
Abstract
Escitalopram is a selective serotonin reuptake inhibitor (SSRI), and is the second antidepressant to be approved for use in treating major depressive disorder (MDD) in adolescent patients (aged 12–17 years) in the US.
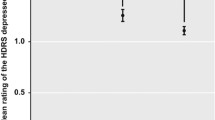
In a randomized, double-blind, flexible-dose, multicenter trial, once-daily escitalopram 10–20 mg (n=154) for 8 weeks was significantly better than placebo (n = 157) in improving the severity of depressive symptoms (as assessed by the change in the Children’s Depression Rating Scale-Revised [CDRS-R] total score) in adolescent patients with MDD. Preliminary data from a combined analysis of the double-blind data from this trial and double-blind data from a 16-week, fixed-dose, extension study suggest a significant difference between escitalopram and placebo recipients in the change in CDRS-R total scores after 24 weeks of treatment.
In a similarly designed flexible-dose trial in pediatric patients (aged 6–17 years), a significant difference between once-daily escitalopram 10–20 mg (n=77) and placebo (n = 80) for 8 weeks, as assessed by the change in CDRS-R total score, was not shown in the primary analysis (i.e. patients of all ages). In a pre-specified subgroup of adolescent patients, no significant difference was shown between the escitalopram and the placebo groups when analyzed using the last observation carried forward method, but was shown using the observed case method.
Escitalopram 10–20 mg/day showed better efficacy than placebo for some secondary endpoints (e.g. the change in the Clinical Global Impression [CGI]-Severity score, the CGI-Improvement response rate) but not others (e.g. CDRS-R response rate, rate of remission).
Once-daily escitalopram 10–20 mg for 8 weeks was generally well tolerated in clinical trials in adolescent or pediatric patients with MDD. The incidence of suicidality-related adverse events was generally similar between escitalopram and placebo recipients.


Similar content being viewed by others

References
Birmaher B, Brent D, Bernet W, et al. Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. AACAP Work Group on Quality Issues. J Am Acad Child Adolesc Psychiatry 2007 Nov; 46(11): 1503–26
Belmaker RH, Agam G. Major depressive disorder. N Engl J Med 2008 Jan 3; 358(1): 55–68
American Psychiatric Association. Mood disorders. In: Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association, 1994: 317–92
Adams SM, Miller KE, Zylstra RG. Pharmacologic management of adult depression. Am Fam Physician 2008 Mar 15; 77(6): 785–92
Bylund DB, Reed AL. Childhood and adolescent depression: why do children and adults respond differently to antidepressant drugs? Nuerochem Int 2007 Oct; 51(5): 246–53
Stone M, Laughren T, Jones ML, et al. Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration. BMJ 2009 Aug 11; 339: b2880
Cohen D, Deniau E, Maturana A, et a1. Are child and adolescent responses to placebo higher in major depression than in anxiety disorders? A systematic review of placebo-controlled trials. PLoS One 2008 Jul 9; 3(7): e2632
Hetrick S, Merry S, McKenzie J, et al. Selective serotonin reuptake inhibitors (SSRIs) for depressive disorders in children and adolescents. Cochrane Database Syst Rev 2007 Jul 18; (3): CD004851
Tsapakis EM, Soldani F, Tondo L, et al. Efficacy of antidepressants in juvenile depression: meta-analysis [published errata appear in Br J Psychiatry 2008 Aug; 193(2): 169, and 2008 Oct; 193(4): 346]. Br J Psychiatry 2008 Jul; 193(1): 10–7
Cheung AH, Zuckerbrot RA, Jensen PS, et al. Guidelines for adolescent depression in primary care (GLAD-PC): II. Treatment and ongoing management [published erratum appears in Pediatrics 2008 Jan; 121 (1): 227]. Pediatrics 2007 Nov; 120(5): e1313–26
National Institute for Health and Clinical Excellence. Depression in children and young people: identification and management in primary, community and secondary care (clinical guideline 28) [online]. Available from URL: http://www.nice.org.uk/nicemedia/pdf/CG028NICEguideline.pdf [Accessed 2010 Mar 10]
Forest Laboratories, Inc. Forest Laboratories, Inc. announces FDA approval of Lexapro(R) for the treatment of major depressive disorder in adolescents [online]. Available from URL: http://www.frx.com/news/PressRelease.aspx?ID=1268211 [Accessed 2010 Mar 10]
Forest Laboratories, Inc. Lexapro® (escitalopram oxalate) tablets and oral solution: US prescribing information [online]. Available from: http://www.frx.com/pi/lexapro_pi.pdf [Accessed 2010 Mar 10]
Murdoch D, Keam SJ. Escitalopram: a review of its use in the management of major depressive disorder. Drugs 2005; 65(16): 2379–404
Sánchez C, Bøgesø KP, Ebert B, et al. Escitalopram versus citalopram: the surprising role of the R-enantiomer. Psychopharmacology (Berl) 2004 Jul; 174(2): 163–76
Kasper S, Sacher J, Klein N, et al. Differences in the dynamics of serotonin reuptake transporter occupancy may explain superior clinical efficacy of escitalopram versus citalopram. Int Clin Psychopharmacol 2009 May; 24(3): 119–25
Duman RS, Monteggia LM. A neurotrophic model for stress-related mood disorders. Biol Psychiatry 2006 Jun 15; 59(12): 1116–27
Rao N. The clinical pharmacokinetics of escitalopram. Clin Pharmacokinet 2007; 46(4): 281–90
Owens MJ, Knight DL, Nemeroff CB. Second-generation SSRIs: human monoamine transporter binding profile of escitalopram and R-fluoxetine. Biol Psychiatry 2001 Sep 1; 50(5): 345–50
Chen F, Larsen MB, Sánchez C, et al. The S-enantiomer of R,S-citalopram, increases inhibitor binding to the human serotonin transporter by an allos-teric mechanism. Comparison with other serotonin transporter inhibitors. Eur Neuropsychopharmacol 2005 Mar; 15(2): 193–8
Mørk A, Kreilgaard M, Sánchez C. The R-enantiomer of citalopram counteracts escitalopram-induced increase in extracellular 5-HT in the frontal cortex of freely moving rats. Neuropharmacology 2003 Aug; 45(2): 167–73
von Moltke LL, Greenblatt DJ, Giancarlo GM, et al. Escitalopram (S-citalopram) and its metabolites in vitro: cytochromes mediating biotransformation, inhibitory effects, and comparison to R-citalopram. Drug Metab Dispos 2001 Aug; 29(8): 1102–9
Periclou A, Rao N, Sherman T, et al. Single-dose pharmacokinetic study of escitalopram in adolescents and adults. Pharmacotherapy 2003 Oct 10; 23(10): 1361–2
Wingen M, Bothmer J, Langer S, et al. Actual driving performance and psychomotor function in healthy subjects after acute and subchronic treatment with escitalopram, mirtazapine, and placebo: a crossover trial. J Clin Psychiatry 2005 Apr; 66(4): 436–43
Søgaard B, Mengel H, Rao N, et al. The pharmacokinetics of escitalopram after oral and intravenous administration of single and multiple doses to healthy subjects. J Clin Pharmacol 2005 Dec; 45(12): 1400–6
Gutierrez MM, Rosenberg J, Abramowitz W. An evaluation of the potential for pharmacokinetic interaction between escitalopram and the cytochrome P450 3A4 inhibitor ritonavir. Clin Ther 2003 Apr; 25(4): 1200–10
Malling D, Poulsen MN, Søgaard B. The effect of cimetidine or omeprazole on the pharmacokinetics of escitalopram in healthy subjects. Br J Clin Pharmacol 2005 Sep; 60(3): 287–90
Cattaneo A, Bocchio-Chiavetto L, Zanardini R, et al. Reduced peripheral brain-derived neurotrophic factor mRNA levels are normalized by anti-depressant treatment. Int J Neuropsychopharmacol 2010 Feb; 13(1): 103–8
Jin Y, Pollock BG, Frank E, et al. Effect of age, weight, and CYP2C19 genotype on escitalopram exposure. J Clin Pharmacol 2010 Jan; 50(1): 62–72
Nadeem HS, Attenburrow M-J, Cowen PJ. Comparison of the effects of citalopram and escitalopram on 5-HT-mediated neuroendocrine responses. Neuropsychopharmacology 2004 Sep; 29(9): 1699–703
Emslie GJ, Ventura D, Korotzer A, et al. Escitalopram in the treatment of adolescent depression: a randomized placebo-controlled multisite trial. J Am Acad Child Adolesc Psychiatry 2009 Jul; 48(7): 721–9
Wagner KD, Jonas J, Findling RL, et al. A double-blind, randomized, placebo-controlled trial of escitalopram in the treatment of pediatric depression. J Am Acad Child Adolesc Psychiatry 2006 Mar; 45(3): 280–8
Forest Laboratories, Inc. A double-blind, fixed-dose extension study of escitalopram in pediatric patients with major depressive disorder [study no. SCT-MD-32A] [online]. Available from URL: http://www.forestclinicaltrials.com/CTR/CTRController/CTRViewPdf?_file_id=scsr/SCSR_SCT-MD-23-23A_final.pdf [Accessed 2010 Mar 10]
Wagner KD, Robb AS, Findling RL, et al. A randomized, placebo-controlled trial of citalopram for the treatment of major depression in children and adolescents. Am J Psychiatry 2004 Jun; 161(6): 1079–83
von Knorring A-L, Olsson GI, Thomsen PH, et al. A randomized, double-blind, placebo-controlled study of citalopram in adolescents with major depressive disorder. J Clin Psychopharmacol 2006 Jun; 26(3): 311–5
Ventura D, Robb A, Bose A, et al. CDRS-R subscale analysis in a randomized placebo-controlled trial of escitalopram in depressed adolescents [abstract no. NR2-073]. 162nd Annual Meeting of the American Psychiatric Association; 2009 May 16–21; San Francisco (CA)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yang, L.P.H., Scott, L.J. Escitalopram. Pediatr-Drugs 12, 155–162 (2010). https://doi.org/10.2165/11204340-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11204340-000000000-00000