
Abstract
Background
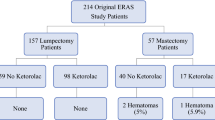
Although ketorolac is an effective adjunct for managing pain in the perioperative period, it is associated with a risk of postoperative bleeding. This study retrospectively investigated the association between ketorolac use and both reoperation and postoperative opioid use among mastectomy patients.
Methods
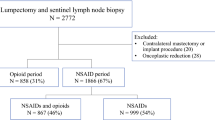
The study identified all women undergoing mastectomy (unilaterally or bilaterally) at our ambulatory surgery cancer center from January 2016 to June 2019. The primary outcome was reoperation for bleeding on postoperative day 0 or 1, and the secondary outcome was postoperative opioid use. The association between ketorolac and outcomes was assessed using multivariable regression models. The covariates were age, body mass index, breast reconstruction, bilateral surgery, peripheral nerve block, and preoperative antiplatelet and/or anticoagulation medication.
Results
A cohort of 3469 women were identified. Ketorolac was given to 1549 (45%) of the women, with 922 women (60%) receiving 30 mg and 627 women (40%) receiving 15 mg. The overall reoperation rate for bleeding was 3.1% (1.8% without ketorolac vs 4.8% with ketorolac). In the multivariable analysis, ketorolac was associated with a higher risk of reoperation [odds ratio (OR) 2.43; 95% confidence interval (CI) 1.60–3.70; P < 0.0001]. Ketorolac also was associated with a lower proportion of patients receiving any postoperative narcotic within 24 h (15 mg: OR 0.73; 95% CI 0.57–0.94; P = 0.014 vs 30 mg: OR 0.52; 95% CI 0.42–0.66; P < 0.0001).
Conclusions
Ketorolac use decreased postoperative opioid use, but this benefit was outweighed by the increased risk of bleeding requiring reoperation. This finding led to a change in practice at the authors’ center, with ketorolac no longer administered in the perioperative care of the mastectomy patient.
Similar content being viewed by others

References
Batdorf NJ, Lemaine V, Lovely JK, et al. Enhanced recovery after surgery in microvascular breast reconstruction. J Plast Reconstr Aesthet Surg. 2015;68:395–402.
Bonde C, Khorasani H, Eriksen K, Wolthers M, Kehlet H, Elberg J. Introducing the fast-track surgery principles can reduce length of stay after autologous breast reconstruction using free flaps: a case–control study. J Plast Surg Hand Surg. 2015;49:367–71.
Dumestre DO, Webb CE, Temple-Oberle C. Improved recovery experience achieved for women undergoing implant-based breast reconstruction using an enhanced recovery after surgery model. Plast Reconstr Surg. 2017;139:550–9.
Jogerst K, Thomas O, Kosiorek HE, et al. Same-day discharge after mastectomy: breast cancer surgery in the era of ERAS. Ann Surg Oncol. 2020;27:3436–45.
Maslin B, Lipana L, Roth B, Kodumudi G, Vadivelu N. Safety considerations in the use of ketorolac for postoperative pain. Curr Drug Saf. 2017;12:67–73.
Rojas KE, Fortes TA, Flom P, Manasseh DM, Andaz C, Borgen P. Intraoperative ketorolac use does not increase the risk of bleeding in breast surgery. Ann Surg Oncol. 2019;26:3368–73.
Gobble RM, Hoang HL, Kachniarz B, Orgill DP. Ketorolac does not increase perioperative bleeding: a meta-analysis of randomized controlled trials. Plast Reconstr Surg. 2014;133:741–55.
Tokita H, Twersky R, Laudone V, et al. Complex cancer surgery in the outpatient setting: the Josie Robertson Surgery Center. Anesth Analg. 2020;131:699–707.
Nielsen S, Degenhardt L, Hoban B, Gisev N. A synthesis of oral morphine equivalents (OME) for opioid utilisation studies. Pharmacoepidemiol Drug Saf. 2016;25:733–7.
Afonso AM, McCormick PJ, Assel MJ, et al. Enhanced recovery programs in an ambulatory surgical oncology center. Anesth Analg. 2021. In press.
Assel MJ, Laudone VP, Twersky RS, Vickers AJ, Simon BA. Assessing rapidity of recovery after cancer surgeries in a single overnight short-stay setting. Anesth Analg. 2019;129:1007–13.
Stephens DM, Richards BG, Schleicher WF, Zins JE, Langstein HN. Is ketorolac safe to use in plastic surgery? A critical review. Aesthet Surg J. 2015;35:462–6.
Chan DK, Parikh SR. Perioperative ketorolac increases post-tonsillectomy hemorrhage in adults but not children. Laryngoscope. 2014;124:1789–93.
Cawthorn TR, Phelan R, Davidson JS, Turner KE. Retrospective analysis of perioperative ketorolac and postoperative bleeding in reduction mammoplasty. Can J Anaesth. 2012;59:466–72.
Davidson AJ. Complication rates in anesthesia. Anesthesiology. 2021;134:7–8.
Acknowledgment
This research was supported by the National Cancer Institute of the National Institutes of Health under Award No. P30CA008748. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. McCormick's spouse holds stock in Johnson & Johnson. Monica Morrow has received honoraria from Roche and Genomic Health. The remaining authors have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
McCormick, P.J., Assel, M., Van Zee, K.J. et al. Intraoperative Ketorolac is Associated with Risk of Reoperation After Mastectomy: A Single-Center Examination. Ann Surg Oncol 28, 5134–5140 (2021). https://doi.org/10.1245/s10434-021-09722-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-09722-4