
Abstract
Background
Eligibility for nipple-sparing mastectomy (NSM) varies widely on the basis of patient and tumor factors.
Methods
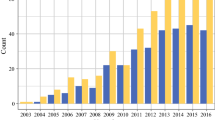
Review of patients undergoing NSM from June 2007 to December 2012 at our institution was performed. Patient and tumor characteristics, complications, and recurrences were collected. NSM from 2007 to 2010 and 2011 to 2012 were compared to assess trends in eligibility and outcomes over time.
Results
NSM was performed on 645 breasts in 370 patients. Indications were risk reduction in 330 (51.2 %), invasive cancer in 226 (35.0 %), and ductal carcinoma-in situ in 89 (13.8 %) breasts. Fifty-one (13.8 %) patients had positive lymph nodes. Twenty-seven (7.3 %) patients received neoadjuvant chemotherapy. Forty-eight (7.4 %) breasts had prior radiotherapy. Total nipple necrosis occurred in 11 (1.7 %) breasts. Twenty-four (3.7 %) breasts had nipples removed as a result of positive subareolar/nipple margins. At 22 months’ mean follow-up, local recurrence occurred in 4 of 156 (2.6 %) breasts operated on for cancer through 2011. No recurrences involved the nipple. NSM performed in 2011–2012 (n = 475) compared to 2007–2010 (n = 170), were more often for cancer, in patients with higher body mass index, and on larger breasts (p < 0.001). There was no significant difference in total nipple necrosis rates between groups. Nipple loss due to positive subareolar/nipple margins was significantly less in 2011–2012 (p = 0.027).
Conclusions
Eligibility for NSM has expanded to include women with higher body mass index and larger breasts, with no increase in nipple loss due to ischemia. Rates of positive subareolar margins have decreased over time, even though NSM is being performed more frequently for cancer, suggesting improved patient selection.

Similar content being viewed by others

References
Toth BA, Lappert P. Modified skin incisions for mastectomy: the need for plastic surgical input in preoperative planning. Plast Reconstr Surg. 1991;87:1048–53.
Pouhaer LB, Sarfati I, Missana MC, Petit JY, Le MG. Cosmetic results and complications in breast cancer patients after total mastectomy with circular incision and immediate breast reconstruction. Plast Reconstr Surg. 1995;95:1324–7.
Gerber B, Krause A, Reimer T, et al. Skin-sparing mastectomy with conservation of the nipple–areola complex and autologous reconstruction is an oncologically safe procedure. Ann Surg. 2003;238:120–7.
Boneti C, Yuen J, Santiago C, et al. Oncologic safety of nipple skin-sparing or total skin-sparing mastectomies with immediate reconstruction. J Am Coll Surg. 2011;212:686–95.
Crowe JP, Patrick RJ, Yetman RJ, Djohan R. Nipple-sparing mastectomy update. Arch Surg. 2008;143:1106–10.
Harness JK, Vetter TS, Salibian AH. Areola and nipple–areola-sparing mastectomy for breast cancer treatment and risk reduction: report of an initial experience in a community hospital setting. Ann Surg Oncol. 2011;18:917–22.
Jensen JA, Orringer JS, Giuliano AE. Nipple-sparing mastectomy in 99 patients with a mean follow-up of 5 years. Ann Surg Oncol. 2011;18:1665–70.
Peled AW, Foster RD, Stover AC, et al. Outcomes after total skin-sparing mastectomy and immediate reconstruction in 657 breasts. Ann Surg Oncol. 2012;19:3402–9.
Petit JY, Veronesi U, Orecchia R, et al. Nipple sparing mastectomy with nipple areola intraoperative radiotherapy: one thousand and one cases of a five years experience at the European Institute of Oncology of Milan (EIO). Breast Cancer Res Treat. 2009;117:333–8.
Wagner JL, Fearmonti R, Hunt KK, et al. Prospective evaluation of the nipple–areola complex sparing mastectomy for risk reduction and for early-stage breast cancer. Ann Surg Oncol. 2012;19:1137–44.
Filho PD, Capko D, Barry JM, Morrow M, Pusic A, Sacchini VS. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: the Memorial Sloan-Kettering Cancer Center experience. Ann Surg Oncol. 2011;18:3117–22.
Stolier AJ, Sullivan SK, Dellacroce FJ. Technical considerations in nipple-sparing mastectomy: 82 consecutive cases without necrosis. Ann Surg Oncol. 2008;15:1341–7.
Blechman KM, Karp NS, Levovitz C, et al. The lateral inframammary fold incision for nipple-sparing mastectomy: outcomes from over 50 immediate implant-based breast reconstructions. Breast J. 2013;19:31–40.
Rusby JE, Brachtel EF, Taghian A, Michaelson JS, Koerner FC, Smith BL. Microscopic anatomy within the nipple: implications for nipple-sparing mastectomy. Am J Surg. 2007;194:433–7.
Rusby JE, Kirstein LJ, Brachtel EF, Michaelson JS, Koerner FC, Smith BL. Nipple-sparing mastectomy: lessons from ex vivo procedures. Breast J. 2008;14:464–70.
Rusby JE, Brachtel EF, Othus M, Michaelson JS, Koerner FC, Smith BL. Development and validation of a model predictive of occult nipple involvement in women undergoing mastectomy. Br J Surg. 2008;95:1356–61.
Lohsiriwat V, Martella F, Rietjens F, et al. Paget’s disease as a local recurrence after nipple-sparing mastectomy: clinical presentation, treatment, outcome, and risk factor analysis. Ann Surg Oncol. 2012;19:850–5.
Steen ST, Chung AP, Han SH, Vinstein AL, Yoon JL, Giuliano AE. Predicting nipple–areolar involvement using preoperative breast MRI and primary tumor characteristics. Ann Surg Oncol. 2013;20:633–9.
Camp MS, Coopey SB, Tang R, et al. Management of positive subareolar margins in nipple sparing mastectomies. Paper presented at: American Society of Breast Disease, April 14, 2012, Dallas TX.
Schneider LF, Chen CM, Stolier AJ, Shapiro RL, Ahn CY, Allen RJ. Nipple-sparing mastectomy and immediate free-flap reconstruction in the large ptotic breast. Ann Plast Surg. 2012;69:425–8.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Coopey, S.B., Tang, R., Lei, L. et al. Increasing Eligibility for Nipple-Sparing Mastectomy. Ann Surg Oncol 20, 3218–3222 (2013). https://doi.org/10.1245/s10434-013-3152-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3152-x