Article Text

Abstract
Given the increasing importance of establishing a microbiological aetiology in pneumonia, we undertook a study assessing the safety and acceptability of bedside ultrasound-guided TLNA (REC No. 09/H0605/12). TLNA has previously reported to have been predominantly undertaken without radiological control.
Methods Participants with community- or hospital-acquired pneumonia completed a baseline assessment of chest pain and pain associated with phlebotomy using a 10 cm visual analogue scale (VAS). Post procedure, participants assessed pain associated with TLNA, and undertook a Likert-based evaluation of the procedure.
Up to 3 mg/kg lidocaine was used to anaesthetise the skin and pleura. An ultrafine 25G needle, attached to a 20 ml luer lock syringe containing 3.5 ml 0.9% sodium chloride solution was inserted into consolidated lung under direct ultrasound guidance by a Respiratory Physician. 0.5 ml of the sodium chloride was injected followed by aspiration with gentle agitation (3 mL of sodium chloride remaining in the syringe as a carrier solution). The needle was then withdrawn. Any pleural fluid present was also aspirated separately.
Samples underwent culture and 16S rRNA gene analysis.
All participants had follow-up chest X-rays post procedure to evaluate for pneumothorax. Participants were systematically assessed while inpatient, and again at 30 days, to assess for any adverse events.
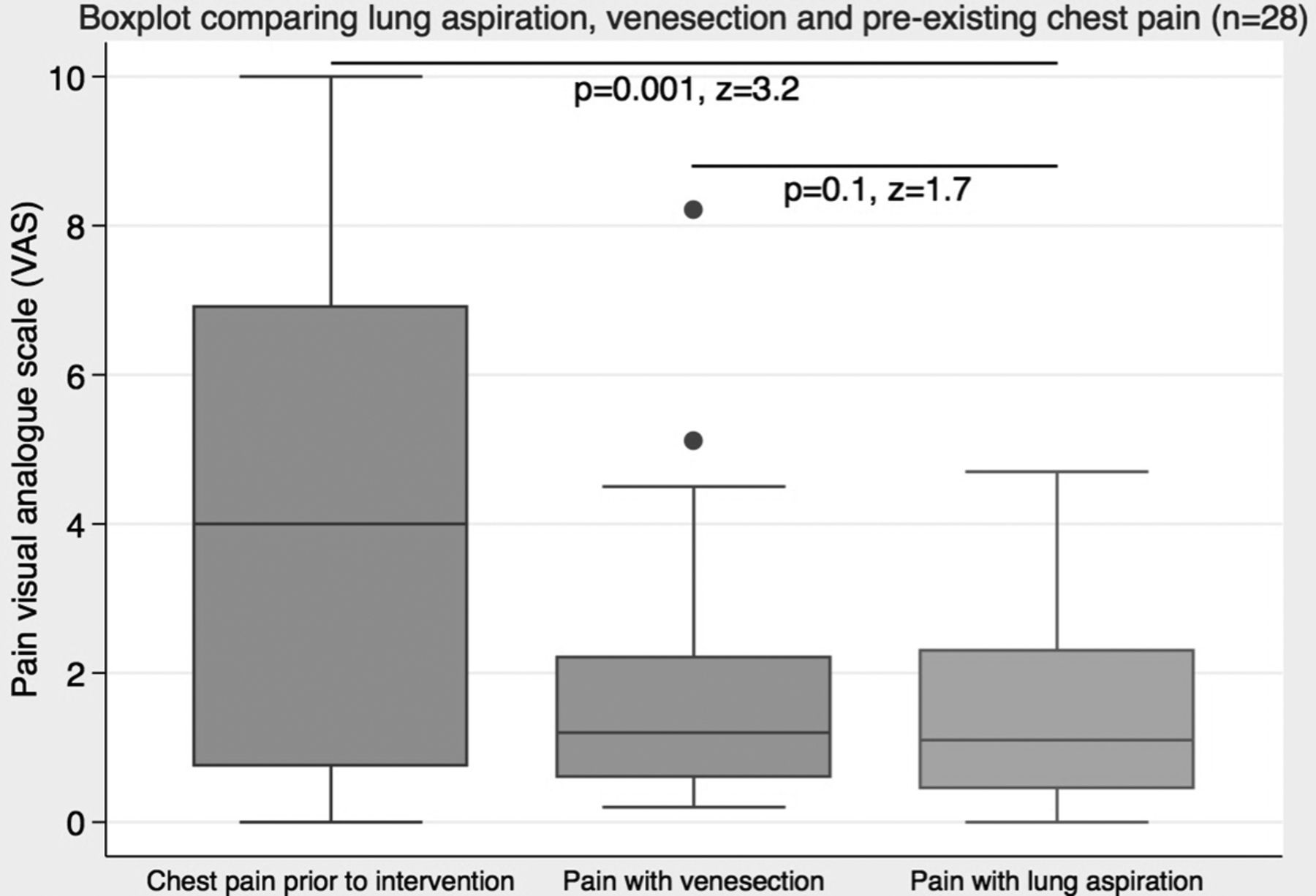
Results 28 participants underwent TLNA, 27 using ultrasound (and one using CT-guidance). No patients experienced haemoptysis or pneumothorax. All patients either ‘strongly agreed’ (most commonly) or ‘agreed’ with the statements: ‘The lung fluid sample to diagnose your pneumonia was tolerable’; and ‘I would have the lung fluid sample again if my doctors thought it was essential’. The VAS-assessed pain of TLNA was significantly lower than any pre-existing chest pain, being similar to any pain associated with venesection (see Figure).
At day 30, one patient had mild ongoing pain at the site of both TLNA and subsequent chest tube insertion, although the relative contribution of each procedure to this pain was unclear.
TLNA increased culture or sequencing-based aetiological diagnosis from 3/28 to 14/28 (18/28 when including pleural fluid analysis).
Conclusions Physician-performed bedside ultrasound-guided TLNA appears safe and well-tolerated.
{kind=link}