
Abstract
Objective: To compare gastrointestinal (GI) healthcare resource use (HCRU) and associated costs in patients taking a fixed combination of diclofenac and misoprostol versus other nonsteroidal anti-inflammatory drugs (NSAIDs).
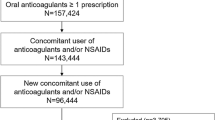
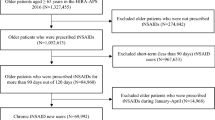
Methods: We analysed a sample (49 033 patients) of the Government of Quebec Health Insurance Agency database. Patients were included in the study if they did not have GI events during the year preceding the date of their first NSAID prescription dispensing (the index date). Patients were followed up for 2 years. A 3-stage model was used to determine the factors that influenced the direct medical costs of GI HCRU: (i) a logistic regression model (model 1) to estimate the risk of GI HCRU; (ii) a linear regression model (model 2) to estimate the direct costs of GI HCRU for those who had such events; (iii) multiplying the estimated risks from model 1 by the estimated costs from model 2 gave the estimated direct costs of GI HCRU for all patients.
Study Perspective: Provincial government of Quebec, Canada.
Results: 1533 patients were prescribed diclofenac/misoprostol at the index date and 10 540 another NSAID. Comorbidity markers were not significantly different between the 2 groups. Of the diclofenac/misoprostol patients, 23 (1.5%) were hospitalised for GI problems compared with 194 (1.8%) of the NSAID group; 403 (26.3%) of diclofenac/misoprostol patients used gastroprotective agents compared with 2849 (27.0%) of the NSAID patients; 118 (7.7%) of diclofenac/misoprostol patients had GI diagnostic tests compared with 682 (6.5%) of the NSAID patients. The average direct medical cost of GI HCRU was 310.52 Canadian dollars ($Can) /patient (1997 values) in the diclofenac/misoprostol group compared with $Can231.19/patient (1997 values) in the NSAID group. When adjusted for baseline factors, the ratio of the total directmedical cost of GI HCRU in the diclofenac/misoprostol group to that of the NSAID group was 1.15 (95% confidence interval: 0.89, 1.48).
Conclusions: Our data showed no significant differences in GI HCRU among patients taking diclofenac/misoprostol compared with those taking NSAIDs.





Similar content being viewed by others

References
Silverstein FE. Improving the gastrointestinal safety of NSAIDs: the development of misoprostol-from hypothesis to clinical practice. Dig Dis Sci 1998; 43 (3): 447–58
Roth SH. NSAID gastropathy. A new understanding. Arch Intern Med 1996; 156 (15): 1623–8
Singh G. Recent considerations in nonsteroidal anti-inflammatory drug gastropathy. Am J Med 1998; 105 (1B): 31S–8S
Bjorkman DJ. Nonsteroidal anti-inflammatory drug-induced gastrointestinal injury. Am J Med 1996; 101 (1A): 25S–32S
Singh G, Ramey DR, Morfeld D, et al. Gastrointestinal tract complications of nonsteroidal anti-inflammatory drug treatment in rheumatoid arthritis. Aprospective observational cohort study. Arch Intern Med 1996; 156 (14): 1530–6
Fries JF. ARAMIS and toxicity measurement. Arthritis Rheumatism and Aging Medical Information System. J Rheumatol 1995; 22 (5): 995–7
Cryer B, Kimmey MB. Gastrointestinal side effects of nonsteroidal anti-inflammatory drugs. Am J Med 1998; 105 (1B): 20S–30S
Wallace JL. Nonsteroidal anti-inflammatory drugs and gastroenteropathy: the second hundred years. Gastroenterology 1997; 112 (3): 1000–16
Solomon DH, Gurwitz JH. Toxicity of nonsteroidal anti-inflammatory drugs in the elderly: is advanced age a risk factor? Am J Med 1997; 102 (2): 208–15
Wolfe MM, Lichtenstein DR, Singh G. Gastrointestinal toxicity of Nonteroidal antiinflammatory drugs. N Engl J Med 1999; 340 (24): 1888–99
Tannenbaum H, Davis P, Russell AS, et al. An evidence-based approach to prescribing NSAIDs in musculoskeletal disease: a Canadian consensus. Canadian NSAID Consensus Participants. CMAJ 1996; 155 (1): 77–88
Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Arthritis Rheum 1995; 38 (11): 1535–46
American College of Rheumatology ad hoc committee of clinical guidelines. Guidelines for the management of rheumatoid arthritis. Arthritis Rheum 1996; 395: 713–22
Yeomans ND, Tulassay Z, Juhasz L, et al. A comparison of omeprazole with ranitidine for ulcers associated with nonsteroidal antiinflammatory drugs. Acid Suppression Trial: Ranitidine versus Omeprazole for NSAID-associated Ulcer Treatment (ASTRONAUT) Study Group. N Engl J Med 1998; 338 (11)
Walt RP. Misoprostol for the treatment of peptic ulcer and anti-inflammatory-drug-induced gastroduodenal ulceration. N Engl J Med 1992; 327 (22): 1575–80
Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduces serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995; 123 (4): 241–9
Hawkey CJ, Karrasch JA, Szczepanski L, et al. Omeprazole compared with misoprostol for ulcers associated with nonsteroidal antiinflammatory drugs. Omeprazole versus Misoprostol for NSAID-induced Ulcer Management (OMNIUM) Study Group. N Engl J Med 1998; 338 (11): 727–34
Taha AS, Hudson N, Hawkey CJ, et al. Famotidine for the prevention of gastric and duodenal ulcers caused by nonsteroidal antiinflammatory drugs. N Engl J Med 1996; 334 (22): 1435–9
Agrawal NM, Van Kerckhove HE, Erhardt LJ, et al. Misoprostol coadministered with diclofenac for prevention of gastroduodenal ulcers. A one-year study. Dig Dis Sci 1995; 40 (5): 1125–31
McKenna F. Efficacy and gastroduodenal safety of a fixed combination of diclofenac and misoprostol in the treatment of arthritis. Br J Rheumatol 1995; 34 Suppl. 1: 11–8
Bocanegra TS, Weaver AL, Tindall EA, et al. Diclofenac/misoprostol compared with diclofenac in the treatment of osteoarthritis of the knee or hip: a randomized, placebo controlled trial. Arthrotec Osteoarthritis Study Group. J Rheumatol 1998; 25 (8): 1602–11
Geis GS. Overall safety of Arthrotec. Scand J Rheumatol Suppl. 1992; 96: 33–6
Tamblyn R, Lavoie G, Petrella L, et al. The use of prescription claims databases in pharmacoepidemiological research: the accuracy and comprehensiveness of the prescription claims database in Quebec. J Clin Epidemiol 1995; 48 (8): 999–1009
Von Korff M, Wagner EH, Saunders K. A chronic disease score from automated pharmacy data. J Clin Epidemiol 1992; 45 (2): 197–203
Discharge Abstract Database Resource Indicators. Ottawa: Canadian Institute for Health Information (CIHI), 1997
Hospital Statistics: preliminary annual report; 83-241-XPB. Ottawa: Statistics Canada, 1996
Desgagne A, Castilloux AM, Angers JF, et al. The use of the bootstrap statistical method for the pharmacoeconomic cost analysis of skewed data. Pharmacoeconomics 1998; 13 (5): 487–97
Casella G, Berger, R. Statistical inference. Wadsworth & Brooks, 1990
Acknowledgements
The authors thank Dr Danielle Pilon for her helpful comments on the management of gastrointestinal disorders in Quebec, and the Régie de l’Assurance Maladie du Québec for the data.
This study was supported by Merck & Co., Inc.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Rahme, E., Joseph, L., Kong, S.X. et al. Gastrointestinal-Related Healthcare Resource Usage Associated with a Fixed Combination of Diclofenac and Misoprostol versus Other NSAIDs. Pharmacoeconomics 19, 577–588 (2001). https://doi.org/10.2165/00019053-200119050-00011
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-200119050-00011