
Abstract
Background: Successful breast conservation surgery (BCS) requires complete tumor excision. Margin status of the initial specimen determines the need for additional surgery. We explored factors associated with residual cancer (RC) upon follow-up surgery in patients with close, positive, or undetermined margins following BCS.
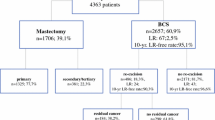
Methods: A retrospective analysis of 276 patients with initial close, positive, or undetermined margins who underwent re-excision (RE) or mastectomy was conducted. All initial excisions were intended as definitive procedures. Chi-square analysis was used to identify factors that may predict RC.
Results: Of 276 patients, 87 had close, 168 had positive, and 21 had undetermined margins on initial excision. Of this group, 63% (175/276) had RC upon RE or mastectomy. Of positive-margin patients, 68% had RC, compared with 53% of close-margin and 67% of undetermined-margin patients (P = .006). Tumors ≥2 cm were more often associated with RC than smaller tumors (70.8% vs. 56.5%; P = .07). This association was strongest in positive-margin patients (P = .04). High tumor grade was associated with RC in all groups. RC linearly increased with the number of involved margins (P = .02). Specimen inking with multiple colors was associated with decreased risk of RC (P = .004).
Conclusions: Over half of patients with involved or undetermined margins had RC upon RE or mastectomy. Positive and undetermined margins were more often associated with RC than close margins. Larger tumor size was associated with RC in patients with positive. Increasing tumor grade suggests a greater chance of detecting RC in all groups. Multiple involved margins led to a greater risk of RC.
Similar content being viewed by others


REFERENCES
Fisher B, Bauer M, Margolese R, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med 1985; 312: 665–73.
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002; 347: 1233–41.
Swanson G, Rynearson K, Symmonds R. Significance of margins of excision on breast cancer recurrence. Am J Clin Oncol 2002; 25: 438–41.
Papa M, Zippel D, Koller M, et al. Positive margins of breast biopsy: Is reexcision always necessary? Surg Oncol 1999; 70: 167–171.
Kearney T, Morrow M. Effect of reexcision on the success of breast conservation surgery. Ann Surg Oncol 1995; 2: 303–7.
Gwin J, Eisenberg B, Hoffman J. Incidence of gross and microscopic carcinoma in specimens from patients with breast cancer after reexcision lumpectomy. Ann Surg 1993; 218: 729–34.
Acosta J, Greenlee J, Gubler K. Surgical margins after needle localization breast biopsy. Am J Surg 1995; 170: 643–5.
Jardines L, Fowble B, Schultz D. Factors associated with a positive reexcision after excisional biopsy for invasive breast cancer. Surgery 1995; 118: 803–9.
Wazer D, Schmidt-Ullrich R, Schmid C, et al. The value of breast lumpectomy margin assessment as a predictor of residual tumor burden. Int J Radiat Oncol Biol Phys 1997; 38: 291–9.
Cheng L, Al-Kaisi N, Gordon N, et al. Relationship between the size and margin status of ductal carcinoma in situ of the breast and residual disease. J Natl Cancer Inst 1997; 89: 1356–60.
Neuschatz A, DiPetrillo T, Steinhoff M, et al. The value of breast lumpectomy margin assessment as a predictor of residual tumor burden in ductal carcinoma in situ of the breast. Cancer 2002; 94: 1917–24.
Ratanawichitrasin A, Rybicki L, Steiger E, et al. Predicting the likelihood of residual disease in women treated for ductal carcinoma in situ. J Am Coll Surgeons 1999; 188: 17–21.
Hollenbeck S, Cellini C, Christos P, et al. Breast cancer patients with residual invasive carcinoma are more accurately staged using additive tumor size assessment. Ann Surg Oncol 2004; 11: 59–64.
Nixon A, Neuberg D, Hayes D, et al. Relationship of patient age to pathologic features of the tumor and prognosis for patients with stage I or II breast cancer. J Clin Oncol 1994; 12: 888–94.
Jacquemier J, Seradour B, Hassoun J, Piana L. Special morphologic features of invasive carcinomas in women under 40 years of age. Breast Dis 1985; 1: 119–22.
Wazer D, Schmidt-Ullrich R, Ruthazer R, et al. The influence of age and extensive intraductal component histology upon breast lumpectomy margin assessment as a predictor of residual tumor. Int J Radiat Oncol Biol Phys 1999; 45: 885–91.
Wazer D, Schmidt-Ullrich R, Ruthazer R, et al. Factors determining outcome for breast-conserving irradiation with margin-directed dose escalation to the tumor bed. Int J Radiat Oncol Biol Phys 1998; 40: 851–8.
Bartelink H, Collette L, Fourquet A. Impact of a boost dose of 16 Gy on the local control and cosmesis in patients with early breast cancer: the EORTC “boost vs. no boost” trial. Int J Radiat Oncol Biol Phys 2000; 48 (Suppl 3): 111.
Smitt MC, Nowels KW, Zdeblick MJ, et al. The importance of the lumpectomy surgical margin status in long-term results of breast conservation. Cancer 1995; 76: 259–67.
Gibson GR, Lesnikoski BA, Yoo J, et al. A comparison of ink-directed and traditional whole-cavity re-excision for breast lumpectomy specimens with positive margins. Ann Surg Oncol 2001; 8: 693–704.
Singletary S. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg 2002; 184: 383–93.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cellini, C., Hollenbeck, S.T., Christos, P. et al. Factors Associated With Residual Breast Cancer After Re-excision for Close or Positive Margins. Ann Surg Oncol 11, 915–920 (2004). https://doi.org/10.1245/ASO.2004.12.037
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2004.12.037