Article Text

Abstract
Lymphangioleiomyomatosis can be associated with reversible airflow obstruction and although no guidelines around reversibility testing or inhaled therapy exist, many patients receive bronchodilators and inhaled corticosteroids. To better identify those who may benefit, we examined bronchodilator reversibility and inhaled therapy in a national cohort of 213 subjects. 20% of those tested had airway reversibility by standard criteria. 55% of patients used 13 different combinations of bronchodilators and inhaled corticosteroids. Increasing inhaler classes were associated with reversibility and more rapid FEV1 decline. Reversibility testing should be performed in all patients and inhaled therapy should be formally studied.
- rare lung diseases
Statistics from Altmetric.com
Introduction
Lymphangioleiomyomatosis (LAM) is a rare disease of women categorised by lung cysts, pneumothorax, lymphatic abnormalities and angiomyolipomas.1 Loss of function of the tuberous sclerosis proteins leads to activation of the mTOR-signalling node, resulting in a clone of ‘LAM cells’ that infiltrate the lungs and lymphatics causing tissue damage.2 Treatment with mammalian target of rapamycin (mTOR) inhibitors can slow disease progression.3 4 LAM cell associated airway narrowing results in airway obstruction which can be partially reversible and may be associated with faster lung function decline.5 6 Consequently, many women with LAM are treated with bronchodilators and also inhaled corticosteroids (ICS).
Reversibility testing and inhaled therapy are not covered by current guidelines and how different bronchodilator classes and ICS are used in women with LAM is unknown. This is of importance as bronchodilators may improve quality of life and beta adrenoceptor agonists have been suggested as potential adjuncts to mTOR inhibitors,7 whereas ICS have not been studied. To identify who may benefit from inhaled therapy and provide a baseline for interventional studies, we examined the prevalence and clinical associations of reversible airway obstruction and the use of inhaled therapy in a national cohort of women with LAM.
Methods
Consecutive women with definite or probable LAM attending a national clinical centre were recruited between 2011 and 2018.8 At first visit, detailed clinical and drug history, lung function, CT of the chest and abdomen were obtained. From 2015 onwards, reversibility was routinely tested in response to 2.5 mg nebulised salbutamol. A positive response was defined as an increase in FEV1 of at least 12% and 200 mL. Prospective loss of FEV1 was calculated from the slope of a regression line of sequential FEV1 measurements.4 All subjects gave written informed consent. Further details are given in the online supplementary file 1.
Supplemental material
Results
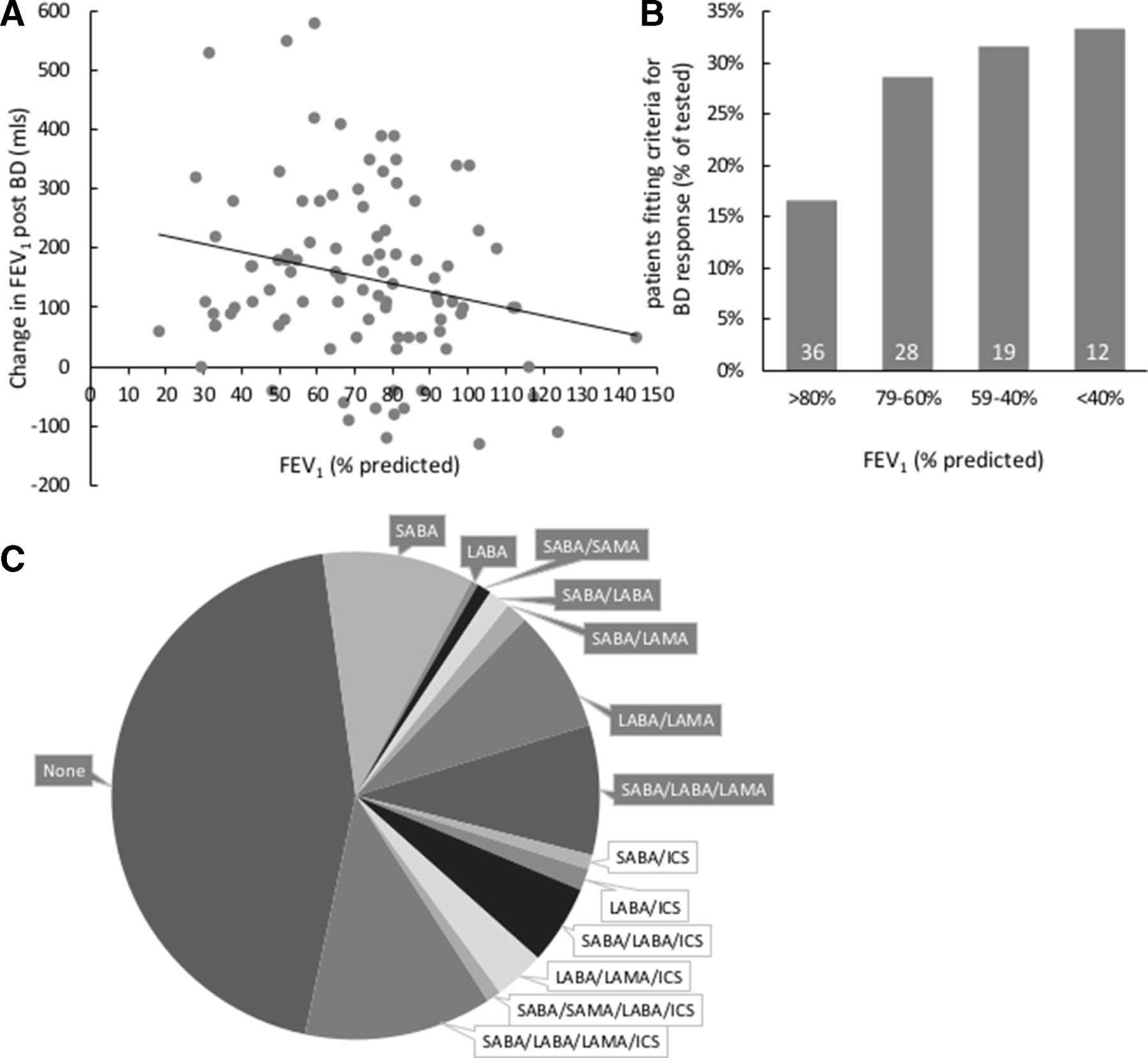
Two hundred and thirteen subjects were recruited; the mean age at onset of symptoms was 37 (SD 12.9) years and subjects were 50 (12.3) years at the time of the study. Ninety-five subjects had had bronchodilator reversibility testing. Subjects tested for reversibility were of similar age and lung function to those who were not (see online supplementary file 1). For those tested, the mean increase in FEV1 after salbutamol was 9.5% (10) with 20% fitting prespecified reversibility criteria.
In the 95 tested, reversibility was associated with airflow obstruction, younger age and lower gas transfer (figure 1 and table 1). Unsurprisingly, those with reversibility were more likely to be treated with bronchodilators, but also ICS and rapamycin (table 1). One hundred and eighteen subjects (55%) were using at least one inhaled drug. Indications for inhaled therapy were LAM in 68%, LAM with coexistent asthma or COPD in 18% and a previous incorrect diagnosis of asthma or COPD in 13%.

{kind=link}
Reversibility and inhaler use in LAM. (A) Change in FEV1 in women with LAM in response to salbutamol correlated with baseline FEV1. N=95, Pearson’s correlation r=−0.22; 95% CI −0.406 to −0.023, p=0.049. (B) Percentage women with LAM fitting criteria for bronchodilator reversibility grouped according to baseline FEV1. White figures in columns represent the number tested in each group. (C) Pie chart representing inhaler classes and combinations used to treat women with LAM. Grey labels highlight bronchodilators only, white labels bronchodilators plus ICS. ICS inhaled corticosteroid; LABA long-acting beta agonist; LAM, lymphangioleiomyomatosis; LAMA, long-acting muscarinic antagonist; SABA, short-acting beta agonist.
Clinical associations with bronchodilator reversibility
Patients who used inhalers had longer disease duration (mean difference 3 years, 95% CI 0.5 to 5.6, p=0.019), lower FEV1 (mean difference −19% predicted, 95% CI −25 to −12, p=0.0001) and diffusing capacity of the lungs for carbon monoxide (DLCO) (mean difference −12% predicted, 95% CI −17 to −6, p=0.0001). Thirteen combinations of inhaler classes were used: these ranged from short-acting beta agonists (SABA) alone in 20% of those treated to SABA, long-acting beta agonist (LABA), long-acting antimuscarinic (LAMA) and ICS in 23%. Fifty-five per cent were using a LAMA/LABA combination either alone or with other therapy (figure 1). We examined the relationship between inhaler use and rate of FEV1 decline. As mTOR inhibitors affect FEV1 decline, these patients were excluded. One hundred and nineteen subjects had FEV1 measurements greater than 12 months apart (mean of 5.5 (3.2) measurements over 47 (37) months). For all subjects, increasing inhaler class use was associated with bronchodilator reversibility (r2 0.254, p<0.0001) and FEV1 decline (r2 0.052, p=0.012). Subjects not using inhalers had a mean loss of FEV1 of 50 (110) mL/year, whereas those treated with four inhaler classes lost 189 (480) mL/year (mean difference 139 mL/year, 95% CI −280 to −7, p=0.039). FEV1 decline was not different in those treated with ICS and bronchodilators compared with bronchodilators alone (mean difference 15 mL/year, 95% CI −146 to 116, p=0.81, table 2).
Inhaler classes and lung function
Discussion
Twenty per cent of women with LAM fitted standard criteria for bronchodilator reversibility. Patients with reversibility were younger, had lower DLCO values and more were likely to be treated with inhalers and rapamycin. Many had lower levels of reversibility that may also be clinically beneficial. Despite airflow obstruction and dyspnoea, many patients were not tested for reversibility (table 1). Over half of all patients were prescribed inhalers, including ICS in almost one quarter. Inhaler use was associated with airflow obstruction and reversibility and both bronchodilator and ICS use were associated with higher rates of FEV1 decline.
Our findings suggest that those with more advanced disease and rapid FEV1 decline are preferentially treated with inhalers. Although the study was not designed to test efficacy, patients continued to take bronchodilators suggesting they may improve symptoms; however, disease progression did not appear significantly improved by bronchodilators or ICS. Anecdotally, patients with airway obstruction and reversibility are likely to benefit from bronchodilators and recent evidence suggests beta agonists may affect disease activity in LAM.7 However, which patient will benefit from which drug is unknown and currently, while many are not being evaluated or treated, others may be overtreated and no consensus on the optimal regimen exists. There have been no studies of ICS in LAM and their use may be based on an initial misdiagnosis of asthma. Although a number of women will have asthma and LAM, these individuals are likely to be identifiable from the history and investigations, whereas reversibility without other features of asthma is likely to be due to LAM alone. As ICS are associated with an increased risk of pneumonia, we suggest ICS be reserved for use in true co-existent asthma and clinical trials.9
Collectively, these observations highlight the need for prospective studies to determine the effect of inhaled therapy on quality of life and disease progression in LAM. LAMA/LABA combinations are well tolerated, more effective than single agents in COPD,10 used frequently in LAM and seem appropriate candidates to evaluate prospectively for LAM.
Footnotes
Contributors SJ devised the study, saw all patients, entered the study data, analysed the results and wrote the paper. JJ analysed the data and wrote the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The East Midlands Research Ethics Committee approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves