
Abstract
Synopsis
Aldesleukin [recombinant interleukin-2 (IL-2)] is a biological response modifier which, like endogenous IL-2, has a range of immunomodulatory properties. Although aldesleukin is currently approved only for treatment of renal cell carcinoma, it has been widely used in patients with metastatic melanoma and has been assessed in numerous noncomparative trials in this indication. Durable complete responses have been reported in a small proportion of patients with good performance status who received immunotherapy or chemoimmunotherapy involving aldesleukin in several clinical trials. Overall median survival times of about 10 or 11 months are typical. Combination chemoimmunotherapy involving aldesleukin has produced relatively high response rates (up to 56%), but these are not predictive of increased survival time. Aldesleukin has not been directly compared with standard chemotherapy in randomised studies.
The use of continuous intravenous infusion and subcutaneous administration of aldesleukin, together with improved patient selection, has successfully reduced the severity of adverse events produced by the drug (the original intravenous bolus regimen is particularly toxic and often necessitates admission to an intensive care unit). However, the risk/benefit profile of aldesleukin in the treatment of melanoma requires further study, particularly after subcutaneous administration.
Thus, aldesleukin has shown modest efficacy in the treatment of metastatic melanoma. Although aldesleukin-containing regimens have produced promising results in many noncomparative trials, their clinical value in comparison with standard chemotherapy remains to be determined in phase HI studies. Until results from such trials are available, clinicians will need to carefully balance the potential benefits of the drug against the risks and likely quality-of-life implications associated with its toxicity in each patient. Current investigations centre on the use of aldesleukin as part of complex biochemotherapy regimens, and results from these trials are awaited with interest.
Pharmacodynamic Properties
Interleukin-2 (IL-2) is a cytokine which plays an important role in both cytotoxic and humoral immune responses. Aldesleukin (recombinant IL-2) has similar pharmacodynamic properties to endogenous IL-2 and, when administered to patients with cancer, stimulates the antitumour immune response. The results of this immunomodulatory activity are most evident as activation and/or proliferation of T lymphocytes, cytotoxic natural killer (NK) cells and lymphokine-activated killer (LAK) cells, and induction of cytokine production and eosinophilia.
The relationship between the immunomodulatory effects of aldesleukin and clinical outcome has yet to be fully characterised. Nevertheless, clinical response associated with T cell activation, increased LAK cell cytotoxicity or increased activation of NK cells has been documented in patients with melanoma. The precise mechanism of action of aldesleukin with respect to antitumour response in patients with metastatic melanoma remains unclear; some melanoma cell lines express the IL-2 receptor and thus may be subject to direct interactions with aldesleukin. Immunotherapy with aldesleukin and interferon-α (IFNα) may either induce or augment strong oligoclonal T cell selection, leading to tumour regression.
Pharmacokinetic Properties
Aldesleukin is rapidly distributed to intravascular and extracellular spaces, with a half-life of 6 to 20 minutes, after intravenous bolus administration in patients with cancer. A slower elimination phase is evident, with a half-life of about 60 to 85 minutes. Serum concentrations are linearly proportional to dose after intravenous aldesleukin administration. The pharmacokinetics of aldesleukin during continuous infusion are similar to those after bolus administration. Subcutaneous administration of aldesleukin produces serum concentrations which are about 2% of those seen with intravenous delivery; peak concentrations were obtained 2 to 6 hours after subcutaneous administration.
Distribution of aldesleukin to body tissues may vary depending on the route of administration and drug formulation. Aldesleukin is metabolised and eliminated via the kidneys, with little or none of the active molecule found in urine. The pharmacokinetic properties of aldesleukin may change during its administration, as a result of some of its pharmacodynamic properties.
Clinical Efficacy
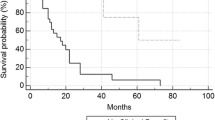
Monotherapy with high-dose bolus aldesleukin produced objective antitumour responses in 10 to 31% of patients with metastatic melanoma in clinical trials. The largest single study of aldesleukin monotherapy produced complete responses in 7% of 134 patients with melanoma, and these responses were maintained for >9 to >91 months. More than half of those with a complete response were still alive after 2 years. The estimated actuarial 3-year and 5-year survival rates for patients in this trial were 22 and 11%.
Combination immunotherapy with aldesleukin and IFNα produced objective responses in 18 to 41% of patients with melanoma (2 to 11% for complete response). The highest response rates were obtained in patients who received an initial high-dose infusion of aldesleukin which was then quickly tapered to maintenance levels; 41% of these patients had objective response (11% were complete responses) and median response duration was >11 months.
Aldesleukin has been combined with a number of single-agent chemotherapy regimens: objective and complete response rates were 4 to 25% and 0 to 5% in combination with cyclophosphamide, 16 to 26% and 2 to 11 % in combination with dacarbazine, and 17 or 37% and 6 or 11% in combination with cisplatin. Addition of IFNα to aldesleukin plus either dacarbazine or cisplatin produced objective and complete response rates of 26 to 54% and 4 to 13%. More complex chemoimmunotherapy regimens (most commonly involving aldesleukin, 2 or more chemotherapeutic drugs and, in some cases, IFNα) produced objective and complete response rates of 35 to 56% and 0 to 16%.
In general, complete responses for aldesleukin-containing regimens were more durable than those seen with dacarbazine, the standard treatment option in this indication, in previous studies (typically ≈9 months to 2 or 3 years vs ≈4 to 6 months), although there are no appropriate prospective comparisons.
Despite a >3-fold difference in objective response rates and a 12-fold difference for complete response rates across a range of clinical trials of aldesleukin, overall median survival times were relatively constant (10 or 11 months in most studies, range ≈9 to 13 months). However, this compares favourably with a typical survival duration of 6 to 9 months for patients with metastatic melanoma (many of whom would have received chemotherapy). A median survival time of 33 (range 13 to >36) months was reported for patients who experienced a complete response (16% of all patients) during treatment with aldesleukin, dacarbazine and cisplatin in one study.
Tolerability
Aldesleukin may be associated with a wide range of clinical adverse events, including cardiopulmonary, renal, hepatic, gastrointestinal, CNS, haematological, endocrine and constitutional effects. The precise profile and severity of events varies with total dose, dose frequency and duration and route of administration. In general, intravenous bolus administration is the most toxic route, while subcutaneous delivery produces the least severe adverse events.
The most common adverse events in clinical trials of aldesleukin (monotherapy or in combination with other treatments, administered by bolus, continuous infusion or subcutaneously) in patients with metastatic melanoma were hypotension, flu-like symptoms, nausea, vomiting, diarrhoea, nephrotoxicity and haematological abnormalities (most commonly thrombocytopenia and neutropenia); grade 4 toxicity was evident in up to a quarter of all patients or treatment courses. Transient and generally nonsevere dermatological reactions (other than injection site events) occur in many patients receiving aldesleukin.
Most recent trials used continuous infusion or subcutaneous delivery; data from patients with a range of malignancies (predominantly renal cell carcinoma) indicate that subcutaneous administration can significantly reduce the severity of aldesleukin toxicity with no apparent loss of antitumour efficacy/Continuous infusion generally produced moderate and manageable toxicity in patients with melanoma. Subcutaneous administration of aldesleukin was associated with mild to moderate adverse events and was generally considered to be ‘well tolerated’ (there was no severe hypotension or oedema caused by capillary leak syndrome). Flu-like symptoms and injection-site events (e.g. transient local inflammation and/or induration) were common with subcutaneous administration.
Dosage and Administration
Aldesleukin is currently approved only for treatment of renal cell carcinoma, but has been widely used in the treatment of melanoma. The original high-dose bolus regimen (based on 6 × 105 IU/kg as a 15-minute intravenous infusion every 8 hours) was initially approved in the US, whereas continuous intravenous infusion (treatment cycle based on 18 × 106 IU/m2 for 5 days) was approved in Europe. In practice, however, lower dose continuous infusion and subcutaneous regimens are most commonly used. Aldesleukin recipients should have a good general performance status (with the exception of their metastatic disease) and should have no significant cardiac, pulmonary, hepatic, renal or CNS impairment (although patients with controlled brain metastases are routinely treated). They should be monitored carefully for toxicity, particularly haematological, cardiac and respiratory adverse events; many aldesleukin-induced adverse events can be managed with routine treatments and interventions. Concurrent treatment with cardiotoxic, myelotoxic, hepatotoxic, nephrotoxic or psychotropic agents may potentiate the toxic effects of aldesleukin. Aldesleukin should be withdrawn (not reduced in dosage) in the event of serious adverse events. Aldesleukin has been used successfully as part of home therapy (self-injection by the patient) in patients with melanoma. Formal dosage or treatment guidelines for subcutaneous administration are not available.
Similar content being viewed by others


References
Jeal W, Goa KL. Aldesleukin (recombinant Interleukin-2): a review of its pharmacological properties, clinical efficacy and tolerability in patients with renal cell carcinoma. BioDrugs 1997 Apr; 7 (4): 285–317
Whittington R, Faulds D. Interleukin-2: a review of its pharmacological properties and therapeutic use in patients with cancer. Drugs 1993 Sep; 46: 446–514
Vlasveld LT, Rankin EM Recombinant interleukin-2 in cancer: basic and clinical aspects. Cancer Treat Rev 1994; 20 (3): 275–311
Chiron BV (Amsterdam). Proleukin® product monograph. 1997. (Data on file)
Winkelhake JL, Gauny SS Human recombinant interleukin-2 as an experimental therapeutic. Pharmacol Rev 1990; 42 (1): 1–28
Bruton JK, Koeller JM. Recombinant interleukin-2. Pharmaco-therapy 1994 Nov–Dec; 14: 635–56
Malek TR, Gutgsell NS. IL-2 and its receptor: structure, function, and regulation of expression. In: Atkins MB, Mier JW, editors. Therapeutic applications of interleukin-2. New York: Marcel Dekker, Inc., 1993: 3–25
Kintzel PE, Calis KA. Recombinant interleukin-2: a biological response modifier. Clin Pharm 1991 Feb; 10: 110–28
Lotze MT, Matory YL, Ettinghausen SE, et al. In vivo administration of purified human interleukin 2. II. Half life, immunologic effects, and expansion of peripheral lymphoid cells in vivo with recombinant IL 2. J Immunol 1985 Oct; 135 (4): 2865–75
Sosman JA, Weiss GR, Margolin KA, et al Phase IB clinical trial of anti-CD3 followed by high-dose bolus interleukin-2 in patients with metastatic melanoma and advanced renal cell carcinoma: clinical and immunologic effects. J Clin Oncol 1993; 11 (8): 1496–505
Castello G, Cornelia P, Manzo T, et al Immunological and clinical effects of intramuscular rIFNα-2a and low dose subcutaneous rIL-2 in patients with advanced malignant melanoma. Melanoma Res 1993; 3 (1): 43–9
Keilholz U, Scheibenbogen C, Tilgen W, et al Interferon-α and interleukin-2 in the treatment of metastatic melanoma: comparison of two phase II trials. Cancer 1993; 72 (2): 607–14
von Rohr A, Ghosh AK, Thatcher N, et al Immunomodulation during prolonged treatment with combined interleukin-2 and interferon-alpha in patients with advanced malignancy. Br J Cancer 1993; 67 (1): 163–71
Lopez M, Carpano S, Cavaliere R, et al. Biochemotherapy with thymosin al, interleukin-2 and dacarbazine in patients with metastatic melanoma: clinical and immunological effects. Ann Oncol 1994 Oct; 5: 741–6
Fiedler W, Jasmin C, De Mulder PHM, et al. A phase II study of sequential recombinant interleukin-2 followed by dacarbazine in metastatic melanoma. Eur J Cancer 1992 Feb–Mar; 28: 443–6
Soubrane C, Mouawad R, Ichen M, et al Follow up of soluble IL-2 receptor level in metastatic malignant melanoma patients treated by chemoimmunotherapy. Clin Exp Immunol 1994; 95 (2): 232–6
Mouawad R, Ichen M, Rixe O, et al Study of IL-2 receptor expression after chemoimmunotherapy in patients treated for metastatic malignant melanoma. Clin Exp Immunol 1994; 97 (3): 342–6
Fossa SD, Aamdal S, Naume B, et al Serum levels of cytokines and soluble cytokine receptors in patients with metastatic renal cell carcinoma or malignant melanoma receiving IL-2/interferon-α combination therapy. Acta Oncol 1995; 34 (5): 599–603
Schneekloth C, Korfer A, Hadam M, et al Low-dose interleukin-2 in combination with interferon-α effectively modulates biological response in vivo. Acta Haematol 1993; 89 (1): 13–21
Atzpodien J, Rirchner H, Korfer A, et al Expansion of peripheral blood natural killer cells correlates with clinical outcome in cancer patients receiving recombinant subcutaneous interleukin- and interferon-α2. Tumor Biol 1993; 14 (6): 354–9
Hanninen EL, Korfer A, Hadam M, et al. Biological monitoring of low-dose interleukin 2 in humans: solunle interleukin 2 receptors, cytokine, and cell surface phenotypes. Cancer Res 1991; 50: 6312–6
Zambello R, Trentin L, Cerutti A, et al Independent expression of p55 and p75 interleukin-2 receptors (IL-2R) during intravenous or subcutaneous administration of recombinant interleukin-2 (rIL-2) by T-lymphocytes and natural killer cells. Cancer 1994; 74 (9): 2562–9
Farace F, Angevin E, Dietrich P-Y, et al Low-dose IL-2 treatment: activation of discrete T- and NK-cell sub-populations in vivo. Int J Cancer 1995; 62 (5): 523–8
Sarna G, Machleder H, Collins J, et al A comparative study of intravenous versus intralymphatic interleukin-2, with assessment of effects of interleukin-2 on both peripheral blood and thoracic-duct lymph. J Immunother 1994; 15 (2): 140–6
Dilloo D, Laws H-J, Hanenberg H, et al Induction of two distinct natural killer-cell populations, activated T cells and antineoplastic cytokines, by interleukin-2 therapy in children with solid tumors. Exp Hematol 1994; 22 (11): 1081–8
Schomburg A, Menzel T, Korfer A, et al In vivo and ex vivo antitumor activity in patients receiving low-dose subcutaneous recombinant interleukin-2. Nat Immun 1992; 11 (3): 133–43
Mitchell MS, Kempf RA, Hard W, et al. Effectiveness and tolerability of low-dose cyclophosphamide and low-dose intravenous interleukin-2 disseminated melanoma. J Clin Oncol 1988 Mar; 6 (3): 409–24
Landmann R, Keilholz U, Scheibenbogen C, et al Relationship between soluble tumor necrosis factor (TNF) receptors and TNFα during immunotherapy with interleukin-2 and/or interferon α. Cancer Immunol Immunother 1994; 38 (2): 113–8
Weidmann E, Bergmann L, Stock J, et al. Rapid cytokine release in cancer patients treated with interleukin-2. J Immunother 1992 Aug; 12: 123–31
Becker JC, Dummer R, Schwinn A, et al Circulating intercellular adhesion molecule-1 in melanoma patients: induction by interleukin-2 therapy. J Immunother 1992; 12 (2): 147–50
Abbate I, Correale M, Musci MD, et al Modification of soluble immunological parameters during treatment with interleukin-2. Int J Biol Markers 1993; 8 (4): 227–32
Schaafsma MR, Falkenburg JHF, Landegent JE, et al. In vivo production of interleukin-5, granulocyte-macrophage colony-stimulating factor, macrophage colony-stimulating factor, and interleukin-6 during intravenous administration of high-dose interleukin-2 in cancer patients. Blood 1991 Oct 15; 78 (8): 1981–7
Baars JW, Wolbink G-J, Hart MHL, et al The release of interleukin-8 during intravenous bolus treatment with interleukin-2. Ann Oncol 1994; 5 (10): 929–34
Lissoni P, Tisi E, Brivio F, et al Increase in soluble interleukin-2 receptor and neopterin serum levels during immunotherapy of cancer with interleukin-2. Eur J Cancer 1991; 27 (8): 1014–6
Rosenberg SA, Lotze MT, Muul LM, et al. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N Engl J Med 1985 Dec 5; 313: 1485–92
Laghi PF, Capecchi PL, Saletti M, et al Haematological findings and tolerance of subcutaneous low-dose interleukin-2 treatment in melanoma patients: preliminary results. Int J Immunother 1992; 8 (1): 7–14
West WH, Tauer KW, Yannelli JR, et al. Constant-infusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N Engl J Med 1987 Apr 9; 316: 898–905
Rivoltini L, Viggiano V, Spinazze S, et al In vitro anti-tumor activity of eosinophils from cancer patients treated with subcutaneous administration of interleukin 2. Role of interleukin 5. Int J Cancer 1993; 54 (1): 8–15
MacFarlane MP, Yang JC, Guleria AS, et al. The hematologic toxicity of interleukin-2 in patients with metastatic melanoma and renal cell carcinoma. Cancer 1995 Feb 15; 75: 1030–7
Flaherty LE, Redman BG, Chabot GG, et al. A phase I-II study of dacarbazine in combination with outpatient interleukin-2 in metastatic malignant melanoma. Cancer 1990 Jun 1; 65: 2471–7
Dummer R, Posseckert G, Sugamura K, et al. Circulating interleukin-2 receptors are a group of multimeric proteins withh immunoreactivity for interleukin-5 receptor α, β and γ chains. J Interferon Cytokine Res 1996; 16: 315–20
Isacson R, Kedar E, Barak V, et al Chemo-immunotherapy in patients with metastatic melanoma using sequential treatment with dacarbazine and recombinant human interleukin-2: evaluation of hematologic and immunologic parameters and correlation with clinical response. Immunol Lett 1992; 33 (2): 127–34
Sanderson CJ Interleukin-5, eosinophils, and disease. Blood 1992; 79 (12): 3101–9
Brossart P, Schmier J-W, Kriiger S, et al. A polymerase chain reaction-based semiquantitative assessment of malignant melanoma cells in peripheral blood. Cancer Res 1995; 55: 4065–8
Hanninen EL, Knuver-Hopf J, Atzpodien J. Immunogenicity of recombinant human interleukin-2: biological features and clinical relevance. Biotherapy 1993; 6: 251–61
Whitehead RP, Ward D, Hemingway L, et al. Subcutaneous recombinant interleukin 2 in a dose escalating regimen in patients with metastatic renal cell adenocarcinoma. Cancer Res 1990 Oct 15; 50: 6708–15
Chiron Corporation. Proleukin prescribing information. Emeryville, USA, 1996
Lindemann A, Brossart P, Hoffken K, et al Immunomodulatory effects of ultra-low-dose interleukin-2 in cancer patients: a phase-IB study. Cancer Immunol Immunother 1993; 37 (5): 307–15
Boon T, Cerottini J-C, Van den Eynde B, et al. Tumor antigens recognized by T lymphocytes. Annu Rev Immunol 1994; 12: 337–65
Boon T. Tumor antigens recognized by cytolytic T lymphocytes: present perspectives for specific immunotherapy. Int J Cancer 1993; 54: 177–80
Plaisance S, Rubinstein E, Alileche A, et al. Human melanoma cells express a functional interleukin-2 receptor. Int J Cancer 1993; 55(1): 164–70
Becker JC, Brocker EB. Lymphocyte-melanoma interaction: role of surface molecules. Recent Results Cancer Res 1995; 139: 205–14
Becker JC, Termeer C, Schmidt RE, et al. Soluble intercellular adhesion molecule-1 inhibits MHC-restricted specific T cell/tumour interaction. J Immunol 1993 Dec 15; 151 (12): 7224–32
Willhauck M, Mohler T, Scheibenbogen C, et al. T-cell receptor β variable region diversity in melanoma metastases after interleukin 2-based immunotherapy. Clin Cancer Res 1996 Apr; 2: 767–72
Konrad MW, Hemstreet G, Hersh EM, et al. Pharmacokinetics of recombinant interleukin 2 in humans. Cancer Res 1990; 50: 2009–17
Bocci V, Carraro F, Zeuli M, et al The lymphatic route. VIII. Distribution and plasma clearance of recombinant human interleukin-2 after SC administration with albumin in patients. Biotherapy 1993; 6 (1): 73–7
Fish R, Keen C, Shelley M, et al. Continuous IV interleukin-2 infusion therapy: unusual pharmacokinetics [abstract]. Eur J Cancer 1991; 27 Suppl. 2: S224
Miller AB, Hoogstraten B, Staquet M, et al. Reporting results of cancer treatment. Cancer 1981; 47: 207–14
Bar MH, Sznol M, Atkins MB, et al. Metastatic malignant melanoma treated with combined bolus and continuous infusion interleukin-2 and lymphokine-activated killer cells. J Clin Oncol 1990 Jul; 8: 1138–47
Dillman RO, Oldham RK, Tauer KW, et al. Continuous interleukin-2 and lymphokine-activated killer cells for advanced cancer: a National Biotherapy Study Group trial. J Clin Oncol 1991 Jul; 9: 1233–40
Dutcher JP, Creekmore S, Weiss GR, et al. A phase II study of interleukin-2 and lymphokine-activated killer cells in patients with metastatic malignant melanoma. J Clin Oncol 1989 Apr; 7: 477–85
Gaynor ER, Weiss GR, Margolin KA, et al. Phase I study of high-dose continuous-infusion recombinant interleukin-2 and autologous lymphokine-activated killer cells in patients with metastatic or unresectable malignant melanoma and renal cell carcinoma. J Natl Cancer Inst 1990; 82: 1397–402
Rosenberg SA, Lotze MT, Yang JC, et al. Experience with the use of high-dose interleukin-2 in the treatment of 652 cancer patients. Ann Surg 1989; 210: 474–85
Dillman RO, Church C, Oldham RK, et al. Inpatient continuous-infusion interleukin-2 in 788 patients with cancer. The National Biotherapy Study Group experience. Cancer 1993 Apr 1; 71: 2358–70
Parkinson DR, Fisher RI, Rayner AA, et al Therapy of renal cell carcinoma with interleukin-2 and lymphokine-activated killer cells: phase II experience with a hybrid bolus and continuous infusion interleukin-2 regimen. J Clin Oncol 1990; 8 (10): 1630–6
Bajorin DF, Chapman PB, Wong G, et al. Phase I evaluation of a combination of monoclonal antibody R24 and interleukin 2 in patients with metastatic melanoma. Cancer Res 1990 Dec 1; 50: 7490–5
Parkinson DR, Abrams JS, Wiernik PH, et al. Interleukin-2 therapy in patients with metastatic malignant melanoma: a phase II study. J Clin Oncol 1990 Oct; 8: 1650–6
Rosenberg SA, Lotze MT, Muul LM, et al. A progress report on the treatment of 157 patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-dose interleukin-2 alone. N Engl J Med 1987; 316(15): 889–97
Rosenberg SA, Yang JC, Topalian SL, et al. Treatment of 283 consecutive patients with metastatic melanoma or renal cell cancer using high-dose bolus interleukin 2. JAMA 1994 Mar 23-30; 271: 907–13
Whitehead RP, Kopecky KJ, Samson MK, et al. Phase II study of intravenous bolus recombinant interleukin-2 in advanced malignant melanoma: Southwest Oncology Group study. J Natl Cancer Inst 1991 Sep 4; 83: 1250–1
Kruit WH, Goey SH, Monson JRT, et al. Clinical experience with the combined use of recombinant interleukin-2 (IL2) and interferon alfa-2a (IFNα) in metastatic melanoma. Br J Haematol 1991 Oct; 79 Suppl. 1: 84–6
Dillman RO, Oldham RK, Barth NM, et al. Continuous interleukin-2 and tumor-infiltrating lymphocytes as treatment of advanced melanoma. Cancer 1991 Jul 1; 68: 1–8
Verdi CJ, Taylor CW, Croghan MK, et al. Phase I study of low-dose cyclophosphamide and recombinant interleukin-2 for the treatment of advanced cancer. J Immunother 1992 May; 11:286–91
Dillman RO, Oldham RK, Barth NM, et al. Recombinant interleukin-2 and adoptive immunotherapy alternated with dacarbazine therapy in melanoma: a National Biotherapy Study Group trial. J Natl Cancer Inst 1990 Aug 15; 82: 1345–9
Dummer R, Gore ME, Hancock BW, et al A multicenter phase II clinical trial using dacarbazine and continuous infusion interleukin-2 for metastatic melanoma: clinical data and immunomonitoring. Cancer 1995; 75 (4): 1038–44
Shiloni E, Pouillart P, Janssens J, et al. Sequential dacarbazine chemotherapy followed by recombinant interleukin-2 in metastatic melanoma. A pilot multicentre phase I–II study. Eur J Cancer Clin Oncol 1989; 25 Suppl. 3: S45–49
Stoter G, Shiloni E, Aamdal S, et al. Sequential administration of recombinant human interleukin-2 and dacarbazine in metastatic melanoma. A multicentre phase II study. Eur J Cancer Clin Oncol 1989; 25 Suppl. 3: S41–43
Demchak PA, Mier JW, Robert NJ, et al. Interleukin-2 and high-dose cisplatin in patients with metastatic melanoma: a pilot study. J Clin Oncol 1991 Oct; 9: 1821–30
Anderson CM, Buzaid AC, Legha SS. Systemic treatments for advanced cutaneous melanoma. Oncology 1995 Nov; 9 (11): 1149–58
Dorval T, Négrier S, Chevreau C, et al. Results of a French multicentric randomized trial of chemoimmunotherapy (cisplatin (P), IL-2 (Proleukin®), with or without IFN (Roferon®) in metastatic malignant melanoma [abstract no. * 1347]. Thirtieth Annual Meeting, American Society of Clinical Oncology; 1994 May 14-17; Dallas, 395
Keilholz U, Goey SH, Punt CJA, et al. Interferon-alpha and interleukin-2 with or without cisplatinum in metastatic melanoma: a randomized trial of the EORTC Melanoma Cooperative Group. J Clin Oncol 1997. In press
Keilholz U, Scheibenbogen C, Stoelben E, et al. Immunotherapy of metastatic melanoma with interferon-α and interleukin-2: pattern of progression in responders and patients with stable disease with or without resection of residual lesions. Eur J Cancer 1994; 30A (7): 955–8
Dreno B, Cupissol D, Joly P, et al Ambulatory treatment of metastatic melanoma associating subcutaneous dacarbazine, interferon α and interleukin-2. J Eur Acad Dermatol Venereol 1995; 4 (3): 248–53
Khayat D, Borel C, Tourani JM, et al Sequential chemoimmunotherapy with cisplatin, interleukin-2, and interferon alfa-2a for metastatic melanoma. J Clin Oncol 1993; 11 (11): 2173–80
Antoine EC, Rixe O, Vuillemin E, et al A phase II study of tamoxifen combined with cisplatin-interleukin 2 and alpha-interferon in metastatic melanoma. Am J Clin Oncol 1995; 18 (5): 421–4
Atkins MB, O’Boyle K, Sosman J, et al. A multi-institutional phase II trial of intensive combination chemoimmunotherapy for metastatic melanoma [abstract no. 1348]. 29th Annual Meeting, American Society of Clinical Oncology; 1993 May 16-18; Orlando, 394
Atzpodien J, Lopez Hanninen E, Kirchner H, et al. Chemoimmunotherapy of advanced malignant melanoma: sequential administration of subcutaneous interleukin-2 and interferon-α after intravenous dacarbazine and carboplatin or intravenous dacarbazine, cisplatin, carmustine and tamoxifen. Eur J Cancer 1995; 31A (6): 876–81
Flaherty LE, Robinson W, Redman BG, et al. A phase II study of dacarbazine and cisplatin in combination with outpatient administered interleukin-2 in metastatic malignant melanoma. Cancer 1993 Jun 1; 71: 3520–5
Guida M, Latorre A, Mastria A, et al. Subcutaneous recombinant interleukin-2 plus chemotherapy with cisplatin and dacarbazine in metastatic melanoma. Eur J Cancer 1996; 32A (4): 730–3
Ron IG, Mordish Y, Eisenthal A, et al A phase II study of combined administration of dacarbazine and carboplatin with home therapy of recombinant interleukin-2 and interferon-α2a in patients with advanced malignant melanoma. Cancer Immunol Immunother 1994; 38 (6): 379–84
Proebstle TM, Scheibenbogen C, Sterry W, et al. A phase II study of dacarbazine, cisplatin, interferon-α and high-dose interleukin-2 in ‘poor-risk’ metastatic melanoma. Eur J Cancer 1996; 32A (9): 1530–3
Barth A, Wanek LA, Morton DL Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg 1995; 181 (3): 193–201
Legha SS. Current therapy for malignant melanoma. Semin Oncol 1989 Feb; 16 (1) Suppl. 1: 34–44
Bergmann L. Malignant melanoma — prognosis and actual treatment strategies with chemotherapy and biological response modifiers. Eur J Cancer Clin Oncol 1989; 25 Suppl. 3: S31–36
National Cancer Institute. Melanoma for Physicians. In: Clinical cancer information for physicians, WWW CancerNet [online]. National Cancer Institute; Mar 1997. Available from: URL: http://www.arc.com/cgi-bin/Cancernet.sh?english/physician=Melanoma_for_Physicians [Accessed 1997 Apr 7].
Tartour E, Dorval T, Mosseri V, et al. Serum interleukin 6 and C-reactive protein levels correlate with resistance to IL-2 therapy and poor survival in melanoma patients. Br J Cancer 1994; 69: 911–3
Tartour E, Blay JY, Dorval T, et al. Predictors of clinical response to interleukin-2-based immunotherapy in melanoma patients: a French multiinstitutional study. J Clin Oncol 1996 May; 14 (5): 1697–703
Keilholz U, Scheibenbogen C, Sommer M, et al. Prognostic factors for response and survival in patients with metastatic melanoma receiving immunotherapy. Melanoma Res 1996; 6: 173–8
Palmer PA, Atzpodien J, Philip T, et al A comparison of 2 modes of administration of recombinant interleukin-2: continuous intravenus infusion alone versus subcutaneous administration plus interferon alpha in patients with advanced renal cell carcinoma. Cancer Biother 1993; 8 (2): 123–36
Schomburg A, Kirchner H, Lopez-Hänninen E, et al Hepatic and serologic toxicity of systemic interleukin-2 and/or interferon-α: evidence of a risk-benefit advantage of subcutaneous therapy. Am J Clin Oncol Cancer Clin Trials 1994; 17 (3): 199–209
Guida M, Abbate I, Casamassima A, et al Long-term subcutaneous recombinant interleukin-2 as maintenance therapy: biological effects and clinical implications. Cancer Biother 1995; 10 (3): 195–203
Dummer R, Miller K, Eilles C, et al. The skin: an immunoreactive target organ during interleukin-2 administration? Dermatologica 1991 Aug; 183: 95–9
Dillman RO. The clinical experience with interleukin-2 in cancer therapy. Cancer Biother 1994 Fall; 9: 183–209
Rifkin RM, Thomas MR, Mughal TI, et al. Malignant melanoma — profile of an epidemic. West J Med 1991 Jul; 149:43–6
American Cancer Society. Skin Cancer. In: Cancer facts & figures — 1997. American Cancer Society; 1997 [online]. Available from: URL: http://www.cancer.org/97skin.html [Accessed 1997 Feb 3].
Greenstein DS, Rogers GS Management of stage I malignant melanoma. Dermatol Surg 1995; 21 (11): 927–37
Lejeune F, Bauer J, Leyvraz S, et al. Disseminated melanoma, preclinical therapeutic studies, clinical trials, and patient treatment. Curr Opin Oncol 1993 Mar; 5: 390–6
Legha SS, Ring S, Bedikian A, et al. Treatment of metastatic melanoma with combined chemotherapy containing cisplatin, vinblastine and dacarbazine (CVD) and biotherapy using interleukin-2 and interferon-α. Ann Oncol 1996; 7: 827–35
Richards JM, Mehta N, Ramming K. Sequential chemoimmunotherapy in the treatment of metastatic melanoma. J Clin Oncol 1992 Aug; 10: 1338–43
Drugs of choice for cancer chemotherapy. Med Lett Drugs Ther 1995; 37 (945): 25-32
Author information
Authors and Affiliations
Corresponding author
Additional information
Various sections of the manuscript reviewed by: L. Bergmann, Medizinische Klinik III, Universitätsklinik, Frankfurt, Germany; R.O. Dillman, Hoag Cancer Center, Hoag Hospital, Newport Beach, California, USA; R. Dummer, Department of Dermatology, University of Zurich Medical School, Zurich, Switzerland; M. Green, Department of Clinical Haematology and Medical Oncology, Royal Melbourne Hospital, Melbourne, Victoria, Australia; U. Keilholz, Medizinische Klinik und Poliklinik V, Hämatologie, Onkologie und Rheumatologie, Universität Heidelberg, Heidelberg, Germany; D. Khayat, Department of Medical Oncology, Salpêtrière Hospital, Paris, France; S.S. Legha, Department of Melanoma/Sarcoma, Medical Oncology, MD Anderson Cancer Center, Texas Medical Center, Houston, Texas, USA; G. Semenzato, Dipartimento di Medicina Clinica e Sperimentale, Università Degli Studi di Padova, Padua, Italy; L.T. Vlasveld, Department of Internal Medicine, Diaconessenhuls, Eindhoven, The Netherlands; R.P. Whitehead, School of Medicine/Department of Internal Medicine, Texas University Health Sciences Center, Lubbock, Texas, USA.
Rights and permissions
About this article
Cite this article
Noble, S., Goa, K.L. Aldesleukin (Recombinant Interleukin-2). BioDrugs 7, 394–422 (1997). https://doi.org/10.2165/00063030-199707050-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00063030-199707050-00007