
Abstract
Purpose
To determine survival differences for patients undergoing colonic or rectal resection for cancer on the basis of the specific anatomical location of primary tumor.
Methods
A total of 143,747 patients undergoing segmental colectomy, hemicolectomy, anterior resection, or abdominoperineal resection (APER) for adenocarcinoma from 1995 to 2009 were identified from 13 Surveillance, Epidemiology, and End Results regions. The primary end point was overall survival determined by adjusted hazard ratios (HRs); the secondary end point was lymph node yield.
Results
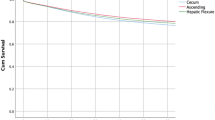
Total lymph node yield significantly decreased from proximal to distal resected segment in stage 0–II cancer, but not in stage III cancer. Lymph node ratio increased from cecum to hepatic flexure and then decreased distally (p < 0.001). Adjusted HRs revealed that survival after right colonic resection for ascending hepatic flexure and transverse colon cancer was not significantly different from cecal cancer. Survival after left colonic resection for descending colon cancer was not different from splenic flexure cancer, but sigmoid colectomy carried improved survival (HR 0.95, p = 0.027). APER carried worse survival compared to anterior resection (HR 1.28, p < 0.001) or right colonic resection for cecal cancer (HR 1.61, p < 0.001).
Conclusions
Survival after resection from colorectal cancer depends on specific anatomical segment and not just the division between colon and rectum, or left and right colon. This may be related to inherent differences in the anatomical characteristics of the particular colorectal segment, with varying lymph node yields contributing to understaging. This supports an individualized approach to colorectal cancer, with particular attention to surgical technique, leading to survival improvement.



Similar content being viewed by others


References
Weiss JM, Pfau PR, O’Connor ES, et al. Mortality by stage for right- versus left-sided colon cancer: analysis of Surveillance, Epidemiology, and End Results–Medicare data. J Clin Oncol. 2011;29:4401–9.
Yamauchi M, Morikawa T, Kuchiba A, et al. Assessment of colorectal cancer molecular features along bowel subsites challenges the conception of distinct dichotomy of proximal versus distal colorectum. Gut. 2012;61:847–54.
Azzoni C, Bottarelli L, Campanini N, et al. Distinct molecular patterns based on proximal and distal sporadic colorectal cancer: arguments for different mechanisms in the tumorigenesis. Int J Colorectal Dis. 2007;22:115–26.
Meguid RA, Slidell MB, Wolfgang CL, Chang DC, Ahuja N. Is there a difference in survival between right- versus left-sided colon cancers? Ann Surg Oncol. 2008;15:2388–94.
Benedix F, Kube R, Meyer F, Schmidt U, Gastinger I, Lippert H. Comparison of 17,641 patients with right- and left-sided colon cancer: differences in epidemiology, perioperative course, histology, and survival. Dis Colon Rectum. 2010;53:57–64.
Wray CM, Ziogas A, Hinojosa MW, Le H, Stamos MJ, Zell JA. Tumor subsite location within the colon is prognostic for survival after colon cancer diagnosis. Dis Colon Rectum. 2009;52:1359–66.
Chou JF, Row D, Gonen M, Liu YH, Schrag D, Weiser MR. Clinical and pathologic factors that predict lymph node yield from surgical specimens in colorectal cancer: a population-based study. Cancer. 2010;116:2560–70.
Shihab OC, Brown G, Daniels IR, Heald RJ, Quirke P, Moran BJ. Patients with low rectal cancer treated by abdominoperineal excision have worse tumors and higher involved margin rates compared with patients treated by anterior resection. Dis Colon Rectum. 2010;53:53–6.
Warren JL, Klabunde CN, Schrag D, Bach PB, Riley GF. Overview of the SEER–Medicare data: content, research applications, and generalizability to the United States elderly population. Med Care. 2002;40(8 Suppl):IV-3–18.
Morris EJ, Maughan NJ, Forman D, Quirke P. Identifying stage III colorectal cancer patients: the influence of the patient, surgeon, and pathologist. J Clin Oncol. 2007;25:2573–9.
Birkenkamp-Demtroder K, Olesen SH, Sorensen FB, et al. Differential gene expression in colon cancer of the caecum versus the sigmoid and rectosigmoid. Gut. 2005;54:374–84.
West NP, Hohenberger W, Weber K, Perrakis A, Finan PJ, Quirke P. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol. 2010;28:272–8.
Habr-Gama A, Perez RO, Proscurshim I, et al. Absence of lymph nodes in the resected specimen after radical surgery for distal rectal cancer and neoadjuvant chemoradiation therapy: what does it mean? Dis Colon Rectum. 2008;51:277–83.
Doll D, Gertler R, Maak M, et al. Reduced lymph node yield in rectal carcinoma specimen after neoadjuvant radiochemotherapy has no prognostic relevance. World J Surg. 2009;33:340–7.
Sprenger T, Rothe H, Homayounfar K, et al. Preoperative chemoradiotherapy does not necessarily reduce lymph node retrieval in rectal cancer specimens—results from a prospective evaluation with extensive pathological work-up. J Gastrointest Surg. 2010;14:96–103.
Disclosures
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Bhangu, A., Kiran, R.P., Slesser, A. et al. Survival After Resection of Colorectal Cancer Based on Anatomical Segment of Involvement. Ann Surg Oncol 20, 4161–4168 (2013). https://doi.org/10.1245/s10434-013-3104-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3104-5