the inclusion of both male and female collegiate athletes from one sport only, and the small sample size of their prospective analysis (n = 21), the present findings provide initial evidence on the relationship between LESS total scores and incidence of future lower extremity injury in female collegiate athletes. In a prior validation study using 3-dimensional motion analysis, authors reported an association between poor LESS total scores and several kinematic (decreased knee and hip flexion angles, increased knee valgus and hip adduction angles) and kinetic (increased hip extension and knee valgus moment) measures.10 Importantly, several of these measures have been shown to be related to ACL injury25 as well as other lower extremity injuries and conditions, including chronic ankle instability32 and iliotibial band syndrome.33 Nonetheless, the results from the present investigation, when using an injury definition that included all lower extremity injuries irrespective of mechanism in a population of female collegiate athletes across multiple sports, suggest that the total LESS score may not be associated with an increased odds of injury. As previously stated, it is reasonable to propose that the methodological heterogeneity across studies may be the reason for the conflicting findings supporting LESS’s predictive value for injury. In addition to the aforementioned variations in scoring rubrics and injury definitions, population characteristics, such as proportion of male and female participants, sport and level of play (i.e. youth, high school, and college), have differed across studies to date.11,14,15 Notably, high school athletes have been found to have higher LESS scores than college athletes,14 suggesting the influence of age on test performance. Likewise, a recent review that included a meta-analysis of twelve studies revealed that females had higher LESS scores than males, though the mean difference (0.6) was not clinically meaningful.34 In sum, these findings suggest that LESS scores, as well as their association with injury incidence, may be influenced by the sex, sport, and playing level of the athletic population. Therefore, additional efforts to examine the association between LESS performance and lower extremity injury in male and female athletes across various levels of play are warranted.
Although several studies have examined the association between total LESS scores and lower extremity injury in athletic populations, limited data exists on the relationship between performance on individual LESS items and injury. In a previous study, Padua et al.11 reported that trunk flexion displacement and overall joint displacement were the most predictive items for identifying non-contact ACL injury risk in youth soccer athletes. In the present investigation, only lateral trunk flexion at initial contact was related to future lower extremity injury as the uninjured group was unexpectedly more likely to demonstrate this fault than those who remained uninjured. Worth noting is that these results are based on a small number of total injuries (n = 25) and for several LESS items, few or no errors were identified. Despite this limitation, the finding that errors occurred infrequently for items such as hip flexion at initial contact, foot position: internal rotation, and hip flexion displacement, is similar to results presented by Padua et al.11 In another study, investigators examined sex differences in the most commonly occurring errors in male and female military cadets. Findings revealed that females were more likely to land with decreased hip and knee flexion as well as increased medial knee displacement at initial contact than their male counterparts yet no relationship to injury incidence was examined.35 Notably, similar results regarding the frequency of increased medial knee displacement were found in the present study as 30% (33 of 110) of all participants presented with this error. Further, injured participants were more likely to display this error than the uninjured group, though results were not statistically significant (p = 0.080). Since the LESS scoring rubric identifies errors for multiple trunk and lower extremity movements, it is possible that individual item scores may have clinical application for injury prevention purposes. Therefore, future efforts to examine the association between individual LESS item scores and injury across varying athletic populations are warranted.
Recent authors have examined the relationship between LESS total scores and incidence of all MSK-Is in military populations.12,13 In a study of 132 male entry-level military recruits undergoing 16-weeks of fitness training, authors reported that recruits with LESS scores (17-item rubric) > 5 had a relative risk of 2.2 (95% CI = 1.0 – 1.7) for any MSK-I compared to those with scores ≤ 5.13 In more recent work, de la Motte et al.12 reported that total LESS scores (22-item rubric) were predictive of any MSK-I in a large cohort of 1,714 male and female military trainees followed throughout their initial 180 days of service. However, results revealed that military trainees categorized as having good LESS performance, as determined by the median score of 5.7, were more likely to be injured than those with higher LESS scores (poor performance). The authors recommended using caution when interpreting the clinical application of these findings since LESS scoring reliability may be influenced by scoring error and rater expertise.12 Notably, the recent development of marker-less motion capture technology, as used in the present study, may be a suitable method for limiting the potential influence of rater error, particularly when large samples of athletic or military cohorts are examined.
A novel aspect of the present study is that LESS measures were automatically provided by the ‘PhysiMax’ system, whereas prior studies examining the association between LESS performance and injury utilized the traditional video recording and scoring method. In a prior study, Mauntel et al.17 reported the ‘PhysiMax system’ to have similar reliability to expert LESS raters (average κ = 0.48 ± 0.40; prevalence and bias-adjusted average κ = 0.71 ± 0.27; percentage agreement = 0.85 ± 0.14), with good to perfect agreement noted for the majority of test items (71.4%; 15 of 21). The authors noted the clinical relevance of these findings since use of expert raters to score the LESS is common in both research and clinical practice. Further, this system was used in a recent study examining stress fracture risk factors, including biomechanical movement patters measured by the LESS, and bone metabolism in a military population.36
Despite the present study’s finding that LESS performance was not related to future lower extremity injury in female collegiate athletes, this marker-less motion capture system was successful in providing an objective and immediate evaluation of jump landing performance in a large cohort of athletes. Therefore, the use of this technology may have clinical application beyond injury risk prediction, such as identifying the most frequently occurring faulty movement patterns across a group of athletes to assist with developing team-specific corrective exercise programs as well as to help monitor the rehabilitation progress of an individual athlete following lower extremity injury. Worth noting is that the results from LESS testing (total scores and errors on individual test items) were not utilized by members of the sports medicine team for the development of individual or team-specific injury prevention exercise programming during the follow-up period in the present study. Athletic trainers and strength and conditioning coaches for each sport had the ability to develop individual team programming at their discretion; however, these decisions were made independently by the sports medicine team and results were not monitored as an outcome of this study.
The average LESS score for participants playing softball (6.78 ± 1.95) was higher than those from other sports. Further, the sports with the lowest average LESS scores in order were gymnastics, field hockey, and volleyball, which all require a higher frequency of cutting and jumping movements. Notably, findings from a recent meta-analysis revealed that neuromuscular training programs of at least six weeks in duration that included plyometric exercises and feedback on jump landing technique resulted in meaningfully improved LESS scores.34 Although the LESS scores captured in the current investigation were not utilized in guiding injury prevention programming for participants during the follow-up period nor was the performance of other injury prevention efforts monitored, it is reasonable to suggest that the neuromuscular demands associated with these sports may have influenced the lower scores achieved by their participants. Future studies may want to consider examining between sport differences in LESS performance across a multitude of different team and individual sports of varying physical and neuromuscular demands.
This study has several limitations. First, the study sample included female athletes from five different sports, each comprised of different sample sizes. In addition, basketball, field hockey, and lacrosse are categorized as contact sports whereas volleyball and gymnastics are classified as non-contact sports. Second, results revealed a relatively small number of participants (n = 25) who sustained a lower extremity injury during the follow-up period (one competitive season). Consequently, it was deemed inappropriate to examine the association between LESS performance and injury to specific segments (e.g., ankle, knee) or structures (ACL), which has been the focus of some prior studies.11,14 However, it is important to note that the injury definition used in the present study was selected because the LESS allows for the evaluation of numerous lower extremity and trunk movement patterns, which may be related to various lower extremity pathologies. Third, the 22-item LESS scoring rubric was modified so that only items automatically scored by the ‘PhysiMax System’ were included in the total score calculation. Although this limited comparisons between total LESS scores from the present investigation and those from previous studies, this omission eliminated any potential for evaluator error or scoring bias. Fourth, roughly 10% of participants were required to complete additional trials based on the system’s inability to score jumps due to capturing error. Despite this requirement, it is notable that this error is immediately visible to the evaluator so that additional trials can be performed during the testing period. Further, this additional time requirement is minimal compared to the potential time spent manually reviewing and scoring jumps using the traditional LESS testing method. Finally, potential confounding variables, such as prior history of lower extremity injury, were not assessed.
CONCLUSION
The present findings suggest that LESS performance is not associated with future lower extremity injury in a cohort of female collegiate athletes across multiple sports. Notably, these results are aligned with some prior studies that also reported the total LESS score was unable to prospectively identify risk of injury in athletic or military populations.12,14 Therefore, practitioners may want to exhibit caution when using the LESS total score as a stand-alone injury prediction tool. However, future studies to examine the association between individual LESS item faults and injury are warranted. Despite these results, the use of a markerless motion capture system to automatically and objectively score a commonly used clinical assessment may have practical application for sports medicine and strength and conditioning professionals interested in evaluating movement patterns in individual or large groups of athletes. Specifically, use of this technology may be an effective time-expedient strategy for assessing movement patterns in an entire team or during pre-participation examinations. Since both total and individual test item scores are automatically provided, results are readily available to assist in the development of corrective exercise programs targeted at improving the most frequently identified movement impairments.
ACKNOWLEDGMENTS
The authors have no conflicts of interest to disclose. Support for this study came from the College of Health Professions and the School of Emerging Technologies at Towson University.