
Summary
In coronary heart disease, β -blockers are beneficial because they limit the increase in heart rate and blood pressure during exercise, and calcium antagonists are useful because they reduce myocardial oxygen demand. Many different pharmacological combinations of a β -blocker and a calcium antagonist are possible, and β-blockade may ameliorate reflex tachycardia induced by peripheral vasodilatation due to calcium antagonists, therefore enhancing the benefit.
Studies have shown that combination therapy with propranolol and nifedipine, verapamil or diltiazem has greater antianginal efficacy based on symptomatic and objective assessment than either agent alone. A similar result has been reported for nifedipine or verapamil combined with atenolol. In combination, atenolol and nifedipine did not depress cardiac output or change the left ventricular ejection fraction (LVEF) at rest. During exercise, atenolol alone resulted in a reduced LVEF response in most patients but the combination did not adversely affect left ventricular function. Nifedipine alone did not significantly change LVEF. When verapamil was combined with atenolol, resting ejection fraction fell, indicating a deterioration in cardiac function.
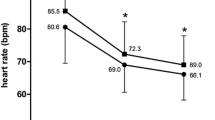
Nifedipine and propranolol combined do not change heart rate significantly. Verapamil and atenolol both reduce resting heart rate and their combination has a greater effect; a combination of propranolol and diltiazem also reduces heart rate to a similar extent. Caution is therefore warranted when prescribing the latter 2 combinations.
An increase in side effects can be expected with combination regimens compared with monotherapy; but with the nifedipine-atenolol combination the calcium antagonist can alleviate β-blocker-induced effects by its vasodilator effect, and β-blockers may ameliorate nifedipine-induced palpitations and flushing.
The effect on prognosis of the combination treatment remains an important question. Evidence suggests that β-blockers and calcium antagonists may favourably influence some of the factors important in the development and rupture of atheromatous plaques. However, any theoretical effect must be tested in a large-scale trial. The most complementary combination appears to be a β-blocker with a dihydropyridine, and, arguably, when tachycardia accompanies use of a vasodilator such agents are best used in the presence of β-blockade.
Similar content being viewed by others


References
Bala Subramanian V, Bowles MJ, Davies AB, Raftery EB. Combined therapy with verapamil and propranolol in chronic stable angina. American Journal of Cardiology 49: 125–132, 1982
Bing RJ, Weishar R, Rackl A, Pawlick G. Antianginal drugs and cardiac metabolism. In Bing (Ed.) New drug therapy with a calcium antagonist diltiazem, pp. 27–37, Excerpta Medica, Amsterdam, 1979
Braunwald E. Coronary artery spasm. Mechanisms and clinical relevance. Journal of the American Medical Association 246: 1957–1959, 1981
Dargie HJ. Combination therapy with beta adrenoceptor blockers and calcium antagonists. British Journal of Clinical Pharmacology 21 (Suppl.): 155–160, 1986
Dargie HJ, Lynch PG, Krikler DM, Harris L, Krikler S, et al. Nifedipine and propranolol: a beneficial drug interaction. American Journal of Medicine 71: 676–682, 1981a
Dargie HJ, Rowland E, Krikler DM. Role of antagonists in cardiovascular therapy. British Heart Journal 46: 8, 1981b
Davies MJ, Thomas M. Thrombosis and acute coronary artery lesions in sudden cardiac ischaemic death. New England Journal of Medicine 310: 1137, 1985
Engel HJ, Lichtlen PR. Beneficial enhancement of coronary blood flow by nifedipine. Comparison with nitroglycerine and beta blocking agents. American Journal of Medicine 71: 658, 1981
European Coronary Surgery Study Group. Longterm results of randomised study of coronary artery bypass surgery and stable angina pectoris. Lancet 2: 1173, 1982
Findlay IN, MacLeod K, Ford M, Gillen G, Elliott AT, et al. Treatment of angina pectoris, nifedipine and atenolol: efficacy and effect on cardiac function. British Heart Journal 55: 240–245, 1986
Findlay IN, MacLeod K, Gillen G, et al. A double blind placebo controlled comparison of verapamil, atenolol and their combination in patients with chronic stable angina pectoris. British Heart Journal 57: 336–343, 1987
Fleckenstein A. Specific pharmacology of calcium pacemakers and vascular smooth muscle. Annual Review of Pharmacology and Toxicology 17: 149, 1977
Greenberg H, McMaster P, Dwyer Jr EM and the multicentre post infarction research group. Left ventricular dysfunction after acute myocardial infarction: results of a prospective multicenter study. Journal of the American College of Cardiology 4: 867–874, 1984
Harris L, Dargie H, Lynch P, Bulpitt C, Krickler D. Blood pressure and heart rate in patients with ischaemic heart disease receiving nifedipine and propranolol. British Medical Journal 284: 1148, 1981
Henry PD. Comparative pharmacology of calcium antagonists: nifedipine, verapamil and diltiazem. American Journal of Medicine 46: 1047, 1980
Henry PD, Bentley KI. Suppression of atherogenesis in cholesterol-fed rabbit treated with nifedipine. Journal of Clinical Investigation 68: 1366–1369, 1981
Johnston DL, Lesoway R, Humen DP, Kostuk WJ. Clinical and hemodynamic evaluation of propranolol in combination with verapamil, nifedipine and diltiazem in exercise angina pectoris: a placebo controlled double blind randomised crossover study. American Journal of Cardiology 55: 680, 1985
Joshi PI, Dalai JJ, Ruttley MS, Steridan DJ, Henderson AH, et al. Nifedipine and left ventricular function in beta-blocked patients. British Heart Journal 45: 457–459, 1981
Julian DG. The practical implications of the coronary artery surgery trials. British Heart Journal 54: 343, 1985
Kurnik PB, Tiefenbrunn AJ, Ludbrook PA. The dependence of the cardiac effects of nifedipine on the responses of the peripheral vascular system. Circulation 69: 963–972, 1984
Leon MB, Rosing DR, Bonow RO, Epstein SE. Clinical efficacy of verapamil alone and combined with propranolol in treated patients with chronic stable angina pectoris. American Journal of Cardiology 48: 131, 1981
Luebs EB, Cohen A, Zaleski EJ, Bing RJ. Effect of nitroglycerine Intensain Isoptin and papaverine on coronary flow in man. American Journal of Cardiology 17: 534, 1966
Maseri A, L’Abbate A, Pesola A, et al. Coronary vasospasm in angina pectoris. Lancet 1: 713, 1977
Nayler WG. Calcium antagonists. European Heart Journal 1: 225–237, 1980
Passamani E, Davis KB, Gillespie MJ, Killip T. A randomised trial of coronary artery bypass surgery. Survival of patients with a low ejection fraction. New England Journal of Medicine 312: 1665, 1985
Simonsen S, Nitter-Hauge S. Effect of nifedipine on coronary hemodynamics in patients with coronary arteriosclerotic disease. Acta Medica Scandinavica 204: 179–184, 1978
Veterans Administration Coronary Artery Bypass Surgery Co-operative Study Group. Eleven years survival in the Veterans Administration randomised trial of coronary bypass surgery for stable angina. New England Journal of Medicine 311: 1333, 1984
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Dargie, H.J. β-Blockers and Calcium Antagonists in Angina Pectoris. Drugs 35 (Suppl 4), 44–50 (1988). https://doi.org/10.2165/00003495-198800354-00011
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-198800354-00011